You might also like
- Risk Factors for Developing LeprosyDocument8 pagesRisk Factors for Developing LeprosyAjie WitamaNo ratings yet
- Esclerosis ArtDocument13 pagesEsclerosis ArtKelly GómezNo ratings yet
- Journal Pone 0034866Document4 pagesJournal Pone 0034866Seki MuminovicNo ratings yet
- MS27x 17 PDFDocument9 pagesMS27x 17 PDFijasrjournalNo ratings yet
- Review Article: Pediatric Multiple Sclerosis: Current Concepts and Consensus DefinitionsDocument24 pagesReview Article: Pediatric Multiple Sclerosis: Current Concepts and Consensus DefinitionsKelly GómezNo ratings yet
- Low level viremia is associated with Serious Non-AIDS Events in People Living with HIVDocument20 pagesLow level viremia is associated with Serious Non-AIDS Events in People Living with HIVAbrahamKatimeNo ratings yet
- Herpes ZosterDocument8 pagesHerpes ZosterPramita SariNo ratings yet
- LSHTM Study Designs NOTES LSTHMDocument39 pagesLSHTM Study Designs NOTES LSTHMKELVIN MAYOMBONo ratings yet
- Risk Factor TuberculinDocument7 pagesRisk Factor TuberculinAnonymous oUg5v1p4zNo ratings yet
- Jurnal PVDocument8 pagesJurnal PVAndreas SudarmadiNo ratings yet
- Antimicrobial Therapy and Late Onset SepsisDocument10 pagesAntimicrobial Therapy and Late Onset SepsisKendy LópezNo ratings yet
- Risk Factors For Herpes Zoster Infection: A Meta-Analysis: Review ArticleDocument8 pagesRisk Factors For Herpes Zoster Infection: A Meta-Analysis: Review Articleyenny handayani sihiteNo ratings yet
- Endemic Kaposi Sarcoma in HIV-negativeDocument7 pagesEndemic Kaposi Sarcoma in HIV-negativeAriana AmarilesNo ratings yet
- Pediatrics 2012Document9 pagesPediatrics 2012Elin TaopanNo ratings yet
- Risk Factors For Tuberculosis InfectionDocument13 pagesRisk Factors For Tuberculosis InfectionIndahMayaSafitriNo ratings yet
- Population-Wide Analysis of Differences in Disease Progression Patterns in Men and WomenDocument14 pagesPopulation-Wide Analysis of Differences in Disease Progression Patterns in Men and WomenSagar SononeNo ratings yet
- Eating Disorders Epidemiology Incidence Prevalence Mortality RatesDocument9 pagesEating Disorders Epidemiology Incidence Prevalence Mortality RatesVictória NamurNo ratings yet
- Trend and Outcome of Sepsis in ChildrenDocument8 pagesTrend and Outcome of Sepsis in ChildrenGunduz AgaNo ratings yet
- Eclinicalmedicine: Victoria Peer, Naama Schwartz, Manfred S. GreenDocument10 pagesEclinicalmedicine: Victoria Peer, Naama Schwartz, Manfred S. GreenBryam Arango HuamanNo ratings yet
- Epidemiological Study of Clinical and Laboratory Profiles of Patients Woth ALL at DR SoetomoDocument5 pagesEpidemiological Study of Clinical and Laboratory Profiles of Patients Woth ALL at DR SoetomoJulia Intan Permata SariNo ratings yet
- Personality disorders and criminal behavior focus of psychiatric studyDocument1 pagePersonality disorders and criminal behavior focus of psychiatric studyAyu Ersya WindiraNo ratings yet
- Epi Descriptive Study DesignsDocument4 pagesEpi Descriptive Study DesignsAndrea BardalesNo ratings yet
- Captura de Pantalla 2024-01-23 A La(s) 11.26.43Document9 pagesCaptura de Pantalla 2024-01-23 A La(s) 11.26.43Dany MorBenNo ratings yet
- RAE - Articulo en InglesDocument3 pagesRAE - Articulo en InglesMaria Alejandra Suarez BaronNo ratings yet
