You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Question and Answers For MFD OSCE ExaminationDocument15 pagesQuestion and Answers For MFD OSCE ExaminationAmeer Fadel100% (1)
- Case Study On MalariaDocument18 pagesCase Study On MalariaBie WeNna100% (4)
- Myofascial Trigger PointsDocument17 pagesMyofascial Trigger PointsVera Belchior100% (3)
- Foods and Purine ContentsDocument7 pagesFoods and Purine ContentsIndah ApsariNo ratings yet
- Ozomed BrochureDocument4 pagesOzomed BrochurechirakiNo ratings yet
- Pharmaceutical CareDocument114 pagesPharmaceutical CareRisdaFitriaNo ratings yet
- Tomatoes and Tomato Products - Nutritional, Medicinal and Therapeutic PropertiesDocument664 pagesTomatoes and Tomato Products - Nutritional, Medicinal and Therapeutic PropertiesAndreea MerţNo ratings yet
- How Food Affects The Mind, As Well As The Body - The EconomistDocument11 pagesHow Food Affects The Mind, As Well As The Body - The Economistgermany23No ratings yet
- One Belief Worksheet Byron KatieDocument2 pagesOne Belief Worksheet Byron Katiegermany23No ratings yet
- Linus Pauling and Vitamin C - Harvard ThesisDocument64 pagesLinus Pauling and Vitamin C - Harvard ThesisBurt HamnerNo ratings yet
- Table KOVACS 8 Stage ServeDocument1 pageTable KOVACS 8 Stage Servegermany23No ratings yet
- Hip Internal Rotation - Stretches and Exercises To Improve MobilitDocument2 pagesHip Internal Rotation - Stretches and Exercises To Improve Mobilitgermany23No ratings yet
- Load Overload and Recovery in Athlete (2019)Document8 pagesLoad Overload and Recovery in Athlete (2019)Ruben CapelaNo ratings yet
- Vitamin C Treatment For COVIDDocument4 pagesVitamin C Treatment For COVIDgermany23No ratings yet
- Using The Overhead Squat For Core DevelopmentDocument3 pagesUsing The Overhead Squat For Core Developmentgermany23No ratings yet
- Tucker - Unelected PowerDocument5 pagesTucker - Unelected Powergermany23No ratings yet
- Harvard BR To Succeed in A Negotiation, Help Your Counterpart Save FaceDocument3 pagesHarvard BR To Succeed in A Negotiation, Help Your Counterpart Save Facegermany23No ratings yet
- Building The Spanish Forehand in TennisDocument7 pagesBuilding The Spanish Forehand in Tennisgermany23No ratings yet
- Emilio Sanchez Vicario - WCC2019 Tennis Drills For Direction and HeightDocument10 pagesEmilio Sanchez Vicario - WCC2019 Tennis Drills For Direction and Heightgermany23No ratings yet
- Jaramillo Periodization Tennis PlanDocument10 pagesJaramillo Periodization Tennis Plangermany23No ratings yet
- Using The Overhead Squat For Core DevelopmentDocument3 pagesUsing The Overhead Squat For Core Developmentgermany23No ratings yet
- Effect of Scapular Stabilization ExercisesDocument5 pagesEffect of Scapular Stabilization Exercisesgermany23No ratings yet
- It F Junior Circuit RegulationsDocument15 pagesIt F Junior Circuit RegulationscandhareNo ratings yet
- Good and Bad Serve PositionsDocument3 pagesGood and Bad Serve Positionsgermany23No ratings yet
- Free Your Neck by Carol KrucoffDocument8 pagesFree Your Neck by Carol Krucoffgermany23No ratings yet
- A Kinetic Chain Approach For Shoulder Rehab MCMULLEN PDFDocument9 pagesA Kinetic Chain Approach For Shoulder Rehab MCMULLEN PDFgermany23No ratings yet
- Original Plum Torte of The NEW YORK TImesDocument2 pagesOriginal Plum Torte of The NEW YORK TImesgermany23100% (1)
- Kovacs 8 Stages of ServeDocument10 pagesKovacs 8 Stages of Servegermany23No ratings yet
- ITF Tennis Science Review. Tennis Log Anxiety Etc - 113912Document19 pagesITF Tennis Science Review. Tennis Log Anxiety Etc - 113912germany23100% (1)
