I.
INTRODUCTION A client diagnosed with Bipolar I disorder, such as Mary Ann Garces, intrigues and challenged the student nurses to applying onto the practical field, their acquired knowledge, attitude and skills from preceding lessons in order to function as an operative and effective member of the multidisciplinary team. he group members are
determined to broaden their knowledge concerning the disorder, particularly in the various methods in which they are supposed to interact with the patient, utili!ing the various appropriate therapeutic approaches, therefore rendering holistic caring care to the said client. he group also aspires to gain a concrete and total e"emplar of the treatment of the disease condition, having only encountered such condition in te"ts. Also, the group feels that and successful intervention is crucial during manifestations of signs and symptoms of the Bipolar I disorder so as to ensure that the client will not have difficulties in functioning in his daily life. If the students are to be efficient nurses, the student nurses should be educated in such matters. Bipolar disorder is a recurrent illness that involves long#term, drastic changes in mood. A person with bipolar disorder e"periences alternating highs $mania% and lows $depression%. A manic period can be brief, lasting from three to fourteen days, or longer, lasting up to several weeks. he depressive periods may also last from days to weeks or even si" to nine months. he periods of mania and depression range from person to person many people may only e"perience very brief periods of these intense moods, and may not even be aware that they have bipolar disorder. he &highs' or manic episodes are characteri!ed by e"treme happiness, hyperactivity, little need for sleep and racing thoughts, which may lead to rapid speech. (ymptoms of the &lows' or depressive periods include e"treme sadness, a lack of energy or )
interest in things, an inability to en*oy normally pleasurable activities and feelings of helplessness and hopelessness. +n average, someone with bipolar disorder has three years of normal mood between episodes of mania or depression. hose with bipolar disorder often describe their e"perience as being on an emotional roller coaster. ,ycling up and down between strong emotions can keep a person from functioning normally. he emotions, thoughts and behavior of a person with bipolar
disorder are beyond his control friends, co#workers and family must intervene to protect his interests. his makes the condition e"hausting not only for the sufferer, but for those in
contact with him as well. Bipolar disorder can create many difficulties. Manic episodes can lead to family conflict or financial problems, especially when the person with bipolar disorder appears to behave erratically and irresponsibly. -uring the manic phase, people often become impulsive and act aggressively. his can result in high#risk behavior, such as
repeated into"ication, e"travagant spending and risky se"ual behavior. -uring severe manic or depressed episodes, people with bipolar disorder may have symptoms that overwhelm their ability to deal with reality. his inability to
distinguish reality from unreality results in psychotic symptoms such as hearing voices, paranoia, visual hallucinations, and false beliefs of special powers or identity. hey may
have distressing periods of great sadness alternating with euphoric optimism $a &natural high'% and.or rage that is not typical of the person during periods of wellness. hese abrupt shifts of mood interfere with reason, logic and perception to such a drastic degree that those affected may be unaware of the need for help.
0owever, if left untreated, bipolar disorder can seriously affect every aspect of a person1s life. Identifying the first episode of mania or depression and receiving early treatment is essential to managing bipolar disorder. In most cases, a depressive episode occurs before a manic episode, and many patients are treated initially as if they have ma*or depression. 2sually, the first recogni!ed episode of bipolar disorder is a manic episode. +nce a manic episode occurs, it becomes clearer that the person is suffering from an illness characteri!ed by alternating moods. Because of this difficulty with diagnosis, family history of similar illness and.or episodes is particularly important. 3atients who first seek treatment as a result of a depressed episode may continue to be treated as someone with unipolar depression until a manic episode develops. Ironically, treatment of depressed bipolar patients with antidepressants can trigger a manic episode in some patients. II. OBJECTIVES (tudent#4urse ,entered5 At the end of this case study, the student nurse will be able to5 ). discuss about the personal, social and familial history of the patient /. recall and review on the normal growth and development of an elderly 6. discuss bipolar disorder 7. trace the pathophysiology of bipolar disorder 8. cite the classical signs and symptoms of disorder 9. make use of the nursing process in caring for a patient with disorder :. instruct health teaching to the patient with the disease condition 6
3atient.(ignificant#+thers ,entered5 At the end of this case study, the patient and his significant#others will be able to5 ). establish trust and rapport with the student nurse /. e"press their feelings and concerns with the current condition 6. state the reason for her stay in the institution 7. utili!e coping skills during her stay in the institution 8. e"hibit positive attitude towards the therapeutic treatment regimen 9. carry out activities of daily living such as self#care
III. NURSING ASSESSMENT 1. PERSONAL HISTORY 1.1 Patients Pr !i"e 4ame5 Mary Ann Garces Age5 7) years old (e"5 ;emale ,ivil (tatus5 (ingle 7
<eligion5 <oman ,atholic -ate of Admission5 =ard5 3sychiatric =aling#=aling =ard Impression. -iagnosis5 Bipolar I -isorder Manic 3hase 3hysician5 -r. 1.# $a%i"& an' In'i(i')a" In! r%ati n he client originally came from alisay ,ity, ,ebu. (he has / sisters of whom she claims are now in Manila. 3rior to her stay in the institution, the client had been drinking / liters of 3epsi ,ola. (he had been admitted to the instituition by her mother to a mischievious conduct of hers. ;urther e"amination in the instituon revealed that the patient had Bipolar -isorder I Manic 3hase. -uring her stay in the 3sychiatric =ard, the client had received visits coming from her family. (he have many friends in the instituition and had known a lot of patients in their. 1.* Le(e" ! Gr +t, an' De(e" -%ent 1.*.1 N r%a" De(e" -%ent .E"'er"&/ PHYSICAL DEVELOPMENT -ramatic physical changes occurs among elder people. heir physical appearance changes in a way which is obvious. (uch changes include that of their skin which has become dry and wrinkled and in some presence of age spots are seen. =hite hair and hair loss are also evident among the elderly. he development of presbyopia and 8
presbycusis are also noted and such has resulted to difficulties of the elderly in maintaing theie activites of daily living. As for the functions of the several systems in the body such as the cradiovascular, neurological and gastrointestinal systems, their functional capability decreases due to the efffect of the aging process. (uch is evident in cases of dementia, confusion, frequent constipation and cardiovascular problems occuring during the old age. PSYCHOSOCIAL DEVELOPMENT >ric >rikson Acquiring a Sense of Integrity While Avoiding Despair $+ld Age% As the aging process creates physical and social losses, the adult may also suffer loss of status and function, such as through retirement or illness. hese e"ternal
struggles are also met with internal struggles such as the search for meaning of life. Meeting these challenges creates the potential for growth and wisdom. Many elders view their lives with a sense of satisfaction even with the inevitable mistakes. +thers see themselves as failures with marked attempt and disgust. MORAL DEVELOPMENT Universal Ethical Principle Orientation his stage defines &right' by the decision of conscience in accord with self# chosen#ethical principles. hese principles are abstract, like the golden rule and appeal to logical comprehensiveness, universality and consistency. It also defines the principles by which agreement will be most *ust. COGNITIVE DEVELOPMENT 9
3eriod I?5 Formal Operations =ith the individual@s thinking moves to abstract and theoritical sub*ects in the formal operation period, thinking can venture into such sub*ects as achieving world peace, finding *ustice and seeking meaning in life. 1.*.# T,e i"" -ers n at -arti0)"ar sta1e ! t,e 0"ient Bipolar disorder causes dramatic mood swingsAfrom overly BhighB and.or irritable to sad and hopeless, and then back again, often with periods of normal mood in between. (evere changes in energy and behavior go along with these changes in mood. he periods of highs and lows are called episodes of mania and depression. 1.*.* A0t)a" I"" Be,a(i r Increased energy, activity, and restlessness >"cessively Bhigh,B overly good, euphoric mood >"treme irritability <acing thoughts and talking very fast, *umping from one idea to another -istractibility, can@t concentrate well Cittle sleep needed 2nrealistic beliefs in one@s abilities and powers 3oor *udgment (pending sprees :
A lasting period of behavior that is different from usual Abuse of drugs, particularly cocaine, alcohol, and sleeping medications 3rovocative, intrusive, or aggressive behavior -enial that anything is wrong
A manic episode is diagnosed if elevated mood occurs with three or more of the other symptoms most of the day, nearly every day, for ) week or longer. If the mood is irritable, four additional symptoms must be present. (igns and symptoms of depression $or a depressive episode% include5 Casting sad, an"ious, or empty mood ;eelings of hopelessness or pessimism ;eelings of guilt, worthlessness, or helplessness Coss of interest or pleasure in activities once en*oyed, including se" -ecreased energy, a feeling of fatigue or of being Bslowed downB -ifficulty concentrating, remembering, making decisions <estlessness or irritability (leeping too much, or can@t sleep ,hange in appetite and.or unintended weight loss or gain
,hronic pain or other persistent bodily symptoms that are not caused by physical illness or in*ury
houghts of death or suicide, or suicide attempts
A depressive episode is diagnosed if five or more of these symptoms last most of the day, nearly every day, for a period of / weeks or longer. A mild to moderate level of mania is called hypomania. 0ypomania may feel good to the person who e"periences it and may even be associated with good functioning and enhanced productivity. hus even when family and friends learn to recogni!e the mood swings as possible bipolar disorder, the person may deny that anything is wrong. =ithout proper treatment, however, hypomania can become severe mania in some people or can switch into depression.
