You might also like
- Manual WashingtonDocument1 pageManual WashingtonArcenciel26No ratings yet
- MG, Forma Oculara MG, Forma GeneralizataDocument1 pageMG, Forma Oculara MG, Forma GeneralizataArcenciel26No ratings yet
- Toxin Induced Neuropathy Presenting As AIDP PDFDocument2 pagesToxin Induced Neuropathy Presenting As AIDP PDFArcenciel26No ratings yet
- Richmond Agitation Sedation Scale (RASS)Document1 pageRichmond Agitation Sedation Scale (RASS)Arcenciel26No ratings yet
- The Neuropathy Resident Tutorial 54Document96 pagesThe Neuropathy Resident Tutorial 54Surat TanprawateNo ratings yet
- Medications Causing ParkinsonismDocument1 pageMedications Causing ParkinsonismArcenciel26No ratings yet
- Medication-Induced Neuropathies PDFDocument11 pagesMedication-Induced Neuropathies PDFArcenciel26No ratings yet
- Chapter 13 Sarcoidosis Joint Muscle and BoneDocument10 pagesChapter 13 Sarcoidosis Joint Muscle and BoneomarbenhagiNo ratings yet
- POEMS SyndromeDocument4 pagesPOEMS SyndromeArcenciel26No ratings yet
- Myositis Disorders PDFDocument3 pagesMyositis Disorders PDFArcenciel26No ratings yet
- Kinesia ParadoxaDocument7 pagesKinesia ParadoxaArcenciel26No ratings yet
- Grapefruit Drug InteractionsDocument5 pagesGrapefruit Drug InteractionsArcenciel26No ratings yet
- Pro TaminaDocument2 pagesPro TaminaArcenciel26No ratings yet
- The Role of Left Prefrontal Cortex in Language and MemoryDocument30 pagesThe Role of Left Prefrontal Cortex in Language and MemoryArcenciel26No ratings yet
- Anticoagulare Post-IMA - 3 Luni Sau Mai MultDocument1 pageAnticoagulare Post-IMA - 3 Luni Sau Mai MultI.m. DanielNo ratings yet
- Anticoagulation Therapy Following Embolic or Hemorrhagic Stroke in The Patient With A Mechanical Heart ValveDocument8 pagesAnticoagulation Therapy Following Embolic or Hemorrhagic Stroke in The Patient With A Mechanical Heart ValveArcenciel26No ratings yet
- CSF Pleocytosis Is Not Always Present in HSV Infection of The Nervous SystemDocument1 pageCSF Pleocytosis Is Not Always Present in HSV Infection of The Nervous SystemArcenciel26No ratings yet
- Practical Guide - DabigatranDocument13 pagesPractical Guide - DabigatranArcenciel26No ratings yet
- Milgamma Si NeuromultivitDocument1 pageMilgamma Si NeuromultivitArcenciel26100% (1)
- Pain and Deficits Associated With Specific Nerve RootsDocument1 pagePain and Deficits Associated With Specific Nerve RootsArcenciel26No ratings yet
- Thalamic Aphasia SyndromeDocument1 pageThalamic Aphasia SyndromeArcenciel26No ratings yet
- Anti-Titin Antibodies in MG - Tight Association With Thymoma and Heterogeneity of Nonthymoma PatientsDocument1 pageAnti-Titin Antibodies in MG - Tight Association With Thymoma and Heterogeneity of Nonthymoma PatientsArcenciel26No ratings yet
- Apraxia and Related SyndromesDocument7 pagesApraxia and Related SyndromesArcenciel26No ratings yet
- Diagnostic Criteria For Myasthenia GravisDocument2 pagesDiagnostic Criteria For Myasthenia GravisArcenciel26No ratings yet
- Reminyl for Mild to Moderate Alzheimer's DementiaDocument4 pagesReminyl for Mild to Moderate Alzheimer's DementiaArcenciel26No ratings yet
- Normal CT ScanDocument1 pageNormal CT ScanArcenciel26No ratings yet
- Statins May Aggravate Myasthenia GravisDocument1 pageStatins May Aggravate Myasthenia GravisArcenciel26No ratings yet
- VimpatDocument43 pagesVimpatArcenciel26No ratings yet
- Memoria Si InvatareaDocument63 pagesMemoria Si InvatareaArcenciel26No ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Nicotrol InhalerDocument19 pagesNicotrol InhalerdebysiskaNo ratings yet
- PharmD 1st Year SyllabusDocument21 pagesPharmD 1st Year SyllabusAshwat ANo ratings yet
- Battle of BrainDocument7 pagesBattle of BrainKhalida Zia SiregarNo ratings yet