- Biology and Mechanisms of Action of The Vitamin D Hormone Nihms910020Document35 pagesBiology and Mechanisms of Action of The Vitamin D Hormone Nihms910020germany23No ratings yet
- Shoulder Injuries in The Overhead Athlete, WILK Et AL, Jospt.2009.2929Document17 pagesShoulder Injuries in The Overhead Athlete, WILK Et AL, Jospt.2009.2929germany23No ratings yet
- PainScience - Does Epsom Salt WorkDocument29 pagesPainScience - Does Epsom Salt Workgermany23No ratings yet
- Large Massive Rotator Cuff Repair - RehabDocument4 pagesLarge Massive Rotator Cuff Repair - Rehabgermany23No ratings yet
- Mucuna and Parkinson's Disease Natural Levodopa PDFDocument22 pagesMucuna and Parkinson's Disease Natural Levodopa PDFgermany23100% (1)
- Integrating Shoulder and Core Exercises When Rehabilitating AthletesDocument9 pagesIntegrating Shoulder and Core Exercises When Rehabilitating Athletesgermany23No ratings yet
- MGH Interval Tennis ProgramDocument1 pageMGH Interval Tennis Programgermany23No ratings yet
- Curcumin Restores Mitochondrial Functions 2014 40659 - 2014 - Article - 61Document8 pagesCurcumin Restores Mitochondrial Functions 2014 40659 - 2014 - Article - 61germany23No ratings yet
- ENERPEEL SA - Rev - 0 - 2011Document48 pagesENERPEEL SA - Rev - 0 - 2011CHONG WEI SHENGNo ratings yet
- US Army Medical Pharmacology IDocument202 pagesUS Army Medical Pharmacology ISpace_Hulker100% (2)
- DAX2018790204 SpainDocument64 pagesDAX2018790204 SpainHarsh BhattNo ratings yet
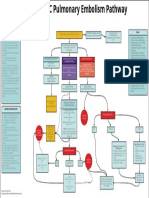
- EMCrit Lae Pulmonary FlowDocument1 pageEMCrit Lae Pulmonary FlowhmsptrNo ratings yet
- Paper - B Written Test Paper For Selection of Teachers: CSB 2013 English (PGT) : Subject Code: P11Document4 pagesPaper - B Written Test Paper For Selection of Teachers: CSB 2013 English (PGT) : Subject Code: P11Amrit SinhaNo ratings yet
- Dosage Chapter 1 PDFDocument4 pagesDosage Chapter 1 PDFLena EmataNo ratings yet
- A Review Paper On Scope of Big Data Analysis in Heath INFORMATICSDocument8 pagesA Review Paper On Scope of Big Data Analysis in Heath INFORMATICSMohamed Aly SowNo ratings yet
- Ashtanga Yoga I and II Complete OCR (Finereader - IsTA SettingsDocument192 pagesAshtanga Yoga I and II Complete OCR (Finereader - IsTA SettingsAndreea Bertea0% (1)
- Elisa PPT Nitub 2019Document57 pagesElisa PPT Nitub 2019Nabila Bahar100% (1)
- Biochemistry of Jaundice 03Document52 pagesBiochemistry of Jaundice 03Cathleen May Dela Cruz50% (2)
- TPNDocument69 pagesTPNMylz MendozaNo ratings yet
- The Importance of Mineral Elements For Humans, Domestic Animals and Plants: A ReviewDocument3 pagesThe Importance of Mineral Elements For Humans, Domestic Animals and Plants: A ReviewMaricel Canlas MacatoNo ratings yet
- Effect of Dragon Fruit On Lipid ProfileDocument2 pagesEffect of Dragon Fruit On Lipid ProfileElindah Ayunin ArrumNo ratings yet
- TOI AhmadabadDocument24 pagesTOI AhmadabadJugarNo ratings yet
- WBC CountingDocument4 pagesWBC CountingMarx AsuncionNo ratings yet
- Classification of Trauma in ChildrenDocument9 pagesClassification of Trauma in ChildrenRita ValenteNo ratings yet
- b1 ChecklistDocument2 pagesb1 ChecklistRoryNo ratings yet
- 9 Dissacharides Metabolism Compatibility ModeDocument16 pages9 Dissacharides Metabolism Compatibility ModeAubrey Nativity Ostulano YangzonNo ratings yet
- Clavicle and Sternoclavicular JointDocument14 pagesClavicle and Sternoclavicular JointChavdarNo ratings yet
- Inles 4Document2 pagesInles 4Astrid CruzNo ratings yet
- Chase Resume 2017Document3 pagesChase Resume 2017api-380500256No ratings yet
- ASV GalileoDocument43 pagesASV GalileoalvyandaniNo ratings yet
- Impaction in Dairy Animals: Ashwani KumarDocument6 pagesImpaction in Dairy Animals: Ashwani KumarGiriNo ratings yet