International Journal of Pharmaceutical Science Invention ISSN (Online): 2319 6718, ISSN (Print): 2319 670X www.ijpsi.
i.org Volume 3 Issue 1 January 2014 PP.36-40
Serum Total Prostatic Specific Antigen and Prostatic Acid Phosphatase Measurement Discriminating Prostate Carcinoma from Benign Prostatic Hyperplasia in Sudanese Patients
Haala M. Gabra1*; Adbelgadir A Elmugadam 2; Badereldein H Elabid 3; Ghada A.Elfadil2, Mohamed H. Arbab A4;Elmutuz H.Elssaig 5;
2,
Clinical Chemistry, Laboratory department, Fedail Hospital. Clinical Chemistry, department of FMLS, Sudan University of Science and Technology. 3, Chemical Pathology, department of FMLS, University of Science and Technology. 4, Medical Microbiology, department of FMLS, Omduraman Ahlia University. 5, Clinical Chemistry, department of FMLS, Al-Zaiem Al-Azhari University.
1,
ABSTRACT : This is a prospective, analytical, hospital based, case control study. The aim of this study was to evaluate the clinical utility of total prostate specific antigen (TPSA) and prostatic acid phosphatase (PAP) for distinction between prostate carcinoma (PCa) and Benign prostatic hyperplasia (BPH) in Sudanese patients in Khartoum state.This study was carried out in Fedail Medical Hospital during the period of 2010 to 2012. It was performed on 200 patients as the study group and 100 healthy volunteers as the control group. The age for the control group and the study group were matched. Serum level of TPSA was measured by Roche immunoassay cobas e411 and serum PAP level was measured spectrophotometericaly.The mean level of serum TPSA was (42.627.2) and (7.85.1) for PCa & BPH respectively ( p<0.01). While mean of PAP value were (37.524.5) and (8.817.05) for PCa & BPH respectively. PAP was elevated in 65% of the patients with cancer confined to the prostate, TPSA in 90%. In those patients with metastatic spread, PAP was elevated in 80% compared with 92% for PSA. In the BPH group, PAP levels were raised in 35% and for PSA in 81%.In conclusion, the results indicated that marked elevation of serum PSA suggests prostate carcinoma and that serum TPSA can discriminate prostate carcinoma from prostatic benign hyperplasia better than serum PAP.
KEY WORDS : Total Prostate Specific Antigen, Prostatic Acid Phosphatase, Benign Prostatic Hyperplasia,
Prostate Cancer, and Sudanese.
I.
INTRODUCTION
Prostate cancer is the second leading cause of cancer-related deaths for men in the United States (1). It has been suggested that screening for prostate cancer may have reduced prostate cancer mortality rates, but this remains controversial (2). Current American Cancer Society guidelines for prostate cancer screening recommend a digital rectal examination and prostate-specific antigen (PSA) measurement annually for all men 50 or older if they have a minimum life expectancy of 10 years (3).Prostate specific antigen (PSA) is a protein manufactured solely in the prostate. The prostate gland manufactures this protein in large quantities. The PSA level in the blood can vary by about 20% from day to day (4). The Food and Drug Administration (FDA) in 1994 approved serum PSA to be used as an early detection of prostate cancer. Like so many serum tumour markers, it is produced by both normal and cancerous glands. In men with prostate cancer, the serum levels can be elevated in both localized and advanced or disseminated disease. PSA levels are generally proportional to the size of the tumour. However, there is a significant overlap between PSA levels found in cancer and benign prostatic hyperplasia cases (BPH) (5). Prostatic acid phosphatase is an enzyme produced by several types of tissue, including normal prostate tissue. PAP is one of the major proteins secreted by prostate columnar epithelium secretory cells following puberty. In healthy individuals, PAP serum levels are low, on the order of 1-3ng/ml, whereas serum levels are elevated in many individuals with metastatic prostate cancer (6, 7). Prostatic specific antigen (PSA) and prostatic acid phosphatase (PAP) are the tumor markers of prostatic carcinoma and have been used for confirming and monitoring prostate cancer (8, 9). The clinical utility of PSA and PAP for early detection of prostate cancer is hampered by elevation of serum PSA levels in men with prostate benign hyperplasia (10, 11).
