You might also like
- Kalpana Srivastava Author Information : Concept of Personality: Indian PerspectiveDocument4 pagesKalpana Srivastava Author Information : Concept of Personality: Indian PerspectiveAnanya NarangNo ratings yet
- Resilience Scale: Please Circle A Number Indicating How Much You Agree or Disagree With Each StatementDocument3 pagesResilience Scale: Please Circle A Number Indicating How Much You Agree or Disagree With Each StatementFarah NoreenNo ratings yet
- All About The Mayer-Salovey-Caruso Emotional Intelligence Test (MSCEIT)Document11 pagesAll About The Mayer-Salovey-Caruso Emotional Intelligence Test (MSCEIT)Fiolin Chang100% (1)
- What Is KaivishamDocument2 pagesWhat Is KaivishamSalim MichaelNo ratings yet
- 16PF BibDocument10 pages16PF BibdocagunsNo ratings yet
- Transpersonal Psychology in The BhagavadDocument9 pagesTranspersonal Psychology in The BhagavadNavneet DhimanNo ratings yet
- Goldstein's Organismic Theory Views the Person HolisticallyDocument2 pagesGoldstein's Organismic Theory Views the Person HolisticallyLeeNo ratings yet
- Eysenck Questionnaire PDFDocument2 pagesEysenck Questionnaire PDFSuz0% (1)
- Psychology Talks 2011 - DR Gitanjali (NUH)Document31 pagesPsychology Talks 2011 - DR Gitanjali (NUH)nuspsycheNo ratings yet
- Developmental Follow Up ProgramsDocument5 pagesDevelopmental Follow Up ProgramsSubramani SambandamNo ratings yet
- Indian Psychology of MotivationDocument12 pagesIndian Psychology of MotivationJuan Luis Köstner MartinoNo ratings yet
- Family TherapyDocument8 pagesFamily TherapyManoj NayakNo ratings yet
- Brain Dominance ScaleDocument3 pagesBrain Dominance ScaleTheoNo ratings yet
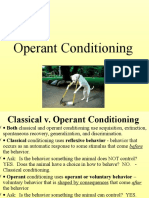
- Operant ConditioningDocument76 pagesOperant ConditioningJiya JanjuaNo ratings yet
- Perception Influencing HR Sensitiveness in Work Place - Conceptual StudyDocument12 pagesPerception Influencing HR Sensitiveness in Work Place - Conceptual StudyTJPRC PublicationsNo ratings yet
- Case History and MseDocument7 pagesCase History and MseILIKA GUHA MAJUMDAR Department of Psychology NCRNo ratings yet
- Type ABDocument4 pagesType ABEswar NaveenNo ratings yet
- Ch. Devi Lal College of Education Jagadhri Psychology Resource CentreDocument3 pagesCh. Devi Lal College of Education Jagadhri Psychology Resource CentreMeenu Minu100% (1)
- Beck Youth ReviewDocument8 pagesBeck Youth ReviewalexutzadulcikaNo ratings yet
- Wisdom Assessment ScaleDocument11 pagesWisdom Assessment ScaleMehar100% (1)
- Oriental ApproachesDocument7 pagesOriental ApproachestabazeemNo ratings yet
- Mental Health Inventory ManualDocument14 pagesMental Health Inventory ManualSunil Rathod100% (2)
- Introduction To Psychological TestingDocument5 pagesIntroduction To Psychological TestingKhushi GandhiNo ratings yet
- A Brief History of The Origins of Behavioral MedicineDocument16 pagesA Brief History of The Origins of Behavioral MedicineAllie WatrenNo ratings yet
- Clinical Psy Training 2015Document10 pagesClinical Psy Training 2015Tejaswi BlsNo ratings yet
- Module 5 Regulation of Internal EnvironmentDocument17 pagesModule 5 Regulation of Internal EnvironmentSakshi Jauhari100% (1)
- Amity University Practical Notebook Guide to Personality TestsDocument68 pagesAmity University Practical Notebook Guide to Personality TestsYamini JohriNo ratings yet
- Sacks Sentence Completion Test ReportDocument16 pagesSacks Sentence Completion Test ReportMatthew CalizonNo ratings yet
- Eysenck Personality Questionnaire AssessmentDocument4 pagesEysenck Personality Questionnaire AssessmentfosterbalaNo ratings yet
- CBT AnxietyDocument4 pagesCBT AnxietyBombey GymnectNo ratings yet
- Health Psychology AssumptionsDocument12 pagesHealth Psychology Assumptionsbrira100% (2)
- DBDA IntroductionDocument5 pagesDBDA IntroductionDrMegha Kharkwal0% (1)
- Bernard Gallagher Cap. 5 Sociology of Mental IllnessDocument16 pagesBernard Gallagher Cap. 5 Sociology of Mental IllnessLaura CristinaNo ratings yet