- Kawasaki Disease: An Update: EpidemiologyDocument10 pagesKawasaki Disease: An Update: EpidemiologyEmma González de BaideNo ratings yet
- Review Article: The Risk Factors of Acquiring Severe Hand, Foot, and Mouth Disease: A Meta-AnalysisDocument13 pagesReview Article: The Risk Factors of Acquiring Severe Hand, Foot, and Mouth Disease: A Meta-AnalysisFan AccountNo ratings yet
- 17akinbolaji EtalDocument5 pages17akinbolaji EtaleditorijmrhsNo ratings yet
- Epidemiologic Study of Langerhans Cell Histiocytosis in Children.Document9 pagesEpidemiologic Study of Langerhans Cell Histiocytosis in Children.marioNo ratings yet
- Johne's Disease and Crohn's Disease, Report in BriefDocument2 pagesJohne's Disease and Crohn's Disease, Report in BriefNational Academies of Science, Engineering, and MedicineNo ratings yet
- Tropmed 86 698 PDFDocument5 pagesTropmed 86 698 PDFsandraldiraNo ratings yet
- International Journal of Pediatric Research Ijpr 9 112Document12 pagesInternational Journal of Pediatric Research Ijpr 9 112VsbshNo ratings yet
- Pediatrics 2013 Iwamoto E817 24Document10 pagesPediatrics 2013 Iwamoto E817 24phobicmdNo ratings yet
- Legionnaires' Disease Incidence and Risk Factors, New York, New York, USA, 2002-2011Document8 pagesLegionnaires' Disease Incidence and Risk Factors, New York, New York, USA, 2002-2011Stella ValenskaNo ratings yet
- Gittle R 2017Document4 pagesGittle R 2017Hari 'hardyboy' PurwantoNo ratings yet
- Journal of Rheumatology 2022 - Trajectory of Damage Accrual in SLE Based On Ethnicity and Socioeconomic FactorsDocument7 pagesJournal of Rheumatology 2022 - Trajectory of Damage Accrual in SLE Based On Ethnicity and Socioeconomic FactorsTengku Reza MaulanaNo ratings yet
- Travel-Associated Antimicrobial Drug-Resistant Nontyphoidal Salmonellae, 2004-2009Document9 pagesTravel-Associated Antimicrobial Drug-Resistant Nontyphoidal Salmonellae, 2004-2009Diandhara NuryadinNo ratings yet
- Community-Acquired Pneumonia Requiring Hospitalization Among U.S. ChildrenDocument11 pagesCommunity-Acquired Pneumonia Requiring Hospitalization Among U.S. ChildrenParasNo ratings yet
- Risk Factors For Childhood Leukemia: A Comprehensive Literature ReviewDocument37 pagesRisk Factors For Childhood Leukemia: A Comprehensive Literature Reviewmisbahhari_mdNo ratings yet
- Survival Analysis of Adult Tuberculosis Disease: Olurotimi Bankole Ajagbe, Zubair Kabair, Terry O'ConnorDocument10 pagesSurvival Analysis of Adult Tuberculosis Disease: Olurotimi Bankole Ajagbe, Zubair Kabair, Terry O'ConnorGetachew GemedaNo ratings yet
- Jurnal AlergiDocument10 pagesJurnal AlergiAbdurrahman HasanuddinNo ratings yet
- Early-Onset Basal Cell CarcinomaDocument11 pagesEarly-Onset Basal Cell CarcinomajxmackNo ratings yet
- Demographic Variations in HIV Testing History Among Emergency Department Patients: Implications For HIV Screening in US Emergency DepartmentsDocument7 pagesDemographic Variations in HIV Testing History Among Emergency Department Patients: Implications For HIV Screening in US Emergency DepartmentsAnyone ElseNo ratings yet