www.ijpsi.org
36 | P a g e
Serum Total Prostatic Specific Antigen and Prostatic II. MATERIALS AND METHODS:
2.1.Study design This study was prospective, analytical, hospital based, case control study conducted in Fedail Hospital, Khartoum state, Sudan during the period of December 2010 to March 2012. 2.2.Subjects This study was performed on 200 male patients as the study group, 100 of them diagnosed with prostatic carcinoma and another 100 diagnosed with benign prostatic hyperplasia. The mean age for them was 68.8.08.3 years. The study, also, included 100 healthy males as the control group with matched mean age 66.7.08.1 year. Interviews with the patients were done to obtain the clinical data. Also, a questionnaire was designed to collect data from the patients. Permission of this study was obtained from the authorized personnel in Fedail hospital. The nature of the study was explained to all participants in this study. Informed consent was obtained from each participant. 2.3.Sample In a sterile condition by using a local antiseptic for skin, 5 ml of venous blood was collected in serum separating gel tubes from patients and controls. The blood samples were separated after complete clotting by centrifugation at 4000 rpm for 5 minutes and serum was collected and stored in tubes at -20C for the analysis of TPSA while for PAP the serum was analyzed immediately after separation. 2.4. Measurements of TPSA & PAP Serum for TPSA was measured by Electrochemiluminesent (ECL) immunoassay on Roche analyzer cobas e411, while the serum for PAP level was measured spectrophotometericaly. All samples were analyzed in the laboratory of Fedail Hospital. 2.5. Statistic evaluation The data obtained were expressed as mean values SD. Statistical analysis was performed using SPSS 17 (Statistical Package for Social Sciences). The means were compared using Independent sample t.test. Pearsons correlation analysis was used for correlation of parameters measured. Analysis using two-tailed and a p-value 0.05 was considered as statistically significant.
III.
RESULTS:
Serum TPSA (42.627.2ng/ml) in the PCa group was found to be higher than that in BPH group (7.85.1ng/ml). The difference between the two means was highly significant at p<0.01. PAP in the PCa group was significantly higher than that of BPH group (4.260.24 and 3.020.97) respectively (p<0.01).Then the study groups were subdivided according to the level of TPSA (<4ng/ml, 4-10ng/ml, 10-20ng/ml and >20 ng/ml) as shown in tables I and II, the TPSA was highly significant than PAP in all ranges. TableI : Comparison between TPSA in PCa group and BPH group according to the level of TPSA TPSA ranges TPSA <4ng/ml TPSA4-10 ng/ml TPSA10-20ng/ml TPSA >20ng/ml PCa meanSD 2.871.16 6.421.75 14.23.13 59.126.6 P value 0.00 0.00 0.00 0.00 BPH meanSD 1.350.37 6.251.54 13.22.9 25.64.2 P value 0.00 0.00 0.00 0.00
www.ijpsi.org
37 | P a g e
Serum Total Prostatic Specific Antigen and Prostatic
Table II: Comparison between PAP in PCa group and BPH group according to the level of TPSA
TPSA ranges TPSA <4ng/ml TPSA 4-10 ng/ml TPSA10-20ng/ml TPSA >20ng/ml PCa meanSD 4.260.25 6.942.3 17.310.4 44.819.5 P value 0.002 0.00 0.33 0.174 BPH meanSD 3.020.97 7.554.98 11.615.8 24.912.6 P value 0.029 0.00 0.00 0.089
The PCa group were sub divided according to Gleason score to well differentiated (2/10, 3/10 and 4/10), moderate differentiated (5/10, 6/10 and 7/10) and poor differentiated (8/10, 9/10, 10/10). TPSA levels were highly significant in all stages of prostate cancer while the PAP was only significant in the moderate differentiated group of the PCa as shown in table III. Table III: Comparison between TPSA and PAP in PCa group according to Gleason score.
PCa Stages Mean SD Well differentiation P value Mean SD Moderate differentiation P value Mean SD Poor differentiation P value 0.00 42.6 33 0.00 0.00 37.5 33 0.236 0.00 27 23 0.37 23.9 22 TPSA 7.7 7.5 PAP 27.1 23
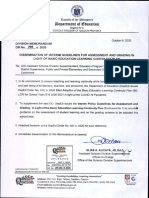
There were strong positive and significant correlations between TPSA and PAP in PCa group (r=0.836, P=0.00) (figure 1) and also there were strong positive and significant correlations between TPSA and PAP in BPH group (r=0.702, p=0.00) (figure 2).
