You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Shelter Quality Protocol 2014Document50 pagesShelter Quality Protocol 2014Tomislav Mikuš100% (1)
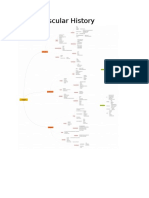
- Cardiovascular History MindmapDocument12 pagesCardiovascular History MindmapThe_BakerNo ratings yet
- RT ConsultDocument5 pagesRT ConsultRick Frea100% (2)
- New Patient FormDocument7 pagesNew Patient Forme-MedTools100% (4)
- Birthmarks Identificationandmx201205ryanDocument4 pagesBirthmarks Identificationandmx201205ryanDanielcc LeeNo ratings yet
- 14 Essentials To MxMT2013!09!029-BRODATY - 0Document11 pages14 Essentials To MxMT2013!09!029-BRODATY - 0Danielcc LeeNo ratings yet
- Full Blood Count Apr04, DR Eva RaikDocument7 pagesFull Blood Count Apr04, DR Eva RaikDanielcc LeeNo ratings yet
- Interpretation of The eGFR Jul 07Document8 pagesInterpretation of The eGFR Jul 07Danielcc LeeNo ratings yet
- 14 Essentials To Assessment and Care PlanMT2013!08!018-BRODATY - 0Document9 pages14 Essentials To Assessment and Care PlanMT2013!08!018-BRODATY - 0Danielcc Lee100% (1)
- Commonrashes in Neonates201205suDocument6 pagesCommonrashes in Neonates201205suDanielcc LeeNo ratings yet
- Lab TSTNG Acute Diarrhoea Sept03Document8 pagesLab TSTNG Acute Diarrhoea Sept03Danielcc LeeNo ratings yet
- DNA Genetic Testing, Mar04, Prof Ron TrentDocument7 pagesDNA Genetic Testing, Mar04, Prof Ron TrentDanielcc LeeNo ratings yet
- Bleeding Disorders March 2008Document8 pagesBleeding Disorders March 2008Danielcc LeeNo ratings yet
- Avoiding Unnecessary Laboratory Tests May 2008Document8 pagesAvoiding Unnecessary Laboratory Tests May 2008Danielcc LeeNo ratings yet
- Diagnosis of Iron Deficiency and Iron Overload Nov 06Document8 pagesDiagnosis of Iron Deficiency and Iron Overload Nov 06Danielcc LeeNo ratings yet
- Biochemical Measurements in OsteoporosisDocument7 pagesBiochemical Measurements in OsteoporosisDanielcc LeeNo ratings yet
- Diabetes Diagnosis and Monitoring, April 2002 Author Peter ColmanDocument13 pagesDiabetes Diagnosis and Monitoring, April 2002 Author Peter ColmanDanielcc LeeNo ratings yet
- Assessing Renal Function Aug04Document9 pagesAssessing Renal Function Aug04Danielcc LeeNo ratings yet
- Nonalcoholic Fatty Liver DiseaseDocument4 pagesNonalcoholic Fatty Liver DiseaseDanielcc LeeNo ratings yet
- Autoimmune Diseases Mar 2003Document12 pagesAutoimmune Diseases Mar 2003Danielcc LeeNo ratings yet
- Antenatal Screening For Down Syndrome - Nov 2007Document8 pagesAntenatal Screening For Down Syndrome - Nov 2007Danielcc LeeNo ratings yet
- Evaluation of Sleepy PatientsDocument4 pagesEvaluation of Sleepy PatientsDanielcc LeeNo ratings yet
- Box Jellyfish - Australian Venom Research UnitDocument2 pagesBox Jellyfish - Australian Venom Research UnitDanielcc LeeNo ratings yet
- Arthritis - Which Tests To Choose, and Which To Avoid Nov08Document9 pagesArthritis - Which Tests To Choose, and Which To Avoid Nov08Danielcc LeeNo ratings yet
- Diagnosis and Management of Chronic Heart Failure 2006: Quick Reference GuideDocument10 pagesDiagnosis and Management of Chronic Heart Failure 2006: Quick Reference GuideasharobeamNo ratings yet
- Mammalian Bites200911dendleDocument6 pagesMammalian Bites200911dendleDanielcc LeeNo ratings yet
- Spider Bites200911Document6 pagesSpider Bites200911Danielcc LeeNo ratings yet
- Blood Transfusion ProcedureDocument0 pagesBlood Transfusion ProcedureDanielcc LeeNo ratings yet