- Age-Related Differences in Hospitalization Rates, Clinical Presentation, and Outcomes Among Older Adults Hospitalized With Influenza-U.S. Influenza Hospitalization Surveillance NetworkDocument8 pagesAge-Related Differences in Hospitalization Rates, Clinical Presentation, and Outcomes Among Older Adults Hospitalized With Influenza-U.S. Influenza Hospitalization Surveillance NetworkTony RobertsNo ratings yet
- Nihms 1688237Document20 pagesNihms 1688237Mohammed KhalidNo ratings yet
- Diag BronchiolitisDocument2 pagesDiag BronchiolitisoussamamusNo ratings yet
- Baldwin 2016Document10 pagesBaldwin 2016Nahda Fini SNo ratings yet
- Autism, Inflammatory Bowel Disease, and MMR VaccineDocument1 pageAutism, Inflammatory Bowel Disease, and MMR VaccineSinn VolleNo ratings yet
- CISH and Susceptibility To Infectious Diseases: Original ArticleDocument10 pagesCISH and Susceptibility To Infectious Diseases: Original ArticlenovianastasiaNo ratings yet
- Do We Need A New Definition of Sepsis?: Intensive Care Medicine February 2015Document4 pagesDo We Need A New Definition of Sepsis?: Intensive Care Medicine February 2015Amirullah AbdiNo ratings yet
- Dengue Hemorrhagic Fever in Infants: A Study of Clinical and Cytokine ProfilesDocument12 pagesDengue Hemorrhagic Fever in Infants: A Study of Clinical and Cytokine ProfilesYono FabiandiNo ratings yet
- HCW Vs Adult Influenza IncidenceDocument9 pagesHCW Vs Adult Influenza Incidencereza_adrian_2No ratings yet
- Epidemiology and Genetics of Rheumatoid Arthritis: Supplement ReviewDocument8 pagesEpidemiology and Genetics of Rheumatoid Arthritis: Supplement ReviewdionysiaNo ratings yet
- Nutritional Status and Tuberculosis Risk in Adult and Pediatric Household ContactsDocument17 pagesNutritional Status and Tuberculosis Risk in Adult and Pediatric Household ContactshasmawihadriantiNo ratings yet
- Research Paper On Aids in AmericaDocument6 pagesResearch Paper On Aids in Americajssoulznd100% (1)
- Respiratory Syncytial Virus Infections in Children With Acute Myeloid Leukemia: A Report From The Children's Oncology GroupDocument3 pagesRespiratory Syncytial Virus Infections in Children With Acute Myeloid Leukemia: A Report From The Children's Oncology GrouperickmattosNo ratings yet
- 30 Scientific Studies Link Vaccines to AutismDocument23 pages30 Scientific Studies Link Vaccines to Autismazrulelias100% (5)
- Gender 22Document4 pagesGender 22andi tzamrah istiqani syamNo ratings yet
- Knowledge Attitudes and Testing Preferences For Herpes Simplex Virus Infections Among Undergraduate Students at A Large University in Los AngelesDocument7 pagesKnowledge Attitudes and Testing Preferences For Herpes Simplex Virus Infections Among Undergraduate Students at A Large University in Los AngelessesiaNo ratings yet
- International Journal of Infectious Diseases: A A B A A A A A A A A B ADocument9 pagesInternational Journal of Infectious Diseases: A A B A A A A A A A A B AzikryauliaNo ratings yet
- Managing Health in the Genomic Era: A Guide to Family Health History and Disease RiskFrom EverandManaging Health in the Genomic Era: A Guide to Family Health History and Disease RiskNo ratings yet
- What Did The Martyrs Die For?: Martyrs or Political Criminals?Document13 pagesWhat Did The Martyrs Die For?: Martyrs or Political Criminals?Mihailo Majk ŽikićNo ratings yet
- Learn English A Beginner S Guide For Esl Learners Swan JennaDocument117 pagesLearn English A Beginner S Guide For Esl Learners Swan Jennasofronelena100% (6)