DIAGNOSIS A physician makes this diagnosis based on the patient@s symptoms. +ther conditions that might also cause these symptoms will be considered and ruled out. he
patient@s medical history, including whether there have been previous episodes of mental illness, will be evaluated. ;amily medical history, particularly of mood disorders, is important information. Blood tests are not routine at present but are being researched as a future aid in diagnosing.
CAUSES here are several different pathways into the set of symptoms given the diagnosis BBipolar Affective -isorderB. Among the e"planations indicated by research and generally accepted are the following5 ). Genetic abnormalities, Bipolar affective disorder has clearly been shown to run in families. $Genetic abnormalities on chromosomes )D and /) are suspected.% /. ,hemical imbalance in the brain, particularly related to leaking membranes in the pathways used for delivering messages within the brain. 6. A sei!ure disorder in the brain@s frontal corte". 4o convulsions occur with frontal corte" sei!ures because there are no psycho#motor centers located in the frontal corte". (ei!ures occurring in this area affect mood and *udgment. *. Present -r !i"e ! $)n0ti na" Hea"t, Patterns 6.) 0ealth 3erception. 0ealth Management 3attern he client despite her current condition does not have any vitamins and only recieves a monthly dose of an antipsychotic drugs monthly. (he claims that she is not well and when asked why she is in the institution, laughs and says that she does know. 6./ 4utritional# Metabolic 3attern he client eats what the instituition has to offer, from breakfast to dinner. +ccassionaly, she ate foods given by student nurses. 2nfortunately, such foods are not that nutricious to meet her metabolic needs as evidenced by her pale color and her body built. 6.6 >limination 3attern )F
he client normally defecates once every day. ;or her urination, she verbali!ed to urinate at least 7 times a day. 6.7 Activity# >"ercise 3attern 0er activity# e"ercise pattern greatly depends on her mood. -uring our time with her, there are days when she actively *oin the activities prepared by the student nurses and en*oys walking in the grounds. =hile in some days, the client all wants is to sit down in her place and remains away from the company of others. 6.8 ,ognitive 3erceptual 3attern he client cognitive and perceptual pattern is distorted, especially in cases mood swings. (he falsely believes that they are all artists and that they had a show. (he also had misperceptions of having a store in front of her which in reality is *ust a window. (he@s also oriented to time and date.
6.9 (leep#<est 3attern As been claimed by the client, she doesn1t sleeps well during night which starts from around )F pm # 8 am. -uring the afternoons, she naps a liittle bit. 6.: (elf#3erception 3attern he client sees herself as a well individual and says that nothing is wrong. (he oftenly says that she speaks with the resident physician with regards to her stay in the institution. ))
6.D <ole#<elationship 3attern here are problems with the client@s relationship to others. his had been due to her
condition and the sign and symptoms accompanying it. -uring her stay in the institution, there had been visits coming from her family. As to her relationship with fellow clients in the instituition, she does have close friends. 6.E (e"uality#(e"ual ;unctioning he client is an elder woman who long time had her menopausal. (he is single and doesn@t have any children at all. 6.)F ,oping#(tress Management 3attern he client whenever provoked or when she hears unpleasant things, easily gets angry and irritable. o cope up, she frequently shouts to the people around her and when she@s happy, she *oins with the activities prepared by student#nurses.
6.)) ?alue#Belief (ystem
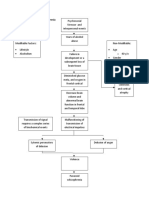
2. PATHOPHYSIOLOGY AND RATIONALE 2.1. Anat %& an' P,&si " 1& ! Or1an3S&ste% a!!e0te' ). 4ervous system )/
hree basic functions are performed by nervous systems5 ). <eceive sensory input from internal and e"ternal environments /. Integrate the input 6. <espond to stimuli Sens r& In-)t <eceptors are parts of the nervous system that sense changes in the internal or e"ternal environments. (ensory input can be in many forms, including pressure, taste, sound, light, blood p0, or hormone levels that are converted to a signal and sent to the brain or spinal cord. Inte1rati n an' O)t-)t In the sensory centers of the brain or in the spinal cord, the barrage of input is integrated and a response is generated. he response, a motor output, is a signal transmitted to
organs than can convert the signal into some form of action, such as movement, changes in heart rate, release of hormones, etc. Di(isi ns ! t,e Ner( )s S&ste% he nervous system monitors and controls almost every organ system through a series of positive and negative feedback loops. brain and spinal cord. he ,entral 4ervous (ystem $,4(% includes the
he 3eripheral 4ervous (ystem $34(% connects the ,4( to other
parts of the body, and is composed of nerves $bundles of neurons%. Peri-,era" Ner( )s S&ste%
)6
he peripheral nervous system consists of the nerves that branch out from the brain and spinal cord. hese nerves form the communication network between the ,4( and the body parts. he peripheral nervous system is further subdivided into the somatic nervous system and the autonomic nervous system. he somatic nervous system consists of nerves that go to the skin and muscles and is involved in conscious activities. he autonomic nervous
system consists of nerves that connect the ,4( to the visceral organs such as the heart, stomach, and intestines. It mediates unconscious activities. wo main components of the 34(5 ). (ensory $afferent% pathways that provide input from the body into the ,4(. /. Motor $efferent% pathways that carry signals to muscles and glands $effectors%. Most sensory input carried in the 34( remains below the level of conscious awareness. Input that does reach the conscious level contributes to perception of our e"ternal environment.
