You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Link To Publication in University of Groningen/UMCG Research DatabaseDocument19 pagesLink To Publication in University of Groningen/UMCG Research Databaseovr79100% (1)
- Canadian Medical Residency GuideDocument239 pagesCanadian Medical Residency GuideSym Y100% (1)
- Peripheral Neuropathies FOR CLASSIFICATIONDocument9 pagesPeripheral Neuropathies FOR CLASSIFICATIONAnnie JoNo ratings yet
- Laminates AND Veneers: Dr. Sakshi Rawal Department of Prosthodontics MDS II YearDocument76 pagesLaminates AND Veneers: Dr. Sakshi Rawal Department of Prosthodontics MDS II Yearsapna100% (2)
- 1 - Hifumax 1Document25 pages1 - Hifumax 1Get It SuplementosNo ratings yet
- Monitoring Levels of Iron, TIBC, HB, Transferrin and Ferritin During Pregnancy Trimesters and Lactation in Sulaimania City /iraqDocument3 pagesMonitoring Levels of Iron, TIBC, HB, Transferrin and Ferritin During Pregnancy Trimesters and Lactation in Sulaimania City /iraqMabel StracciaNo ratings yet
- Mycobacterium Tuberculosis,: Molecular Epidemiology of Buenos Aires, ArgentinaDocument4 pagesMycobacterium Tuberculosis,: Molecular Epidemiology of Buenos Aires, ArgentinaMabel StracciaNo ratings yet
- NIH Public Access: Vitamin D and Gestational Diabetes MellitusDocument10 pagesNIH Public Access: Vitamin D and Gestational Diabetes MellitusMabel StracciaNo ratings yet
- Hashimoto 2015Document4 pagesHashimoto 2015Mabel StracciaNo ratings yet
- Lucica GA-L Glycated Albumin Assay Kit: A New Diagnostic Test For Diabetes MellitusDocument3 pagesLucica GA-L Glycated Albumin Assay Kit: A New Diagnostic Test For Diabetes MellitusMabel StracciaNo ratings yet
- Transferable Vancomycin Resistance in A Community-Associated MRSA LineageDocument8 pagesTransferable Vancomycin Resistance in A Community-Associated MRSA LineageMabel StracciaNo ratings yet
- Palliative Care: NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines)Document101 pagesPalliative Care: NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines)jackeline RodriguezNo ratings yet
- Pterygium CaseDocument8 pagesPterygium CaseNandita JaliNo ratings yet
- Induction and Augmentation of LaborDocument20 pagesInduction and Augmentation of Laborjssamc prasootitantraNo ratings yet
- Krisdayani Martha Sukma (P1337424117012) Vio Waliyatun Hasna (P1337424117036)Document5 pagesKrisdayani Martha Sukma (P1337424117012) Vio Waliyatun Hasna (P1337424117036)LabibaNo ratings yet
- B2 MicroglobulinDocument1 pageB2 MicroglobulinPhong Nguyễn WindyNo ratings yet
- Case Formulation in PsychiatryDocument8 pagesCase Formulation in PsychiatryMarius PaţaNo ratings yet
- Odontogenic CystsDocument5 pagesOdontogenic CystsBH ASMRNo ratings yet
- Definition of Terms: Herbaceous Plant Costaceae Brazil Bahia Espirito SantoDocument1 pageDefinition of Terms: Herbaceous Plant Costaceae Brazil Bahia Espirito SantoAshly Jamiah DelRosario ManatoNo ratings yet
- Position PaperDocument1 pagePosition PaperTristan Josh FortichNo ratings yet
- Traumatic Aortic RuptureDocument20 pagesTraumatic Aortic RuptureLisa MoyoNo ratings yet
- IHD - JalalDocument46 pagesIHD - JalalMituran IshwarNo ratings yet
- Viral Diseases in Honey BeesDocument7 pagesViral Diseases in Honey BeesMalsawmsanga ChhakchhuakNo ratings yet
- Management of Renal Stones: Theme From January 2013 ExamDocument123 pagesManagement of Renal Stones: Theme From January 2013 ExamBela VitoriaNo ratings yet
- Love To Fear You - Kati McRaeDocument310 pagesLove To Fear You - Kati McRaeKlee IdkNo ratings yet
- MHP 1Document3 pagesMHP 1Asna anwerNo ratings yet
- Efficacy of The anti-VZV (anti-HSV3) Vaccine in HSV1 and HSV2 Recurrent Herpes Simplex Disease: A Prospective StudyDocument8 pagesEfficacy of The anti-VZV (anti-HSV3) Vaccine in HSV1 and HSV2 Recurrent Herpes Simplex Disease: A Prospective StudymostafaNo ratings yet
- English 3 w5Document6 pagesEnglish 3 w5Almie Adarayan BrosotoNo ratings yet
- Fish and Shell Fish Immunology: Full Length ArticleDocument9 pagesFish and Shell Fish Immunology: Full Length ArticleKirana Rahmada SafitriNo ratings yet
- CS Drug Study NotesDocument11 pagesCS Drug Study NotestwnynyiskaNo ratings yet
- Kathryn Clavier ResumeDocument2 pagesKathryn Clavier Resumeapi-654404237No ratings yet
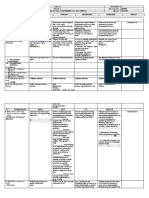
- DLL Mapeh g4 q2 w3Document6 pagesDLL Mapeh g4 q2 w3Daniel MingoyNo ratings yet
- April 3, 2020 Strathmore TimesDocument12 pagesApril 3, 2020 Strathmore TimesStrathmore TimesNo ratings yet
- TPS 2020 Bahasa InggrisDocument9 pagesTPS 2020 Bahasa InggrisYopi Panca YudhaNo ratings yet
- Urinary Tract InfectionDocument50 pagesUrinary Tract InfectionJanuaryNo ratings yet
- Chole CystitisDocument1 pageChole CystitisEirah Nicole JumawanNo ratings yet