You might also like
- Factors Uncontrolled BPDocument8 pagesFactors Uncontrolled BPErvina Meraih BintangNo ratings yet
- Pathway GGKDocument1 pagePathway GGKDwi Setyo PurnomoNo ratings yet
- Factors Uncontrolled BPDocument8 pagesFactors Uncontrolled BPErvina Meraih BintangNo ratings yet
- Illness Perception and AdherenceDocument11 pagesIllness Perception and AdherenceErvina Meraih BintangNo ratings yet
- Lamp IranDocument1 pageLamp IranErvina Meraih BintangNo ratings yet
- Factor Affecting Medicine AdherenceDocument9 pagesFactor Affecting Medicine AdherenceErvina Meraih BintangNo ratings yet
- Media Medika Indonesiana: Pengaruh Pemberian Jus Jambu Biji (Psidium Guajava L) Terhadap Volume Kaki Dan Kadar Ion NitritDocument9 pagesMedia Medika Indonesiana: Pengaruh Pemberian Jus Jambu Biji (Psidium Guajava L) Terhadap Volume Kaki Dan Kadar Ion NitritErvina Meraih BintangNo ratings yet
- ErvinaDocument10 pagesErvinaErvina Meraih BintangNo ratings yet
- Exercise Is The Activity To Keep Our HealthDocument2 pagesExercise Is The Activity To Keep Our HealthErvina Meraih BintangNo ratings yet
- Etret Aplikasi PDFDocument6 pagesEtret Aplikasi PDFErvina Meraih BintangNo ratings yet
- Etret Aplikasi PDFDocument6 pagesEtret Aplikasi PDFErvina Meraih BintangNo ratings yet
- Ganda DescriptipDocument13 pagesGanda DescriptipErvina Meraih BintangNo ratings yet
- ErvinaDocument10 pagesErvinaErvina Meraih BintangNo ratings yet
- Id Dragon NestDocument1 pageId Dragon NestErvina Meraih BintangNo ratings yet
- Ganda DescriptipDocument13 pagesGanda DescriptipErvina Meraih BintangNo ratings yet
- Ganda DescriptipDocument13 pagesGanda DescriptipErvina Meraih BintangNo ratings yet
- TwentygggggggggggggggggggggggggDocument1 pageTwentygggggggggggggggggggggggggErvina Meraih BintangNo ratings yet
- The Bear and RabbitDocument2 pagesThe Bear and RabbitErvina Meraih BintangNo ratings yet
- Ganda DescriptipDocument13 pagesGanda DescriptipErvina Meraih BintangNo ratings yet
- TwentygggggggggggggggggggggggggDocument1 pageTwentygggggggggggggggggggggggggErvina Meraih BintangNo ratings yet
- The Bear and RabbitDocument2 pagesThe Bear and RabbitErvina Meraih BintangNo ratings yet
- Ganda DescriptipDocument13 pagesGanda DescriptipErvina Meraih BintangNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (120)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Asthma - FactsDocument24 pagesAsthma - Factsvsvp100No ratings yet
- DsDocument4 pagesDseloisa rabanesNo ratings yet
- Quarter: 4 / Semester: 2 / WEEK: 4: Online Resource/sDocument17 pagesQuarter: 4 / Semester: 2 / WEEK: 4: Online Resource/sTristan Paul PagalananNo ratings yet
- Nle - High-Risk PregnancyDocument113 pagesNle - High-Risk Pregnancytachycardia01No ratings yet
- Surgical TermsDocument10 pagesSurgical TermsCLaui SagibalNo ratings yet
- Pathophysiology of Native Coronary, Vein Graft, and In-Stent Atherosclerosis PDFDocument20 pagesPathophysiology of Native Coronary, Vein Graft, and In-Stent Atherosclerosis PDFJorge Arturo Bustos MartinezNo ratings yet
- Heart FailureDocument21 pagesHeart FailureJazzy Kathlene Dumable0% (1)
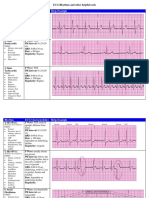
- Rhythm ECG Characteristics Strip Example: ECG Rhythms and Other Helpful ToolsDocument6 pagesRhythm ECG Characteristics Strip Example: ECG Rhythms and Other Helpful ToolsJohnildy MatiasNo ratings yet
- A Case Study On UtiDocument10 pagesA Case Study On UtiMark Tristan AsuncionNo ratings yet
- RCAT WindowDocument2 pagesRCAT WindowEric Jake LimNo ratings yet
- General PathomorpholoDocument127 pagesGeneral Pathomorpholokapil pancholiNo ratings yet
- 2021 MyelopathiesDocument271 pages2021 MyelopathiesNatasha MarksNo ratings yet
- Arterial Thrombosis by AbrarDocument20 pagesArterial Thrombosis by AbrarZain HadiNo ratings yet
- Questions PharmcologyDocument17 pagesQuestions Pharmcologylalitrajindolia100% (2)
- File 146 - Stupid-UsmleDocument14 pagesFile 146 - Stupid-UsmlePrarthana100% (4)
- Heart Disease Prediction Using Machine LearningDocument7 pagesHeart Disease Prediction Using Machine LearningIJRASETPublicationsNo ratings yet
- Velocity Hospital Health Checkup PlansDocument11 pagesVelocity Hospital Health Checkup Plansdipesh2509No ratings yet
- Buerger Disease 1Document27 pagesBuerger Disease 1nadiaNo ratings yet
- All Small Letters For Brand Name, First Letter Is Capitalized Bold Dosage Frequency RouteDocument15 pagesAll Small Letters For Brand Name, First Letter Is Capitalized Bold Dosage Frequency RouteNiña Jean Tormis AldabaNo ratings yet
- Artikel Nama Medis DhionDocument2 pagesArtikel Nama Medis DhionDhion HernandoNo ratings yet
- 2006 Lange OutlineDocument570 pages2006 Lange Outlinemequanint kefieNo ratings yet
- Early Detection of Hepato-Biliary DisorderDocument68 pagesEarly Detection of Hepato-Biliary DisorderIbsa GetachoNo ratings yet
- The Ischemic ElectrocardiogramDocument16 pagesThe Ischemic ElectrocardiogramAdiel OjedaNo ratings yet
- Ha&P - Semi ReviewerDocument71 pagesHa&P - Semi ReviewerLittle StuartNo ratings yet
- MODULE 23 BLOOD and URINEDocument31 pagesMODULE 23 BLOOD and URINECrystal ManguneNo ratings yet
- Oxygen TherapyDocument42 pagesOxygen TherapyZayar SweNo ratings yet
- DR Anu Sachdeva Rational Use of Oxygen in NeonatesDocument11 pagesDR Anu Sachdeva Rational Use of Oxygen in NeonatesBhoomika PandeyNo ratings yet
- Syllab bscct1819-24102018Document65 pagesSyllab bscct1819-24102018vasanthNo ratings yet
- Fluid Volume Deficit (Dehydration) Nursing Care Plan - NurseslabsDocument17 pagesFluid Volume Deficit (Dehydration) Nursing Care Plan - NurseslabsA.No ratings yet