You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- SI Joint Dysfunction Treatment Protocols: Presenter NotesDocument15 pagesSI Joint Dysfunction Treatment Protocols: Presenter NotesMichel BakkerNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Alternative Health TherapiesDocument415 pagesAlternative Health TherapiesTris TanNo ratings yet
- Westside For Skinny Bastards, Part III: The Final ChapterDocument20 pagesWestside For Skinny Bastards, Part III: The Final ChapterMichel BakkerNo ratings yet
- Treatment of Sacroiliac Joint DysfunctionDocument46 pagesTreatment of Sacroiliac Joint DysfunctionMichel Bakker100% (5)
- Vimśottari Daśā: The Best Udu DaśāDocument19 pagesVimśottari Daśā: The Best Udu Daśāpaparock34100% (5)
- Integration Procedure of Telecom System WHP andDocument53 pagesIntegration Procedure of Telecom System WHP andselamet riantoNo ratings yet
- MC Sci 101 - Module 1Document12 pagesMC Sci 101 - Module 1Judith Valenzuela100% (2)
- Lumbar Instability Ands Exercises 2000Document11 pagesLumbar Instability Ands Exercises 2000Francisco Javier Quinteros GarcíaNo ratings yet
- The Pain Catastrophizing Scale: User ManualDocument36 pagesThe Pain Catastrophizing Scale: User ManualAlina Isabela CurtNo ratings yet
- Case Report - Low Back BainDocument2 pagesCase Report - Low Back BainMichel BakkerNo ratings yet
- IFOMPT Examination Cervical Spine Doc September 2012 DefinitiveDocument37 pagesIFOMPT Examination Cervical Spine Doc September 2012 DefinitiveMichel BakkerNo ratings yet
- Bekken. Load Transfer TestsDocument6 pagesBekken. Load Transfer TestsMichel BakkerNo ratings yet
- Filip D - Kineclub 2011 Herkennen CSDocument8 pagesFilip D - Kineclub 2011 Herkennen CSMichel BakkerNo ratings yet
- Mulligan Concept Conference Abstract BookDocument89 pagesMulligan Concept Conference Abstract BookMichel BakkerNo ratings yet
- Wedel SIGDocument120 pagesWedel SIGMichel BakkerNo ratings yet
- Sacrum Self Study GuideDocument24 pagesSacrum Self Study GuideMichel BakkerNo ratings yet
- 1g El©:1g Mwg÷vi (1: Course No Course Tittle Hours/Week Theory + Lab CreditsDocument29 pages1g El©:1g Mwg÷vi (1: Course No Course Tittle Hours/Week Theory + Lab Creditsshajib_sustNo ratings yet
- MEIOSIS and MITOSISDocument4 pagesMEIOSIS and MITOSISHannaj May De GuzmanNo ratings yet
- 12V 1AMP Power Supply Using LM7182 RegulatorDocument13 pages12V 1AMP Power Supply Using LM7182 RegulatorNURUL AISYAHNo ratings yet
- Certificate of Appreciation: Kingdom of Cambodia Nation Religion KingDocument18 pagesCertificate of Appreciation: Kingdom of Cambodia Nation Religion KingLittle NerdNo ratings yet
- Bonaventure ResumeDocument1 pageBonaventure Resumeapi-631877498No ratings yet
- ESSAYDocument4 pagesESSAYFrans Raff LopezNo ratings yet
- Tales of The Grotesque and Arabesque - Edgar Allan Poe PDFDocument274 pagesTales of The Grotesque and Arabesque - Edgar Allan Poe PDFCosmin PopaNo ratings yet
- Safe ImportETABSintoSAFEFAQ 200321 0833 121826Document1 pageSafe ImportETABSintoSAFEFAQ 200321 0833 121826Harshit NagarNo ratings yet
- Module 1 2020Document130 pagesModule 1 2020Shemin Shaji33% (9)
- African Forest ElephantDocument13 pagesAfrican Forest ElephantAlison_VicarNo ratings yet
- Proposed Block of Four Flats Design InformationDocument2 pagesProposed Block of Four Flats Design InformationChristopher UcheNo ratings yet
- CE 555 Hydraulics Lecture and Tutorial OverviewDocument5 pagesCE 555 Hydraulics Lecture and Tutorial OverviewbakrichodNo ratings yet
- 2 ENGLISH Board AKDocument4 pages2 ENGLISH Board AKRoseMay JimenaNo ratings yet
- United States International University - Africa: Master of Science Management & Organizational Development (Mod)Document5 pagesUnited States International University - Africa: Master of Science Management & Organizational Development (Mod)Brian LubangaNo ratings yet
- Learning Targets and Success CriteriaDocument10 pagesLearning Targets and Success Criteriaapi-310199974No ratings yet
- კემპბელი თ16 353 363 დნმ და რეპლიკაციაDocument11 pagesკემპბელი თ16 353 363 დნმ და რეპლიკაციაSosoNo ratings yet
- Autopoiesis and Cognition The Realization of The Living - Humberto Maturana and Francisco VarelaDocument86 pagesAutopoiesis and Cognition The Realization of The Living - Humberto Maturana and Francisco VarelaRodrigo Córdova ANo ratings yet
- S10.s4 Bearing-CapacityDocument20 pagesS10.s4 Bearing-CapacityRodolfo Jesus Calle FloresNo ratings yet
- Lubication Oil SystemDocument3 pagesLubication Oil SystemAustin UdofiaNo ratings yet
- A Safe Container For FearDocument3 pagesA Safe Container For FearMārs LaranNo ratings yet
- Empowerment Technology 10 FinalDocument9 pagesEmpowerment Technology 10 Finalandy gamingNo ratings yet
- 6486e4d8261cf100191eca5d - ## - Units and Dimension Assignment 01 Arjuna NEET 2024Document3 pages6486e4d8261cf100191eca5d - ## - Units and Dimension Assignment 01 Arjuna NEET 2024BhupendraNo ratings yet
- Apga Code of Environmental Practice PDFDocument130 pagesApga Code of Environmental Practice PDFmichaelsullivan1973No ratings yet
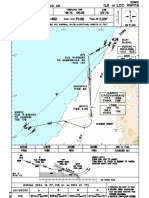
- Ils or Loc Rwy18: Apt Elev: Rwy18 THR Elev: Trans Level: Trans AltDocument1 pageIls or Loc Rwy18: Apt Elev: Rwy18 THR Elev: Trans Level: Trans AlttommyNo ratings yet
- HP1000 Chapter 1 Psychology Core Concepts NotesDocument8 pagesHP1000 Chapter 1 Psychology Core Concepts NotesRaidon JantanataNo ratings yet
- A Comparison Study of Credit Card Fraud Detection - Supervised Versus UnsupervisedDocument9 pagesA Comparison Study of Credit Card Fraud Detection - Supervised Versus Unsupervisedsahki hNo ratings yet