You might also like
- Provisional Splinting 2013Document87 pagesProvisional Splinting 2013felicedaNo ratings yet
- Orthodontics: Myofunctional AppliancesDocument10 pagesOrthodontics: Myofunctional AppliancesSaif HashimNo ratings yet
- Comparison of Anterior Retraction and Anchorage Control BetweenDocument44 pagesComparison of Anterior Retraction and Anchorage Control BetweenAnushriya DuttaNo ratings yet
- Case Report - Complete Denture - 2Document4 pagesCase Report - Complete Denture - 2Astri Ggamjong Xiao LuNo ratings yet
- Magnetic Twin BlockDocument28 pagesMagnetic Twin BlockSwapnil MangwadeNo ratings yet
- Space Regainers in Pediatric DentistryDocument6 pagesSpace Regainers in Pediatric DentistryFayiz SäbNo ratings yet
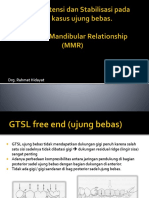
- Dok Rahmat Desain, Retensi N Stabilisasi GTSL Free End N MMRDocument53 pagesDok Rahmat Desain, Retensi N Stabilisasi GTSL Free End N MMRAditya ZulfikarNo ratings yet
- Prosthodontic DiagnosisDocument15 pagesProsthodontic DiagnosisYashpreetsingh Bhatia100% (1)
- Multiloop Edgewise Archwire in The Treatment of A Patient With An Anterior Open Bite and A Long FaceDocument7 pagesMultiloop Edgewise Archwire in The Treatment of A Patient With An Anterior Open Bite and A Long FaceKanchit SuwanswadNo ratings yet
- Review Correlation Between Diabetes Mellitus and Residual Ridge Resorption PDFDocument3 pagesReview Correlation Between Diabetes Mellitus and Residual Ridge Resorption PDFInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Majalah IKORTI Desember 2015 PDFDocument56 pagesMajalah IKORTI Desember 2015 PDFAbdi utomoNo ratings yet
- Systematic Review of Selective GrindingDocument6 pagesSystematic Review of Selective GrindingNiranjanaNo ratings yet
- Vto Ricketts Vs HoldawayDocument80 pagesVto Ricketts Vs HoldawayhenryNo ratings yet
- Predictable Diastema Closure Using An Innovative Indirect Mock Up TechniqueDocument4 pagesPredictable Diastema Closure Using An Innovative Indirect Mock Up TechniqueJane JaneeNo ratings yet
- Comparative Evaluation of The Mechanical Properties of Three Commercially Available Flexible Denture Base Materials - An in Vitro StudyDocument132 pagesComparative Evaluation of The Mechanical Properties of Three Commercially Available Flexible Denture Base Materials - An in Vitro StudySkAliHassanNo ratings yet
- Introduction To Dental Implantology: Dr. Nigam Sattar KhanDocument49 pagesIntroduction To Dental Implantology: Dr. Nigam Sattar KhanNigam SattarNo ratings yet
- Space RegainerDocument7 pagesSpace RegainerdelfNo ratings yet
- 7 Indirect RetainerDocument16 pages7 Indirect RetainerArun ThathiNo ratings yet
- BionatorDocument10 pagesBionatorDiana DennisNo ratings yet
- Eccentric RelationDocument10 pagesEccentric RelationKiana TediNo ratings yet
- Immediate DentureDocument52 pagesImmediate Denturedkdinesh020No ratings yet
- Bedah Buku Prosto FixDocument22 pagesBedah Buku Prosto FixLeliNo ratings yet
- Finger-Spring (Single Cantilever) : Ms. Nimrah Razzque MemonDocument8 pagesFinger-Spring (Single Cantilever) : Ms. Nimrah Razzque MemonNimrah Razzaque MemonNo ratings yet
- Lec - 2 - Z, Double Z, T SpringDocument4 pagesLec - 2 - Z, Double Z, T SpringRebin Ali100% (1)
- Philosophy of Orthodontic 1Document54 pagesPhilosophy of Orthodontic 1debbyaprilia12No ratings yet
