You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The China Study PDFDocument7 pagesThe China Study PDFPatrice108365No ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Advances in Extraction TechniquesDocument13 pagesAdvances in Extraction TechniquesashajangamNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Clinical Cases For MRCPCH PART 2 Applied Knowledge in PracticeDocument218 pagesClinical Cases For MRCPCH PART 2 Applied Knowledge in Practiceaeyousef88% (16)
- Sanctification of The Heart 4th Edition by DR Michelle StrydomDocument771 pagesSanctification of The Heart 4th Edition by DR Michelle StrydomDios Estrella67% (3)
- Moh ExamsDocument12 pagesMoh ExamsPankaj Jindal100% (5)
- Review of Literature on Rabies Prevention and ControlDocument24 pagesReview of Literature on Rabies Prevention and ControlBeah Claudette AbundoNo ratings yet
- Nephrons (Functional Unit)Document44 pagesNephrons (Functional Unit)Nur SanaaniNo ratings yet
- Treatment of Cardiac Arrest in The Hyperbaric Environment - Key Steps On The Sequence of Care - Case ReportsDocument8 pagesTreatment of Cardiac Arrest in The Hyperbaric Environment - Key Steps On The Sequence of Care - Case Reportstonylee24No ratings yet
- AcanthamoebaDocument7 pagesAcanthamoebaYohanna YohannaNo ratings yet
- ACS, ZaiDocument61 pagesACS, ZaiHelmi HaronNo ratings yet
- Ascitesupdate2013 PDFDocument27 pagesAscitesupdate2013 PDFKun Anupong WansukhNo ratings yet
- Tumor Jinak PayudaraDocument2 pagesTumor Jinak PayudaraHelmi HaronNo ratings yet
- Femur and Pelvis Fracture (Trauma)Document20 pagesFemur and Pelvis Fracture (Trauma)Ree YahNo ratings yet
- QuestionsDocument6 pagesQuestionsLorvic Andrew Juanson UmaliNo ratings yet
- Not Eligible As No Experience of Teaching and ResearchDocument5 pagesNot Eligible As No Experience of Teaching and ResearchVasanth Kumar AllaNo ratings yet
- Int Obs PDFDocument37 pagesInt Obs PDFsurgeon77No ratings yet
- Amavatha & VathasonithaDocument125 pagesAmavatha & VathasonithaCicil AbrahamNo ratings yet
- Journal BalakrishnaDocument3 pagesJournal BalakrishnafandheanayaNo ratings yet
- Multiple PregnancyDocument16 pagesMultiple Pregnancyjane7arian7berzabalNo ratings yet
- Daftar PustakaDocument2 pagesDaftar PustakaNurfauziyahNo ratings yet
- Understanding the Benefits of Physical ActivitiesDocument17 pagesUnderstanding the Benefits of Physical ActivitiesRealisan DulnuanNo ratings yet
- Stanford Letter Criticizes Trump COVID-19 AppointeeDocument11 pagesStanford Letter Criticizes Trump COVID-19 AppointeeBayAreaNewsGroup100% (2)
- Prostaglandins: An Overview of Structure and FunctionDocument33 pagesProstaglandins: An Overview of Structure and FunctionMuhammad JamalNo ratings yet
- Mgi Presentation - ReyDocument65 pagesMgi Presentation - ReyCharlot Jade Paderes67% (3)
- Abu Dhabi DRGDocument62 pagesAbu Dhabi DRGDolly creationsNo ratings yet
- Hypokalemia and Hyperkalemia in Infants and Children: Pathophysiology and TreatmentDocument11 pagesHypokalemia and Hyperkalemia in Infants and Children: Pathophysiology and TreatmentAnantaBenvenutoNo ratings yet
- 2012 Karshaniya YavaguDocument4 pages2012 Karshaniya YavaguRANJEET SAWANTNo ratings yet
- Delafloxacin 4Document23 pagesDelafloxacin 4Muhammad RamzanNo ratings yet
- Anterior Segment OctDocument53 pagesAnterior Segment OctA.c. RaghuNo ratings yet
- Nursing Management - Colon CancerDocument7 pagesNursing Management - Colon CancerReese Alessandra GandulfoNo ratings yet
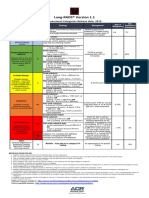
- Lung RADS® Version 1.1: Assessment Categories Release Date: 2019Document1 pageLung RADS® Version 1.1: Assessment Categories Release Date: 2019S Francisco MotNo ratings yet
- List of Empanelled Hospitals in CGHS NagpurDocument58 pagesList of Empanelled Hospitals in CGHS NagpurRajatNo ratings yet
- Audiometric Evaluation Report .: Left Ear Right EarDocument1 pageAudiometric Evaluation Report .: Left Ear Right EarRaja IsaacNo ratings yet
- Prevalence of Hypothyroidism in Adults An EpidemioDocument6 pagesPrevalence of Hypothyroidism in Adults An EpidemioCindy Auliah NasutionNo ratings yet