You might also like
- Tsalikakis Growth Search & IGFDocument8 pagesTsalikakis Growth Search & IGFtsalikakisNo ratings yet
- Tsalikakis - Kolletis - European Journal of PharmacologyDocument9 pagesTsalikakis - Kolletis - European Journal of PharmacologytsalikakisNo ratings yet
- Tsalikakis Clinical ScienceDocument7 pagesTsalikakis Clinical SciencetsalikakisNo ratings yet
- Tsalikakis Cardiovascular ResearchDocument8 pagesTsalikakis Cardiovascular ResearchtsalikakisNo ratings yet
- Tsalikakis - Ieee Trans Biom EngDocument5 pagesTsalikakis - Ieee Trans Biom EngtsalikakisNo ratings yet
- Tsalikakis - Computers in Med and BiologyDocument13 pagesTsalikakis - Computers in Med and BiologytsalikakisNo ratings yet
- Gholizade Narm 2009 Bio Medical Signal Processing and ControlDocument10 pagesGholizade Narm 2009 Bio Medical Signal Processing and ControltsalikakisNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Astm-e855 Изгиб МеталлаDocument8 pagesAstm-e855 Изгиб МеталлаАлесь БуяковNo ratings yet
- VDVDVXVCFDBCVCDocument390 pagesVDVDVXVCFDBCVCHafiz Rahmat UllahNo ratings yet
- Land Based SensorsDocument40 pagesLand Based SensorsJ.MichaelLooneyNo ratings yet
- FFA Furfural Fire and Health HazardsDocument2 pagesFFA Furfural Fire and Health HazardsYuga Pria PungkasanNo ratings yet
- A Steganography Intrusion Detection SystemDocument21 pagesA Steganography Intrusion Detection SystemjamessomNo ratings yet
- Periodization: Effects of Manipulating Volume and Intensity. Part 2Document7 pagesPeriodization: Effects of Manipulating Volume and Intensity. Part 2nachox_99No ratings yet
- PSE YRC1000micro 00Document25 pagesPSE YRC1000micro 00LiemNo ratings yet
- Preparation Exam API 510:N°01 QuestionsDocument3 pagesPreparation Exam API 510:N°01 QuestionskorichiNo ratings yet
- Data Assigment 1Document32 pagesData Assigment 1Sukhwinder Kaur100% (1)
- GPT 7000L User: Manual'Document26 pagesGPT 7000L User: Manual'Adel Abo AdamNo ratings yet
- Bandura Et Al.Document16 pagesBandura Et Al.Siddhant JhawarNo ratings yet
- Electric Charges and Fields All DerivationsDocument9 pagesElectric Charges and Fields All DerivationsFlame kaiserNo ratings yet
- (Advanced Techniques For 4G Systems) : Name: Alaa Ashraf Abdelmoneim Elagrody Sec: 1 ID:1Document11 pages(Advanced Techniques For 4G Systems) : Name: Alaa Ashraf Abdelmoneim Elagrody Sec: 1 ID:1alaa elagrodiNo ratings yet
- Hkts 210 Sub/Hkts 200 Sub: SubwooferDocument6 pagesHkts 210 Sub/Hkts 200 Sub: SubwooferDan PopNo ratings yet
- Structural Geology From Barmer Basin (India)Document12 pagesStructural Geology From Barmer Basin (India)Sankhajit SahaNo ratings yet
- Academic Performance of Face-to-Face and Online Students in An Introductory Economics Course and Determinants of Final Course GradesDocument13 pagesAcademic Performance of Face-to-Face and Online Students in An Introductory Economics Course and Determinants of Final Course GradesLou BaldomarNo ratings yet
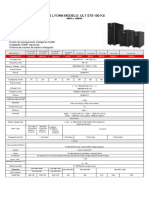
- Ups Lyonn Modelo: Ult St5-100 KS: 10KVA A 120KVADocument1 pageUps Lyonn Modelo: Ult St5-100 KS: 10KVA A 120KVASebastian Matias CruzNo ratings yet
- Hitachi ZW550Document12 pagesHitachi ZW550ForomaquinasNo ratings yet
- SE Unit - 1Document30 pagesSE Unit - 1Sanketh KanuguNo ratings yet
- HP LaserJet 5P - 6P Service Manual (Proper)Document116 pagesHP LaserJet 5P - 6P Service Manual (Proper)maroudasp100% (1)
- Triac BT137-600DDocument6 pagesTriac BT137-600DEverton AlvesNo ratings yet
- Pages 296-298 Module 6 ReviewDocument4 pagesPages 296-298 Module 6 Reviewapi-332361871No ratings yet
- Huawei Site Design GuidelineDocument7 pagesHuawei Site Design GuidelineHeru BudiantoNo ratings yet
- 20-SDMS-02 Overhead Line Accessories PDFDocument102 pages20-SDMS-02 Overhead Line Accessories PDFMehdi SalahNo ratings yet
- 19Ma2Icmat Module 5 - Elementary Numerical MethodsDocument4 pages19Ma2Icmat Module 5 - Elementary Numerical Methods1DS19CH011 Jashwanth C RNo ratings yet
- Unitplan2 Chi-SquareDocument11 pagesUnitplan2 Chi-Squareapi-285549920No ratings yet
- Sterlization of Water Using Bleaching Powder PDFDocument20 pagesSterlization of Water Using Bleaching Powder PDFradha krishnanNo ratings yet
- (Advances in Cryogenic Engineering 37) Takayuki Kishi, Mizuo Kudo, Hiromasa Iisaka (Auth.), R. W. Fast (Eds.) - Advances in Cryogenic Engineering-Springer US (1991)Document729 pages(Advances in Cryogenic Engineering 37) Takayuki Kishi, Mizuo Kudo, Hiromasa Iisaka (Auth.), R. W. Fast (Eds.) - Advances in Cryogenic Engineering-Springer US (1991)ksvvijNo ratings yet
- KUKA Sim 30 Installation enDocument49 pagesKUKA Sim 30 Installation enRégis Naydo0% (1)