You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- 111Document10 pages111Phước Ng50% (2)
- Presentation On Drowsiness Detection SystemDocument11 pagesPresentation On Drowsiness Detection Systemmovies downloaderNo ratings yet
- BIBLIOMETRICDocument30 pagesBIBLIOMETRICkalaranishanmuganathNo ratings yet
- Individual Spirituality, Workplace Spirituality and Work Attitudes An Empirical Test of Direct and Interaction EffectsDocument19 pagesIndividual Spirituality, Workplace Spirituality and Work Attitudes An Empirical Test of Direct and Interaction EffectsBasharat NaeemNo ratings yet
- Beration of LightDocument7 pagesBeration of LightAnonymous i71HvPXNo ratings yet
- Plate Fin Heat ExchangerDocument14 pagesPlate Fin Heat ExchangerTushar PanchalNo ratings yet
- Deductive ReasoningDocument2 pagesDeductive ReasoningMariel C. BombitaNo ratings yet
- Lab ReportDocument5 pagesLab Reportivan glenn baldomerostNo ratings yet
- TM 9 1276 Carbines Cal 30 M1 M1A1 M2 and M3 1947Document111 pagesTM 9 1276 Carbines Cal 30 M1 M1A1 M2 and M3 1947hammonje100% (3)
- Shared Memory ArchitectureDocument2 pagesShared Memory ArchitectureNeethu RajeshNo ratings yet
- The Whys and Wherefores of Microphone Array Crosstalk in Multichannel Microphone Array DesignDocument6 pagesThe Whys and Wherefores of Microphone Array Crosstalk in Multichannel Microphone Array DesignmewarulesNo ratings yet
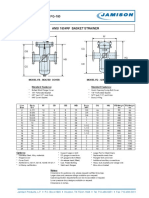
- FB-150 FQ-150 Basket StrainerDocument1 pageFB-150 FQ-150 Basket Strainerklich77No ratings yet
- Mha Mca Cet SyllabusDocument20 pagesMha Mca Cet Syllabusm kumarNo ratings yet
- Caie As Computer Science 9618 Theory v3Document20 pagesCaie As Computer Science 9618 Theory v3James HoangNo ratings yet
- Measurement of Earthing Systems: Central Networks Earthing Manual Section E4Document45 pagesMeasurement of Earthing Systems: Central Networks Earthing Manual Section E4ahmed_k7117No ratings yet
- Mitchell-Banki Turbine Design Document PDFDocument37 pagesMitchell-Banki Turbine Design Document PDFprojetosschillingNo ratings yet
- Unit 2 MCB Key PDFDocument19 pagesUnit 2 MCB Key PDFDafne Fertig88% (32)
- QE and Complex Numbers DPPDocument9 pagesQE and Complex Numbers DPPsatishmhbdNo ratings yet
- Thermodynamics NotesDocument2 pagesThermodynamics Notesjpu_48No ratings yet
- Temporal BroadeningDocument10 pagesTemporal BroadeningMohamed BouhaddaNo ratings yet
- TFT SDK ManualDocument107 pagesTFT SDK ManualRenier ServenNo ratings yet
- 7 - Introduction To Intelligent ControlDocument21 pages7 - Introduction To Intelligent ControlIsmael Espinoza100% (1)
- Squall (Better) Training Manual: ModelsDocument83 pagesSquall (Better) Training Manual: ModelsSilomo-saka MambaNo ratings yet
- GENERAL PHYSICS 2 - Q3 - Week 2Document22 pagesGENERAL PHYSICS 2 - Q3 - Week 2vrejie46No ratings yet
- ITTC Surface TreatmentDocument63 pagesITTC Surface Treatments_brizzolaraNo ratings yet
- Stacks - Quesues and DequesDocument23 pagesStacks - Quesues and DequesAbdallateef ShohdyNo ratings yet
- USN 18CS654: B. E. Degree (Autonomous) Sixth Semester End Examination (SEE)Document2 pagesUSN 18CS654: B. E. Degree (Autonomous) Sixth Semester End Examination (SEE)Sarmi HarshaNo ratings yet
- Clipping Clamping CircuitsDocument7 pagesClipping Clamping CircuitsPavan SaiNo ratings yet
- Nut & Bolt ScienceDocument3 pagesNut & Bolt SciencetanujaayerNo ratings yet
- Science 3 PDFDocument12 pagesScience 3 PDFJelyn CandoNo ratings yet