A)t n %i0 ner( )s s&ste% he autonomic nervous system is a visceral efferent system, which means it sends motor impulses to the visceral organs. It functions automatically and continuously, without conscious effort, to innervate smooth muscle, cardiac muscle, and glands. It is concerned with heart rate, breathing rate, blood pressure, body temperature, and other visceral activities that work together to maintain homeostasis. )7
he autonomic nervous system has two parts, the sympathetic division and the parasympathetic division. Many visceral organs are supplied with fibers from both divisions. In this case, one stimulates and the other inhibits. his antagonistic functional relationship serves as a balance to help maintain homeostasis. S %ati0 Ner( )s S&ste% he (omatic 4ervous (ystem $(4(% includes all nerves controlling the muscular system and e"ternal sensory receptors. >"ternal sense organs $including skin% are receptors. Muscle fibers and gland cells are effectors. he refle" arc is an automatic, involuntary
reaction to a stimulus. =hen the doctor taps your knee with the rubber hammer, she.he is testing your refle" $or knee#*erk%. he reaction to the stimulus is involuntary, with the ,4( being informed but not consciously controlling the response. >"amples of refle" arcs include balance, the blinking refle", and the stretch refle". (ensory input from the 34( is processed by the ,4( and responses are sent by the 34( from the ,4( to the organs of the body. Motor neurons of the somatic system are distinct from those of the autonomic system. Inhibitory signals cannot be sent through the motor neurons of the somatic system. Centra" Ner( )s S&ste% he ,entral 4ervous (ystem $,4(% is composed of the brain and spinal cord. he ,4( is surrounded by bone#skull and vertebrae. ;luid and tissue also insulate the brain and spinal cord.
)8
he brain is composed of three parts5 the cerebrum $seat of consciousness%, the cerebellum, and the medulla oblongata $these latter two are Bpart of the unconscious brainB%. he medulla oblongata is closest to the spinal cord, and is involved with the regulation of heartbeat, breathing, vasoconstriction $blood pressure%, and refle" centers for vomiting, coughing, snee!ing, swallowing, and hiccuping. he hypothalamus regulates homeostasis. It has regulatory areas for thirst, hunger, body temperature, water balance, and blood pressure, and links the 4ervous (ystem to the >ndocrine (ystem. he midbrain and pons are also part of the unconscious brain. incoming nervous messages. he cerebellum is the second largest part of the brain, after the cerebrum. It functions for muscle coordination and maintains normal muscle tone and posture. coordinates balance. he conscious brain includes the cerebral hemispheres, which are are separated by the corpus callosum. In reptiles, birds, and mammals, the cerebrum coordinates sensory data and motor functions. he cerebrum governs intelligence and reasoning, learning and he cerebellum he thalamus serves as a central relay point for
memory. =hile the cause of memory is not yet definitely known, studies on slugs indicate learning is accompanied by a synapse decrease. =ithin the cell, learning involves change in gene regulation and increased ability to secrete transmitters. T,e Brain Most brains e"hibit a substantial distinction between the gray matter and white matter. Gray matter consists primarily of the cell bodies of the neurons, while white matter is comprised mostly of the fibers $a"ons% which connect neurons. he a"ons are surrounded by a fatty )9
insulating sheath called myelin $oligodendroglia cells%, giving the white matter its distinctive color. he outer layer of the brain is gray matter called cerebral corte". -eep in the brain, compartments of white matter $fasciculi, fiber tracts%, gray matter $nuclei% and spaces filled with cerebrospinal fluid $ventricles% are found. he brain innervates the head through cranial nerves, and it communicates with the spinal cord, which innervates the body through spinal nerves. 4ervous fibers transmitting signals from the brain are called efferent fibers. he fibers transmitting signals to the brain are
called afferent $or sensory% fibers. 4erves can be afferent, efferent or mi"ed $i.e., containing both types of fibers%. he brain is the site of reason and intelligence, which include such components as cognition, perception, attention, memory and emotion. he brain is also responsible for
control of posture and movements. It makes possible cognitive, motor and other forms of learning. he brain can perform a variety of functions automatically, without the need for
conscious awareness, such as coordination of sensory systems $eg. sensory gating and multisensory integration%, walking, and homeostatic body functions such as heart rate, blood pressure, fluid balance, and body temperature. Many functions are controlled by coordinated activity of the brain and spinal cord. Moreover, some behaviors such as simple refle"es and basic locomotion, can be e"ecuted under spinal cord control alone. he brain undergoes transitions from wakefulness to sleep $and subtypes of these states%. hese state transitions are crucially important for proper brain functioning. $;or e"ample, it is believed that sleep is important for knowledge consolidation, as the neurons appear to organi!e the day@s stimuli during deep sleep by randomly firing off the most recently used ):
neuron pathwaysG additionally, without sleep, normal sub*ects are observed to develop symptoms resembling mental illness, even auditory hallucinations%. >very brain state is associated with characteristic brain waves. T,e $ re4rain he forebrain is the largest and most comple" part of the brain. It consists of the cerebrum # the area with all the folds and grooves typically seen in pictures of the brain # as well as some other structures beneath it. he cerebrum contains the information that essentially makes us who we are5 our intelligence, memory, personality, emotion, speech, and ability to feel and move. (pecific areas of the cerebrum are in charge of processing these different types of information. hese are called lobes, and there are four of them5 the frontal, parietal, temporal, and occipital. he cerebrum has right and left halves, called hemispheres, which are connected in the middle by a band of nerve fibers $the corpus collosum% that enables the two sides to communicate. hough these halves may look like mirror images of each other, many he left side is considered the logical,
scientists believe they have different functions. analytical, ob*ective side.
he right side is thought to be more intuitive, creative, and
sub*ective. (o when you@re balancing the checkbook, you@re using the left sideG when you@re listening to music, you@re using the right side. It@s believed that some people are more Bright# brainedB or Bleft#brainedB while others are more Bwhole#brained,B meaning they use both halves of their brain to the same degree. he outer layer of the cerebrum is called the corte" $also known as Bgray matterB%. Information collected by the five senses comes into the brain from the spinal cord to the )D
corte".