Figure1: A scatter plot shows correlation between TPSA & PAP in the PCa study group
www.ijpsi.org
38 | P a g e
Serum Total Prostatic Specific Antigen and Prostatic
Figure2: A scatter plot shows correlation between TPSA & PAP in the BPH study group TableIV: The sensitivity, specificity, PPV & NPV for TPSA & PAP Parameter Sensitivity Specificity Positive Predictive Value Negative Predictive Value TPSA 95% 96% 0.96 0.95 PAP 77% 91% 0.89 0.81
Efficiency of discrimination of prostate carcinoma from benign prostatic hyperplasia by PAP assay, as indicated in tables V and VI, is inferior to that of TPSA assay. Table V: TPSA measurement discrimination of prostatic cancer from benign prostatic hyperplasia
Parameter TPSA <4 ng/ml TPSA 4-10 ng/ml TPSA 10-20 ng/ml TPSA >20 ng/ml No. of PCa 25% 32% 58% 91% No. of BPH 75% 68% 41% 9%
*Normal range is 0- 4 ng/ml. Table VI: PAP measurement discrimination of prostatic cancer from benign prostatic hyperplasia
Parameter PAP <5 ng/ml PAP 5-10 ng/ml PAP >10 ng/ml No. of PCa 14% 26% 59% No. of BPH 38% 25% 35%
*Normal range is 0- 5 ng/ml.
www.ijpsi.org
39 | P a g e
Serum Total Prostatic Specific Antigen and Prostatic IV. DISCUSSION:
The results in this study showed that in the BPH group, PAP was raised in 35% and 81% for PSA. PAP was elevated in 65% of the patients with cancer confined to the prostate, TPSA in 90%. In those patients with metastatic spread, PAP was elevated in 80% compared with 92% for PSA. TPSA results show highly statistically significance (P value < 0.01) in the PCa group & BPH group even when the TPSA stratified to levels (<4, 4-10, 10-20 & >20 ng/ml). However PAP shows highly significance in PCa group only when TPSA in the range of (< 4 & 4-10 ng/ml) while in the BPH group it was statistically significant in all ranges (P value <0.01) except when TPSA > 20 ng/ml it was statistically insignificant (P value >0.05).In the PCa group and according to the Gleasons score TPSA shows highly significance in all stages (P value <0.01), however PAP shows only highly significance in the moderate differentiated group (P value <0.01).Results in this study indicate that prostate carcinoma can be discriminated from Benign Prostatic Hyperplasia by serum TPSA with 95% sensitivity and by PAP with only 77 % sensitivity. The combined use of PSA and PAP do not give a greater accuracy in the screening of prostate cancer when compared with the sole use of PSA. This finding was consistent with the results reported by Bogdanowicz, et al (12) and Shih, et al (13). Although Bogdanowicz, et al (12) reported that PAP was elevated in only 4 patients when PSA was normal; however, in this study, the results obtained indicate that PAP was elevated in only one patient when PSA was normal.In conclusion, the study showed that PAP was a less sensitive than TPSA in screening of the prostate cancer. TPSA was superior to PAP for the detection of prostatic cancer. PAP does not give a greater accuracy in the screening of prostate cancer when compared with the TPSA. Prostatic specific antigen measurements can be used for discrimination of Benign Prostatic Hyperplasia from Prostatic Carcinoma, since PSA measurements are simple, painless, and relatively inexpensive procedures.
