You might also like
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Wireless Ecg Monitoring System For The Detection of Cardiac ArrhythmiaDocument14 pagesWireless Ecg Monitoring System For The Detection of Cardiac ArrhythmiaSree Rag KNo ratings yet
- APC Cardio Catalina-1Document21 pagesAPC Cardio Catalina-1Carmelo ScavoneNo ratings yet
- ECG Viewer Manager - Prince 180D, PC-80D User Manual V1.8Document35 pagesECG Viewer Manager - Prince 180D, PC-80D User Manual V1.8Brian JonesNo ratings yet
- Cardiomera: Better Care Improving HealthDocument2 pagesCardiomera: Better Care Improving HealthHusti AdrianNo ratings yet
- The HeartDocument58 pagesThe HeartJULIUS NAKANYALANo ratings yet
- Heart Electr Act-120830-StudentDocument10 pagesHeart Electr Act-120830-Studentapi-400575655No ratings yet
- Ecg - AclsDocument338 pagesEcg - AclsPete Cobra CobraitiNo ratings yet
- Ecg en LabviewDocument61 pagesEcg en LabviewHarold David Gil MuñozNo ratings yet
- Monitoring Solutions B125 v1 Spec Sheet - DOC1937971 - Rev3 - Apr6Document5 pagesMonitoring Solutions B125 v1 Spec Sheet - DOC1937971 - Rev3 - Apr6malakmounirNo ratings yet
- Ekg MorphologyDocument1 pageEkg MorphologyTeresa MartinsNo ratings yet
- NURS 6512N 53 Advanced Health Assessment.2020 FINAL EXAMDocument17 pagesNURS 6512N 53 Advanced Health Assessment.2020 FINAL EXAMerick kanyiNo ratings yet
- Management of Patients With Dysrhythmias and Conduction Problems DysrhythmiasDocument15 pagesManagement of Patients With Dysrhythmias and Conduction Problems DysrhythmiasRoyce Vincent TizonNo ratings yet
- 14 - EKG-kegawatanDocument63 pages14 - EKG-kegawatanIka HayaturrohmahNo ratings yet
- Test Taking StratDocument24 pagesTest Taking Stratpaulzilicous.artNo ratings yet
- Syllabus Group - C & DDocument87 pagesSyllabus Group - C & DAnupam DhawaleNo ratings yet
- ZQ-1203G DatasheetDocument1 pageZQ-1203G DatasheetkrsrinivasarajuNo ratings yet
- Myocardial InfarctionDocument18 pagesMyocardial InfarctionMarc Lorenz DucusinNo ratings yet
- الوحدة الثانيهDocument7 pagesالوحدة الثانيهHUAWEI HUAWEINo ratings yet
- Tndlive Medicine1Document45 pagesTndlive Medicine1Madhu SowmithaNo ratings yet
- ECG InterpretationDocument6 pagesECG InterpretationANDREW DEL ROSARIONo ratings yet
- COMEN - Veterinary CatalogDocument4 pagesCOMEN - Veterinary CatalogSurta DevianaNo ratings yet
- ECG and ArrhythmiasDocument25 pagesECG and ArrhythmiasRashed ShatnawiNo ratings yet
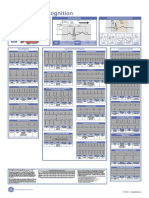
- Poster1 Arrhythmia Recognition e PDFDocument1 pagePoster1 Arrhythmia Recognition e PDFMiko RamosoNo ratings yet
- Heart BlocksDocument6 pagesHeart BlocksMark Hammerschmidt100% (1)
- Life Window LW 6000Document73 pagesLife Window LW 6000Mossad MinayaNo ratings yet
- Desfibrilador Cadio Aid200 Sanro enDocument1 pageDesfibrilador Cadio Aid200 Sanro enPablo TaboadaNo ratings yet
- Design and Development of A Heart Rate Measuring Device Using FingertipDocument6 pagesDesign and Development of A Heart Rate Measuring Device Using FingertipKazandra Cassidy GarciaNo ratings yet
- Cardio NclexDocument40 pagesCardio NclexGabrielle WashingtonNo ratings yet
- An Online ECG QRS Detection TechniqueDocument6 pagesAn Online ECG QRS Detection TechniqueIDESNo ratings yet
- BibliographyDocument4 pagesBibliographynikskool5No ratings yet