You might also like
- Edu3460 Lesson PlanDocument6 pagesEdu3460 Lesson Planapi-250084180No ratings yet
- Set A: Nursing Practice 3CDocument9 pagesSet A: Nursing Practice 3CMar BleNo ratings yet
- Learning To Tickle: How To Transmit Knowledge As If Re-Telling A JokeDocument12 pagesLearning To Tickle: How To Transmit Knowledge As If Re-Telling A JokejananiwimukthiNo ratings yet
- Social Theory - A Basic Tool Kit - SummaryDocument33 pagesSocial Theory - A Basic Tool Kit - SummaryPaulo BentoNo ratings yet
- Ebp PaperDocument7 pagesEbp Paperapi-238680155No ratings yet
- Impression ManagementDocument96 pagesImpression ManagementAulia Suminar AyuNo ratings yet
- Ethical Use of AssessmentDocument8 pagesEthical Use of AssessmentBrian SrotaNo ratings yet
- MI6 Plenum2 Dejours EnglishDocument6 pagesMI6 Plenum2 Dejours EnglishEmilio FacasNo ratings yet
- Psikopatologi: Tugas Makalah Perbaikan UjianDocument40 pagesPsikopatologi: Tugas Makalah Perbaikan UjiancrossdressNo ratings yet
- Muestra Del Formato de Tesis Actualizada Con InformacionDocument28 pagesMuestra Del Formato de Tesis Actualizada Con InformacionJuan Carlos López PardoNo ratings yet
- Éric Laurent: Guiding Principles For Any Psychoanalytic ActDocument3 pagesÉric Laurent: Guiding Principles For Any Psychoanalytic ActLuiz Felipe MonteiroNo ratings yet
- Glasser'S Reality TherapyDocument5 pagesGlasser'S Reality Therapyana9311No ratings yet
- Practical EthicsDocument7 pagesPractical EthicsSaiteja ChintaNo ratings yet
- Psych Practice 5 1 6Document3 pagesPsych Practice 5 1 6api-240005267No ratings yet
- Esping Andersen Social FoundationsDocument15 pagesEsping Andersen Social FoundationsMadalina GabrielaNo ratings yet
- Psi Homo Tric It AteDocument66 pagesPsi Homo Tric It AteTanasescu Bogdan-emilNo ratings yet
- Qualifications of Er NurseDocument3 pagesQualifications of Er NurseMC CudalNo ratings yet
- Introducere in Manag EdDocument266 pagesIntroducere in Manag Edmocutam97No ratings yet
- Meps CHD Project Executive NotesDocument7 pagesMeps CHD Project Executive Notesapi-261666555No ratings yet
- Portelles - Uplan Full v1 Portfolio EditionDocument42 pagesPortelles - Uplan Full v1 Portfolio Editionapi-242672944No ratings yet
- Informatics and SocietyDocument6 pagesInformatics and SocietyaadiljohnNo ratings yet
- Balancing Act Clinical Practices That Respond ToDocument50 pagesBalancing Act Clinical Practices That Respond ToJoão SuzartNo ratings yet
- KineticDocument8 pagesKineticOchee De Guzman CorpusNo ratings yet
- The Lens Model: A S e S eDocument6 pagesThe Lens Model: A S e S eRana Sharjeel AhmedNo ratings yet
- Micropolitics and The LeftDocument16 pagesMicropolitics and The LeftAragorn Eloff100% (1)
- Csunfa 1Document16 pagesCsunfa 1api-239581752No ratings yet
- Compression Fracture PathoDocument13 pagesCompression Fracture PathoMarrahCarrollNo ratings yet
- Rachel Knee Isearch FinalDocument8 pagesRachel Knee Isearch Finalapi-241767153No ratings yet
- American GovernmentDocument23 pagesAmerican GovernmentrealsilverleNo ratings yet
- Blood Bag Manufacturing FinalDocument39 pagesBlood Bag Manufacturing FinalAbhishek Behl100% (1)
- Article 2Document10 pagesArticle 2api-260371701No ratings yet
- Thaler 2016Document22 pagesThaler 2016Roberto PaezNo ratings yet
- Projeto Vivendo Valores - ArleteDocument16 pagesProjeto Vivendo Valores - ArleteArlete AmaralNo ratings yet
- Cell Biology and Disease Ubd Lesson PlanDocument9 pagesCell Biology and Disease Ubd Lesson Planapi-257779671No ratings yet