REFERENCES:
[1] [2] [3] [4] Jemal, A; Siegel, R; Ward, E; Murray, T; Xu, J and Thun M J. (2007). Cancer statistics.CA Cancer J Clin. ;57:43-66. Hoffman, RM. Viewpoint. (2006). limiting prostate cancer screening. Ann Intern Med.; 144:438-440. Smith, R; Cokkinides, V and Eyre, HJ. (2004). American Cancer Society guidelines for the early detection of cancer.CA Cancer J Clin.; 54:41- 52. Sltormos, G; Semjonow, A; Sibley, PEC; Lamerz, R; Petersen, PH; Albrecht, W; Bialk, P; Gion, M; Junker, F; Schmid, HP and Poppe HV. (2005). Biological Variation of total prostate-specific antigen: A Survey of published estimates and consequences for clinical practice. Clin Chem; 51: 1342-1351. Carter, HB; Epstein, JI and Partin, AW. (1997). Influence of age and prostate-specific antigen on the cancer of curable prostate cancer among men with nonpalpable disease. Urology; 53: 126-130. Ahmann, FR and Schifman, RB. (1987). Prospective comparison between serum monoclonal prostate specific antigen and acid phosphatase measurements in metastatic prostatic cancer. J Urol ; 137: 431-434. Robles, JM; Morell, AR; De Torres, JA and Rosello, AS. (1989). Clinical behavior of prostatic specific antigen and prostatic acid phosphatase: a comparative study. Int J Biol Markers; 4: 87- 94. Hudson, MA; Bahnson, RR and Catalona, WJ. (1989). Clinical use of prostate specific antigen in patients with prostate cancer J Urol.; 142:1011-1 017. Stamey, TA; Yang, N; Hay, AR; McNeal, JE; Freiha, FS and Redwine, E. (1987). Prostate-specific antigen as a serum marker for adenocarcinoma of the prostate. N Engl J Med.; 317:909-916. Ercole, CJ; Lange, PH; Mathisen, M; Chiou, RK; Reddy, PK and Vessella, RL. (1987)Prostatic specific antigen and prostatic acid phosphatase in the monitoring and staging of patients with prostatic cancer. J Urol.; 1 38:1181-1 184. Heaney, JA; Allen, MA; Keane, T and Duffy, MJ. (1987). Prostate specific antigen superior serum marker for prostatic carcinoma. IrJ Med Sci.; 156:138-141. Bogdanowicz, JF; Bentvelsen, FM; Oosterom, R and Schroeder, FH. (1991).Evaluation of prostate-specific antigen and prostatic acid phosphatase in untreated prostatic carcinoma and benign prostatic hyperplasia Scand J Urol Nephrol Suppl. 138:97-103. Shih, W-J; Collins, J; Mitchell, B and Wierzbinski. (1994). Serum PSA and PAP measurements discriminating patients with prostate carcinoma from patients with nodular hyperplasia J Nati Med Assoc.; 86:667-670.
[5] [6] [7] [8] [9] [10] [11] [12] [13]
www.ijpsi.org
40 | P a g e
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- A Discourse On Modern Civilization: The Cinema of Hayao Miyazaki and GandhiDocument6 pagesA Discourse On Modern Civilization: The Cinema of Hayao Miyazaki and GandhiinventionjournalsNo ratings yet
- The Effect of Transformational Leadership, Organizational Commitment and Empowerment On Managerial Performance Through Organizational Citizenship Behavior at PT. Cobra Direct Sale IndonesiaDocument9 pagesThe Effect of Transformational Leadership, Organizational Commitment and Empowerment On Managerial Performance Through Organizational Citizenship Behavior at PT. Cobra Direct Sale Indonesiainventionjournals100% (1)
- Islamic Insurance in The Global EconomyDocument3 pagesIslamic Insurance in The Global EconomyinventionjournalsNo ratings yet
- Effects of Online Marketing On The Behaviour of Consumers in Selected Online Companies in Owerri, Imo State - Nigeria.Document12 pagesEffects of Online Marketing On The Behaviour of Consumers in Selected Online Companies in Owerri, Imo State - Nigeria.inventionjournalsNo ratings yet
- The Network Governance in Kasongan Industrial ClusterDocument7 pagesThe Network Governance in Kasongan Industrial ClusterinventionjournalsNo ratings yet
- Effects of Online Marketing On The Behaviour of Consumers in Selected Online Companies in Owerri, Imo State - NigeriaDocument12 pagesEffects of Online Marketing On The Behaviour of Consumers in Selected Online Companies in Owerri, Imo State - Nigeriainventionjournals100% (1)
