You might also like
- Public Health NutritionDocument58 pagesPublic Health NutritionJaime TaylorNo ratings yet
- Nutrition in AdolescenceDocument53 pagesNutrition in AdolescenceAbdhanie Panontongan100% (2)
- Eating Habits and Behaviors Physical Activity Nutr PDFDocument14 pagesEating Habits and Behaviors Physical Activity Nutr PDFEDUARDO JOSUE ALBERTO VENTONo ratings yet
- The History of BanquetsDocument6 pagesThe History of BanquetsBlaze QuibanNo ratings yet
- Basic Knife SkillsDocument19 pagesBasic Knife SkillsMary Ann Dela CernaNo ratings yet
- Nutritional Deficiency For ClassDocument74 pagesNutritional Deficiency For ClassBelayneh TadesseNo ratings yet
- MalnutrionDocument44 pagesMalnutrionnajeebNo ratings yet
- Adolescent Nutrition OutLineDocument38 pagesAdolescent Nutrition OutLineJedeth MamoraNo ratings yet
- Nutrition Research PaperDocument6 pagesNutrition Research PaperAshley NoblesNo ratings yet
- Types of Catering Establishments PRINTDocument3 pagesTypes of Catering Establishments PRINTSrinibas Jena100% (2)
- Importance & Principle of Meal PlanningDocument18 pagesImportance & Principle of Meal PlanningSaher YasinNo ratings yet
- Culinary Arts Welcome LetterDocument16 pagesCulinary Arts Welcome LetterWhena RiosNo ratings yet
- Intro To NASDocument32 pagesIntro To NASchoa hannahNo ratings yet
- The Food & Nutrition Program Planning CycleDocument8 pagesThe Food & Nutrition Program Planning CycleGabriel PhilippeNo ratings yet
- Fundamentals of PlatingDocument16 pagesFundamentals of PlatingEda GadoyNo ratings yet
- Assessment of Nutritional SituationDocument24 pagesAssessment of Nutritional SituationMawasumi Ayu Andini0% (1)
- ElderlyDocument19 pagesElderlyrjNo ratings yet
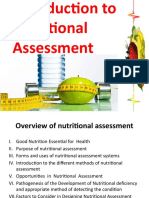
- Lesson 3 Nutritional AssessmentDocument84 pagesLesson 3 Nutritional AssessmentJake ArizapaNo ratings yet
- NCM 105 Lecture Covers Nutrition Through Life StagesDocument17 pagesNCM 105 Lecture Covers Nutrition Through Life StagesSyed FlyntNo ratings yet
- Unit 6-Nutrition and HydrationDocument109 pagesUnit 6-Nutrition and Hydration1sylvialee100% (2)
- Nutritioninoldage 170316191924Document24 pagesNutritioninoldage 170316191924Alefiyah IndorewalaNo ratings yet
- Foodborne IllnessesDocument30 pagesFoodborne IllnessesNicoel100% (6)
- Hiv / Aids and Nutrition IssuesDocument13 pagesHiv / Aids and Nutrition IssuesMINANI TheobaldNo ratings yet
- Concept of Community NutritionDocument4 pagesConcept of Community NutritionNrs Sani Sule MashiNo ratings yet
- Fish and ShellfishDocument117 pagesFish and Shellfishshanley cyra aboNo ratings yet
- MenuDocument25 pagesMenuAnonymous n2DjmCHQ8CNo ratings yet
- Chapter 9 - Sensory EvaluationDocument15 pagesChapter 9 - Sensory EvaluationLiyana ShahiminNo ratings yet
- Food and Nutrition II SyllabusDocument2 pagesFood and Nutrition II Syllabusapi-239512266No ratings yet
- Community NutritionDocument22 pagesCommunity NutritionLilis IndriNo ratings yet
- An Analysis of Consumers Attitude Towards Food LabelingDocument48 pagesAn Analysis of Consumers Attitude Towards Food LabelingIvy Miraña CarulloNo ratings yet
- Nutritional AssessmentDocument6 pagesNutritional AssessmentReyna Mee AhiyasNo ratings yet