his information is then directed to other parts of the nervous system for further
processing. ;or e"ample, when you touch the hot stove, not only does a message go out to move your hand but one also goes to another part of the brain to help you remember not to do that again. In the inner part of the forebrain sits the thalamus, hypothalamus, and pituitary gland. he thalamus carries messages from the sensory organs like the eyes, ears, nose, and fingers to the corte". he hypothalamus controls the pulse, thirst, appetite, sleep patterns, and
other processes in our bodies that happen automatically. It also controls the pituitary gland, which makes the hormones that control our growth, metabolism, digestion, se"ual maturity, and response to stress. T,e Mi'4rain he midbrain, located underneath the middle of the forebrain, acts as a master coordinator for all the messages going in and out of the brain to the spinal cord. T,e Hin'4rain he hindbrain sits underneath the back end of the cerebrum, and it consists of the cerebellum, pons, and medulla. he cerebellum # also called the Blittle brainB because it
looks like a small version of the cerebrum # is responsible for balance, movement, and coordination. he pons and the medulla, along with the midbrain, are often called the brainstem. he
brainstem takes in, sends out, and coordinates all of the brain@s messages. It is also controls many of the body@s automatic functions, like breathing, heart rate, blood pressure, swallowing, digestion, and blinking. )E
T,e S-ina" C r' he spinal cord runs along the dorsal side of the body and links the brain to the rest of the body. ?ertebrates have their spinal cords encased in a series of $usually% bony vertebrae that comprise the vertebral column. he gray matter of the spinal cord consists mostly of cell bodies and dendrites. he
surrounding white matter is made up of bundles of interneuronal a"ons $tracts%. (ome tracts are ascending $carrying messages to the brain%, others are descending $carrying messages from the brain%. he spinal cord is also involved in refle"es that do not immediately involve the brain. T,e Brain an' Dr)1s (ome neurotransmitters are e"citory, such as acetylcholine, norepinephrine, serotonin, and dopamine. (ome are associated with rela"ation, such as dopamine and serotonin. -opamine release seems related to sensations of pleasure. >ndorphins are natural opioids that produce elation and reduction of pain, as do artificial chemicals such as opium and heroin. 4eurological diseases, for e"ample 3arkinson@s disease and 0untington@s disease, are due to imbalances of neurotransmitters. 3arkinson@s is due to a dopamine deficiency. 0untington@s disease is thought to be cause by malfunctioning of an inhibitory neurotransmitter. Al!heimer@s disease is associated with protein plaques in the brain. -rugs are stimulants or depressants that block or enhance certain neurotransmitters. -opamine is thought involved with all forms of pleasure. ,ocaine interferes with uptake of dopamine from the synaptic cleft. Alcohol causes a euphoric BhighB followed by a depression. /F
Mari*uana, material from the Indian hemp plant $,annabis sativa%, has a potent chemical 0, $tetrahydracannibinol% that in low, concentrations causes a euphoric high $if inhaled, the most common form of action is smoke inhalation%. 0igh dosages may cause severe effects such as hallucinations, an"iety, depression, and psychotic symptoms. ,ocaine is derives from the plant >rtho"ylon coca Inhaled, smoked or in*ected. ,ocaine users report a BrushB of euphoria following use. ;ollowing the rush is a short $8#6F minute% period of arousal followed by a depression. <epeated cycle of use terminate in a BcrashB when the cocaine is gone. 3rolonged used causes production of less dopamine, causing the user to need more of the drug. 0eroin is a derivative of morphine, which in turn is obtained from opium, the milky secretions obtained from the opium poppy, 3apaver somniferum. 0eroin is usually in*ected intravenously, although snorting and smoking serve as alternative delivery methods. 0eroin binds to opioid receptors in the brain, where the natural chemical endorphins are involved in the cessation pain. 0eroin is physically addictive, and prolonged use causes less endorphin production. +nce this happens, the euphoria is no longer felt, only dependence and delay of withdrawal symptoms.
C"assi0a" S&%-t %
C"ini0a" S&%-t %
Rati na"e
/)
BIPOLAR DISORDER TYPE II
3recipitating ;actors stress social status psychosocial
3redisposing ;actors genetics biogenic amines cardiac dysfunction //
PSYCHODYNAMICS 1. Si1%)n' $re)'s Ps&0, ana"&ti0a" T,e r&
/6
+ne of the leading psychoanalytical theories concerning depression was first proposed by (igmund ;reud. ;reud argued that at some point in early childhood, the depressed patient suffered the loss, real or imagined, of someone with whom they were very close. Moreover, the individual depended on that other person to maintain his.her self# esteem. 2nable to cope with the loss, the person then creates an internal representation of the lost individual so that they can maintain the close relationship. Anger begins to develop to develop towards the lost individual, but since this anger is not recogni!ed and dealt with on a conscious level and since the ob*ect is internali!ed, the person directs the feelings toward him# or herself. #. Be05s C 1niti(e M 'e" Beck proposed that the depressed individual@s tendency to e"press more negativity than non#depressed individuals is derived from his or her cognitive distortions, or erroneous ways, of thinking about the self. 4egative and derogatory views of the self, the world, and of the future are core features of the depressed individual. More specifically, a depressed individual tends to attribute global, personali!ed reasons for failure, form overarching principles of the self based on negative e"periences, to e"aggerate negative events and dismiss positive events, and to selectively recall more negative events. +ne could then say that these self#defeating biases lead to the development of a cognitive schema that affects the way the individual interprets, perceives, and interacts with the environment. his negative schema in turn increases the probability of the individual being more negatively affected by stressful life events. *. Se"i1%ans Learne' ,e"-"essness6H -e"essness T,e r&
/7
(eligman suggested that depression was similar to the passive behavior shown by animals that had been e"posed to shock. -epressed individuals, then, like the animals in the lab e"periments, begin to believe that they are helpless##that they do not have the power to control the events in their lives. hey therefore fail to reali!e the
contingency between their actions and the outcome of events. Cearned#helplessness theory, in an attempt to answer some of the criticisms rose against it, such as the fact that most people do not become depressed after e"periencing a negative life event, was later revised and described instead in terms of Bhopelessness.B C. H. Abramson and his colleagues proposed that individuals who are vulnerable to depression possess an attribution style consisting of negative e"pectations concerning future events, regardless of their own actions. After the occurrence of a negative life event, the causal attribution $e"planations and importance% that the person ascribes to the event is correlated with the probability of then becoming depressed. his attribution style also consists of the tendency to e"plain negative events as internal, stable, and global factors. his means that unlike
non#depressed individuals, a depressed person is more likely to think of negative events as proof of their own inadequacies $internal%, as having e"isted in the past and continuing to persist in the future $stable%, and responsible for his or her failure in other areas of life $global%. 2. O47e0t L ss T,e r& Is the idea that the alleged to be universal emotional states that are ma*or building blocks of the personality ego#self e"ists only in relation to other ob*ects which may be e"ternal or internal. Internal ob*ects are internali!ed versions of e"ternal ob*ects, primarily formed from early interactions with the parents. According to ob*ect#relations theory there are three fundamental BaffectsB that can e"ist between the self and the other # /8
attachment, frustration, and re*ection. hese affects are alleged to be universal emotional states that are ma*or building blocks of the personality. 8. Pers na"it& Or1ani9ati n T,e r& (ubtle differences in neurotransmitter availability and re#uptake vary the sensitivity of individuals to cues about their environment that predict future resource availability and e"ternal rewards and punishments. It is the way these cues are detected, attended to, stored, and integrated with previous e"periences that makes each individual unique. ,urrent work on the bases of individual differences is concerned with understanding this delicate interplay of biological propensities with environmental opportunities and constraints as they are ultimately represented in an individual1s information processing system. =ith time we can e"pect to increase our ta"onomic and predictive power by using these causal bio#social theories of individual differences. T,e Disease Pr 0ess Bipolar -isorder, formerly known as manic#depression, is a diagnosis in psychiatry referring to mania $or hypomania or mi"ed states% alternating with clinical depression $or depressed or euthymic mood% over a significant period of time. 2nlike highs and lows a normal person might e"perience, one with bipolar disorder e"periences e"treme mood swings that can last for minutes to months. Mood changes of this nature are associated with distress and disruption, and a relatively high risk of suicide. -isorder is commonly categori!ed as either Bipolar I or Bipolar
ype I, where an individual
e"periences full#blown mania, or Bipolar II or ype II, in which the BhighsB do not go beyond hypomania $unless triggered in to mania by medication%. he latter is much more difficult to diagnose, since the hypomanic episodes may simply appear as a period of successful high /9
productivity. 3sychosis can occur, particularly in manic periods.
here are also @rapid
cycling@ subtypes. Because there is so much variation in the severity and nature of mood# related problems, the concept of a bipolar spectrum is often employed, which includes cyclothymia. here is no consensus as to how many @types@ of bipolar disorder e"ist. Many patients with bipolar disorder suffer from severe an"iety and panic when in a manic state, while others are euphoric. (ome do not e"perience full#blown mania, and will display milder symptoms, known as hypomania. -epression medications are often contraindicated for patients with bipolar disorder, as these medications may induce mania and worsen the disorder. In addition, many patients with bipolar disorder are inaccurately diagnosed with unipolar depression $clinical depression%, further complicating diagnosis. In fact, it often takes more than a decade before patients are accurately diagnosed and treated for their bipolar disorder. NURSING INTERVENTIONS a. Care G)i'e ! C"ients +it, Bi- "ar II 'is r'er De-ressi(e state ry to sit beside and be in the person1s space I often people who are depressed do not like to make demands on others but they appreciate company. Cikewise, you will need to do the talking rather than e"pecting the person to do so Jeep up good levels of communication even when not reciprocated eg Cet the person know where you are going even if there is no response. 3rovide for the safety of the client and others. Begin a therapeutic relationship by spending non#demanding time with the client. /:
3romote completion of activities of daily living by assisting the client only as necessary
>stablish adequate nutrition and hydration. 3romote sleep and rest. >ngage the client in activities. >ncourage the client to verbali!e and describe the emotion. (et realistic tasks and have realistic e"pectations. Be aware of suicide risk. Ask the appropriate questions and communicate with treating team about this issue. his issue may be a reason for hospitali!ation.