- Vineland Social Maturity ScaleDocument2 pagesVineland Social Maturity ScaleJavier Eduardo Rendon Ramirez100% (1)
- Structuring Skill (Revised)Document18 pagesStructuring Skill (Revised)Khairina ZaiadiNo ratings yet
- MCQ Practice For HappinessDocument5 pagesMCQ Practice For HappinessSanjeev Kumar100% (1)
- Practical 4 CASI Kaashvi Dubey PSYBSC18038Document18 pagesPractical 4 CASI Kaashvi Dubey PSYBSC18038kaashvi dubeyNo ratings yet
- Dimensionality of the Brief Self-Control ScaleDocument32 pagesDimensionality of the Brief Self-Control ScaleRicardo LunaNo ratings yet
- Vsms Page 1 13 Vsms ManualDocument72 pagesVsms Page 1 13 Vsms ManualRizwan ReyazNo ratings yet
- Psychophysiological Disorders: Bs 6A+B Urwah AliDocument29 pagesPsychophysiological Disorders: Bs 6A+B Urwah Aliareesha naseerNo ratings yet
- Dbda Introduction - Group 4Document6 pagesDbda Introduction - Group 4mrinalini bhatNo ratings yet
- Resilience ScaleDocument6 pagesResilience ScaleileanasinzianaNo ratings yet
- Beck Cognitive Insight ScaleDocument3 pagesBeck Cognitive Insight ScalesrinivasanaNo ratings yet
- Physical and Mental Disability TestDocument9 pagesPhysical and Mental Disability TestANITTA SNo ratings yet
- Jaina Psychology: Jagdish Prasad JainDocument18 pagesJaina Psychology: Jagdish Prasad JainJuan Luis Köstner MartinoNo ratings yet
- PSC-17 Scoring Guide for Pediatric Symptom ChecklistDocument1 pagePSC-17 Scoring Guide for Pediatric Symptom ChecklistMayang Sukma SatriaNo ratings yet
- Viva Questions 11Document1 pageViva Questions 11sheby babu100% (1)
- A Case Study On Hostel LifeDocument14 pagesA Case Study On Hostel Lifesabitri sharma100% (1)
- Firo-B PracDocument29 pagesFiro-B Prackhushi chopra 0050No ratings yet
- Guidelines For Psychological Testing of Deaf and Hard of Hearing StudentsDocument23 pagesGuidelines For Psychological Testing of Deaf and Hard of Hearing StudentsMihai Predescu100% (1)
- CBSE Psychology Practical XIIDocument78 pagesCBSE Psychology Practical XIIRajit krishnaNo ratings yet
- Emotional Maturity ScaleDocument4 pagesEmotional Maturity ScaleVidhya SNo ratings yet
- Marital adjustment questionnaireDocument1 pageMarital adjustment questionnaireGiridharan Venkatesh0% (1)
- A Primer On Workplace CounsellingDocument19 pagesA Primer On Workplace CounsellingPiaa Raj100% (1)
- Interpersonalrelationships ContentmethodDocument2 pagesInterpersonalrelationships ContentmethodmeghaputhusseryNo ratings yet
- Gender Issues in Career CounselingDocument2 pagesGender Issues in Career CounselingNur Qatrunnada100% (2)
- Response Set (Psychological Perspective)Document15 pagesResponse Set (Psychological Perspective)MacxieNo ratings yet
- Undertanding PTSDDocument18 pagesUndertanding PTSDaladenteNo ratings yet
- Management Guidelines For Anxiety Disorders in Children and AdolescentsDocument23 pagesManagement Guidelines For Anxiety Disorders in Children and AdolescentsHari HaranNo ratings yet
- Attachment Measures in Middle Childhood and Adolescence A SystematicDocument12 pagesAttachment Measures in Middle Childhood and Adolescence A SystematicSabrina HortopanNo ratings yet
- Depp Rev Seligman 1999Document24 pagesDepp Rev Seligman 1999sarara1No ratings yet
- The Development of Cognitive Vulnerability HOPELESSNESS DepressionDocument13 pagesThe Development of Cognitive Vulnerability HOPELESSNESS Depressionsarara1No ratings yet
- Rezilienta MasurareDocument16 pagesRezilienta Masuraresarara1No ratings yet
- Resiliency TheoryDocument8 pagesResiliency Theorysarara1No ratings yet
- Resilience in SchoolDocument21 pagesResilience in Schoolsarara1No ratings yet
- Pubhealthrep00100 0085Document8 pagesPubhealthrep00100 0085Ioana JecanNo ratings yet
- Anger and Reactive Agression ArticolDocument20 pagesAnger and Reactive Agression Articolsarara1No ratings yet
- Basic Emotions PECSDocument0 pagesBasic Emotions PECSsarara1No ratings yet
- Aikido Exercises For Teaching and Training (Quality Book Copy)Document82 pagesAikido Exercises For Teaching and Training (Quality Book Copy)sarara1100% (1)
