You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Anger, Hostility and AggressionDocument15 pagesAnger, Hostility and AggressionJhoe NuevoNo ratings yet
- Principles of Geriatric Physiotherapy-CDDocument194 pagesPrinciples of Geriatric Physiotherapy-CDFerdinan Fangestu100% (2)
- Nursing Job DescriptionDocument3 pagesNursing Job DescriptionmineasaroeunNo ratings yet
- Impact Events Scale RevisedDocument2 pagesImpact Events Scale RevisedRoxana HolicNo ratings yet
- Bag TechniqueDocument14 pagesBag TechniqueCarissa De Luzuriaga-Balaria100% (1)
- Dementia Rating ScaleDocument2 pagesDementia Rating ScaleIqbal BaryarNo ratings yet
- Bio Mechanics of Tai Chi - A ReviewDocument13 pagesBio Mechanics of Tai Chi - A Reviewjopepinho5796No ratings yet
- Step-Up To GeriatricsDocument328 pagesStep-Up To GeriatricsPhiNguyen89% (9)
- Nursing For Wellness in Older Adults 8th Edition Ebook PDFDocument61 pagesNursing For Wellness in Older Adults 8th Edition Ebook PDFhelena.williams785100% (41)
- Patterns of Nursing Care Delivery in IndiaDocument22 pagesPatterns of Nursing Care Delivery in IndiaJeenaJohn100% (2)
- 阿茲海默症之生物標記Document31 pages阿茲海默症之生物標記洪侊增No ratings yet
- Overview of Integrated Eldercare CourseDocument2 pagesOverview of Integrated Eldercare Coursedelap05No ratings yet
- Beck's Depression ScaleDocument5 pagesBeck's Depression ScaleVitalia Putri PradanaNo ratings yet
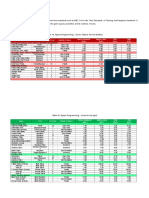
- Spatial programming parametersDocument7 pagesSpatial programming parametersDaryl Deladia DichosoNo ratings yet
- BibliographyDocument7 pagesBibliographyptsievccdNo ratings yet
- Evidence Based Practice - A Primer For Paramedics - Prehospital Research Support Site PDFDocument6 pagesEvidence Based Practice - A Primer For Paramedics - Prehospital Research Support Site PDFcarloshgmedeirosNo ratings yet
- Cynthia Stierman ResumeDocument2 pagesCynthia Stierman Resumeapi-487498704No ratings yet
- 2187 Optiflo Brochure AW Amended WebDocument2 pages2187 Optiflo Brochure AW Amended WebShalom BhopaleNo ratings yet
- Public vs Private Healthcare Findings on Income, Services and SatisfactionDocument4 pagesPublic vs Private Healthcare Findings on Income, Services and SatisfactionapplesbyNo ratings yet
- Intradermal Meds ChecklistDocument2 pagesIntradermal Meds ChecklistMonika Sarmiento100% (1)
- The Importance of Diagnosing and Managing ICU DeliriumDocument13 pagesThe Importance of Diagnosing and Managing ICU DeliriumPablo RamirezNo ratings yet
- 2018-Journal of The American Geriatrics SocietyDocument369 pages2018-Journal of The American Geriatrics SocietyKevin PatrickNo ratings yet
- Total Knee Replacement Surgery TKR IndiaDocument3 pagesTotal Knee Replacement Surgery TKR IndiaAnonymous x8fY69CrnNo ratings yet
- Aira Noreen Leyva - Resume ReviewDocument2 pagesAira Noreen Leyva - Resume Reviewapi-447475293No ratings yet
- Fall Prevention in Elderly AaprmDocument9 pagesFall Prevention in Elderly AaprmNaren RenNo ratings yet
- A Review of Screening Tests For Cognitive ImpairmentDocument22 pagesA Review of Screening Tests For Cognitive ImpairmentSaravananNo ratings yet
- Client Care Plan with Nursing GoalsDocument1 pageClient Care Plan with Nursing GoalsTancred UyNo ratings yet
- 2 Nutrition and AgingDocument11 pages2 Nutrition and AgingAlyzza Zheena Leyva AqueNo ratings yet
- Republic of The Philippines University Town, Northern SamarDocument5 pagesRepublic of The Philippines University Town, Northern SamarZalde TuballasNo ratings yet
- Geriatric Assessment of Lola MaconDocument4 pagesGeriatric Assessment of Lola MaconMark Zedrix MediarioNo ratings yet