- Creation Out of Nothing: King Lear IV, 4, 122-6Document7 pagesCreation Out of Nothing: King Lear IV, 4, 122-6Mihailo Majk ŽikićNo ratings yet
- Data Science and Big Data Computing - Frameworks and MethodologiesDocument332 pagesData Science and Big Data Computing - Frameworks and MethodologiesMihailo Majk Žikić89% (9)
- Roman Catholic Church of CorruptionDocument4 pagesRoman Catholic Church of CorruptionherbertheadNo ratings yet
- Writing Magazine - August 2016Document112 pagesWriting Magazine - August 2016Mihailo Majk ŽikićNo ratings yet
- Word 2010 Thesis FinalDocument13 pagesWord 2010 Thesis FinalMihailo Majk ŽikićNo ratings yet
- 2005 09798 012Document7 pages2005 09798 012Mihailo Majk ŽikićNo ratings yet
- Nursing Growth and Development - G and D General OverviewDocument15 pagesNursing Growth and Development - G and D General OverviewMihailo Majk ŽikićNo ratings yet
- Biodiversity LichensDocument7 pagesBiodiversity LichensMihailo Majk ŽikićNo ratings yet
- Monasteries and Churches On Aegina IslandDocument2 pagesMonasteries and Churches On Aegina IslandMihailo Majk ŽikićNo ratings yet
- Severe Defects in Absorptive Ion Transport in Distal Colons of Mice That Lack ClC-2 ChannelsDocument7 pagesSevere Defects in Absorptive Ion Transport in Distal Colons of Mice That Lack ClC-2 ChannelsMihailo Majk ŽikićNo ratings yet
- Rabit Distal Colon Epithelium - IIDocument4 pagesRabit Distal Colon Epithelium - IIMihailo Majk ŽikićNo ratings yet
- Bcl-2 Gene Promotes Haemopoietic Cell Survival and Co... (NatureDocument1 pageBcl-2 Gene Promotes Haemopoietic Cell Survival and Co... (NatureMihailo Majk ŽikićNo ratings yet
- Active Potassium Transport Across Guinea-Pig Dista... (J PhysiolDocument1 pageActive Potassium Transport Across Guinea-Pig Dista... (J PhysiolMihailo Majk ŽikićNo ratings yet
- 8 Tones PresentationDocument42 pages8 Tones PresentationMihailo Majk Žikić100% (1)
- NURE 212course SyllabusDocument11 pagesNURE 212course SyllabusMihailo Majk ŽikićNo ratings yet
- Erikson's 8 Stages of Psychosocial Development Summary ChartDocument1 pageErikson's 8 Stages of Psychosocial Development Summary ChartMihailo Majk ŽikićNo ratings yet
- 001Document48 pages001Mihailo Majk ŽikićNo ratings yet
- Basolateral K-CL Cotransporter Regulates Colonic Potassium Absorption in Potassium Depletion PDFDocument7 pagesBasolateral K-CL Cotransporter Regulates Colonic Potassium Absorption in Potassium Depletion PDFMihailo Majk ŽikićNo ratings yet
- Active Potassium Transport Across Guinea-Pig Distal Colon - Action of S - by Gerhard Rechkemmer, Et Al PDFDocument2 pagesActive Potassium Transport Across Guinea-Pig Distal Colon - Action of S - by Gerhard Rechkemmer, Et Al PDFMihailo Majk ŽikićNo ratings yet
- Biological and Medical PhysicsDocument21 pagesBiological and Medical PhysicsMihailo Majk ŽikićNo ratings yet
- Principles of Embryonic DevelopmentDocument29 pagesPrinciples of Embryonic DevelopmentMihailo Majk ŽikićNo ratings yet
- Impact of Dairy Subsidies in NepalDocument123 pagesImpact of Dairy Subsidies in NepalGaurav PradhanNo ratings yet
- Egg Pasteurization Manual 1969Document54 pagesEgg Pasteurization Manual 1969Tomas MuzzioNo ratings yet