- The Usage and Understanding of Information and Communication Technology On Housewife in Family Welfare Empowerment Organization in Manado CityDocument10 pagesThe Usage and Understanding of Information and Communication Technology On Housewife in Family Welfare Empowerment Organization in Manado CityinventionjournalsNo ratings yet
- An Appraisal of The Current State of Affairs in Nigerian Party PoliticsDocument7 pagesAn Appraisal of The Current State of Affairs in Nigerian Party PoliticsinventionjournalsNo ratings yet
- Negotiated Masculinities in Contemporary American FictionDocument5 pagesNegotiated Masculinities in Contemporary American FictioninventionjournalsNo ratings yet
- The Social Composition of Megaliths in Telangana and Andhra: An Artefactual AnalysisDocument7 pagesThe Social Composition of Megaliths in Telangana and Andhra: An Artefactual AnalysisinventionjournalsNo ratings yet
- The Impact of Leadership On Creativity and InnovationDocument8 pagesThe Impact of Leadership On Creativity and InnovationinventionjournalsNo ratings yet
- Non-Linear Analysis of Steel Frames Subjected To Seismic ForceDocument12 pagesNon-Linear Analysis of Steel Frames Subjected To Seismic ForceinventionjournalsNo ratings yet
- Inter-Caste or Inter-Religious Marriages and Honour Related Violence in IndiaDocument5 pagesInter-Caste or Inter-Religious Marriages and Honour Related Violence in IndiainventionjournalsNo ratings yet
- Student Engagement: A Comparative Analysis of Traditional and Nontradional Students Attending Historically Black Colleges and UniversitiesDocument12 pagesStudent Engagement: A Comparative Analysis of Traditional and Nontradional Students Attending Historically Black Colleges and Universitiesinventionjournals100% (1)
- H0606016570 PDFDocument6 pagesH0606016570 PDFinventionjournalsNo ratings yet
- Literary Conviviality and Aesthetic Appreciation of Qasa'id Ashriyyah (Decaodes)Document5 pagesLiterary Conviviality and Aesthetic Appreciation of Qasa'id Ashriyyah (Decaodes)inventionjournalsNo ratings yet
- Muslims On The Margin: A Study of Muslims OBCs in West BengalDocument6 pagesMuslims On The Margin: A Study of Muslims OBCs in West BengalinventionjournalsNo ratings yet
- Effect of P-Delta Due To Different Eccentricities in Tall StructuresDocument8 pagesEffect of P-Delta Due To Different Eccentricities in Tall StructuresinventionjournalsNo ratings yet
- Non-Linear Analysis of Steel Frames Subjected To Seismic ForceDocument12 pagesNon-Linear Analysis of Steel Frames Subjected To Seismic ForceinventionjournalsNo ratings yet
- E0606012850 PDFDocument23 pagesE0606012850 PDFinventionjournalsNo ratings yet
- C0606011419 PDFDocument6 pagesC0606011419 PDFinventionjournalsNo ratings yet
- D0606012027 PDFDocument8 pagesD0606012027 PDFinventionjournalsNo ratings yet
- E0606012850 PDFDocument23 pagesE0606012850 PDFinventionjournalsNo ratings yet
- A Critical Survey of The MahabhartaDocument2 pagesA Critical Survey of The MahabhartainventionjournalsNo ratings yet
- F0606015153 PDFDocument3 pagesF0606015153 PDFinventionjournalsNo ratings yet
- F0606015153 PDFDocument3 pagesF0606015153 PDFinventionjournalsNo ratings yet
- H0606016570 PDFDocument6 pagesH0606016570 PDFinventionjournalsNo ratings yet
- Development of Nighttime Visibility Assessment System For Road Using A Low Light CameraDocument5 pagesDevelopment of Nighttime Visibility Assessment System For Road Using A Low Light CamerainventionjournalsNo ratings yet
- C0606011419 PDFDocument6 pagesC0606011419 PDFinventionjournalsNo ratings yet
- D0606012027 PDFDocument8 pagesD0606012027 PDFinventionjournalsNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- International Journal of Radiology and Imaging Technology Ijrit 7 082Document3 pagesInternational Journal of Radiology and Imaging Technology Ijrit 7 082Zafitri AsrulNo ratings yet