If the person e"presses une"pected happiness and begins to give possessions away, seek assistance immediately.
Avoid placing unrealistic demands on the person. Be patient.
Mani0 state Be calm. -o not participate in the escalation of e"citement. 2se simple, clear communications, and make sure the message has been understood.
/D
Make sure that you move away from potential conflictual situations. 2se their distract ability to come back again.
-o not make too many demands. <educe stimulation and loud noises. Avoid conflict. Jeep the person1s real level of e"pertise in mind. -o not allow yourself to be overly influenced by their persuasive presentation of advice.
his is very tiring so make sure that you get some space, which you will need to regulate for yourself I the other person will not recogni!e your need.
=hen you want space, try to manage your emotional state as the individual will pick up on your distress and you may have to defend yourself, as the person will not see themselves as unreasonable.
Be genuine, try not to turn off. =hen something is funny en*oy it. Be conscious of the safety factor. he danger of physical complications may be one of the trigger factors to indicate the need for hospitali!ation.
<emember it is very easy for this person to end up with disturbed sleep patterns, sleep late and spend half the evening ringing people. Hou may need to seek advice about medication for sleep.
In hot weather, fluid replacement is important, particularly when the person is on lithium. 3eople can become so dehydrated that the blood concentration of lithium /E
increases to such an e"tent that the person can go into a hepatic coma. Cithium also increases sensitivity to sun >ncourage the person to drink small amounts regularly. ,onsider what the person likes to drink and make it easily available. Address nutrition in the same way, thinking of high#energy food. >ncourage the person to have a bath or a shower (ome people suggest warm drinks, but not coffee or tea. his helps the person feel looked after. Be assertive about your own boundaries in a friendly manner <educe access to dangerous situations.
3atient5 Mary Ann Garces ,omplaint5 Bipolar )-isorder NURSING CARE PLAN 4eed.3roblem. 4ursing +b*ectives of (cientific Basis ,ues -iagnosis ,are I. 3sychologic (ensory I Mania is 3erceptual reflected in A. -eficit Alteration5 periods of Inapproriate euphoria, 3erception e"uberant ). Inappropriate of (timuli activity, perception of related to grandiosity and stimuli manic false sense of phase well#being. +b*ective cues5 e"perienced (ome clients manifest mania (topping in . with an midsentences After D# hours of holistic caring#care, the client will be able to5
Age5 7/ years old (e"5 ;emale
4ursing Interventions Measures to minimi!e occurrence of sensory and perceptual misperceptions5
<ationale
). recogni!e ). +bserve client and restate for signs of correctly hallucinations, previously listening pose, interpreted laughing or stimuli talking to self
>arly interventions may prevent aggressive responses to command 6F
while conversing and not continiung statements previously constructed. alking to herself. Mood swings from day to day. ,hanges in usual response to a visual stimuli seen.
aggressive tone and are sarcastic and irritable especially when others set limits on their behavior.
and stopping in hallucinations. midsentece. /. Avoid touching the client before ,lient may warning him or perceive her that you are touch as about to do so. threatening and respond in an aggressive manner. 6. An attitude of acceptance will encourage the client to share the content of the hallucination with you. his is important to prevent possible in*ury to the client or others form command hallucinations.
(ource5 3sychiatric Mental 0ealth 4ursing /nd >d. By (heila C. ?idebeckl p. 689.
(ub*ective ,ues5 ,laims that the another patient who had *ust passed by is the famous actress Imelda 3apin. -isorientation to time and date . &Cantawa ra gud nang nawonga, nawong bag
If client can 7. ry to connect learn to the times of the interrupt the misperceptions escalating an"iety, reality to times of orientation increased an"iety. 0elp may be maintained. client to understand this connection. (o patient 8. -o not reinforce reali!es that the hallucinations hallucinations. are unreal. Involvement in interpersonal 9. ry not to activities and distract the e"ploration in client away the actual from the misperceptions situation may 6)
tindera...' as verbali!ed by the patient when another student nurse had pass by.
bring the client back to reality.
(ource 5
(ource 5
). 4ursing /. 4ursing -iagnoses in -iagnoses 3sychiatric in 4ursing ,are 3sychiatric 3lans and 4ursing 3sychiatric ,are 3lans Medications and th 8 >d. By Mary 3sychiatric ownsend. Medications pp.)ED#/FF. 8th>d. By Mary ownsend. pp.)ED#/FF.
NURSING CARE PLAN 4eed.3roblem. 4ursing +b*ectives of (cientific Basis ,ues -iagnosis ,are /. ;light of Ideas ,ues5 >asily distracted upon first interaction Making statements which are not related to one another <estlessness 6/ Altered hought 3rocess5 ;light of Ideas related to imbalance in biochemical processes. ,ognitive /.differentiate ability or between thinking is reality and confused and unrealistic *umbled with events or thoughts racing situations. one after another. ,lients cannot connect concepts and *ump from one sub*ect to another. 4ursing Interventions Measures to reorient client to reality5 <ationale
). ,onvey your acceptance of the client@s need for the false belief while telling him or her that you do not share the delusion.
A positive response would convey to the client that you accept the delusion as reality.
Answering questions first correctly then suddenly saying things not within conte"t.
(ource5 3sychiatric Mental 0ealth 4ursing /nd >d. By (heila ?idebeck p. 689.
/. -o not argue Arguing with the or deny the client or denying belief. the belief serves no purpose because delusional ideas are not eliminated by this approach and the development of a trusting relationship may be impeded.
6. 2se the technique of consensual validation and seeking clarification when communication reflects alteration in thinking.
hese techniques reveal to the client how she or he is being perceived by others and the responsibility for not understanding is accepted by the nurse.
o divert client 7. 2se real situations ans away from long, tendious, events. <einforce and repetitive focus on reality. verbali!ations of false ideas. 3ositive 8. Give positive reinforcements reinforcement enhances self# as client is able esteem and to differentiate encourages between repetition of reality#based desirable and non#reality# behaviors based thinking. 66
9. each client to intervene, using thought stopping techniques when irrational thoughts prevail.
his noise or command distracts the individual from the undesirable thinking which often precedes undesirable emotions or behaviors.
:. 2se touch ,lients who are cautiously, suspicious may particularly if perceive touch thoughts reveal as threatening ideas of and may premonition. respond with aggression.
(ource 5
(ource 5 4ursing -iagnoses in 3sychiatric 4ursing ,are 3lans and 3sychiatric Medications 8th>d. By Mary ownsend. pp.)E:#)ED
7. 6. 4ursing -iagnoses in 3sychiatric 4ursing ,are 3lans and 3sychiatric Medications 8th>d. By Mary ownsend. pp.)E:#)ED
67
NURSING CARE PLAN 4eed.3roblem 4ursing (cientific Basis +b*ectives 4ursing .,ues -iagnosis of ,are Interventions II. 3hysiologic (elf#,are -eficit 5 A. -eficit Inability to perform hygienic ). Inability to measures perform related to hygienic alterations measures in sensory and thought processes. ,ues5 3resence of long nails in Inattention to hygiene and grooming is common during psychotic episodes. he patient can become so preoccupied with delusions or other hallucinations that she fails to perform even the basic <ationale
Measures to promote self# 6. perform care5 self#care activities ). 3romote with little client enhances assistance participation in commitment to plan, from the problem optimi!ing outcomes student identification nurse. and decision# making.