- Role of DieticianDocument18 pagesRole of DieticianAnju RaniNo ratings yet
- Nutrition Care ProcessDocument7 pagesNutrition Care ProcessALYSSA NICOLE GINESNo ratings yet
- Assesment of Nutritional Status in Emergency-Affected PopulationsDocument28 pagesAssesment of Nutritional Status in Emergency-Affected PopulationsIrma ArmiyahNo ratings yet
- Factors Affecting Food Choices: Culture, Social, Emotions, Agriculture, Technology, Economics, PoliticsDocument24 pagesFactors Affecting Food Choices: Culture, Social, Emotions, Agriculture, Technology, Economics, Politicsspartanstar100% (1)
- Table AppointmentsDocument11 pagesTable AppointmentsAbby ManaoisNo ratings yet
- Nutrition Care Process Midterm NotesDocument12 pagesNutrition Care Process Midterm NotesJecel LazarraNo ratings yet
- Hunger and MalnutritionDocument4 pagesHunger and MalnutritionCarlos LleverNo ratings yet
- Nutritional Assessment Methods SummaryDocument45 pagesNutritional Assessment Methods SummaryJrose CuerpoNo ratings yet
- 5 Nutrition Care ProcessDocument10 pages5 Nutrition Care ProcessMilagros ConstantinoNo ratings yet
- Financial & Cash Flow Problems for EntrepreneursDocument9 pagesFinancial & Cash Flow Problems for EntrepreneursCda ShidaNo ratings yet
- UNIT 5 - The MenuDocument7 pagesUNIT 5 - The MenuRHTi BDNo ratings yet
- Nutritional AssessmentDocument7 pagesNutritional AssessmentCm MacaliaNo ratings yet
- VN Nutr Exam 2 CH 11-15: QuestionsDocument18 pagesVN Nutr Exam 2 CH 11-15: QuestionsNursyNurseNo ratings yet
- Nutritional AssessmentDocument8 pagesNutritional AssessmentOutour KhNo ratings yet
- Meal Planning GuideDocument39 pagesMeal Planning GuidePrincess Jane BalagtasNo ratings yet
- The Changing Nutritional Needs Across The Life CycleDocument24 pagesThe Changing Nutritional Needs Across The Life CycleFrance Dave CantorNo ratings yet
- Activity in Professional Ethics MIDTERMDocument10 pagesActivity in Professional Ethics MIDTERMAr Jay JuanNo ratings yet
- Food LabelsDocument39 pagesFood LabelsWahyu Erwin FirmansyahNo ratings yet
- Public Health Nutrition: Its Importance For Health Promotion & Health PreservationDocument36 pagesPublic Health Nutrition: Its Importance For Health Promotion & Health PreservationSumaia Rahman100% (1)
- Plan Effective School Menus with Cycle Menu TemplatesDocument7 pagesPlan Effective School Menus with Cycle Menu TemplatesMahlodi LamolaNo ratings yet
- 7th National Nutrition SurveyDocument2 pages7th National Nutrition SurveyJorace VillamilNo ratings yet
- Food SecurityDocument23 pagesFood SecurityCabdicasiis xiisNo ratings yet
- Life CycleDocument30 pagesLife Cycleapi-246570276100% (1)
- Casestudy 1Document6 pagesCasestudy 1api-240055755No ratings yet
- Menu DevelopmentDocument24 pagesMenu DevelopmentnadkecikNo ratings yet
- Basic Concepts of Food and NutritionDocument14 pagesBasic Concepts of Food and NutritionDilon MendoncaNo ratings yet
- Community NutritionDocument14 pagesCommunity NutritionVaishali JainarainNo ratings yet
- Analysis of Food Products 1.: 1.1. Reasons For Analyzing FoodsDocument27 pagesAnalysis of Food Products 1.: 1.1. Reasons For Analyzing FoodsAngelo Aureus DelossantosNo ratings yet
