You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Health History and Phys Exam SP 07 Web VersionDocument19 pagesHealth History and Phys Exam SP 07 Web VersionAdrian CordayNo ratings yet
- Neph301 CommentsDocument1 pageNeph301 CommentsjeffreyianNo ratings yet
- Neph301 CommentsDocument1 pageNeph301 CommentsjeffreyianNo ratings yet
- Nephro301 - 1st AssignmentDocument5 pagesNephro301 - 1st AssignmentjeffreyianNo ratings yet
- 1879 Herald of The MorningDocument104 pages1879 Herald of The MorningjeffreyianNo ratings yet
- Does Mankind Have A SpiritDocument4 pagesDoes Mankind Have A SpiritjeffreyianNo ratings yet
- 06 Case StudiesDocument35 pages06 Case StudiesMAURICIONo ratings yet
- Four Recruitment Scenarios - SWDocument23 pagesFour Recruitment Scenarios - SWjeffreyian0% (1)
- ONA & CUPE - Enrollment FormDocument3 pagesONA & CUPE - Enrollment FormjeffreyianNo ratings yet
- Antriep ResearchDocument53 pagesAntriep ResearchjeffreyianNo ratings yet
- Antriep ResearchDocument53 pagesAntriep ResearchjeffreyianNo ratings yet
- Kai Calling CardDocument1 pageKai Calling CardjeffreyianNo ratings yet
- Fundamental Principles of Administration and SupervisionDocument35 pagesFundamental Principles of Administration and SupervisionRustico Y Jerusalem90% (21)
- IssuesDocument33 pagesIssuesDhif L EenaNo ratings yet
- Community Participation in Quality EducationDocument9 pagesCommunity Participation in Quality EducationBishnu Prasad Mishra100% (5)
- Developed By: Name of Developer Approved By: Name of ApproverDocument14 pagesDeveloped By: Name of Developer Approved By: Name of ApproverjeffreyianNo ratings yet
- 4 18 Perform AppraiseDocument13 pages4 18 Perform AppraisejeffreyianNo ratings yet
- Answer SheetDocument1 pageAnswer SheetjeffreyianNo ratings yet
- Firearm Evidence and The Role of ER and Forensic NurseDocument3 pagesFirearm Evidence and The Role of ER and Forensic NursejeffreyianNo ratings yet
- NUR9999 M7 Theoretical Approaches.v5Document2 pagesNUR9999 M7 Theoretical Approaches.v5jeffreyianNo ratings yet
- (Ebook) Polynesian MythologyDocument118 pages(Ebook) Polynesian MythologyFreezy FrizzleNo ratings yet
- Attendance Monitoring SystemDocument2 pagesAttendance Monitoring Systemjeffreyian100% (2)
- Jeff Calling CardDocument1 pageJeff Calling CardjeffreyianNo ratings yet
- Ciip Sample LetterDocument1 pageCiip Sample LetterjeffreyianNo ratings yet
- Health PromoDocument33 pagesHealth PromojeffreyianNo ratings yet
- Jeff Calling CardDocument1 pageJeff Calling CardjeffreyianNo ratings yet
- Jeff Calling CardDocument1 pageJeff Calling CardjeffreyianNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- NCGG Irish Festival Grand Marshals 2017Document1 pageNCGG Irish Festival Grand Marshals 2017NewzjunkyNo ratings yet
- Ensayo StreptococoDocument3 pagesEnsayo StreptococoEfraín Carrera FigueroaNo ratings yet
- The Mystery of Metamorphosis - Foreword by Lynn Margulis and Dorion SaganDocument5 pagesThe Mystery of Metamorphosis - Foreword by Lynn Margulis and Dorion SaganChelsea Green Publishing100% (1)
- TorchbearerDocument5 pagesTorchbearerRobert BestNo ratings yet