- Refeeding SyndromeDocument4 pagesRefeeding SyndromeallyNo ratings yet
- Come Thirsty Chapter1Document4 pagesCome Thirsty Chapter1Natalia Lupasco100% (1)
- Anesthesiology Resident Survival Guide 2014-2015Document32 pagesAnesthesiology Resident Survival Guide 2014-2015Karla Matos100% (1)
- Pancoast Tumour: Rare Lung Cancer FormDocument2 pagesPancoast Tumour: Rare Lung Cancer FormobligatraftelNo ratings yet
- Template POMRDocument8 pagesTemplate POMRPPDS IPD ULMNo ratings yet
- Anesthesia For The Pet Practitioner (2011 3rd Edition)Document216 pagesAnesthesia For The Pet Practitioner (2011 3rd Edition)Amela Dolittle Halilbašić100% (5)
- Pathology - Cardiovascular SystemDocument17 pagesPathology - Cardiovascular SystemNdegwa Jesse100% (2)
- Anatomy of A ClamDocument6 pagesAnatomy of A ClamRU VickNo ratings yet
- 2018 Life Sciences Tsset (Answers With Explanation)Document24 pages2018 Life Sciences Tsset (Answers With Explanation)Swetha SrigirirajuNo ratings yet
- Upper Limb MCQsDocument50 pagesUpper Limb MCQsstephen victory100% (1)
- Pengaruh Faktor-Faktor Psikososial Dan Insomnia Terhadap Depresi Pada Lansia Di Kota YogyakartaDocument5 pagesPengaruh Faktor-Faktor Psikososial Dan Insomnia Terhadap Depresi Pada Lansia Di Kota YogyakartaKristina Puji LestariNo ratings yet
- Led Light Therapy GuideDocument23 pagesLed Light Therapy GuidePeter Freimann100% (4)
- The Management of Intra Abdominal Infections From A Global Perspective 2017 WSES Guidelines For Management of Intra Abdominal InfectionsDocument34 pagesThe Management of Intra Abdominal Infections From A Global Perspective 2017 WSES Guidelines For Management of Intra Abdominal InfectionsJuan CastroNo ratings yet
- COPING WITH STRESSDocument16 pagesCOPING WITH STRESSDionisius KevinNo ratings yet
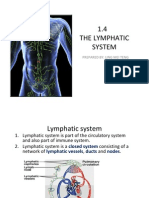
- 1.4 The Lymphatic System: Prepared By: Ling Mei TengDocument15 pages1.4 The Lymphatic System: Prepared By: Ling Mei TengJuliet LingNo ratings yet
- Muscles of Mastication Functions and Clinical SignificanceDocument130 pagesMuscles of Mastication Functions and Clinical SignificanceDevanand GuptaNo ratings yet
- AP PSYCHOLOGY EXAM REVIEW SHEETDocument6 pagesAP PSYCHOLOGY EXAM REVIEW SHEETNathan HudsonNo ratings yet
- 16th Week of Pregnancy: Tips for Safe Travel While ExpectingDocument4 pages16th Week of Pregnancy: Tips for Safe Travel While ExpectingNaveenbabu SoundararajanNo ratings yet
- He History of ArticulatorsDocument13 pagesHe History of ArticulatorsrekabiNo ratings yet
- Head to Toe Physical Assessment GuideDocument16 pagesHead to Toe Physical Assessment Guideabagatsing100% (5)
- Zoology: Zoology Previous Eamcet QuestionsDocument8 pagesZoology: Zoology Previous Eamcet QuestionsGaganpreetSingh100% (1)
- Biology: Revised Syllabus For Higher Secondary First Year CourseDocument4 pagesBiology: Revised Syllabus For Higher Secondary First Year CourseamitumikoibNo ratings yet
- The Relativistic Brain by Ronald Cicurel and Miguel L. Nicolelis (2015)Document5 pagesThe Relativistic Brain by Ronald Cicurel and Miguel L. Nicolelis (2015)Sinem SerapNo ratings yet
- DLL - Science 6 - Q2Document7 pagesDLL - Science 6 - Q2Angelica GuillermoNo ratings yet
- The Normal Anterior Inferior Cerebellar ArteryDocument19 pagesThe Normal Anterior Inferior Cerebellar Artery16fernandoNo ratings yet
- Chronobiology and Anesthesia: Review ArticleDocument15 pagesChronobiology and Anesthesia: Review ArticleGabriela Lizbeth ArmentaNo ratings yet
- 2016 - 13 - Fleming - Lagged Syndesmotic Fixation - Our Clinical ExperienceDocument8 pages2016 - 13 - Fleming - Lagged Syndesmotic Fixation - Our Clinical ExperienceJacob DoughertyNo ratings yet