- (Cambridge Studies in Indian History and Society 23) Daniel Marston - The Indian Army and The End of The Raj-Cambridge University Press (2014)Document398 pages(Cambridge Studies in Indian History and Society 23) Daniel Marston - The Indian Army and The End of The Raj-Cambridge University Press (2014)mandeep5No ratings yet
- 112RESEARCHAGENDACORRODocument4 pages112RESEARCHAGENDACORROMar Angelo FlorescaNo ratings yet
- Iso 11979-10 2006Document25 pagesIso 11979-10 2006Alberto FernándezNo ratings yet
- A Comprehensive Guide To 21st Century SkillsDocument26 pagesA Comprehensive Guide To 21st Century SkillsRaul Coria TinocoNo ratings yet
- Structural Analysis of Steering Knuckle For Weight ReductionDocument6 pagesStructural Analysis of Steering Knuckle For Weight ReductionMithun V KulkarniNo ratings yet
- Sma4801 - Lu3 - Framing The Proposed Study and Developing A Research ProposalDocument8 pagesSma4801 - Lu3 - Framing The Proposed Study and Developing A Research ProposalMolepa Isaac SeabelaNo ratings yet
- Model-Based Systems Engineering (MBSE) Challenge: Modeling & Simulation Interoperability (MSI) Team Status UpdateDocument105 pagesModel-Based Systems Engineering (MBSE) Challenge: Modeling & Simulation Interoperability (MSI) Team Status UpdateNaveen TripuraneniNo ratings yet
- 2005 Amisha PrakashDocument36 pages2005 Amisha PrakashAmisha PrakashNo ratings yet
- Gardner Et Al. (2007) Biol ConsDocument15 pagesGardner Et Al. (2007) Biol ConsFabio ZabalaNo ratings yet
- Ansari Et Al 2012 Influence of Nanotechnology On Herbal DrugsDocument5 pagesAnsari Et Al 2012 Influence of Nanotechnology On Herbal DrugsElton-Patrícia Brito RibeiroNo ratings yet
- Self DevelopmentDocument22 pagesSelf DevelopmentDeepa BhaskarNo ratings yet
- DM 299, S. 2020-LqEblBRhyfiSaTlTux76Document259 pagesDM 299, S. 2020-LqEblBRhyfiSaTlTux76MJ ReyesNo ratings yet
- Sample Invitation Letter For Lawmaker To Visit YouDocument1 pageSample Invitation Letter For Lawmaker To Visit Youarnaldo nepthaly caspeNo ratings yet
- Olivia Schronce Final Senior Project ReportDocument21 pagesOlivia Schronce Final Senior Project Reportapi-320829276No ratings yet
- Nursing Lecture NotesDocument11 pagesNursing Lecture NotesKwabena AmankwaNo ratings yet
- Batch Fermentation Modeling, Monitoring, and Control (Chemical Industries, Vol. 93) PDFDocument620 pagesBatch Fermentation Modeling, Monitoring, and Control (Chemical Industries, Vol. 93) PDFVinicius De Holanda Pasolini100% (1)
- Planning Information SystemDocument12 pagesPlanning Information SystemedelitaNo ratings yet
- Citrus MaximaDocument40 pagesCitrus MaximaMin YoongiNo ratings yet
- Lecture 5 - Literature ReviewDocument20 pagesLecture 5 - Literature ReviewIsha ShaikhNo ratings yet
- Rubric For The Search of Outstanding.Document10 pagesRubric For The Search of Outstanding.Manuelito MontoyaNo ratings yet
- Agustin, FS-2-LE-4-act1Document8 pagesAgustin, FS-2-LE-4-act1Melissa AgustinNo ratings yet
- Chapter 3: Quality Management 1Document92 pagesChapter 3: Quality Management 1Randy CavaleraNo ratings yet
- Impact of An Out-Of-Class Activity On Students' English Awareness, Vocabulary, and AutonomyDocument12 pagesImpact of An Out-Of-Class Activity On Students' English Awareness, Vocabulary, and AutonomyEka AdeNo ratings yet
- Sources of Sales Force RecruitmentDocument8 pagesSources of Sales Force RecruitmentTanya Patel50% (2)
- Expressive Arts 1Document5 pagesExpressive Arts 1fundira tashingaNo ratings yet
- Occupation 2Document16 pagesOccupation 2api-300148801No ratings yet
- MM 499-FINAL YEAR PROJECT PresentationDocument33 pagesMM 499-FINAL YEAR PROJECT PresentationCHACHAGodsonNo ratings yet
- Programme WFHSS 2022 BDDocument46 pagesProgramme WFHSS 2022 BDAudreyNo ratings yet
- Competency Based Education (Shikha)Document5 pagesCompetency Based Education (Shikha)Abhilash Paul100% (1)