- The 12 Days of ChristmasDocument2 pagesThe 12 Days of ChristmasCarla Muss-JacobsNo ratings yet
- Passion and Deceit Part VI PDFDocument20 pagesPassion and Deceit Part VI PDFno2meNo ratings yet
- The Nail and Its StructureDocument22 pagesThe Nail and Its StructureHarlene OzarNo ratings yet
- Explorers 4 Unit 6 Under The Sea 2Document3 pagesExplorers 4 Unit 6 Under The Sea 2Gregorio CuadradoNo ratings yet
- 1 Applications: Matching/mating Yusen SungDocument4 pages1 Applications: Matching/mating Yusen Sung1030966ckjanananwnnNo ratings yet
- TASK SHEET No. 1.2-1 Title: Perform Different Knots Used in Restraining Animals Performance ObjectiveDocument7 pagesTASK SHEET No. 1.2-1 Title: Perform Different Knots Used in Restraining Animals Performance ObjectiveRoh NaldzNo ratings yet
- Latihan Soal Bahasa Inggris Sma Kelas X Semester 2Document14 pagesLatihan Soal Bahasa Inggris Sma Kelas X Semester 2tyasajeng100% (2)
- Reinforcement and Extension 2Document12 pagesReinforcement and Extension 2Patri Pardellas BlunierNo ratings yet
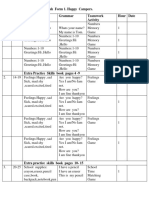
- English Form 1. Happy Campers. Unit Pages Vocabulary Grammar Teamwork Activity Hour DateDocument4 pagesEnglish Form 1. Happy Campers. Unit Pages Vocabulary Grammar Teamwork Activity Hour Dateİlkanə CabbarovaNo ratings yet
- CLS Aipmt-19-20 XI Zoo Study-Package-1 Level-1 Chapter-1 PDFDocument20 pagesCLS Aipmt-19-20 XI Zoo Study-Package-1 Level-1 Chapter-1 PDFJainil PatelNo ratings yet
- Sarnat Scoring Tool: Normal/Mild Moderate HIE Severe HIEDocument1 pageSarnat Scoring Tool: Normal/Mild Moderate HIE Severe HIEBilly WijayaNo ratings yet
- Federación Cinoglosa BelgaDocument2 pagesFederación Cinoglosa Belgalucasl2ossiNo ratings yet
- The Five Human SensesDocument17 pagesThe Five Human SensesAntonio Gonzalez100% (1)
- Hymns of OrpheusDocument71 pagesHymns of OrpheusJustice DubhghaillNo ratings yet
- Wild Life PDFDocument27 pagesWild Life PDFSaagar SenniNo ratings yet
- Sentence Corrections PracticeDocument112 pagesSentence Corrections Practicebook_reader_regularNo ratings yet
- FMA2 - Endless ArmiesDocument38 pagesFMA2 - Endless ArmiesMike100% (1)
- Psychology of ThinkingDocument19 pagesPsychology of ThinkingDiyana HalimNo ratings yet
- Harcourt GK Phonics Practice Book StudentDocument144 pagesHarcourt GK Phonics Practice Book StudentІрина КрупаNo ratings yet
- Animation Changelog 12.25.2022Document3 pagesAnimation Changelog 12.25.2022Miguel CortesNo ratings yet
- Principles of Selection and Mating SystemsDocument29 pagesPrinciples of Selection and Mating SystemsUnknown StudentNo ratings yet
- To Be/ Have Got Test (A1)Document2 pagesTo Be/ Have Got Test (A1)Velislava IvanovaNo ratings yet
- Gameshark Pokemon GbaDocument76 pagesGameshark Pokemon Gbanine starNo ratings yet
- TaxonomiDocument22 pagesTaxonomiDiaz Busthomi FaiziNo ratings yet
- Pulpal Reactions To Caries and Dental ProceduresDocument58 pagesPulpal Reactions To Caries and Dental ProceduresSony RajbhandariNo ratings yet
- Annotatedbib2 DebockDocument2 pagesAnnotatedbib2 Debockapi-282281003No ratings yet