You might also like
- Jurnal Mata 5Document6 pagesJurnal Mata 5Dahru KinanggaNo ratings yet
- 8894 Jacobs2017Document11 pages8894 Jacobs2017Fahrizal Al-fatihNo ratings yet
- Ledderose2021 Article EndoscopicEndonasalRepairOfComDocument7 pagesLedderose2021 Article EndoscopicEndonasalRepairOfComAlejandra Oliveros VargasNo ratings yet
- Articulo 8Document7 pagesArticulo 8Marcela RodriguezNo ratings yet
- Lower Eyelid Complications Associated With Transconjunctival Versus Subciliary Approaches To Orbital Floor FracturesDocument5 pagesLower Eyelid Complications Associated With Transconjunctival Versus Subciliary Approaches To Orbital Floor Fracturesstoia_sebiNo ratings yet
- Steriod Cataract PDFDocument4 pagesSteriod Cataract PDFLisa IskandarNo ratings yet
- Episcleral Brachytherapy For RetinoblastomaDocument6 pagesEpiscleral Brachytherapy For Retinoblastomamadimadi11No ratings yet
- Multimodal Treatment in Pediatric Orbital Rhabdomyosarcoma: About 8 CasesDocument3 pagesMultimodal Treatment in Pediatric Orbital Rhabdomyosarcoma: About 8 CasesIJAR JOURNALNo ratings yet
- Efficacy of Second-Course Intra-Arterial Chemo-Therapy in Children For Advanced Retinoblastoma Recurrence After Intra-Arterial ChemotherapyDocument4 pagesEfficacy of Second-Course Intra-Arterial Chemo-Therapy in Children For Advanced Retinoblastoma Recurrence After Intra-Arterial ChemotherapyilhamNo ratings yet
- Effective Dose of Dental CBCT LudlowDocument25 pagesEffective Dose of Dental CBCT LudlowMaríaPazSalinasVillagraNo ratings yet
- Retinoblastoma - EyeWikiDocument11 pagesRetinoblastoma - EyeWikimay171989No ratings yet
- Prophylactic Cervical Lymph Node Irradiation Provides No Benefit For Patients of Stage IE Extranodal Natural Killer/t Cell Lymphoma, Nasal TypeDocument8 pagesProphylactic Cervical Lymph Node Irradiation Provides No Benefit For Patients of Stage IE Extranodal Natural Killer/t Cell Lymphoma, Nasal TypeCleysser Antonio Custodio PolarNo ratings yet
- Tugas Ibu RetinoblastomaDocument7 pagesTugas Ibu RetinoblastomamalaNo ratings yet
- Efficacy and Toxicity of Intravitreous Chemotherapy For Retinoblastoma: Four-Year ExperienceDocument8 pagesEfficacy and Toxicity of Intravitreous Chemotherapy For Retinoblastoma: Four-Year ExperienceSlr RandiNo ratings yet
- Pediatric Orbital Cellulitis Experience from Tertiary CenterDocument3 pagesPediatric Orbital Cellulitis Experience from Tertiary CenterMuthu V RanNo ratings yet
- Splenectomy For Immune Thrombocytopenic Purpura: Surgery For The 21st CenturyDocument4 pagesSplenectomy For Immune Thrombocytopenic Purpura: Surgery For The 21st Centurykevin stefanoNo ratings yet
- Brolucizumab EstudioDocument13 pagesBrolucizumab EstudioJuan Carlos Mejía SernaNo ratings yet
- Iris Melanoma Diagnosis and Conservative Treatment OutcomesDocument7 pagesIris Melanoma Diagnosis and Conservative Treatment Outcomesmiftahul masruriNo ratings yet
- Articol MedicalDocument4 pagesArticol MedicalCBkingstonNo ratings yet
- None 3Document11 pagesNone 3Yehiel FlaviusNo ratings yet
- Serial Laser Treatment Controls Vocal Fold LeukoplakiaDocument8 pagesSerial Laser Treatment Controls Vocal Fold LeukoplakiaG WNo ratings yet
- Surgical Intervention of Periocular Infantile Hemangiomas in the Era of β-BlockersDocument4 pagesSurgical Intervention of Periocular Infantile Hemangiomas in the Era of β-BlockersLuisa Fernanda ArboledaNo ratings yet
