You might also like
- Intraoral Fluoride-Releasing Devices A Literature ReviewDocument5 pagesIntraoral Fluoride-Releasing Devices A Literature ReviewBagis Emre GulNo ratings yet
- Terapia de Fluor AAPDDocument4 pagesTerapia de Fluor AAPDAndy HerreraNo ratings yet
- BP FluorideTherapyDocument4 pagesBP FluorideTherapyKavana SrinivasNo ratings yet
- Article Fluocaril Casals Boukpessi FALTANGRAFICASDocument20 pagesArticle Fluocaril Casals Boukpessi FALTANGRAFICASLira May LachicaNo ratings yet
- Guide to Fluoride TherapyDocument4 pagesGuide to Fluoride TherapymirfanulhaqNo ratings yet
- G Fluoridetherapy PDFDocument4 pagesG Fluoridetherapy PDFChandrika VeerareddyNo ratings yet
- Fluoride Therapy: Latest RevisionDocument4 pagesFluoride Therapy: Latest RevisionLaura ZahariaNo ratings yet
- Fluorides in Periodontal Therapy: A Review of the Benefits and ConsiderationsDocument4 pagesFluorides in Periodontal Therapy: A Review of the Benefits and ConsiderationsNurhikmah RnNo ratings yet
- Topical Application of Fluoride and Its Anti-Cariogenic EffectDocument7 pagesTopical Application of Fluoride and Its Anti-Cariogenic Effectsintia saputraNo ratings yet
- Malaysian Dental Council Backs Water FluoridationDocument35 pagesMalaysian Dental Council Backs Water FluoridationYeoh Wei Keong100% (1)
- 04-14-08 Application of F and CaPDocument8 pages04-14-08 Application of F and CaPvelangniNo ratings yet
- Topical Application of Fluoride and Its Anti-Cariogenic EffectDocument7 pagesTopical Application of Fluoride and Its Anti-Cariogenic Effectkhalisha salsabilaNo ratings yet
- Cosmetics 08 00113Document12 pagesCosmetics 08 00113Lira May LachicaNo ratings yet
- Fluoride Therapy: Latest RevisionDocument4 pagesFluoride Therapy: Latest RevisionHamdy AlmaghrabyNo ratings yet
- Fluoride TherapyDocument4 pagesFluoride TherapyمعتزباللهNo ratings yet
- FluoridesDocument54 pagesFluoridesNAUMAN SHAHNo ratings yet
- Topical Application of Fluoride and Its Anti-Cariogenic EffectDocument7 pagesTopical Application of Fluoride and Its Anti-Cariogenic EffectRifka Zahrotun NisaNo ratings yet
- Advanced Drug Delivery Systems For Local Treatment of The Oral CavityDocument24 pagesAdvanced Drug Delivery Systems For Local Treatment of The Oral CavityanjaNo ratings yet
- Guideline On Fluoride Therapy: Review Council Latest RevisionDocument4 pagesGuideline On Fluoride Therapy: Review Council Latest RevisionThesya Aulia GeovanyNo ratings yet
- Polymers 03 00314Document16 pagesPolymers 03 00314Ulfahanny RachsetyaNo ratings yet
- Carie PreventionDocument13 pagesCarie Preventionatul_singh2001No ratings yet
- We Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistsDocument19 pagesWe Are Intechopen, The World'S Leading Publisher of Open Access Books Built by Scientists, For ScientistselNo ratings yet
- Topical Application of Fluoride and Its Anti-Cariogenic EffectDocument7 pagesTopical Application of Fluoride and Its Anti-Cariogenic EffectghozyelyussaNo ratings yet
- A Review of The Uses of Fluoride and Outcomes of - Dental Caries Control in SingaporeDocument5 pagesA Review of The Uses of Fluoride and Outcomes of - Dental Caries Control in SingaporeMichelleLeeNo ratings yet
- Wisdom Towards Remineralization, A Literature ReviewDocument5 pagesWisdom Towards Remineralization, A Literature ReviewIJAR JOURNALNo ratings yet
- Flouride in Dentistry by Ammar MohammedDocument10 pagesFlouride in Dentistry by Ammar Mohammedعمار محمد عباسNo ratings yet
- Essay SDFDocument20 pagesEssay SDFDebasmita Datta GuptaNo ratings yet
- A Novel Approach in Oral Fast Dissolving Drug Delivery System and Their PatentsDocument14 pagesA Novel Approach in Oral Fast Dissolving Drug Delivery System and Their PatentsnikitoNo ratings yet
- Topical Fluoride PrintDocument45 pagesTopical Fluoride PrintAmal ANo ratings yet
- Fluoride Toothpastes and Fluoride Mouthrinses For Home UseDocument11 pagesFluoride Toothpastes and Fluoride Mouthrinses For Home UsePînzariu GeorgeNo ratings yet