/. 3lan time for listening
o discover barriers 68
the feet and hands with dirt stuck on it. eeth not brushed well. Bad# smelling breath. 0air is shoulder length, not combed and not tied.
activities of daily living.
to the client.
to participation
(ource5 3sychiatric Mental 0ealth 4ursing /nd ed. By ?idebeck p.6))
6. 3rovide for communicatio >nhances n among those who are coordination and continuity of care involved in caring for the client.
7. Assist with o enhance the rehabilitation capabilities program.
8.3rovide o avoid privacy during embarassment. personal care activities.
9. Assist with o encourage client necessary and build on adaptations to successes. accomplish A-Cs. Begin with familiar, easily accomplished tasks.
(ource G
(ource G
4ursing 4ursing -iagnoses -iagnoses in in 3sychiatric 4ursing 3sychiatric 4ursing ,are ,are 3lans and 69
3lans and 3sychiatric Medications 8th >d. By Mary ownsend. pp.)E:#)ED G>issler I Murr pp.
3sychiatric Medications 8th >d. By Mary ownsend. pp.)E:#)ED
HEALTH TEACHING PLAN +b*ective ,ontent Methodology >valuation
General +b*ective After 8 days of nurse#client interaction the client will be able to gain knowledge, attitude, and skills in caring for person with 3sychologic illness After 78 minutes 6:
of
student
nurse#
client interaction the client will be able to5 ).state proper hygiene the ).Importance of having good hygiene ).) best defense against diseases Informal discussion ,lient looks clean when we met her on the ne"t day.
importance of having
)./ pleasing to look ).6 stress free person is not irritable ).7 proper blood circulation
).8 promotes optimum level of functioning
/.cite hygiene
ways
in
maintaining
proper
/. =ays in maintaining proper hygiene /.) taking a bath /./ brushing teeth /.6 changing clothes everyday /.7 wearing slippers
Informal discussion
,lient is seen brushing her teeth and her fingernails are already short.
6D
/.8 keeping fingernails short 6.enumerate loneliness ways loneliness 6.) listening to music 6./ watching television 6.6 talking with other people 6.7 playing ball games 6.8 playing cards with friends Informal discussion ,lient talks to the student nurses around her.
on how to cope with 6.=ays to cope with
7.demonstrate proper way in taking a bath
7.3roper way in taking a bath 7.) wet your body 7./ apply shampoo and massage your hair properly and rinse 7.6 apply soap and rinse 7.7 wipe your body with a towel until dry
-emonstration and return demonstration
,lient looks clean on the ne"t day we met.
6E
7.8 change dirty clothes with clean one
EVALUATION Ms. Mary Ann Garces, diagnosed of Bipolar I disorder, and based on the client1s medical history and all other assessment data gathered, it was observed that the client manifested and e"perienced certain signs and symptoms of the particular disorder during the investigation and the student nurses conduct this case study. he behavioral findings have proven that the client is mentally ill as evidenced by altered behavior alternating from depression to mania when interacting with the student nurse. (he is aware of what is currently happening in her life. RECOMMENDATION 7F
he psychiatric home staff he researchers recommend to the psychiatric staff that in the care of the client, they should not only be able to provide the clients with their maintained medications as prescribed by the physician, but also to provide the patients with the utmost care that each client needs. he staff should also continue he therapies started by the student nurses to further improve the client1s development. (tudent nurses he researchers would like to recommend to the present and future student nurses to use proper therapeutic communication techniques in dealing with the psychiatric clients. Also, the student nurses must always encourage the clients to actively participate in the different therapies se in order to help them improve the client1s present condition such as remotivation therapy, sensory stimulation therapy, psycho therapy, art therapy, music therapy and dance therapy which aims to provide the relief of the clients aggravation and so as to be able to divert the clients aggravated behavior into a more positive one. VI. IMPLICATIONS O$ CASE STUDY TO: 1. N)rsin1 Pra0ti0e hrough this case study , the researchers hope that present and future nurses in the psychiatric filed of nursing practice will be guided in carrying out psychiatric#related activities of such mentioned disorder and therefore be able to5 collect, report and record accurate Bipolar I disorder offer bipolar I disorder information and resources 7)
participate in ongoing management of patients with bipolar I disorder evaluate and monitor the impact of bipolar I disorder and the treatment on the individual and family
#. N)rsin1 E')0ati n his case study will hopefully improve the health care givers regarding education to the significant others on how to manage these patients and protect them from developing further complications. It provides a broader knowledge on the person1s normal behavior, psychopathology, signs and symptoms, predisposing and precipitating factors, medical and nursing management. It also allows a greater understanding of the patient1s condition since it portrays the actual patient portraying the different signs and symptoms of the disorder. 4urses will be equipped with actual clinical information regarding the predictable outcomes of the disease and its medical nursing management. *. N)rsin1 Resear0, his case study will hopefully encourage nursing research on finding new management which have a faster effect to this kind of condition and can serve as a tool guide or basis for future research on studies concerning about psychosis, which may acquire the researcher, added information about the case of the patient with psychosis. It can hopefully serve as a foundation for present and future nurses in the psychiatric field of nursing practice in rendering effective and holistic caring care to clients with bipolar I disorder.
7/
3<+,>(( <>,+<-I4G 4+. ) I. +b*ectives General5 After / weeks of student nurse patient interaction, the patient will be able to establish rapport and make use of the different adaptive coping mechanisms in dealing stress or crisis. (pecific5 After 78 minutes of student nurse patient interaction, the patient will be able to5 ). introduce self to the student nurse /. establish rapport to the student nurse 6. give information about herself with her past e"periences 76
7. verbali!e feelings about self with her past e"periences 8. set contract with the client II. (etting of Interaction -A >5 4ovember /E, /F)) IM>5 :588 AM I D5)8 AM 3CA,>5 ?icente (otto 3sychiatric ;emale =ard <oom
A33>A<A4,>5 Ms. M.G was seen wearing a clean skinny *eans and a black and white stripes shirt. (he has a long curly hair, black uncombed hair. Ms. M.G is petite appro"imately five feet tall. (he is not always well groomed until told to do so. (he has clean fingernails. Ms. M.G is always wearing her rosary as a necklace. (he en*oys singing religious songs that everybody when talking. 4evertheless, she has short attention span when talking. Ms. M.G displaces regression as she acts childish and dependent. B>0A?I+<5 77
Ms. M.G was seen standing and singing with the other patient. (he sometimes argues with the other patient. (ometimes goes to bed acting like meditating. Moreover, she interrupt other patients. (he seems talkative and easily distracted. (he usually have flight of ideas and most of the time delucinating. ,+MM24I,A I+45 Ms. M.G speaks in a high#toned voice. (he is responsive when ever asked but sometimes answered the questions not related to the topic. (he sing every time we talk. (he talks using >nglish and ,ebuano language during interaction. (he speaks clear words and very long phrases that is out of the topic. IM3CI,A I+45 Ms. M.G talks too much, easily get mad when someone interrupts her. (he is having delusions and most of the time has flight of ideas.
