You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Curso Moodle MiiriadaxDocument1 pageCurso Moodle Miiriadaxrafdiaz2No ratings yet
- Cursos UdacityDocument3 pagesCursos Udacityrafdiaz2No ratings yet
- Eczema, Immunity & The Skin Microbiome: Heidi H. Kong Dermatology Branch, CCR, NCIDocument38 pagesEczema, Immunity & The Skin Microbiome: Heidi H. Kong Dermatology Branch, CCR, NCIrafdiaz2No ratings yet
- .Imagineer LogDocument1 page.Imagineer Lografdiaz2No ratings yet
- SYLLABUSDocument3 pagesSYLLABUSrafdiaz2No ratings yet
- Videoconferencia BrazilDocument2 pagesVideoconferencia Brazilrafdiaz2No ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Perbedaan Status Gizi Bayi Usia 6-9 Bulan Yang Diberi MPASI Buatan Pabrik Dan RumahDocument8 pagesPerbedaan Status Gizi Bayi Usia 6-9 Bulan Yang Diberi MPASI Buatan Pabrik Dan RumahdenissaNo ratings yet
- The PH Miracle For CancerDocument4 pagesThe PH Miracle For CancerSusyq0% (1)
- Autism Spectrum Disorder Symptoms Improve With Combination Therapy Directed at Improving Gut Microbiota and Reducing InflammationDocument7 pagesAutism Spectrum Disorder Symptoms Improve With Combination Therapy Directed at Improving Gut Microbiota and Reducing InflammationSarah Naomi Jeanett ObenhoferNo ratings yet
- Nutrient Refererence Dietary IntakesDocument320 pagesNutrient Refererence Dietary IntakesApril OrfordNo ratings yet
- Sports Nutrition Lecture 3Document17 pagesSports Nutrition Lecture 3Alif syadhasif UpnmNo ratings yet
- Budwig Cancer GuideDocument116 pagesBudwig Cancer GuideStanley ChanNo ratings yet
- NDP Performance EvaluationDocument1 pageNDP Performance EvaluationAlibasher MacalnasNo ratings yet
- Comparative Evaluation of Quality and Composition of Ostrich, Turkey and Broiler Meat - V. Jukna, J. Klementavičiūtė, E. Meškinytė-Kaušilienė, N. Pečiulaitienė, M. Samborskytė, L. AmbrasūnasDocument8 pagesComparative Evaluation of Quality and Composition of Ostrich, Turkey and Broiler Meat - V. Jukna, J. Klementavičiūtė, E. Meškinytė-Kaušilienė, N. Pečiulaitienė, M. Samborskytė, L. AmbrasūnasCk_psihNo ratings yet
- Pocari SweatDocument4 pagesPocari SweatDinda ClarissaNo ratings yet
- Lifestyle Focus December 1 2006Document19 pagesLifestyle Focus December 1 2006api-3717780No ratings yet
- 304 Stanbul Yabanc 305 Lar 304 231 in T 252 RK 231 e 199 Al 305 351 Ma Kitab 305 A2Document33 pages304 Stanbul Yabanc 305 Lar 304 231 in T 252 RK 231 e 199 Al 305 351 Ma Kitab 305 A2Eleni KartsonakiNo ratings yet
- Final Project Report AnandDocument8 pagesFinal Project Report AnandKrupa GadhaviNo ratings yet
- 60 Days Fitness Challenge - Weight Loss GuidelinesDocument4 pages60 Days Fitness Challenge - Weight Loss GuidelinesDinesh HandeNo ratings yet
- DietPlan 2Document3 pagesDietPlan 2Rahul SoniNo ratings yet
- NCPPPPDocument6 pagesNCPPPPIvan Liquiran AvenadoNo ratings yet
- Operan Rawat InapDocument2 pagesOperan Rawat InapFarmasi Primaya HospitalNo ratings yet
- Manufacturing of Flavoured Milk: Submitted byDocument15 pagesManufacturing of Flavoured Milk: Submitted byDipu AhirNo ratings yet
- Moisture Sorption Isotherm Characteristics of Ground FlaxseedDocument3 pagesMoisture Sorption Isotherm Characteristics of Ground FlaxseedLintang Sawitri NugraheniNo ratings yet
- The History of ChocolateDocument12 pagesThe History of ChocolateDina CordovaNo ratings yet
- 4 As Lesson Plan Final 2023Document6 pages4 As Lesson Plan Final 2023Kim Valeri TomsonNo ratings yet
- Lightweight Rowers. Seasonal Variations in The Body Composition ofDocument5 pagesLightweight Rowers. Seasonal Variations in The Body Composition ofGizem OzkayaNo ratings yet
- Calder 2013Document34 pagesCalder 2013Lastrie BuluatieNo ratings yet
- Practical Psychology - Body Image in AdolescentsDocument23 pagesPractical Psychology - Body Image in AdolescentsLekshmiNo ratings yet
- LongevityDocument12 pagesLongevitychai7750% (2)
- Topic-Ks1 Science Yr 2 Autumn 1 Healthy Animals OverviewDocument3 pagesTopic-Ks1 Science Yr 2 Autumn 1 Healthy Animals OverviewEdwin FongNo ratings yet
- Sugar Film Movie ReviewDocument2 pagesSugar Film Movie ReviewJocel VictoriaNo ratings yet
- Fisiolog 160Document14 pagesFisiolog 160saul BrawlNo ratings yet
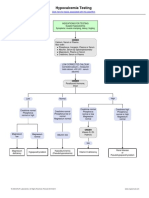
- Hypocalcemia Testing AlgorithmDocument1 pageHypocalcemia Testing AlgorithmAnonymous HdHd7ePNo ratings yet
- Department of Education: Activity Sheets in Pe 10 Quarter 1Document8 pagesDepartment of Education: Activity Sheets in Pe 10 Quarter 1Gine Bert Fariñas PalabricaNo ratings yet
- Who Do You Live With?: at The MomentDocument10 pagesWho Do You Live With?: at The MomentThuy linh Huynh thi100% (1)