- Work Related Asthma201001Document4 pagesWork Related Asthma201001Danielcc LeeNo ratings yet
- Bed Bugs: What The GP Needs To KnowDocument5 pagesBed Bugs: What The GP Needs To KnowDanielcc LeeNo ratings yet
- Mosquito InfoDocument4 pagesMosquito InfoJessica FornoNo ratings yet
- Diarrhoea in TravellersDocument5 pagesDiarrhoea in TravellersMazo KhanNo ratings yet
- Deteting Familial Hyperholesterolaemia in General PratieDocument4 pagesDeteting Familial Hyperholesterolaemia in General PratieDanielcc LeeNo ratings yet
- Acute Bronchitis HandoutDocument5 pagesAcute Bronchitis HandoutDianne LegionNo ratings yet
- BPOC in Medicina PrimaraDocument3 pagesBPOC in Medicina PrimaraAlina GheNo ratings yet
- Pediatrics RemarksDocument62 pagesPediatrics RemarksGÖKSU SAYGILINo ratings yet
- 741 PUB Working Paper 35 PDFDocument34 pages741 PUB Working Paper 35 PDFBushra AsifNo ratings yet
- Cause and EffectDocument6 pagesCause and Effectpuskesmas sukaraja tigaNo ratings yet
- Atelectasis. Mechanisms, Diagnosis and Management (Peroni, 2000)Document5 pagesAtelectasis. Mechanisms, Diagnosis and Management (Peroni, 2000)Renato Li SoldevillaNo ratings yet
- Fast Facts On CoughsDocument12 pagesFast Facts On CoughsLany T. CataminNo ratings yet
- CÁC ĐỀ TỰ LUYỆNDocument25 pagesCÁC ĐỀ TỰ LUYỆNMai Anh NguyễnNo ratings yet
- Chronic Cough Differential DiagnosisDocument6 pagesChronic Cough Differential DiagnosisUbaidillah HafidzNo ratings yet
- RITS. Bronchial AsthmaDocument56 pagesRITS. Bronchial AsthmaRita100% (1)
- Funda Lab Mod 5-7Document13 pagesFunda Lab Mod 5-7Liane BartolomeNo ratings yet
- Who FCH Cah 00.1Document175 pagesWho FCH Cah 00.1Regita AyuNo ratings yet
- Formic Acid C BASF Medguidelines E036Document4 pagesFormic Acid C BASF Medguidelines E036varrsinneNo ratings yet
- Nursing Care Plan Proper CapcDocument4 pagesNursing Care Plan Proper CapcKit LaraNo ratings yet
- Mid Exam - General Pathology Ii - Siahs - Karim Ullah - Su-17!01!154-012Document6 pagesMid Exam - General Pathology Ii - Siahs - Karim Ullah - Su-17!01!154-012Bilal KhanNo ratings yet
- 2021 QuestionsDocument112 pages2021 QuestionsMohammad Alrefai100% (1)
- NR 509 Midterm PPDocument76 pagesNR 509 Midterm PPLou EscobarNo ratings yet
- Lung Meridian PDFDocument1 pageLung Meridian PDFrinkyNo ratings yet
- Orem's Assessment GuideDocument39 pagesOrem's Assessment Guidemaynard bairdNo ratings yet
- Nurs 5002 - Case Study 4Document17 pagesNurs 5002 - Case Study 4api-308904543100% (2)
- A Text Book of Materia Medica and Therapeutics of Rare Homoeopathic Remedies by Oscar HansenDocument136 pagesA Text Book of Materia Medica and Therapeutics of Rare Homoeopathic Remedies by Oscar Hansensunnyjamiel75% (4)
- Material Safety Data Sheet: Page 1 of 6Document6 pagesMaterial Safety Data Sheet: Page 1 of 6EndraNo ratings yet
- MCQ Nas Inggris 12 12 2013 Kirim PDFDocument16 pagesMCQ Nas Inggris 12 12 2013 Kirim PDFRoni ArmandaNo ratings yet
- Everest AyurvedaDocument29 pagesEverest AyurvedaSamhitha Ayurvedic ChennaiNo ratings yet
- Global Initiative For Asthma (2021) Guidelines: Peter Miranda 3 Year IM ResidentDocument32 pagesGlobal Initiative For Asthma (2021) Guidelines: Peter Miranda 3 Year IM ResidentPeter MirandaNo ratings yet
- Problem Nursing Diagnosis Background Knowledge Goal and Objective Nursing Intervention Rationale EvaluationDocument2 pagesProblem Nursing Diagnosis Background Knowledge Goal and Objective Nursing Intervention Rationale Evaluationcherrymae mataNo ratings yet