- Adolescent Eating Habits - UpToDateDocument33 pagesAdolescent Eating Habits - UpToDateDaniela Herrera LozanoNo ratings yet
- Monday Start - Dashboard Weekly - Productivity DailyDocument15 pagesMonday Start - Dashboard Weekly - Productivity DailyDS Nan SalimNo ratings yet
- Ramadan Calendar 2021 Islamabad HanafiDocument1 pageRamadan Calendar 2021 Islamabad HanafiIltaf KhalidNo ratings yet
- C0222-小学英语语法专项练习-few a Few Little a Little辨析练习 100题 9页Document9 pagesC0222-小学英语语法专项练习-few a Few Little a Little辨析练习 100题 9页SudepeNo ratings yet
- Ideas For Microactivities For Physical Activity - Sedentary BehaviorDocument3 pagesIdeas For Microactivities For Physical Activity - Sedentary BehavioralbamarchrubioNo ratings yet
- Easier to Gain than Lose WeightDocument38 pagesEasier to Gain than Lose WeightBari SyedNo ratings yet
- Ket Speaking Part 1Document5 pagesKet Speaking Part 1Marck AlvarezNo ratings yet
- Food of Chinese CultureDocument6 pagesFood of Chinese Culturexin weiNo ratings yet
- Weekly Meal Plan and Diet TrackerDocument4 pagesWeekly Meal Plan and Diet TrackerAnnie Mae Salazar CentinoNo ratings yet
- Neighborhood Community Public Transportation Restaurant: Teacher SonnyDocument21 pagesNeighborhood Community Public Transportation Restaurant: Teacher SonnySonny ObienaNo ratings yet
- Malaysian Nasi LemakDocument3 pagesMalaysian Nasi Lemakpapa_terakhir0% (1)
- Tarea 2 Writing: Universidad Nacional Abierta Y A Distancia - UnadDocument4 pagesTarea 2 Writing: Universidad Nacional Abierta Y A Distancia - UnadJaime Leon AlvarezNo ratings yet
- Diagnostic Test On Food and BeveragesDocument2 pagesDiagnostic Test On Food and BeveragesRonald Serrano100% (3)
- Nutritional Status ReportDocument23 pagesNutritional Status ReportJada Kate SarciaNo ratings yet
- Sample Meal Plan - 3000 Calories: Breakfast Protein Carbohydrates FAT CaloriesDocument3 pagesSample Meal Plan - 3000 Calories: Breakfast Protein Carbohydrates FAT CaloriesAlex CastleNo ratings yet
- Your Wellness IntelligenceDocument1 pageYour Wellness Intelligencelackua100% (1)
- I. Choose The Word That Has The Underlined Part Pronounced Differently From The RestDocument4 pagesI. Choose The Word That Has The Underlined Part Pronounced Differently From The RestLe Thanh TrieuNo ratings yet
- Reverse Diet GuideDocument10 pagesReverse Diet Guidesergio viquezNo ratings yet
- Raw - The Yoga of Food PDFDocument5 pagesRaw - The Yoga of Food PDFSusan Karpp Sgroi100% (2)
- Sushi Takeout and Delivery Menu at China Blossom in North Andover, MADocument2 pagesSushi Takeout and Delivery Menu at China Blossom in North Andover, MAchinablossom0% (1)
- Yippee Recipe BookletDocument32 pagesYippee Recipe BookletIdol RockNo ratings yet
- ULANGAN KENAIKAN KELAS BAHASA INGGRIS KELAS 3Document3 pagesULANGAN KENAIKAN KELAS BAHASA INGGRIS KELAS 3Yusak Budi SantosoNo ratings yet
- Simple Ways to Plan, Enjoy, and Stick to a Healthy DietDocument6 pagesSimple Ways to Plan, Enjoy, and Stick to a Healthy DietWanNurAtikahNo ratings yet
- Final Exam Basico 5 EFDocument5 pagesFinal Exam Basico 5 EFJULIO CHRISTIAN RAMIREZ VARGASNo ratings yet
- 3 Steps To Lose Weight That Will LastDocument3 pages3 Steps To Lose Weight That Will Lastarie hendNo ratings yet