- Penetrating Keratoplasty in Active Acanthamoeba KeratitisDocument5 pagesPenetrating Keratoplasty in Active Acanthamoeba Keratitisdrvishalkulkarni2007No ratings yet
- Alamanos 2016Document12 pagesAlamanos 2016dana40018256No ratings yet
- PBC 20606Document5 pagesPBC 20606skocabzzNo ratings yet
- Primary Surgery Versus Chemoradiotherapy For Advanced Oropharyngeal Cancers: A Longitudinal Population StudyDocument7 pagesPrimary Surgery Versus Chemoradiotherapy For Advanced Oropharyngeal Cancers: A Longitudinal Population StudyLuvita Amallia SyadhatinNo ratings yet
- Differences Between Children and Adults With Otitis Media With Effusion Treated With CO Laser MyringotomyDocument7 pagesDifferences Between Children and Adults With Otitis Media With Effusion Treated With CO Laser MyringotomyIndra PratamaNo ratings yet
- Tic Treatment of Teeth With Apical Period On Tit Is Single vs. Multi Visit TreatmentDocument6 pagesTic Treatment of Teeth With Apical Period On Tit Is Single vs. Multi Visit Treatmentgpv38No ratings yet
- PARS Reader's Digest - Jan 2013Document9 pagesPARS Reader's Digest - Jan 2013info8673No ratings yet
- Miiringotomi OMEDocument7 pagesMiiringotomi OMEamaliaNo ratings yet
- The Number of Karyorrhexis in PatientsDocument5 pagesThe Number of Karyorrhexis in PatientsAdhitya Sofiyati DewiNo ratings yet
- Clinical Characteristics and Surgical Outcomes in Patients With Intermittent ExotropiaDocument6 pagesClinical Characteristics and Surgical Outcomes in Patients With Intermittent ExotropiaIkmal ShahromNo ratings yet
- Survival and Complications of Zygomatic Implants (PDFDrive)Document36 pagesSurvival and Complications of Zygomatic Implants (PDFDrive)Lê Minh KhôiNo ratings yet
- Retina Clinica Trials Update - 0813 - Supp2Document16 pagesRetina Clinica Trials Update - 0813 - Supp2cmirceaNo ratings yet
- Otolaryngology Journal Article on Proliferative Verrucous LeukoplakiaDocument2 pagesOtolaryngology Journal Article on Proliferative Verrucous LeukoplakiaGus JanantaraNo ratings yet
- PARS Reader's Digest - Apr 2013Document12 pagesPARS Reader's Digest - Apr 2013info8673No ratings yet
- 102 FullDocument5 pages102 FullMohebNo ratings yet
- Effets Pronostiques de La Chirurgie Ou de La Radiothérapie Sur Le Carcinome Adénoïde Kystique de La Tête Et Du CouDocument17 pagesEffets Pronostiques de La Chirurgie Ou de La Radiothérapie Sur Le Carcinome Adénoïde Kystique de La Tête Et Du CouMamadou DIENENo ratings yet
- Dental ArticleDocument7 pagesDental ArticleBen LevineNo ratings yet
- Engel 2018Document11 pagesEngel 2018GonzaloNo ratings yet
- Research ArticleDocument10 pagesResearch ArticleastutikNo ratings yet
- 157 161 RadiotherapyDocument5 pages157 161 RadiotherapyEko SetiawanNo ratings yet
- European Multicenter Trial of The Prevention of Cystoid Macular Edema After Cataract Surgery in Nondiabetics: ESCRS PREMED Study Report 1Document11 pagesEuropean Multicenter Trial of The Prevention of Cystoid Macular Edema After Cataract Surgery in Nondiabetics: ESCRS PREMED Study Report 1salvadorNo ratings yet
- Landmark Studies in GlaucomaDocument53 pagesLandmark Studies in GlaucomaDrEknathPawarNo ratings yet