- Fluoride - Is It Capable of Fighting Old and New Dental Diseases?Document4 pagesFluoride - Is It Capable of Fighting Old and New Dental Diseases?Mara MHNo ratings yet
- Systemic FluoridesDocument18 pagesSystemic FluoridesLilly PaulNo ratings yet
- Project Final 2023 PratikDocument24 pagesProject Final 2023 PratikPratik sableNo ratings yet
- Presentation On Mitigation of FluorosisDocument67 pagesPresentation On Mitigation of FluorosisViswa NathanNo ratings yet
- Actives in Oral Care Products Reduce Tooth DecayDocument5 pagesActives in Oral Care Products Reduce Tooth DecayparekhtechNo ratings yet
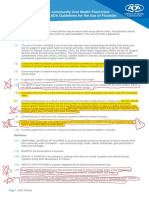
- Community Oral Health Promotion: Fluoride Use PolicyDocument5 pagesCommunity Oral Health Promotion: Fluoride Use PolicyTalat SultanaNo ratings yet
- FluoridesDocument52 pagesFluoridesRahel CharikarNo ratings yet
- Adsorption of Flouride Using Nanoparticles of Aluminium OxideDocument15 pagesAdsorption of Flouride Using Nanoparticles of Aluminium OxideIsa musaNo ratings yet
- The Rule of Fluoride Varnish in The Prevention of Dental Caries Among ChildrenDocument6 pagesThe Rule of Fluoride Varnish in The Prevention of Dental Caries Among ChildrenTariq AzizNo ratings yet
- CCIDEN 15943 A Concise Review Regarding Erosion and Abrasion On Tooth STR 071511Document8 pagesCCIDEN 15943 A Concise Review Regarding Erosion and Abrasion On Tooth STR 071511Floria DimitriuNo ratings yet
- Oral Health Promotion and FluorideDocument42 pagesOral Health Promotion and FluorideZAWWIN HLAINGNo ratings yet
- IC Method ToothpasteDocument8 pagesIC Method ToothpasteLira May LachicaNo ratings yet
- Defluoridation Methods - ReviewDocument9 pagesDefluoridation Methods - ReviewHansa KunduNo ratings yet
- Topical Fluorides in Caries Prevention and Management: A North American PerspectiveDocument6 pagesTopical Fluorides in Caries Prevention and Management: A North American PerspectivecsryderNo ratings yet
- Anticaries AgentsDocument12 pagesAnticaries AgentsHridoyul IslamNo ratings yet
- IJHS-5126+1-9Document9 pagesIJHS-5126+1-9hariniNo ratings yet
- BDA Fact File - FluorideDocument4 pagesBDA Fact File - FluorideAainaa KhairuddinNo ratings yet
- Cariology FellowshipDocument70 pagesCariology Fellowshipraghh roooNo ratings yet
- Fluoride: Its Role in Dentistry: Understanding Dental Caries and The Fluoride EffectDocument9 pagesFluoride: Its Role in Dentistry: Understanding Dental Caries and The Fluoride Effectfoncl brc sphNo ratings yet
- FluoridesDocument2 pagesFluoridesEshal MuzaffarNo ratings yet
- Topical Fluorides in Caries Prevention and Management: A North American PerspectiveDocument7 pagesTopical Fluorides in Caries Prevention and Management: A North American PerspectiveRohma DwiNo ratings yet
- Short-Term Fluoride Release and Recharge From Pit-and-Fissure SealantsDocument0 pagesShort-Term Fluoride Release and Recharge From Pit-and-Fissure SealantsPascalis Adhi KurniawanNo ratings yet
- Non Fluoride Caries Preventive AgentsDocument45 pagesNon Fluoride Caries Preventive AgentsSalwa HegazyNo ratings yet
- 32-IJDM-Rev-20200209Document5 pages32-IJDM-Rev-20200209amulya.kukutlaNo ratings yet
- Preparing the tooth for a celluloid crown restorationDocument4 pagesPreparing the tooth for a celluloid crown restorationCristinaNo ratings yet
- Topical and Systemic FluorideDocument12 pagesTopical and Systemic Fluoridemidoo47No ratings yet
- SDF, THE MAGIC BULLET FOR CARIES MANAGEMENTDocument22 pagesSDF, THE MAGIC BULLET FOR CARIES MANAGEMENTVinay MuppanaNo ratings yet
- Dentifrice PDFDocument16 pagesDentifrice PDFdivyarati100% (1)
- Flouride - and - Oral - Health - PDFDocument31 pagesFlouride - and - Oral - Health - PDFnatalyaNo ratings yet
- Flowering Trees CowenDocument97 pagesFlowering Trees CowenzzmehulNo ratings yet
- Unprotected-Okdokey Medical Passwords 2004 - 搜尋引擎 - JSEMTSDocument63 pagesUnprotected-Okdokey Medical Passwords 2004 - 搜尋引擎 - JSEMTSmanikantatssNo ratings yet
- Australian Dental JournalDocument7 pagesAustralian Dental JournalmanikantatssNo ratings yet