- LunchDocument1 pageLuncheatlocalmenusNo ratings yet
- Activity 4 Food & Beverage ServiceDocument13 pagesActivity 4 Food & Beverage ServiceEricka Rose AlvarezNo ratings yet
- Skrip Role Play at RestaurantDocument5 pagesSkrip Role Play at RestaurantDaffa AndiNo ratings yet
- The Government Should Implement Sugar Taxes To Reduce ObesityDocument2 pagesThe Government Should Implement Sugar Taxes To Reduce ObesityVivek sharmaNo ratings yet
- Objective: Martin L. GriffinDocument4 pagesObjective: Martin L. GriffinMartin GriffinNo ratings yet
- The Oberoi New Delhi Baoshuan Chinese Restaurant - A La CarteDocument9 pagesThe Oberoi New Delhi Baoshuan Chinese Restaurant - A La CarteAjay BhardwajNo ratings yet
- The Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyFrom EverandThe Diabetes Code: Prevent and Reverse Type 2 Diabetes NaturallyRating: 5 out of 5 stars5/5 (1)
- Summary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisFrom EverandSummary: Fast Like a Girl: A Woman’s Guide to Using the Healing Power of Fasting to Burn Fat, Boost Energy, and Balance Hormones: Key Takeaways, Summary and AnalysisRating: 3 out of 5 stars3/5 (2)
- Keto Friendly Recipes: Easy Keto For Busy PeopleFrom EverandKeto Friendly Recipes: Easy Keto For Busy PeopleRating: 3.5 out of 5 stars3.5/5 (2)
- Instant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookFrom EverandInstant Loss On a Budget: Super-Affordable Recipes for the Health-Conscious CookRating: 3.5 out of 5 stars3.5/5 (2)
- Allen Carr's Easy Way for Women to Lose Weight: The original Easyway methodFrom EverandAllen Carr's Easy Way for Women to Lose Weight: The original Easyway methodRating: 4.5 out of 5 stars4.5/5 (18)
- Summary of Mary Claire Haver's The Galveston DietFrom EverandSummary of Mary Claire Haver's The Galveston DietRating: 5 out of 5 stars5/5 (1)
- Forever Strong: A New, Science-Based Strategy for Aging WellFrom EverandForever Strong: A New, Science-Based Strategy for Aging WellNo ratings yet
- Body Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomFrom EverandBody Love Every Day: Choose Your Life-Changing 21-Day Path to Food FreedomRating: 4 out of 5 stars4/5 (1)
- Glucose Goddess Method: A 4-Week Guide to Cutting Cravings, Getting Your Energy Back, and Feeling AmazingFrom EverandGlucose Goddess Method: A 4-Week Guide to Cutting Cravings, Getting Your Energy Back, and Feeling AmazingRating: 5 out of 5 stars5/5 (59)
- The Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsFrom EverandThe Arm: Inside the Billion-Dollar Mystery of the Most Valuable Commodity in SportsRating: 4 out of 5 stars4/5 (49)
- The Fast800 Diet: Discover the Ideal Fasting Formula to Shed Pounds, Fight Disease, and Boost Your Overall HealthFrom EverandThe Fast800 Diet: Discover the Ideal Fasting Formula to Shed Pounds, Fight Disease, and Boost Your Overall HealthRating: 5 out of 5 stars5/5 (37)
- Hungry for Change: Ditch the Diets, Conquer the Cravings, and Eat Your Way to Lifelong HealthFrom EverandHungry for Change: Ditch the Diets, Conquer the Cravings, and Eat Your Way to Lifelong HealthRating: 4 out of 5 stars4/5 (7)