- Pan or The DevilDocument8 pagesPan or The DevilMarguerite and Leni Johnson100% (1)
- Preventing Stroke PointsDocument2 pagesPreventing Stroke PointsGermán Mariano Torrez GNo ratings yet
- 5 Job Interview Tips For IntrovertsDocument5 pages5 Job Interview Tips For IntrovertsSendhil RevuluriNo ratings yet
- Thematic Language-Stimulation TherapyDocument19 pagesThematic Language-Stimulation TherapyPipa Yau100% (1)
- Women &literatureDocument54 pagesWomen &literatureAicha ZianeNo ratings yet
- Conversations With Scientists Initiates Brain and Technology UpdateDocument48 pagesConversations With Scientists Initiates Brain and Technology UpdateJorge Baca LopezNo ratings yet
- Scan To Folder Easy Setup GuideDocument20 pagesScan To Folder Easy Setup GuideJuliana PachecoNo ratings yet
- Literature Review 2.1. Shodhana A. Ayurvedic System of ShodhanaDocument93 pagesLiterature Review 2.1. Shodhana A. Ayurvedic System of ShodhanasiesmannNo ratings yet
- ABC Pre School: (Please Refer Advertisement in This Section)Document5 pagesABC Pre School: (Please Refer Advertisement in This Section)hemacrcNo ratings yet
- How The Government Was Formed After Prophet MuhammadDocument48 pagesHow The Government Was Formed After Prophet MuhammadMUSALMAN BHAINo ratings yet
- (1964) AC 763 Help: House of Lords Chandler and OthersDocument22 pages(1964) AC 763 Help: House of Lords Chandler and OthersShehzad HaiderNo ratings yet
- 5 Reasons To Exercise PDFReadingDocument2 pages5 Reasons To Exercise PDFReadingMỹ HàNo ratings yet
- 7 Day Diet AnalysisDocument5 pages7 Day Diet AnalysislipakevinNo ratings yet
- ME8513 & Metrology and Measurements LaboratoryDocument3 pagesME8513 & Metrology and Measurements LaboratorySakthivel KarunakaranNo ratings yet
- Oracle Induction - Introduction Foot Print and Instances For Perfect ExecutionDocument11 pagesOracle Induction - Introduction Foot Print and Instances For Perfect Executioneuge_prime2001No ratings yet
- Business Communication - Case - Josh Miller Is A Finance Student - 2Document4 pagesBusiness Communication - Case - Josh Miller Is A Finance Student - 2Sailpoint CourseNo ratings yet
- AC413 Operations Auditing Outline & ContentDocument29 pagesAC413 Operations Auditing Outline & ContentErlie CabralNo ratings yet
- Communicative Approach - ChomskyDocument4 pagesCommunicative Approach - ChomskyMiss AbrilNo ratings yet
- Personnel ManagementDocument3 pagesPersonnel ManagementmicomiNo ratings yet
- Sap HCM loclalization-EGDocument124 pagesSap HCM loclalization-EGrania abdelghanyNo ratings yet
- Dentsply Sirona Q2 Earnings Presentation - FINALDocument18 pagesDentsply Sirona Q2 Earnings Presentation - FINALmedtechyNo ratings yet
- Analogs of Quantum Hall Effect Edge States in Photonic CrystalsDocument23 pagesAnalogs of Quantum Hall Effect Edge States in Photonic CrystalsSangat BaikNo ratings yet
- Psychotherapy Relationships That Work: Volume 1: Evidence-Based Therapist ContributionsDocument715 pagesPsychotherapy Relationships That Work: Volume 1: Evidence-Based Therapist ContributionsErick de Oliveira Tavares100% (5)
- QDEGNSWDocument2 pagesQDEGNSWSnehin PoddarNo ratings yet
- Group 2Document3 pagesGroup 2sharmisthahalder21No ratings yet
- Rietveld Made Easy - OverviewDocument3 pagesRietveld Made Easy - Overviewhp2020No ratings yet
- PSCAD Power System Lab ManualDocument23 pagesPSCAD Power System Lab ManualShiva Kumar100% (2)
- Motivation and Frustration: Understanding the Causes and Types of ConflictDocument6 pagesMotivation and Frustration: Understanding the Causes and Types of ConflictKamlakar Sadavarte100% (1)
- Daß Ich Erkenne, Was Die Welt Im Innersten Zusammenhält (Lines 382-83) So That I Know What Holds The Innermost World TogetherDocument2 pagesDaß Ich Erkenne, Was Die Welt Im Innersten Zusammenhält (Lines 382-83) So That I Know What Holds The Innermost World TogetherEmanuel MoşmanuNo ratings yet
- Objective/Multiple Type QuestionDocument14 pagesObjective/Multiple Type QuestionMITALI TAKIAR100% (1)