- RESEARCH PROPOSAL-Final AfraaaazzzzzzzzzDocument13 pagesRESEARCH PROPOSAL-Final AfraaaazzzzzzzzzRizwan Abdul Maalik50% (2)
- The Motive Journal (3rd Edition)Document42 pagesThe Motive Journal (3rd Edition)Shubham Sharma0% (1)
- 432 HZ - Unearthing The Truth Behind Nature's FrequencyDocument6 pages432 HZ - Unearthing The Truth Behind Nature's FrequencyShiv KeskarNo ratings yet
- 3.SAFA AOCS 4th Ed Ce 2-66 1994Document6 pages3.SAFA AOCS 4th Ed Ce 2-66 1994Rofiyanti WibowoNo ratings yet
- SafewayDocument70 pagesSafewayhampshireiiiNo ratings yet
- Test Units and Accessories: Sinteso™Document22 pagesTest Units and Accessories: Sinteso™Imad QsnNo ratings yet
- Myofascial Release for Piriformis MyalgiaDocument14 pagesMyofascial Release for Piriformis MyalgiaApoorvNo ratings yet
- Research PaperDocument12 pagesResearch PapershreyanshNo ratings yet
- DSUSJRC01161350 Corail ST-Total Hip SystemDocument20 pagesDSUSJRC01161350 Corail ST-Total Hip SystemXeniaNo ratings yet
- 9 Oet Reading Summary 2.0-195-213Document19 pages9 Oet Reading Summary 2.0-195-213Vijayalakshmi Narayanaswami0% (1)
- Versidrain 150: Green RoofDocument2 pagesVersidrain 150: Green RoofMichael Tiu TorresNo ratings yet
- VentilationDocument92 pagesVentilationRobert Nixon100% (1)
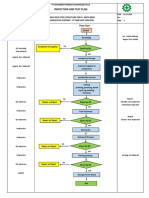
- Inspection and Test Plan: Flow Chart Start IncomingDocument1 pageInspection and Test Plan: Flow Chart Start IncomingSinden AyuNo ratings yet
- Rice Research: Open Access: Black Rice Cultivation and Forming Practices: Success Story of Indian FarmersDocument2 pagesRice Research: Open Access: Black Rice Cultivation and Forming Practices: Success Story of Indian Farmersapi-420356823No ratings yet
- Platinum Gazette 29 November 2013Document12 pagesPlatinum Gazette 29 November 2013Anonymous w8NEyXNo ratings yet
- Refresher 2 (Pipe)Document12 pagesRefresher 2 (Pipe)Kira YagamiNo ratings yet
- Final TLE9 Nail Care9 Q1 Module 3Document20 pagesFinal TLE9 Nail Care9 Q1 Module 3Ma. Andrea LagmanNo ratings yet
- Presentation On Data Integrity in PharmaDocument80 pagesPresentation On Data Integrity in Pharmaskvemula67% (3)
- Evolution Chart 3Document1 pageEvolution Chart 3sasupraNo ratings yet
- SEXUALABUSEDocument12 pagesSEXUALABUSERyoman EchozenNo ratings yet
- PR Cuisine vs US CuisineDocument2 pagesPR Cuisine vs US CuisineJannette HernandezNo ratings yet
- Electrolyte AE 11 - MSDSDocument8 pagesElectrolyte AE 11 - MSDSShinta Nugraha MughniNo ratings yet
- Flexible and Alternative Seating: in ClassroomsDocument5 pagesFlexible and Alternative Seating: in ClassroomsweningNo ratings yet
- Carbon Cycle Game Worksheet - EportfolioDocument2 pagesCarbon Cycle Game Worksheet - Eportfolioapi-264746220No ratings yet
- Limetas Maximos ResidualesDocument27 pagesLimetas Maximos ResidualesXjoelx Olaya GonzalesNo ratings yet
- El Bill PDFDocument2 pagesEl Bill PDFvinodNo ratings yet
- The Congressional Committee and Philippine Policymaking: The Case of The Anti-Rape Law - Myrna LavidesDocument29 pagesThe Congressional Committee and Philippine Policymaking: The Case of The Anti-Rape Law - Myrna LavidesmarielkuaNo ratings yet
- Catalogo Unidad Enfriadora Trane R-407C PDFDocument8 pagesCatalogo Unidad Enfriadora Trane R-407C PDFJUAN FRANCISCO AYALANo ratings yet