- Patient Safety Book PDFDocument59 pagesPatient Safety Book PDFshakeel mohmad100% (11)
- Straumann Sla: Scientific Evidence First Edition (2011)Document36 pagesStraumann Sla: Scientific Evidence First Edition (2011)manikantatssNo ratings yet
- Preprocedural Anxiety and Pain Perception Following Root Surface Debridement in Chronic Periodontitis PatientsDocument8 pagesPreprocedural Anxiety and Pain Perception Following Root Surface Debridement in Chronic Periodontitis PatientsmanikantatssNo ratings yet
- Comparison Hand Scaler, Ultrasonic and Vector in CGPDocument7 pagesComparison Hand Scaler, Ultrasonic and Vector in CGPmanikantatssNo ratings yet
- Sample Id: Sample Id: 6284347 Icmr Specimen Referral Form Icmr Specimen Referral Form For For Covid-19 (Sars-Cov2) Covid-19 (Sars-Cov2)Document2 pagesSample Id: Sample Id: 6284347 Icmr Specimen Referral Form Icmr Specimen Referral Form For For Covid-19 (Sars-Cov2) Covid-19 (Sars-Cov2)Praveen KumarNo ratings yet
- Utility and Validity of A Single-Item Visual Analog Scale ForDocument6 pagesUtility and Validity of A Single-Item Visual Analog Scale FormanikantatssNo ratings yet
- Relationship Between Dental Anxiety and Pain PerceptionDocument8 pagesRelationship Between Dental Anxiety and Pain PerceptionmanikantatssNo ratings yet
- Utility and Validity of A Single-Item Visual Analog Scale ForDocument6 pagesUtility and Validity of A Single-Item Visual Analog Scale FormanikantatssNo ratings yet
- Mahajns Modification Pblished IndexedDocument6 pagesMahajns Modification Pblished IndexedmanikantatssNo ratings yet
- Evaluation of The Ability of Dental Clinicians To Rate Dental AnxietyDocument7 pagesEvaluation of The Ability of Dental Clinicians To Rate Dental AnxietymanikantatssNo ratings yet
- Relationship Between Dental Anxiety and Pain PerceptionDocument8 pagesRelationship Between Dental Anxiety and Pain PerceptionmanikantatssNo ratings yet
- Gingivitis en inDocument2 pagesGingivitis en inmanikantatssNo ratings yet
- Listerine Oral Health Care Program: Department of PeriodonticsDocument1 pageListerine Oral Health Care Program: Department of PeriodonticsmanikantatssNo ratings yet
- IjosDocument0 pagesIjosmanikantatssNo ratings yet
- Longitudinal Studies Observing Gingival Recession - Rate of Gingival Recession - Quote StudiesDocument2 pagesLongitudinal Studies Observing Gingival Recession - Rate of Gingival Recession - Quote StudiesmanikantatssNo ratings yet
- Determination of Optimum Adhesive Thickness Using Varying Degrees of Force Application With Light-Cured Adhesive and Its Effect On The Shear Bond Strength of Orthodontic Brackets - An in Vitro StudyDocument2 pagesDetermination of Optimum Adhesive Thickness Using Varying Degrees of Force Application With Light-Cured Adhesive and Its Effect On The Shear Bond Strength of Orthodontic Brackets - An in Vitro StudymanikantatssNo ratings yet
- Eur J Orthod 2012 Yoshida 493 7Document5 pagesEur J Orthod 2012 Yoshida 493 7manikantatssNo ratings yet
- Eur J Orthod 2012 Yoshida 493 7Document5 pagesEur J Orthod 2012 Yoshida 493 7manikantatssNo ratings yet
- ClassificationDocument85 pagesClassificationmanikantatssNo ratings yet
- Eur J Orthod 2012 Al Hity 505 11Document7 pagesEur J Orthod 2012 Al Hity 505 11manikantatssNo ratings yet
- IjosDocument0 pagesIjosmanikantatssNo ratings yet
- Work Invoice for DateDocument1 pageWork Invoice for DatemanikantatssNo ratings yet
- Antibiotics in DentistryDocument3 pagesAntibiotics in DentistrymanikantatssNo ratings yet
- 41Document10 pages41manikantatssNo ratings yet
- Dental Management of Patients Receiving Anticoagulation or Antiplatelet TreatmentDocument0 pagesDental Management of Patients Receiving Anticoagulation or Antiplatelet TreatmentmanikantatssNo ratings yet
- 3 2 2 PBDocument14 pages3 2 2 PBmanikantatssNo ratings yet
- Intraoral Fluoride-Releasing Devices: A Literature ReviewDocument0 pagesIntraoral Fluoride-Releasing Devices: A Literature ReviewmanikantatssNo ratings yet