You might also like
- Local Anesthesia Made Easy: Complete Guide on How to make your Local Anesthetic Procedure a Success (Including a List of Anesthetic Equipment and their Uses)From EverandLocal Anesthesia Made Easy: Complete Guide on How to make your Local Anesthetic Procedure a Success (Including a List of Anesthetic Equipment and their Uses)No ratings yet
- Equipment Evaluation ReportDocument6 pagesEquipment Evaluation ReportemotionkuNo ratings yet
- Differentiating Anesthesia Equipment: Identify and Understand Anesthesia Equipment in 1 Hour (Including the most popular manufacturers and suppliers to buy Anesthesia Equipment)From EverandDifferentiating Anesthesia Equipment: Identify and Understand Anesthesia Equipment in 1 Hour (Including the most popular manufacturers and suppliers to buy Anesthesia Equipment)No ratings yet
- Types of InhalersDocument23 pagesTypes of Inhalersshamie1110No ratings yet
- Aersolterapia HTMLDocument21 pagesAersolterapia HTMLEN BUNo ratings yet
- An Introduction To InhalersDocument21 pagesAn Introduction To Inhalerswd4899237No ratings yet
- How To Choose Delivery Devices For Asthma: Leading ArticlesDocument3 pagesHow To Choose Delivery Devices For Asthma: Leading ArticlescryptoNo ratings yet
- Description of The Product:: Instructions: Think of A Specific Equipment/product /item That Is Applicable ToDocument4 pagesDescription of The Product:: Instructions: Think of A Specific Equipment/product /item That Is Applicable ToSlepy chngNo ratings yet
- Nebulization PRDocument8 pagesNebulization PRAmy LalringhluaniNo ratings yet
- How To Use InhalerDocument84 pagesHow To Use InhalerharyatiNo ratings yet
- What Are Nebulizers and Why Use ThemDocument3 pagesWhat Are Nebulizers and Why Use ThemcryptoNo ratings yet
- Nebulization and MDIDocument31 pagesNebulization and MDIAlvin E. PeraltaNo ratings yet
- Metered Dose InhalersDocument16 pagesMetered Dose InhalerssahildhingaliNo ratings yet
- Pumonary Drug Delivery Sy 3856380Document30 pagesPumonary Drug Delivery Sy 3856380Chaitanya Kumar ReddyNo ratings yet
- Routes of Drug Delivery To The LungsDocument4 pagesRoutes of Drug Delivery To The LungsAquiles VaestoNo ratings yet
- A Practical Guide To Nebulization TherapyDocument23 pagesA Practical Guide To Nebulization Therapyshahajahan_aa100% (1)
- Mdi & DpiDocument14 pagesMdi & DpiFandi HarmikiNo ratings yet
- About A Metered-Dose Inhaler (MDI)Document6 pagesAbout A Metered-Dose Inhaler (MDI)Sasgia ArumNo ratings yet
- Nebu&CPTDocument32 pagesNebu&CPTAbigail Bantayan100% (1)
- Neb Ul IzationDocument29 pagesNeb Ul Izationannududi378556No ratings yet
- NebulizationDocument2 pagesNebulizationArmie Joy Embat CariazoNo ratings yet
- NebulisationDocument26 pagesNebulisationSilpa Jose TNo ratings yet
- Inhaler: Types: 1. Metered-Dose InhalersDocument10 pagesInhaler: Types: 1. Metered-Dose InhalersGhulam MurtazaNo ratings yet
- Inhaller, Turbuhaler, Disk Haler Dan NebulizerDocument1 pageInhaller, Turbuhaler, Disk Haler Dan NebulizerhendiwijayantoNo ratings yet
- NebulizationDocument4 pagesNebulizationleoNo ratings yet
- Comparing Clinical Features of The Nebulizer, Metered-Dose Inhaler, and Dry Powder InhalerDocument10 pagesComparing Clinical Features of The Nebulizer, Metered-Dose Inhaler, and Dry Powder InhalerDesi EryonNo ratings yet
- Aerosol TherapyDocument10 pagesAerosol Therapy04lubna_869632400No ratings yet
- Dyspnea and NebulizationDocument42 pagesDyspnea and NebulizationHema AnkamreddyNo ratings yet
