You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Pure HeartDocument72 pagesPure HeartSrilatha VangaruNo ratings yet
- Cc12sas Access ImportDocument5 pagesCc12sas Access ImportSrilatha VangaruNo ratings yet
- Crossover Design Fiction ManuscriptDocument4 pagesCrossover Design Fiction ManuscriptSrilatha VangaruNo ratings yet
- Piping PDFDocument46 pagesPiping PDFGORO43100% (1)
- The Nakshatra of Vedic AstrologyDocument9 pagesThe Nakshatra of Vedic Astrologyashishbhagoria100% (1)
- Accenture Clinical Trial Management Enabling Operational EfficiencyDocument20 pagesAccenture Clinical Trial Management Enabling Operational EfficiencySrilatha Vangaru100% (1)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- (20100401) Stryker Spin Boldak Report MinDocument90 pages(20100401) Stryker Spin Boldak Report MinNoel Jameel AbdullahNo ratings yet
- Creative Associates International Inc. (CAII) : Career ObjectivesDocument3 pagesCreative Associates International Inc. (CAII) : Career Objectiveszohra jamaliNo ratings yet
- NEDA-ODA Review Main Report (2009)Document38 pagesNEDA-ODA Review Main Report (2009)ivy4iskoNo ratings yet
- Barangay Resolution (Not Final) LandaDocument4 pagesBarangay Resolution (Not Final) LandaHaa Lim DimacanganNo ratings yet
- Donor MappingDocument4 pagesDonor MappingIbrahimHatibuNo ratings yet
- Audit Firm Assessment Questionnaire - INDIADocument32 pagesAudit Firm Assessment Questionnaire - INDIARicha SachdevaNo ratings yet
- Producing Gari From CassavaDocument32 pagesProducing Gari From Cassavaparna71100% (1)
- PR3.2.7.3 Contractor Employee Bio Data SheetDocument2 pagesPR3.2.7.3 Contractor Employee Bio Data Sheetali_tumraniNo ratings yet
- Feed The Future and IrrigationDocument66 pagesFeed The Future and IrrigationGetu TadesseNo ratings yet
- Annex A: Technical Application Template: Amanat Afghanistan USAID CONTRACT NUMBER AID-306-H-17-00003Document34 pagesAnnex A: Technical Application Template: Amanat Afghanistan USAID CONTRACT NUMBER AID-306-H-17-00003wafiullah sayedNo ratings yet
- Close Out Guide For USAID ProjectsDocument43 pagesClose Out Guide For USAID Projectsokulluocen100% (1)
- Story BookDocument138 pagesStory BookPergie Acabo Telarma100% (1)
- FY24 State Foreign Operations and Related Programs - Bill SummaryDocument10 pagesFY24 State Foreign Operations and Related Programs - Bill SummaryKyle Becker100% (1)
- AVERT PD AD 12 Aug 08Document3 pagesAVERT PD AD 12 Aug 08scuds85No ratings yet
- WFP - Building Resilience Through Asset CreationDocument24 pagesWFP - Building Resilience Through Asset CreationKevin YaptencoNo ratings yet
- Mozambique: Language OF Instruction Country ProfileDocument14 pagesMozambique: Language OF Instruction Country ProfileSamuel EkpoNo ratings yet
- P 11 FormDocument13 pagesP 11 FormRaj K PandeyNo ratings yet
- Monawar CVDocument3 pagesMonawar CVArman Hossain WarsiNo ratings yet
- Our Mendicant Foreign PolicyDocument18 pagesOur Mendicant Foreign PolicySteve B. Salonga100% (2)
- Child Welfare and Social Work in Africa 508 1.15.10Document66 pagesChild Welfare and Social Work in Africa 508 1.15.10Harsha RamchurnNo ratings yet
- VSF Germany South Sudan livestock assessmentDocument1 pageVSF Germany South Sudan livestock assessmentJohn Michael KuolNo ratings yet
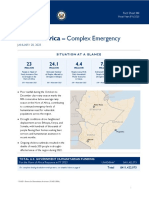
- 2023-01-20 USG Horn of Africa Complex Emergency Fact Sheet 4 0Document6 pages2023-01-20 USG Horn of Africa Complex Emergency Fact Sheet 4 0Suad AbdulmajedNo ratings yet
- US Nation-Building in Afghanistan: Conor KeaneDocument257 pagesUS Nation-Building in Afghanistan: Conor KeaneSyed AbdiNo ratings yet
- Gap Analysis in EgyptDocument369 pagesGap Analysis in EgyptRosaline Lo0% (1)
- Biodata Forms CVsDocument25 pagesBiodata Forms CVsLaurie MoyNo ratings yet
- Notice: Meetings: Board For International Food and Agricultural Development One Hundred and Fifty-Third MeetingDocument2 pagesNotice: Meetings: Board For International Food and Agricultural Development One Hundred and Fifty-Third MeetingJustia.comNo ratings yet
- Web-English ROA Report 2010Document304 pagesWeb-English ROA Report 2010junvNo ratings yet
- The Standard - 2014-07-25Document104 pagesThe Standard - 2014-07-25jorina807No ratings yet
- Evaluation of The World Bank Group Program in AfghanistanDocument287 pagesEvaluation of The World Bank Group Program in AfghanistanIndependent Evaluation GroupNo ratings yet
- Peace Corps Small Project Assistance Program USAID Activities Report 1994Document135 pagesPeace Corps Small Project Assistance Program USAID Activities Report 1994Accessible Journal Media: Peace Corps Documents100% (1)