- Role of Bone Screw (Izc & BSS) in Skeletal Anchorage System - A Review ArticleDocument5 pagesRole of Bone Screw (Izc & BSS) in Skeletal Anchorage System - A Review ArticleAlvaro ChacónNo ratings yet
- Bimaxillary Protrusion - A Case ReportDocument4 pagesBimaxillary Protrusion - A Case ReportLisbethNo ratings yet
- Anterior GuidanceDocument122 pagesAnterior Guidancementacity100% (1)
- Modified Bluegrass Appliance PDFDocument4 pagesModified Bluegrass Appliance PDFRenieKumalaNo ratings yet
- Development of Dental OcclusionDocument89 pagesDevelopment of Dental OcclusionMothi KrishnaNo ratings yet
- Activatoranditsmodifications 120531102843 Phpapp02Document91 pagesActivatoranditsmodifications 120531102843 Phpapp02CarlosAndresPabonCortesNo ratings yet
- Canine Impaction-A Review of The Prevalence, Etiology, Diagnosis and TreatmentDocument26 pagesCanine Impaction-A Review of The Prevalence, Etiology, Diagnosis and TreatmentAnil MarnaNo ratings yet
- Bilateral First Premolar Scissor Bite Correction Using Cross Arch Elastics: A Case ReportDocument4 pagesBilateral First Premolar Scissor Bite Correction Using Cross Arch Elastics: A Case ReportYousif AbdullaNo ratings yet
- SSCDocument10 pagesSSCYanuar MegaNo ratings yet
- Adhesive BridgesDocument9 pagesAdhesive BridgesShilpa ShrivastavaNo ratings yet
- DriftodonticsDocument2 pagesDriftodonticssweetieNo ratings yet
- The Monoplane Occlusion For Complete Dentures: T H e SP Herical TheoryDocument7 pagesThe Monoplane Occlusion For Complete Dentures: T H e SP Herical TheorySahana RangarajanNo ratings yet
- A Comparison Between Arbitrary and KinematicDocument4 pagesA Comparison Between Arbitrary and KinematicsmritinarayanNo ratings yet
- Stem Cells - A Ray of Hope in OrthodonticsDocument3 pagesStem Cells - A Ray of Hope in OrthodonticsInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- Alternate Technique For Fabrication of A Custom Impression Tray For Definitive Obturator ConstructionDocument3 pagesAlternate Technique For Fabrication of A Custom Impression Tray For Definitive Obturator ConstructionRaven Roth100% (1)
- Occlusal SplintsDocument25 pagesOcclusal SplintsSalim MalikNo ratings yet
- A Modified Bluegrass Appliance For Interception of Tongue Thrust Habit - A Clinical InnovatiDocument3 pagesA Modified Bluegrass Appliance For Interception of Tongue Thrust Habit - A Clinical InnovatiAdvanced Research PublicationsNo ratings yet
- Art of Debonding in OrthodonticsDocument2 pagesArt of Debonding in OrthodonticsmalifaragNo ratings yet
- Periodontics: Treatment Planning For Patients With Periodontal DiseasesDocument17 pagesPeriodontics: Treatment Planning For Patients With Periodontal Diseasesفاطمة فالح ضايف مزعلNo ratings yet
- Orthodontics 2 Lec M1 M2Document18 pagesOrthodontics 2 Lec M1 M2bambam1aNo ratings yet
- Functional OcclusionDocument8 pagesFunctional OcclusionNoor SolikhahNo ratings yet
- Begg1977 PDFDocument39 pagesBegg1977 PDFKhyati GuptaNo ratings yet
- Clinical Management of The MARADocument59 pagesClinical Management of The MARAShannon Victor Peter100% (1)
- Importance of 1st Permanent MolarDocument28 pagesImportance of 1st Permanent MolarAdyasha SahuNo ratings yet
- ActivatorDocument1 pageActivatorMuhammad DaltonNo ratings yet