- A Practical Guide To Nebulization TherapyDocument24 pagesA Practical Guide To Nebulization TherapySidhartha Satapathy100% (2)
- Inhalationtherapy 120807161343 Phpapp02Document38 pagesInhalationtherapy 120807161343 Phpapp02Anonymous X0Rm9zNo ratings yet
- Terapi Inhalasi Pit Pdui 8Document36 pagesTerapi Inhalasi Pit Pdui 8Noval LiadyNo ratings yet
- Aero SalDocument3 pagesAero SalPoova RagavanNo ratings yet
- Adult NebuliserDocument13 pagesAdult NebuliserBeh Boon CongNo ratings yet
- Drug Delivery and Its Developments For Pulmonary System: Available Online atDocument17 pagesDrug Delivery and Its Developments For Pulmonary System: Available Online atayusisminarniNo ratings yet
- Nebulization: Presented By: Ms. Sinsu Rachel Alex Msc. (N) Prev YrDocument29 pagesNebulization: Presented By: Ms. Sinsu Rachel Alex Msc. (N) Prev Yrmanoj reddy100% (1)
- How To Use A Metered Dose Inhaler - Breathe Freely NetworkDocument8 pagesHow To Use A Metered Dose Inhaler - Breathe Freely NetworkJiela CarbonillaNo ratings yet
- CD NebDocument8 pagesCD NebPATEL NEHAKUMARI VIMALBHAINo ratings yet
- NebulizationprocedureDocument20 pagesNebulizationprocedureSyehta WardaniNo ratings yet
- Natural HerbsDocument5 pagesNatural HerbsMohammad ZameeruddinNo ratings yet
- Nebulization (Final Output)Document5 pagesNebulization (Final Output)Tamil Villardo100% (2)
- Pharmaceutical AerosolDocument9 pagesPharmaceutical AerosolMaruf MominNo ratings yet
- Rle Procedure StudyDocument4 pagesRle Procedure StudyMyangel LoiseNo ratings yet
- Nebuliser - Care of Your NebuliserDocument13 pagesNebuliser - Care of Your NebuliserRahulNargotraNo ratings yet
- International Journal of Research in Pharmaceutical SciencesDocument16 pagesInternational Journal of Research in Pharmaceutical SciencesSatyam SachanNo ratings yet
- Metered Dose Inhalers and Spacer Devices: C. TerzanoDocument11 pagesMetered Dose Inhalers and Spacer Devices: C. TerzanoDwi MindriNo ratings yet
- Incentive SpirometerDocument25 pagesIncentive SpirometerAnalyn Salvacion100% (2)
- Terapi InhalasiDocument4 pagesTerapi Inhalasiblueiceland100% (1)
- NebulizationDocument8 pagesNebulizationbajaocNo ratings yet
- Ppk-Lf-Far-004-I-2016 InhalasiDocument2 pagesPpk-Lf-Far-004-I-2016 InhalasiVivi SusantiNo ratings yet
- Resp Handout - 3rd YearDocument15 pagesResp Handout - 3rd YearNuruddin MuhamadNo ratings yet
- Neb Ul IzationDocument28 pagesNeb Ul Izationlawkumar952387No ratings yet
- Home Nebulizer TherapyDocument6 pagesHome Nebulizer TherapyOdie MoralesNo ratings yet
- NEBULIZATIONDocument21 pagesNEBULIZATIONjohncarneo400No ratings yet
- Nurs - 00 - Nebulizer A Nebulizer Changes Liquid Medicine Into Fine Droplets (In Aerosol orDocument6 pagesNurs - 00 - Nebulizer A Nebulizer Changes Liquid Medicine Into Fine Droplets (In Aerosol orYmon TuallaNo ratings yet
- Neb Ul Ization 2Document31 pagesNeb Ul Ization 2RegineJoyCarinoNo ratings yet
- Nebulization and Steam InhalationDocument31 pagesNebulization and Steam InhalationManisha Thakur100% (1)
- Nebulization and Steam InhalationDocument31 pagesNebulization and Steam InhalationManisha Thakur100% (1)
- NebulizerDocument15 pagesNebulizerEndahNo ratings yet
- SuctionDocument9 pagesSuctionNovi LisnawatiNo ratings yet
- Evidence From Thomas Croft Euthanasia and Assisted Suicide A Legal and Ethical DilemmaDocument14 pagesEvidence From Thomas Croft Euthanasia and Assisted Suicide A Legal and Ethical Dilemmaaneece786No ratings yet
- Reichert Cone Concentrator SystemDocument9 pagesReichert Cone Concentrator Systemaneece786No ratings yet
