You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Icu Masterclass - Inotropes and Vasopressors: Christopher R. Tainter, MDDocument78 pagesIcu Masterclass - Inotropes and Vasopressors: Christopher R. Tainter, MDHhaNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Dr. Madaan Anatomy MCQ 2-2 (Muhadharaty)Document46 pagesDr. Madaan Anatomy MCQ 2-2 (Muhadharaty)Joseph Brima SambaNo ratings yet
- DR. APPIAH'S GUIDE TO KIDNEY FUNCTION AND DISEASEDocument71 pagesDR. APPIAH'S GUIDE TO KIDNEY FUNCTION AND DISEASEreuben kwotaNo ratings yet
- CC Lab 6 TransesDocument6 pagesCC Lab 6 TransesCiara PamonagNo ratings yet
- Textbook of Echocardiography For Intensivists and Emergency PhysiciansDocument567 pagesTextbook of Echocardiography For Intensivists and Emergency PhysiciansYeseniaNo ratings yet
- Beta Blockers and Other Sympatholytic AgentsDocument43 pagesBeta Blockers and Other Sympatholytic AgentsAriel OlshevskyNo ratings yet
- Case Report: Hepatic Artery Aneurysm.a Rare Visceral AneurysmDocument5 pagesCase Report: Hepatic Artery Aneurysm.a Rare Visceral AneurysmIJAR JOURNALNo ratings yet
- Fry Et Al 2017Document9 pagesFry Et Al 2017Ernest YipNo ratings yet
- Eacpr: European Association For Cardiovascular Prevention and RehabilitationDocument76 pagesEacpr: European Association For Cardiovascular Prevention and RehabilitationalbasudNo ratings yet
- Study Guide Cvs 2016Document24 pagesStudy Guide Cvs 2016Muhammad FaizanNo ratings yet
- Ezetimibe An Overeview of Analytical Methods For The Drug SubstanceDocument6 pagesEzetimibe An Overeview of Analytical Methods For The Drug SubstanceEditor IJTSRDNo ratings yet
- Blank 10Document4 pagesBlank 10Pari SharmaNo ratings yet
- Cooperative Activity 3-4 Through 3-8Document7 pagesCooperative Activity 3-4 Through 3-8Thalia Sanders0% (1)
- Haemodynamic Monitoring With Pulse-Induced Contour Cardiac Output (PiCCO) in Critical CareDocument7 pagesHaemodynamic Monitoring With Pulse-Induced Contour Cardiac Output (PiCCO) in Critical CareClaudia IsabelNo ratings yet
- Programa de Instrumentacion Quirurgica: Planeamiento Quirurgico Formativa IQX-FT-003-BUCDocument7 pagesPrograma de Instrumentacion Quirurgica: Planeamiento Quirurgico Formativa IQX-FT-003-BUCapi-688140642No ratings yet
- Infant of A Diabetic MotherDocument20 pagesInfant of A Diabetic MotherElvisNo ratings yet
- Pediatric Surgery Notes For NursesDocument8 pagesPediatric Surgery Notes For NursesAhmed SamyNo ratings yet
- Inotropes: Learning ObjectivesDocument7 pagesInotropes: Learning ObjectivesOrion JohnNo ratings yet
- Epithelial and connective tissue types in the human bodyDocument4 pagesEpithelial and connective tissue types in the human bodyrenee belle isturisNo ratings yet
- ASCOT Hypertension StudyDocument12 pagesASCOT Hypertension StudyAnonymous NeRC5JYiSNo ratings yet
- Assignment 1 B2019010Document9 pagesAssignment 1 B2019010bhushanNo ratings yet
- DR Suhail Sarwar Siddiqui MD, DM, Edic Assistant Professor Department of Critical Care Medicine King George's Medical University (KGMU) LucknowDocument39 pagesDR Suhail Sarwar Siddiqui MD, DM, Edic Assistant Professor Department of Critical Care Medicine King George's Medical University (KGMU) LucknowRaghavNo ratings yet
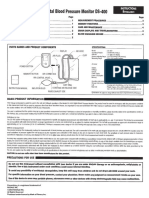
- Digital Blood Pressure Monitor DS-400: Parts Names and Product ComponentsDocument4 pagesDigital Blood Pressure Monitor DS-400: Parts Names and Product ComponentsJorNo ratings yet
- Cardiopulmonary Cerebral ResuscitationDocument17 pagesCardiopulmonary Cerebral ResuscitationrizalNo ratings yet
- Acido BaseDocument10 pagesAcido Basebenitez1228No ratings yet
- The Heart Pumps Blood CirculationDocument9 pagesThe Heart Pumps Blood CirculationShokefun OlawaleNo ratings yet
- Essence of Anesthesia Practice e Book 4th Edition Ebook PDFDocument61 pagesEssence of Anesthesia Practice e Book 4th Edition Ebook PDFalla.adams464100% (45)
- Hesi Hints Part 4Document2 pagesHesi Hints Part 4Sharon TanveerNo ratings yet
- Biology Practice Questions on Respiratory and Circulatory SystemsDocument9 pagesBiology Practice Questions on Respiratory and Circulatory SystemsDarshini SankerNo ratings yet
- CVA Stroke Guide: Symptoms, Causes, TreatmentDocument6 pagesCVA Stroke Guide: Symptoms, Causes, TreatmentBrenn Marie RamosNo ratings yet