- Happy Gut: The Cleansing Program to Help You Lose Weight, Gain Energy, and Eliminate PainFrom EverandHappy Gut: The Cleansing Program to Help You Lose Weight, Gain Energy, and Eliminate PainRating: 3.5 out of 5 stars3.5/5 (6)
- Proteinaholic: How Our Obsession with Meat Is Killing Us and What We Can Do About ItFrom EverandProteinaholic: How Our Obsession with Meat Is Killing Us and What We Can Do About ItRating: 4.5 out of 5 stars4.5/5 (19)
- How to Be Well: The 6 Keys to a Happy and Healthy LifeFrom EverandHow to Be Well: The 6 Keys to a Happy and Healthy LifeRating: 5 out of 5 stars5/5 (1)
- Eat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouFrom EverandEat to Lose, Eat to Win: Your Grab-n-Go Action Plan for a Slimmer, Healthier YouNo ratings yet
- Metabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeFrom EverandMetabolism Revolution: Lose 14 Pounds in 14 Days and Keep It Off for LifeNo ratings yet
- The Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthFrom EverandThe Candida Cure: The 90-Day Program to Balance Your Gut, Beat Candida, and Restore Vibrant HealthNo ratings yet
- Grit & Grace: Train the Mind, Train the Body, Own Your LifeFrom EverandGrit & Grace: Train the Mind, Train the Body, Own Your LifeRating: 4 out of 5 stars4/5 (3)
- Lose Weight by Eating: 130 Amazing Clean-Eating Makeovers for Guilt-Free Comfort FoodFrom EverandLose Weight by Eating: 130 Amazing Clean-Eating Makeovers for Guilt-Free Comfort FoodRating: 2 out of 5 stars2/5 (1)
- Rapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreFrom EverandRapid Weight Loss Hypnosis: How to Lose Weight with Self-Hypnosis, Positive Affirmations, Guided Meditations, and Hypnotherapy to Stop Emotional Eating, Food Addiction, Binge Eating and MoreRating: 5 out of 5 stars5/5 (17)
- The Intuitive Eating Workbook: 10 Principles for Nourishing a Healthy Relationship with FoodFrom EverandThe Intuitive Eating Workbook: 10 Principles for Nourishing a Healthy Relationship with FoodRating: 4.5 out of 5 stars4.5/5 (20)
- Ultrametabolism: The Simple Plan for Automatic Weight LossFrom EverandUltrametabolism: The Simple Plan for Automatic Weight LossRating: 4.5 out of 5 stars4.5/5 (28)
- The Raw Food Detox Diet: The Five-Step Plan for Vibrant Health and Maximum Weight LossFrom EverandThe Raw Food Detox Diet: The Five-Step Plan for Vibrant Health and Maximum Weight LossRating: 4 out of 5 stars4/5 (22)
- The Whole Body Reset: Your Weight-Loss Plan for a Flat Belly, Optimum Health & a Body You'll Love at Midlife and BeyondFrom EverandThe Whole Body Reset: Your Weight-Loss Plan for a Flat Belly, Optimum Health & a Body You'll Love at Midlife and BeyondRating: 4.5 out of 5 stars4.5/5 (28)
- Power Souping: 3-Day Detox, 3-Week Weight-Loss PlanFrom EverandPower Souping: 3-Day Detox, 3-Week Weight-Loss PlanRating: 3.5 out of 5 stars3.5/5 (3)
- The Longevity Plan: Seven Life-Transforming Lessons from Ancient ChinaFrom EverandThe Longevity Plan: Seven Life-Transforming Lessons from Ancient ChinaNo ratings yet
- Think Yourself Thin: A 30-Day Guide to Permanent Weight LossFrom EverandThink Yourself Thin: A 30-Day Guide to Permanent Weight LossRating: 4.5 out of 5 stars4.5/5 (22)