- Polar MoleculeDocument2 pagesPolar Moleculeaneece786No ratings yet
- Acetylsalicylic AcidDocument3 pagesAcetylsalicylic Acidaneece786No ratings yet
- Entropy, Gibbs EnergyDocument4 pagesEntropy, Gibbs Energyaneece786No ratings yet
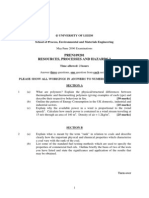
- PREN109201 Resources, Processes and Hazards 2Document3 pagesPREN109201 Resources, Processes and Hazards 2aneece786No ratings yet
- PREN109201 Resources, Processes and Hazards 2: School of Process, Environmental and Materials EngineeringDocument2 pagesPREN109201 Resources, Processes and Hazards 2: School of Process, Environmental and Materials Engineeringaneece786No ratings yet
- Sulphonation and LABS Formulation Using SO3-AIR MethodDocument3 pagesSulphonation and LABS Formulation Using SO3-AIR Methodaneece786No ratings yet
- 1e3rd - Medication NotesDocument35 pages1e3rd - Medication NotesKen LaguiabNo ratings yet
- Medical Auditing Training: CPMA®: Practical Application WorkbookDocument32 pagesMedical Auditing Training: CPMA®: Practical Application WorkbookAnthony El HageNo ratings yet
- Guide For Alternative Inhalers During Stock Shortages Related To Coronavirus (COVID-19)Document2 pagesGuide For Alternative Inhalers During Stock Shortages Related To Coronavirus (COVID-19)Devs AbdouNo ratings yet
- MARTDocument3 pagesMARTIncy CyvaNo ratings yet
- 3607micro Moments Jan 2013 Low Res PDFDocument24 pages3607micro Moments Jan 2013 Low Res PDFSiddhartha PachisiaNo ratings yet
- v1200 Owners ManualDocument2 pagesv1200 Owners ManualDanny MartinNo ratings yet
- B.well SwissDocument1 pageB.well SwissZumrud QafarliNo ratings yet
- Module 4 - Topic 1 AsthmaDocument22 pagesModule 4 - Topic 1 AsthmaZEITAIMENo ratings yet
- Inhalation or Aerosols Therapy1Document21 pagesInhalation or Aerosols Therapy1drnasir31No ratings yet
- Principles of Nano-Sized Drug Delivery SystemsDocument81 pagesPrinciples of Nano-Sized Drug Delivery SystemsMelis Nur YılmazNo ratings yet
- Severe Asthma Patient Referral ChecklistDocument4 pagesSevere Asthma Patient Referral Checklistsiti nur aishah jalilNo ratings yet
- Medicine Name by Company Wise in Goribullah PharmacyDocument22 pagesMedicine Name by Company Wise in Goribullah PharmacyAbdul KaderNo ratings yet
- Iadt 03 I 3 P 176Document2 pagesIadt 03 I 3 P 176Santhosh MohanNo ratings yet
- Asthalin InhalerDocument5 pagesAsthalin InhalerRajib MandalNo ratings yet
- Ashama Best Home RemdiesDocument57 pagesAshama Best Home RemdiesRahulsinghoooo100% (1)
- 46 Emergency Motion For Release From CustodyDocument5 pages46 Emergency Motion For Release From CustodyJake OffenhartzNo ratings yet
- FDA Briefing Book - TOBIDocument135 pagesFDA Briefing Book - TOBISnigdha Santra SaxenaNo ratings yet
- Discharge Planning ASTHMADocument4 pagesDischarge Planning ASTHMANadja JamilahNo ratings yet
- Module 4 - Nebulization Through Aerosol Mask Metered-Dose Inhaler STUDENTDocument5 pagesModule 4 - Nebulization Through Aerosol Mask Metered-Dose Inhaler STUDENTfebie pachecoNo ratings yet
- Dosage Forms 2Document91 pagesDosage Forms 2Palak BatraNo ratings yet
- Types of DFDocument48 pagesTypes of DFIdenyi Daniel EwaNo ratings yet
- Review of Related Literature On Blood PressureDocument9 pagesReview of Related Literature On Blood Pressureaflrpjser100% (1)
- Adult Asthma Action PlanDocument2 pagesAdult Asthma Action PlanantonioforteseNo ratings yet
- Metered Dose Inhaler (Mdi)Document4 pagesMetered Dose Inhaler (Mdi)arn0ld21No ratings yet