>?AC2A I+45 he client Ms. M.G was feeling well during the interaction with the student# nurse but after for a while she felt sleepy. -uring the interaction, Ms. M.G was able to establish rapport with the student#nurse because she introduced herself, made an eye#to#eye contact and she is aware of what is happening surrounding her and keeps on singing and shouting. (he is able to identify her own condition and asked the student nurse. he student nurse
regarding the contract, as to time, date, and place for the ne"t interaction, reminded the client. 78
79
You might also like
- Case Study - Bipolar DisorderDocument24 pagesCase Study - Bipolar Disordermattheus101100% (11)
- Case Presentation of Bipolar Affective Disorder, Current Episode, Manic With Psychotic DisorderDocument37 pagesCase Presentation of Bipolar Affective Disorder, Current Episode, Manic With Psychotic DisorderEarl John Natividad89% (9)
- Case Study of Bipolar DisorderDocument1 pageCase Study of Bipolar DisorderIrene Mae Villanueva Ariola0% (1)
- Bipolar CaseDocument41 pagesBipolar CaseEmariel Dulana25% (4)
- Bipolar 1 Case PresentationDocument111 pagesBipolar 1 Case PresentationJhensczy Hazel Maye AlbaNo ratings yet
- Bipolar 2 Disorder Case StudyDocument11 pagesBipolar 2 Disorder Case Studyapi-402293970100% (2)
- Case Study BipolarDocument22 pagesCase Study BipolarRobert de Guzman Jr.93% (29)
- Bipolar Disorder Case StudyDocument14 pagesBipolar Disorder Case StudyValiant Baybay67% (3)
- Schizophrenia Case StudyDocument72 pagesSchizophrenia Case StudyNissie Degulacion100% (4)
- A Case Study On SchizophreniaDocument11 pagesA Case Study On SchizophreniaRosa Isabel57% (7)
- Case Study On SchizophreniaDocument21 pagesCase Study On SchizophreniaAdrian Mallar100% (1)
- Case StudyDocument8 pagesCase StudyAmberlynn Stolarski100% (2)
- Cases Study On BipolarDocument37 pagesCases Study On BipolarjaoNo ratings yet
- Bipolar Mood Disorder Case RevisionDocument11 pagesBipolar Mood Disorder Case RevisionEden Marie Francisco100% (1)
- Schizophrenia Case StudyDocument8 pagesSchizophrenia Case Studyaira2350% (2)
- Case Study NCMHDocument41 pagesCase Study NCMHDiana Ortiz100% (1)
- Disturbed Sleep Pattern in Bipolar ClientDocument2 pagesDisturbed Sleep Pattern in Bipolar ClientJermaine Anne MadayagNo ratings yet
- Nursing Care Plan For A Patient With Bipolar DisorderDocument20 pagesNursing Care Plan For A Patient With Bipolar Disordermjk2100% (4)
- Depression Case StudyDocument9 pagesDepression Case StudySara Lynn LeSage86% (7)
- Schizophrenia NCMH Case StudyDocument41 pagesSchizophrenia NCMH Case StudyJohn Crisostomo89% (36)
- Psychiatric Case StudyDocument32 pagesPsychiatric Case Studyrachael85% (33)
- Schizophrenia Case StudyDocument75 pagesSchizophrenia Case StudyDatujen Sanayatin100% (1)
- Bipolar NCPDocument4 pagesBipolar NCPcandy19agustin100% (1)
- Undifferentiated SchizophreniaDocument190 pagesUndifferentiated Schizophreniaallexiscampaner100% (16)
- Mood Disorder Case PresentationDocument65 pagesMood Disorder Case PresentationRhomizal Mazali83% (6)
- Case Study BipolarDocument22 pagesCase Study BipolarMaria Visitacion100% (1)
- Bipolar NCPDocument2 pagesBipolar NCPweehdinga89% (9)
- Comprehensive Case Study Paranoid SchizophreniaDocument168 pagesComprehensive Case Study Paranoid SchizophreniaAlvin Cruz Quiambao100% (2)
- Pathophysiology of Bipolar DisorderDocument1 pagePathophysiology of Bipolar DisorderGab Abalos100% (2)
- NCPDocument8 pagesNCPTrixia Diaz67% (3)
- Somatoform DisordersDocument18 pagesSomatoform Disordersapi-376421589% (9)
- Paranoid Schizophrenia - Case StudyDocument181 pagesParanoid Schizophrenia - Case StudyLouie Anne Cardines Angulo76% (25)
- Nursing Care Plan For Bipolar Disorder NCPDocument2 pagesNursing Care Plan For Bipolar Disorder NCPderic94% (36)
- Process Recording On Mentally Ill PatientDocument6 pagesProcess Recording On Mentally Ill Patientkyeria40% (5)
- Psychopathology of Schizophrenia (Client)Document1 pagePsychopathology of Schizophrenia (Client)Robert Joseph Sison67% (3)
- Case Study On PARANOID SCHIZOPHRENIA Melisa 19Document29 pagesCase Study On PARANOID SCHIZOPHRENIA Melisa 19MELISA ELEUTHERENo ratings yet
- Bipolar NCPDocument2 pagesBipolar NCPGenevieve VLs100% (1)
- Schizophrenia CaseDocument14 pagesSchizophrenia CaseFrancez Anne Guanzon100% (1)
- Nursing Care for Schizophrenic PatientsDocument1 pageNursing Care for Schizophrenic PatientsMabhel Fatima Abayan EspinosaNo ratings yet
- Bipolar Case StudyDocument45 pagesBipolar Case StudyRanusha AnushaNo ratings yet
- Case Study - Bipolar DisorderDocument25 pagesCase Study - Bipolar DisorderPeter GoNo ratings yet
- Mood Disorders Defnition, Types, Treatment & Nursing CareDocument5 pagesMood Disorders Defnition, Types, Treatment & Nursing CareNico PaneloNo ratings yet
- Mania: Caring For A Person ExperiencingDocument6 pagesMania: Caring For A Person ExperiencingGutsy JewelNo ratings yet
- BehavioralDocument7 pagesBehavioralAnjo Pasiolco CanicosaNo ratings yet
- Case Study: Anna Liza CorpuzDocument72 pagesCase Study: Anna Liza CorpuzAnna Liza Adon CorpuzNo ratings yet
- A Psychiatric Case Study On Chronic SchizoDocument33 pagesA Psychiatric Case Study On Chronic SchizoRendezvouZHDNo ratings yet
- Understanding Historical Context of Abnormal BehaviourDocument11 pagesUnderstanding Historical Context of Abnormal BehaviourAyesha FayyazNo ratings yet
- BC UDPD First 4 Back and FrontDocument23 pagesBC UDPD First 4 Back and FrontAPOORVA PANDEYNo ratings yet
- NHHDocument30 pagesNHHRuth Jazelle MendozaNo ratings yet
- Finals P PTTDocument114 pagesFinals P PTTIelle FranciscoNo ratings yet
- Psychology Project: Akshay Mathur Class - XII - KDocument14 pagesPsychology Project: Akshay Mathur Class - XII - KMandeep BatraNo ratings yet
- Appearance and General BehaviorDocument3 pagesAppearance and General BehaviorHardeep KaurNo ratings yet
- Psychiatric Nursing HesiDocument6 pagesPsychiatric Nursing HesiKarla Lopez91% (11)
- Mental Status Assessment: A. General Appearance The Patient Grooming WasDocument4 pagesMental Status Assessment: A. General Appearance The Patient Grooming Wassandyzgurl100% (3)
- Case Study Psychia Bipolar 2Document57 pagesCase Study Psychia Bipolar 2Joule PeirreNo ratings yet