- 10.1007@s00405 016 3899 3Document5 pages10.1007@s00405 016 3899 3Vincentius Novian RomilioNo ratings yet
- Radiofrequency Ablation of Small Follicular Neoplasms Initial Clinical OutcomesDocument8 pagesRadiofrequency Ablation of Small Follicular Neoplasms Initial Clinical Outcomesivan dario hernandez erazoNo ratings yet
- 02 In-Office Laryngeal Procedures (IOLP) in CanadaDocument6 pages02 In-Office Laryngeal Procedures (IOLP) in CanadaG WNo ratings yet
- Ultrasound in Emergency Medicine: Use of Ocular Ultrasound For The Evaluation of Retinal DetachmentDocument5 pagesUltrasound in Emergency Medicine: Use of Ocular Ultrasound For The Evaluation of Retinal DetachmentZarella Ramírez BorreroNo ratings yet
- Medip,+15 59 1 CEDocument7 pagesMedip,+15 59 1 CEKabir Ahmed LaskarNo ratings yet
- Fractionated Radiation For MeningiomasDocument2 pagesFractionated Radiation For MeningiomasGil LedermanNo ratings yet
- Outcomes of Descemet Membrane Endothelial Keratoplasty in Patients With PreviouDocument6 pagesOutcomes of Descemet Membrane Endothelial Keratoplasty in Patients With PreviouRaúl Plasencia SaliniNo ratings yet
- Health Effects From Exposure To Dental Diagnostic X-Ray: Environmental Health and ToxicologyDocument6 pagesHealth Effects From Exposure To Dental Diagnostic X-Ray: Environmental Health and ToxicologyhelmysiswantoNo ratings yet
- Pediatric Sialoblastoma Evaluation and ManagementDocument22 pagesPediatric Sialoblastoma Evaluation and ManagementDear Farah SielmaNo ratings yet
- 247 2011 Article 2201 PDFDocument13 pages247 2011 Article 2201 PDFArdianNo ratings yet
- Powell 1995Document9 pagesPowell 1995Phạm Thanh NhânNo ratings yet
- A Painful Red EyeDocument2 pagesA Painful Red EyeCristhian Agustin ParedesNo ratings yet
- What's New in Spine Surgery: Specialty UpdateDocument11 pagesWhat's New in Spine Surgery: Specialty UpdatePoliceNo ratings yet
- Lack of Efficacy of Long-Term, Low-Dose Azithromycin in Chronic Rhinosinusitis: A Randomized Controlled TrialDocument12 pagesLack of Efficacy of Long-Term, Low-Dose Azithromycin in Chronic Rhinosinusitis: A Randomized Controlled Trialpaijo09No ratings yet
- Choroidal NeovascularizationFrom EverandChoroidal NeovascularizationJay ChhablaniNo ratings yet
- Blepharitis: A Comprehensive Clinical GuideFrom EverandBlepharitis: A Comprehensive Clinical GuideAsim V. FarooqNo ratings yet
- Schaum S Outline of Human A PDFDocument193 pagesSchaum S Outline of Human A PDFFahlevie EpinNo ratings yet
- I12 Surg Hand Scrub - 2 - 121945 PDFDocument6 pagesI12 Surg Hand Scrub - 2 - 121945 PDFFikaAriskaNo ratings yet
- Tranexamic Acid For Spontaneous Intracerebral Hemorrhage A Randomized Controlled Pilot TrialDocument7 pagesTranexamic Acid For Spontaneous Intracerebral Hemorrhage A Randomized Controlled Pilot TrialAnsh NviariyntiNo ratings yet
- PTC EngDocument39 pagesPTC EngFahlevie Epin100% (1)
- DM Retinopati JurnalDocument36 pagesDM Retinopati JurnalAmelia PutriNo ratings yet
- Diabetic Retinopathy:: Prevention, Treatment and DietDocument2 pagesDiabetic Retinopathy:: Prevention, Treatment and DietFahlevie EpinNo ratings yet
- DM Retinopati JurnalDocument36 pagesDM Retinopati JurnalAmelia PutriNo ratings yet
- Primary Trauma Care: Authors Douglas A Wilkinson and Marcus W SkinnerDocument51 pagesPrimary Trauma Care: Authors Douglas A Wilkinson and Marcus W SkinnerFahlevie EpinNo ratings yet