- Soldering in RPDDocument4 pagesSoldering in RPDPraveen KumarNo ratings yet
- 1 FrameDentureDocument8 pages1 FrameDentureJennieNo ratings yet
- Fixed Orthodontic Appliances: A Practical GuideFrom EverandFixed Orthodontic Appliances: A Practical GuideRating: 1 out of 5 stars1/5 (1)
- Oral Wound Healing: Cell Biology and Clinical ManagementFrom EverandOral Wound Healing: Cell Biology and Clinical ManagementHannu LarjavaNo ratings yet
- Occlusal Adjustment Technique Made Simple: Masticatory System and Occlusion As It Relates to Function and How Occlusal Adjustment Can Help Treat Primary and Secondary Occlusal TraumaFrom EverandOcclusal Adjustment Technique Made Simple: Masticatory System and Occlusion As It Relates to Function and How Occlusal Adjustment Can Help Treat Primary and Secondary Occlusal TraumaNo ratings yet
- Understanding Masticatory Function in Unilateral CrossbitesFrom EverandUnderstanding Masticatory Function in Unilateral CrossbitesNo ratings yet
- 04 WongDocument10 pages04 WongNam BuiNo ratings yet
- PendulumDocument8 pagesPendulumNam BuiNo ratings yet
- Face BowDocument2 pagesFace BowNam BuiNo ratings yet
- Articulator (Mobile and Smart)Document4 pagesArticulator (Mobile and Smart)Nam BuiNo ratings yet
- Eur J Orthod 1998 Celar 579 87Document167 pagesEur J Orthod 1998 Celar 579 87Nam BuiNo ratings yet
- Analisis Tridimensional Meaw2004Document9 pagesAnalisis Tridimensional Meaw2004Abad SalcedoNo ratings yet
- Functional OcclusionDocument186 pagesFunctional OcclusionNam Bui100% (1)
- Occlusion of TermDocument44 pagesOcclusion of TermNam BuiNo ratings yet
- Simon Lip Surgery AACDDocument7 pagesSimon Lip Surgery AACDdrzana78No ratings yet
- Ijoi Vol 32Document132 pagesIjoi Vol 32Chin-lungHsieh100% (2)
- 3.good Occlusal Practice in Simple Restorative Dentistry PDFDocument13 pages3.good Occlusal Practice in Simple Restorative Dentistry PDFaleeza sanaNo ratings yet
- Asia 1Document94 pagesAsia 1Nam BuiNo ratings yet
- C&B 12 RBBDocument89 pagesC&B 12 RBBNam BuiNo ratings yet
- Causes of Anterior WearDocument3 pagesCauses of Anterior WearNam BuiNo ratings yet
- C&B 7 Anterior PVCDocument12 pagesC&B 7 Anterior PVCNam BuiNo ratings yet
- Increasing Vertical DimensionDocument6 pagesIncreasing Vertical DimensionAriel AcevedoNo ratings yet
- 02 D003 44769Document17 pages02 D003 44769Nam BuiNo ratings yet
- C&B 11 ImpressionDocument24 pagesC&B 11 ImpressionNam BuiNo ratings yet
- Occlusion of TermDocument44 pagesOcclusion of TermNam BuiNo ratings yet
- Icmr Specimen Referral Form For Covid-19 (Sars-Cov2) : Nic - (Https://Covid19Cc - Nic.In) Page 1/18 27-04-2021 13:49:04Document18 pagesIcmr Specimen Referral Form For Covid-19 (Sars-Cov2) : Nic - (Https://Covid19Cc - Nic.In) Page 1/18 27-04-2021 13:49:04Sumit PatelNo ratings yet
- Health Lesson Plan-BandagesDocument8 pagesHealth Lesson Plan-BandagesJaybee MacadangdangNo ratings yet
- Spinal SurgeryDocument19 pagesSpinal SurgerySalomeSibashviliNo ratings yet
- Ficha Tecnica ANTIGENO 120006841 v3 Panbio COVID-19 Ag Nasopharyngeal IFU BoDocument132 pagesFicha Tecnica ANTIGENO 120006841 v3 Panbio COVID-19 Ag Nasopharyngeal IFU BoYessica Marisol Custodio ReinosoNo ratings yet
- Interstitial Lung Diseases Radiology 22222Document26 pagesInterstitial Lung Diseases Radiology 22222Daniel AshooriNo ratings yet