- Attitudes and Attitude TheoriesDocument28 pagesAttitudes and Attitude TheoriesRakesh Mohan SaxenaNo ratings yet
- Personal Nursing PhilosophyDocument8 pagesPersonal Nursing PhilosophyNicole Rowland100% (1)
- Main Eda 721 (HRM in Education)Document131 pagesMain Eda 721 (HRM in Education)mdjefryNo ratings yet
- Bab IiDocument17 pagesBab IiDebi JasmarNo ratings yet
- Are You A Weather VaneDocument3 pagesAre You A Weather Vanerksingh00722No ratings yet
- OME Reflections ON THE EGODocument18 pagesOME Reflections ON THE EGOFer RubioNo ratings yet
- Aruna Zizek 4Document22 pagesAruna Zizek 4gaweshajeewaniNo ratings yet
- Clinical Science SessionDocument9 pagesClinical Science SessionEdwin DarmawanNo ratings yet
- Research PaperDocument9 pagesResearch Paperapi-244831834No ratings yet
- E Ed Exam NotesDocument17 pagesE Ed Exam Noteskataruka123No ratings yet
- 02 BaumgartenDocument14 pages02 BaumgartenParaschivoiu BogdanNo ratings yet
- Our Great EpochDocument147 pagesOur Great EpochAaronTalleyNo ratings yet
- ESP Experiments With LSD 25 and PsilocybinDocument5 pagesESP Experiments With LSD 25 and PsilocybinLupita ReyesNo ratings yet
- Addressing Personality StructureDocument9 pagesAddressing Personality StructureKewkew AzilearNo ratings yet
- 25 3 CompleteDocument178 pages25 3 CompleteLiza MohamadNo ratings yet
- Animal Tissues and Organs: Chapter OutlineDocument5 pagesAnimal Tissues and Organs: Chapter OutlineAmirah SyahirahNo ratings yet
- Alabang Development Corp V ValenzuelaDocument14 pagesAlabang Development Corp V ValenzuelakizztarNo ratings yet
- Aristotle - RhetoricDocument100 pagesAristotle - RhetoricJogesh SinghNo ratings yet
- 1 Util Good: Philosophy, June, P. 328)Document7 pages1 Util Good: Philosophy, June, P. 328)Elias GarciaNo ratings yet
- Major in Finance: Letter of SubmissionDocument33 pagesMajor in Finance: Letter of SubmissionprospereducationNo ratings yet
- Personality Theories: An Introduction: Dr. C. George BoereeDocument4 pagesPersonality Theories: An Introduction: Dr. C. George BoereeBenitez GheroldNo ratings yet
- DR Faustus EssayDocument6 pagesDR Faustus EssayAnjan SomeNo ratings yet
- All About PhobiasDocument5 pagesAll About PhobiasRichard SteelNo ratings yet
- Multiobjective Optimization in Water Resources Systems: The surrogate worth trade-off methodFrom EverandMultiobjective Optimization in Water Resources Systems: The surrogate worth trade-off methodNo ratings yet
- Restraints in Dementia Care: A Nurse’s Guide to Minimizing Their UseFrom EverandRestraints in Dementia Care: A Nurse’s Guide to Minimizing Their UseNo ratings yet
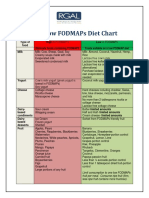
- Fodmap Diet ChartDocument3 pagesFodmap Diet Chartelisadone7001100% (4)
- Family Therapy - TimelineDocument2 pagesFamily Therapy - Timelineelisadone7001No ratings yet
- History - TimelineDocument2 pagesHistory - Timelineelisadone7001No ratings yet
- TIMEline 4Document2 pagesTIMEline 4elisadone7001No ratings yet
- Family Therapy Phase III 1963 To 1985 Family Therapy Incorporates Other ApproachesDocument2 pagesFamily Therapy Phase III 1963 To 1985 Family Therapy Incorporates Other Approacheselisadone7001No ratings yet
- TIMEline 2Document1 pageTIMEline 2elisadone7001No ratings yet
- TIMEline 1Document1 pageTIMEline 1elisadone7001No ratings yet
- Temperature ReadingDocument2 pagesTemperature Readingelisadone7001No ratings yet
- Change ModelDocument2 pagesChange Modelelisadone7001No ratings yet
- Communication StancesDocument5 pagesCommunication Stanceselisadone7001No ratings yet