- How To Use Your Ellipta Inhaler: Why Is Inhaler Technique Important?Document2 pagesHow To Use Your Ellipta Inhaler: Why Is Inhaler Technique Important?rayy taeNo ratings yet
- Respiratory Drugs Midterm ExamDocument10 pagesRespiratory Drugs Midterm ExamKevin VillaranteNo ratings yet
- bIOLOGIC cRISIS FINAL QUIZ pHARMACOCHENETICSDocument35 pagesbIOLOGIC cRISIS FINAL QUIZ pHARMACOCHENETICSSusan MaglaquiNo ratings yet
- Practice-Tests Correction: Estimated Grade BDocument1 pagePractice-Tests Correction: Estimated Grade BDr. Emad Elbadawy د عماد البدويNo ratings yet
- Aerosol Science and Technology Final EliasDocument50 pagesAerosol Science and Technology Final EliassmithalexNo ratings yet
- v1200 Owners Manual PDFDocument2 pagesv1200 Owners Manual PDFDanny MartinNo ratings yet
- Machinery Lubrication Technician (MLT) I and II Certification Exam GuideFrom EverandMachinery Lubrication Technician (MLT) I and II Certification Exam GuideRating: 2 out of 5 stars2/5 (1)
- Well Integrity for Workovers and RecompletionsFrom EverandWell Integrity for Workovers and RecompletionsRating: 5 out of 5 stars5/5 (3)
- Well Control for Completions and InterventionsFrom EverandWell Control for Completions and InterventionsRating: 4 out of 5 stars4/5 (10)
- Asset Integrity Management for Offshore and Onshore StructuresFrom EverandAsset Integrity Management for Offshore and Onshore StructuresNo ratings yet
- Advanced Production Decline Analysis and ApplicationFrom EverandAdvanced Production Decline Analysis and ApplicationRating: 3.5 out of 5 stars3.5/5 (4)
- Internal Combustion: How Corporations and Governments Addicted the World to Oil and Subverted the AlternativesFrom EverandInternal Combustion: How Corporations and Governments Addicted the World to Oil and Subverted the AlternativesRating: 4 out of 5 stars4/5 (2)
- Asphaltene Deposition Control by Chemical Inhibitors: Theoretical and Practical ProspectsFrom EverandAsphaltene Deposition Control by Chemical Inhibitors: Theoretical and Practical ProspectsNo ratings yet
- Hydrocarbon Fluid Inclusions in Petroliferous BasinsFrom EverandHydrocarbon Fluid Inclusions in Petroliferous BasinsNo ratings yet
- Casing and Liners for Drilling and Completion: Design and ApplicationFrom EverandCasing and Liners for Drilling and Completion: Design and ApplicationRating: 5 out of 5 stars5/5 (3)
- An Operations Guide to Safety and Environmental Management Systems (SEMS): Making Sense of BSEE SEMS RegulationsFrom EverandAn Operations Guide to Safety and Environmental Management Systems (SEMS): Making Sense of BSEE SEMS RegulationsNo ratings yet
- Oil: An Overview of the Petroleum IndustryFrom EverandOil: An Overview of the Petroleum IndustryRating: 4.5 out of 5 stars4.5/5 (3)
- Essentials of Oil and Gas Utilities: Process Design, Equipment, and OperationsFrom EverandEssentials of Oil and Gas Utilities: Process Design, Equipment, and OperationsRating: 4.5 out of 5 stars4.5/5 (4)
- A Practical Guide to Piping and Valves for the Oil and Gas IndustryFrom EverandA Practical Guide to Piping and Valves for the Oil and Gas IndustryRating: 5 out of 5 stars5/5 (3)
- Deepwater Drilling: Well Planning, Design, Engineering, Operations, and Technology ApplicationFrom EverandDeepwater Drilling: Well Planning, Design, Engineering, Operations, and Technology ApplicationRating: 4.5 out of 5 stars4.5/5 (2)
- Industrial Piping and Equipment Estimating ManualFrom EverandIndustrial Piping and Equipment Estimating ManualRating: 5 out of 5 stars5/5 (7)