You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- ASD Diagnosis Tools - UpToDateDocument3 pagesASD Diagnosis Tools - UpToDateEvy Alvionita Yurna100% (1)
- Nitric AcidDocument7 pagesNitric AcidKuldeep BhattNo ratings yet
- Class Two Summer Vacation AssignmentDocument1 pageClass Two Summer Vacation AssignmentshahbazjamNo ratings yet
- Gendec - Inbound HS-HTNDocument1 pageGendec - Inbound HS-HTNKhalidNo ratings yet
- Pay Details: Earnings Deductions Code Description Quantity Amount Code Description AmountDocument1 pagePay Details: Earnings Deductions Code Description Quantity Amount Code Description AmountVee-kay Vicky KatekaniNo ratings yet
- Outlook 2Document188 pagesOutlook 2Mafer Garces NeuhausNo ratings yet
- Xi 3 1Document1 pageXi 3 1Krishnan KozhumamNo ratings yet
- IPG Or-01 - PTC Train Infrastructure Electrical Safety RulesDocument50 pagesIPG Or-01 - PTC Train Infrastructure Electrical Safety Rules4493464No ratings yet
- ATI Respiratory PowerpointDocument90 pagesATI Respiratory PowerpointAnn KelseaNo ratings yet
- Brody2012 PDFDocument13 pagesBrody2012 PDFfrancisca caceresNo ratings yet
- GEC - ReviewerDocument23 pagesGEC - ReviewerGlycel BagabagonNo ratings yet
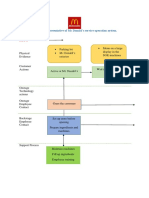
- Blueprint Huynh My Ky Duyen 2022 McDonald'sDocument2 pagesBlueprint Huynh My Ky Duyen 2022 McDonald'sHuỳnh Mỹ Kỳ DuyênNo ratings yet
- RRC Group D Notification 70812Document11 pagesRRC Group D Notification 70812admin2772No ratings yet
- Chapter 2 Unfinished RRLDocument22 pagesChapter 2 Unfinished RRLGM XylerNo ratings yet
- Jun Judging ClinicDocument1 pageJun Judging Cliniccsponseller27No ratings yet
- What Is A VolcanoDocument2 pagesWhat Is A VolcanonatachaNo ratings yet
- Royal British College IncDocument5 pagesRoyal British College IncLester MojadoNo ratings yet
- K EtaDocument14 pagesK EtaJosue Teni BeltetonNo ratings yet
- Mid Day Meal Scheme-Case Study of BiharDocument4 pagesMid Day Meal Scheme-Case Study of BiharKaran singh RautelaNo ratings yet
- Carboset CA-600 - CST600 - CO - enDocument3 pagesCarboset CA-600 - CST600 - CO - enNilsNo ratings yet
- MajorProjects 202112 e 1Document64 pagesMajorProjects 202112 e 1xtrooz abiNo ratings yet
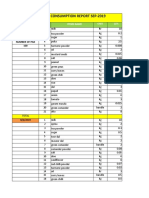
- Daily Staff Food Consumption Reports Sep-2019Document4 pagesDaily Staff Food Consumption Reports Sep-2019Manjit RawatNo ratings yet
- Viscoline Annular UnitDocument4 pagesViscoline Annular UnitjoquispeNo ratings yet
- SGT PDFDocument383 pagesSGT PDFDushyanthkumar DasariNo ratings yet
- Classification of Speech ActDocument1 pageClassification of Speech ActDarwin SawalNo ratings yet
- Senior Project RiceberryDocument76 pagesSenior Project RiceberryIttisak PrommaNo ratings yet
- Reaction Paper-RprDocument6 pagesReaction Paper-Rprapi-543457981No ratings yet
- India Wine ReportDocument19 pagesIndia Wine ReportRajat KatiyarNo ratings yet
- Pip-Elsmt01 P66 Midstream Projects 0 1/02/18: Document Number S & B Job Number Rev Date SheetDocument11 pagesPip-Elsmt01 P66 Midstream Projects 0 1/02/18: Document Number S & B Job Number Rev Date SheetAjay BaggaNo ratings yet
- Basic Electrical Engineering NotesDocument25 pagesBasic Electrical Engineering NotesAnas AnsariNo ratings yet