- Od PDFDocument26 pagesOd PDFsomimemonNo ratings yet
- Family Therapy Chapter 7Document14 pagesFamily Therapy Chapter 7elisadone7001No ratings yet
- German Language CourseDocument210 pagesGerman Language Course42099% (71)
- Tibial Plateau FracturesDocument22 pagesTibial Plateau FracturesvadimmadanNo ratings yet
- Amistoso - DMDDDocument25 pagesAmistoso - DMDDAndréAmistosoNo ratings yet
- Effect of Anxiety To The Academic PerformanceDocument23 pagesEffect of Anxiety To The Academic PerformanceIvan Mhel Salamat100% (6)
- New Year's Resolution Why Do We FailDocument4 pagesNew Year's Resolution Why Do We FailVivitsa UpastiNo ratings yet
- AnaesthesiologyDocument6 pagesAnaesthesiologyCodillia CheongNo ratings yet
- HIPEC ProtocolDocument7 pagesHIPEC ProtocolMariaNo ratings yet
- Meditation ProjectDocument2 pagesMeditation Projectapi-411448305No ratings yet
- Pulmonary Atresia With Ventricular Septal Defect: Systematic ReviewDocument10 pagesPulmonary Atresia With Ventricular Septal Defect: Systematic ReviewIvan VeriswanNo ratings yet
- Gender Affirmation Surgery For The Treatment of Gender DysphoriaDocument4 pagesGender Affirmation Surgery For The Treatment of Gender DysphoriaJess Aloe100% (1)
- DKS CatalogueDocument17 pagesDKS CatalogueHorea Mihai OargaNo ratings yet
- For E-PortfolioDocument14 pagesFor E-Portfolioapi-174496267No ratings yet
- Appendicitis Case StudyDocument13 pagesAppendicitis Case StudyMelanie Agaran Bautista100% (1)
- Pain Assessment and Management in Cancer Patients: Saint Louis University School of NursingDocument3 pagesPain Assessment and Management in Cancer Patients: Saint Louis University School of NursingSoniaMarieBalanayNo ratings yet
- Brief Intro To CBTDocument12 pagesBrief Intro To CBTfrogway100% (4)
- Remotivation TherapyDocument2 pagesRemotivation TherapyMelissa David100% (1)
- DyslexiaDocument7 pagesDyslexiaZumairi TaminNo ratings yet
- Intravenous PyelogramDocument23 pagesIntravenous Pyelogramrachael100% (1)
- ElectrocutionDocument4 pagesElectrocutionVijayakanth VijayakumarNo ratings yet
- Models of AbnormalityDocument18 pagesModels of AbnormalityMark ColesNo ratings yet
- Endo FinalDocument52 pagesEndo Finalspamboy6464No ratings yet
- ParacetamolDocument24 pagesParacetamolFriné MirandaNo ratings yet
- Periodontics & Restorative: MaintenanceDocument10 pagesPeriodontics & Restorative: Maintenancechakri1089No ratings yet
- Calc Drip Rates 2Document2 pagesCalc Drip Rates 2Charisse Nicole DiazNo ratings yet
- PN Study Guide Dosage Proficiency ExamDocument40 pagesPN Study Guide Dosage Proficiency ExamHeather SmithNo ratings yet
- Acute Exacerbation of COPD Nursing Application of Evidence-Based GuidelinesDocument17 pagesAcute Exacerbation of COPD Nursing Application of Evidence-Based GuidelinesCandice ChengNo ratings yet
- An Analysis of Gestalt Group Psychotherapy in The Context of MulticulturalismDocument4 pagesAn Analysis of Gestalt Group Psychotherapy in The Context of MulticulturalismLena KongNo ratings yet
- Minnesota Multiphasic Personality Inventory TestDocument26 pagesMinnesota Multiphasic Personality Inventory TestGicu BelicuNo ratings yet
- Endotracheal Intubation & ER Board Exam QuestionsDocument33 pagesEndotracheal Intubation & ER Board Exam QuestionsJo-Anne Karen Serdeña0% (1)
- Cure Headache NaturallyDocument4 pagesCure Headache NaturallySN WijesinheNo ratings yet
- Phase III Clinical Trials - 2014-15Document23 pagesPhase III Clinical Trials - 2014-15Ali TasleemNo ratings yet