- Diabetes Retinopathy GuidelineDocument24 pagesDiabetes Retinopathy GuidelineFahlevie EpinNo ratings yet
- Antibiotics: Choices For Common InfectionsDocument30 pagesAntibiotics: Choices For Common InfectionsAlfeus GradyNo ratings yet
- WHO Pain LadderDocument1 pageWHO Pain LadderBagus Burhan MuhammadNo ratings yet
- STEMI-Optimal Antiplateletantithrombotic in Emergency DepDocument5 pagesSTEMI-Optimal Antiplateletantithrombotic in Emergency DepFadhilAfifNo ratings yet
- Kuliah Urinary Tract StoneDocument31 pagesKuliah Urinary Tract StoneMisbahsaragihNo ratings yet
- Uro - Radiologi: Iskandar ZakariaDocument47 pagesUro - Radiologi: Iskandar ZakariaFahlevie EpinNo ratings yet
- Soal-Soal UKDI dr.Rahma Tsania Zhuhra FK UNANDDocument1 pageSoal-Soal UKDI dr.Rahma Tsania Zhuhra FK UNANDFahlevie EpinNo ratings yet
- 2.1 Classification of SVT by Structures Required For Initiation and Maintenance......Document1 page2.1 Classification of SVT by Structures Required For Initiation and Maintenance......Fahlevie EpinNo ratings yet
- Kul-Tumor Traktus UrogenitalDocument26 pagesKul-Tumor Traktus UrogenitalFahlevie EpinNo ratings yet
- Jurnal ReadingDocument16 pagesJurnal ReadingFahlevie EpinNo ratings yet
- Acute Diarrhea Long FINAL 120604Document24 pagesAcute Diarrhea Long FINAL 120604Aizat KamalNo ratings yet
- Kul-Tumor Traktus UrogenitalDocument21 pagesKul-Tumor Traktus UrogenitalFahlevie EpinNo ratings yet
- Kul-Tumor Traktus UrogenitalDocument26 pagesKul-Tumor Traktus UrogenitalFahlevie EpinNo ratings yet
- Paliatif CareDocument13 pagesPaliatif CareNicholas PetrovskiNo ratings yet
- 17 Visual PathwaysDocument4 pages17 Visual PathwaysFahlevie EpinNo ratings yet
- LEUKOKORIADocument3 pagesLEUKOKORIAFahlevie EpinNo ratings yet
- Rekap Pasien Stase: BTKV Tanggal:17/8/2015: Ruangan: PJTDocument7 pagesRekap Pasien Stase: BTKV Tanggal:17/8/2015: Ruangan: PJTFahlevie EpinNo ratings yet
- Daftar PustakaDocument1 pageDaftar PustakaFahlevie EpinNo ratings yet
- Peripheral Vascular DiseaseDocument8 pagesPeripheral Vascular DiseaseFahlevie EpinNo ratings yet
- ReferensiDocument1 pageReferensiFahlevie EpinNo ratings yet
- BAB V Daftar PustakaDocument2 pagesBAB V Daftar PustakaFahlevie EpinNo ratings yet
- ReferensiDocument1 pageReferensiFahlevie EpinNo ratings yet
- Term Paper ExampleDocument16 pagesTerm Paper ExampleZhengYang ChinNo ratings yet
- Use of Oral Rehydration Therapy in The Treatment of Childhood Diarrhoea in Douala, CameroonDocument5 pagesUse of Oral Rehydration Therapy in The Treatment of Childhood Diarrhoea in Douala, CameroonKiti AstutiNo ratings yet
- Department of HealthDocument2 pagesDepartment of HealthdenNo ratings yet
- Ben - Morgan A Case of Diabetes 2Document2 pagesBen - Morgan A Case of Diabetes 2api-463462603No ratings yet
- Approach To Child With Fever: Liew Qian YiDocument33 pagesApproach To Child With Fever: Liew Qian YinavenNo ratings yet
- Swellings of The JawDocument36 pagesSwellings of The JawSumaNo ratings yet
- Essay-Mike Lemuel BacayoDocument1 pageEssay-Mike Lemuel BacayoLem MikeeNo ratings yet
- Practical Review of Diagnosis and Management of Cutaneous Tuberculosis in IndonesiaDocument6 pagesPractical Review of Diagnosis and Management of Cutaneous Tuberculosis in IndonesiaAde Afriza FeraniNo ratings yet