- Antenatal CareDocument13 pagesAntenatal CareOjambo Flavia50% (2)
- Clinical EnzymologyDocument23 pagesClinical EnzymologyKishore KaranNo ratings yet
- Hema - Guide Notes PDFDocument21 pagesHema - Guide Notes PDFVanessa Ladra100% (1)
- Hematology Unit: Complete Blood Count (CBC)Document2 pagesHematology Unit: Complete Blood Count (CBC)Rasha ElbannaNo ratings yet
- ICON 2016 Febrile Neutropenia GuidelinesDocument34 pagesICON 2016 Febrile Neutropenia GuidelinesTor Ja100% (1)
- Which Hard Tissue Augmentation Techniques Are The Most Succesful in Furnishing Bony Support For Implant PlacementDocument25 pagesWhich Hard Tissue Augmentation Techniques Are The Most Succesful in Furnishing Bony Support For Implant PlacementJuan Andres CastilloNo ratings yet
- Course in The WardDocument7 pagesCourse in The WardDanicaEdonFelarcaNo ratings yet
- Paper PE Rabies Bali - Chaerul BasriDocument14 pagesPaper PE Rabies Bali - Chaerul BasriAulia Miftakhur RahmanNo ratings yet
- Anti Diare SGDocument17 pagesAnti Diare SGludoy03No ratings yet
- Konsep Wound ManajemenDocument24 pagesKonsep Wound ManajemenNiken DewiNo ratings yet
- Medicago Sativa LloydDocument4 pagesMedicago Sativa LloydDr Rushen SinghNo ratings yet
- Pedia ADCONDocument24 pagesPedia ADCONRaul MangrobangNo ratings yet
- General AnaestheticsDocument71 pagesGeneral AnaestheticsTamilarasanNo ratings yet
- DM 2021-0114 Guidelines On The MGMT and Admin of The Initial 600,000 Donated SARS-CoV-2 Vaccine (Vero Cell) Inactivated Coronavac (Sinovac) DosesDocument17 pagesDM 2021-0114 Guidelines On The MGMT and Admin of The Initial 600,000 Donated SARS-CoV-2 Vaccine (Vero Cell) Inactivated Coronavac (Sinovac) DosesRalph Julius MendozaNo ratings yet
- 32 Oet Reading Summary 2.0-697-717Document21 pages32 Oet Reading Summary 2.0-697-717Santhus100% (7)
- Penatalaksanaan CAPDocument31 pagesPenatalaksanaan CAPridhoNo ratings yet
- Shared Psychotic Disorder - NCBIDocument8 pagesShared Psychotic Disorder - NCBI5KevNo ratings yet
- Acute Complications of Diabetes Mellitus: Hypoglycemia and Hypoglycemic ComaDocument30 pagesAcute Complications of Diabetes Mellitus: Hypoglycemia and Hypoglycemic ComaCristinaGheorgheNo ratings yet
- Hepatitis D Virus (HDV) : PathogenesisDocument30 pagesHepatitis D Virus (HDV) : PathogenesisJc GaldosNo ratings yet
- Aace - Ace - 2016 - Comprehensive Clinical Practice Guidelines For Medical Care of Patients With ObesityDocument203 pagesAace - Ace - 2016 - Comprehensive Clinical Practice Guidelines For Medical Care of Patients With ObesityLintang AdhiNo ratings yet
- Khushboo PPT Covid 19Document17 pagesKhushboo PPT Covid 19Birlal SinghNo ratings yet
- Antenatal Care Services: by DR - Chinedu Ibeh Thursday, 16 APRIL 2015Document81 pagesAntenatal Care Services: by DR - Chinedu Ibeh Thursday, 16 APRIL 2015SehaRizaNo ratings yet
- UNIT-I: General Pharmacology As Per Syllabus Unit-1, Chapter A (Half)Document18 pagesUNIT-I: General Pharmacology As Per Syllabus Unit-1, Chapter A (Half)Atthapu ThirupathaiahNo ratings yet
- Jcih 2007Document29 pagesJcih 2007Ankur BanerjeeNo ratings yet
- Perineal Techniques During The Second Stage of Labour For Reducing Perineal Trauma (Review)Document118 pagesPerineal Techniques During The Second Stage of Labour For Reducing Perineal Trauma (Review)Ppds ObgynNo ratings yet