- Psychiatric AnswersDocument14 pagesPsychiatric AnswersChloie Marie RosalejosNo ratings yet
- Bipolar DisorderDocument2 pagesBipolar Disorderhuskergrad10No ratings yet
- NPIDocument16 pagesNPIBianca de Guzman100% (1)
- Emrgncy Psych in NHDocument12 pagesEmrgncy Psych in NHdahlia4No ratings yet
- Nursing Review NotesDocument88 pagesNursing Review NotesNissie DegulacionNo ratings yet
- Fingertip Day 1 - 3 (10copies)Document4 pagesFingertip Day 1 - 3 (10copies)Nissie DegulacionNo ratings yet
- Fingertip Day 1 - 3 (10copies)Document4 pagesFingertip Day 1 - 3 (10copies)Nissie DegulacionNo ratings yet
- Case StudyDocument38 pagesCase StudyNissie DegulacionNo ratings yet
- Compliance and ResistanceDocument5 pagesCompliance and ResistanceNissie DegulacionNo ratings yet
- Chapter 1-4Document58 pagesChapter 1-4Nissie DegulacionNo ratings yet
- Fingertip Day 1 - 3 (10copies)Document4 pagesFingertip Day 1 - 3 (10copies)Nissie DegulacionNo ratings yet
- Ojt ExperienceDocument1 pageOjt ExperienceNissie Degulacion100% (8)
- Please Be Guided of The Following ScheduleDocument1 pagePlease Be Guided of The Following ScheduleNissie DegulacionNo ratings yet
- MVDocument5 pagesMVNissie DegulacionNo ratings yet
- Maternal & Child Nursing Bullets (Nle & Nclex)Document38 pagesMaternal & Child Nursing Bullets (Nle & Nclex)Richard Ines Valino95% (22)
- University of San Jose - Recoletos College of Nursing Cebu CityDocument3 pagesUniversity of San Jose - Recoletos College of Nursing Cebu CityNissie DegulacionNo ratings yet
- Nursing Review NotesDocument88 pagesNursing Review NotesNissie DegulacionNo ratings yet
- Bipolar 1 Sample 1 CsDocument43 pagesBipolar 1 Sample 1 CsNissie DegulacionNo ratings yet
- Nursing Fundamentals Part 1: Assessment, Nursing Process, Vital SignsDocument10 pagesNursing Fundamentals Part 1: Assessment, Nursing Process, Vital SignsNissie DegulacionNo ratings yet
- Irrigating Cystoclysis Final OutputDocument6 pagesIrrigating Cystoclysis Final OutputNissie Degulacion100% (3)
- DTRDocument2 pagesDTRNissie DegulacionNo ratings yet
- Schizophrenia Case StudyDocument72 pagesSchizophrenia Case StudyNissie Degulacion100% (4)
- Endorsement SheetDocument2 pagesEndorsement SheetNissie DegulacionNo ratings yet
- Physical AssessmentDocument3 pagesPhysical AssessmentNissie DegulacionNo ratings yet
- HattttDocument15 pagesHattttFrences Ann VillamorNo ratings yet
- Principles of Radiographic InterpretationDocument104 pagesPrinciples of Radiographic InterpretationPraney SlathiaNo ratings yet
- TDS PE91 (Sama DGN Euxyl PE9010) ENGDocument3 pagesTDS PE91 (Sama DGN Euxyl PE9010) ENGDhea 'Chiu' SamanthaNo ratings yet
- Emergency Action Code 2013Document200 pagesEmergency Action Code 2013MiguelNo ratings yet
- Neuro ImagingDocument41 pagesNeuro ImagingNauli Panjaitan100% (1)
- Developmental Dysplasia of The HipDocument16 pagesDevelopmental Dysplasia of The Hipjonathan_alvaNo ratings yet
- The Federation of Telangana Chambers of Commerce and IndustryDocument71 pagesThe Federation of Telangana Chambers of Commerce and IndustryPeyush MehtoNo ratings yet
- Symptoms of Low PotassiumDocument3 pagesSymptoms of Low PotassiumCharlene Mae Calanoy100% (1)
- Appendix II DNV-M-scatDocument1 pageAppendix II DNV-M-scatGökhan Ulukuz100% (1)
- De Leon v. MaunladDocument4 pagesDe Leon v. MaunladTibsNo ratings yet
- Fundamentals of Nursing: Urinary Elimination, Catheterization, Ostomy Care & Pain ManagementDocument29 pagesFundamentals of Nursing: Urinary Elimination, Catheterization, Ostomy Care & Pain ManagementKatrina Issa A. GelagaNo ratings yet
- Research Report 339: Promoting Health and Safety As A Key Goal of The Corporate Social Responsibility AgendaDocument52 pagesResearch Report 339: Promoting Health and Safety As A Key Goal of The Corporate Social Responsibility AgendaGordon FreemanNo ratings yet
- OSCARES V MAGSAYSAY MARITIME DEC 2, 2020 GR No 245858Document10 pagesOSCARES V MAGSAYSAY MARITIME DEC 2, 2020 GR No 245858John Leonard BernalNo ratings yet
- Strong Letter of Recommendation for Radiology ResidencyDocument1 pageStrong Letter of Recommendation for Radiology Residencydrsanjeev15No ratings yet
- Patient Satisfaction About Hospital Services: A Study From The Outpatient Department of Tertiary Care Hospital, Jabalpur, Madhya Pradesh, IndiaDocument6 pagesPatient Satisfaction About Hospital Services: A Study From The Outpatient Department of Tertiary Care Hospital, Jabalpur, Madhya Pradesh, IndiaVikram AripakaNo ratings yet
- Boston Carpal Tunnel Syndrome Questionnaire BCTQDocument2 pagesBoston Carpal Tunnel Syndrome Questionnaire BCTQElsye Lalupanda75% (4)
- Material Safety Data Sheet Dibutyl PhthalateDocument4 pagesMaterial Safety Data Sheet Dibutyl PhthalateKameliza Saranghe Choi-siwon SujuelfNo ratings yet
- Case Study On LEUKEMIADocument55 pagesCase Study On LEUKEMIAmacky90% (21)
- WCC Career Focus Magazine: Spring Summer 2011Document28 pagesWCC Career Focus Magazine: Spring Summer 2011Washtenaw Community CollegeNo ratings yet
- Aggression QuestionnaireDocument2 pagesAggression QuestionnaireMichelle LanguianNo ratings yet
- Okamura 1999Document4 pagesOkamura 1999Araceli Enríquez OvandoNo ratings yet
- 2015 ESC Guidelines For The Management of Infective EndocarditisDocument54 pages2015 ESC Guidelines For The Management of Infective EndocarditisFernando Muñoz SolteroNo ratings yet
- Gender Inequality & Its Impact On Mental HealthDocument22 pagesGender Inequality & Its Impact On Mental Healthbanipreet kaurNo ratings yet
- Pol 324Document176 pagesPol 324James IkegwuohaNo ratings yet
- Construction Site Manager Resume Samples - Velvet JobsDocument21 pagesConstruction Site Manager Resume Samples - Velvet JobsRakesh DasNo ratings yet
- Reading Test Text A Corona Virus Disease 19 - A Brief NoteDocument23 pagesReading Test Text A Corona Virus Disease 19 - A Brief Notedevaki dangalNo ratings yet
- LiposarcomaDocument9 pagesLiposarcomaKenneth ColeNo ratings yet
- Plant Pathology LabDocument79 pagesPlant Pathology Labpraveenhansraj87% (15)
- Doctors OrderDocument2 pagesDoctors Ordermarc_alvin0% (1)
- Thesis On Food AdulterationDocument4 pagesThesis On Food Adulterationkatieparkersaintpaul100% (1)