- Monocyte: FunctionDocument9 pagesMonocyte: FunctionMatelyn OargaNo ratings yet
- Package Leaflet: Information For The User Cetirizine Hydrochloride 5 MG/ 5 ML Oral SolutionDocument7 pagesPackage Leaflet: Information For The User Cetirizine Hydrochloride 5 MG/ 5 ML Oral SolutionZulva Chairunnisa BudimanNo ratings yet
- National Geographic USA - October 2022Document140 pagesNational Geographic USA - October 2022joaquin.ca.garcia80% (5)
- Orthopaedics: Questions&AnswersDocument49 pagesOrthopaedics: Questions&AnswersRajesh Kumar AsunalaNo ratings yet
- Alpha 1 AT DefficiencyDocument22 pagesAlpha 1 AT DefficiencySensing NonsenseNo ratings yet
- MycobacteriumDocument23 pagesMycobacteriumTJ Goli CruzNo ratings yet
- Pharm 316 Case Presentation: Statins in The Golden Years - Statin For Primary Prevention in ElderlyDocument37 pagesPharm 316 Case Presentation: Statins in The Golden Years - Statin For Primary Prevention in ElderlyKevin JiaNo ratings yet
- PDF of Cor Final DessertationDocument71 pagesPDF of Cor Final DessertationJay SharmaNo ratings yet
- Contaminated Drinking Water As A Risk Factor For Colibacilosis - PlusVet Animal HealthDocument8 pagesContaminated Drinking Water As A Risk Factor For Colibacilosis - PlusVet Animal HealthEduardo ViolaNo ratings yet
- Homeopathy For Joint PainsDocument3 pagesHomeopathy For Joint PainsstarhomeoNo ratings yet
- Safety and Operating Instructions: Hydraulic Breakers RX 2, 3, 4, 6, 8Document28 pagesSafety and Operating Instructions: Hydraulic Breakers RX 2, 3, 4, 6, 8juan gonzalez burgosNo ratings yet
- Thalassemia in Iraq Review Article: AbstractDocument4 pagesThalassemia in Iraq Review Article: AbstractRana RaedNo ratings yet
- IL Junior CI Plus Rider (U149) : (IL Unit Deduction Rider - Investment Linked Insurance Plan)Document4 pagesIL Junior CI Plus Rider (U149) : (IL Unit Deduction Rider - Investment Linked Insurance Plan)Lishalini GunasagaranNo ratings yet
- Anaphylactic Reactions 397 ReportsDocument85 pagesAnaphylactic Reactions 397 ReportsJosh SingerNo ratings yet
- Medical History FormatDocument5 pagesMedical History Formatkrzia TehNo ratings yet
- Test Bank Advanced Health Assessment Clinical Diagnosis in Primary Care 6th Edition DainsDocument4 pagesTest Bank Advanced Health Assessment Clinical Diagnosis in Primary Care 6th Edition DainsCarlton Caughey100% (36)
- AQA Biology A-Level: Required Practical 6Document4 pagesAQA Biology A-Level: Required Practical 6Alfred SangNo ratings yet
- Pollution The SDocument15 pagesPollution The SWasil SaipodenNo ratings yet
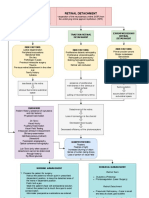
- Retinal Detachment: Traction Retinal Detachment Rhegmatogenous Detachment Exudative/Serous Retinal DetachmentDocument3 pagesRetinal Detachment: Traction Retinal Detachment Rhegmatogenous Detachment Exudative/Serous Retinal DetachmentJordz Placi100% (1)
- TOPIC 6 - Regulatory ControlDocument8 pagesTOPIC 6 - Regulatory ControlOliver100% (1)
- Value of Chest Ultrasound in Diagnosis of Community Acquired PneumoniaDocument5 pagesValue of Chest Ultrasound in Diagnosis of Community Acquired PneumoniaHarlan SiMarmutNo ratings yet
- Transes 1 (PEDIATRICS-LAB)Document2 pagesTranses 1 (PEDIATRICS-LAB)Ashley Judd EmpaynadoNo ratings yet