You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- Raza's ECGDocument45 pagesRaza's ECGcozmoxxxNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- From: Rapid Interpretation of EKG'sDocument14 pagesFrom: Rapid Interpretation of EKG'sLucija Kljaić100% (1)
- ECG InterpretationDocument52 pagesECG InterpretationMarcus, RN98% (44)
- Assessing Potential Divers Congenital Heart DiseaseDocument5 pagesAssessing Potential Divers Congenital Heart Diseasetonylee24No ratings yet
- Mini Test QUIZDocument9 pagesMini Test QUIZAbdul RohimNo ratings yet
- Dobutamine - IV AdministrationDocument4 pagesDobutamine - IV AdministrationArcee Rentillo100% (1)
- Dominga A. Salmone vs. Employees' Compensation Commission and Social Security SystemDocument3 pagesDominga A. Salmone vs. Employees' Compensation Commission and Social Security SystemmarielNo ratings yet
- Managing Palpitations and Arrhythmias During Pregnancy: Dawn L Adamson, Catherine Nelson-PiercyDocument7 pagesManaging Palpitations and Arrhythmias During Pregnancy: Dawn L Adamson, Catherine Nelson-PiercyFlo ArdyansyahNo ratings yet
- Acute Bioligic CrisisDocument141 pagesAcute Bioligic CrisisJanelle MatamorosaNo ratings yet
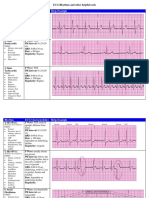
- Rhythm ECG Characteristics Strip Example: ECG Rhythms and Other Helpful ToolsDocument6 pagesRhythm ECG Characteristics Strip Example: ECG Rhythms and Other Helpful ToolsJohnildy MatiasNo ratings yet
- Brugada SyndromeDocument12 pagesBrugada SyndromeIslam KhedrNo ratings yet
- AH2 Hesi ReviewDocument46 pagesAH2 Hesi ReviewJamie Antonini Grant100% (1)
- Systematic Approach To ECGDocument12 pagesSystematic Approach To ECGAmr El TaherNo ratings yet
- Complication of MI (Myocardial Infarction)Document2 pagesComplication of MI (Myocardial Infarction)Zahid QamarNo ratings yet
- Drug Study (GBS)Document16 pagesDrug Study (GBS)Mary Rose Verzosa LuisNo ratings yet
- Guidelines Aca HolterDocument39 pagesGuidelines Aca HolterMiguel PeixotoNo ratings yet
- Learn ECG in A DayDocument99 pagesLearn ECG in A DayKamogelo MabotjaNo ratings yet
- ARRHYTHMIADocument25 pagesARRHYTHMIAAsma MuhammadiNo ratings yet
- Datex S5 - User ManualDocument142 pagesDatex S5 - User ManualAndrea Nathaly Medina SanchezNo ratings yet
- Cardiomyopathy 1223958636063843 9Document87 pagesCardiomyopathy 1223958636063843 9Dainy ThomasNo ratings yet
- Pediatric Dilated CardiomyopathyDocument10 pagesPediatric Dilated CardiomyopathyRiduan Adoro Lumban GaolNo ratings yet
- Atrial Fibrillation HandoutDocument5 pagesAtrial Fibrillation HandoutAlfa AlfinNo ratings yet
- Historia EKGDocument19 pagesHistoria EKGibigrachuNo ratings yet
- Skill Lab #7: Abnormal ECG Interpretation and Treatment: Aed/DDocument10 pagesSkill Lab #7: Abnormal ECG Interpretation and Treatment: Aed/Dاكرم صالحينNo ratings yet
- Cardiac MonitoringDocument5 pagesCardiac MonitoringAmit Kl100% (1)
- Thyroid StormDocument16 pagesThyroid StormRaquid MariaNo ratings yet
- Management of Perioperative ArrhythmiasDocument15 pagesManagement of Perioperative Arrhythmiaszuraini_mdnoorNo ratings yet
- Nclex Cardio QuestionsDocument4 pagesNclex Cardio QuestionsMichelleNo ratings yet
- ACLS DrugsDocument16 pagesACLS Drugstostc100% (2)
- EKG Quick and Dirty - GD v3.0Document2 pagesEKG Quick and Dirty - GD v3.0Sheema Sh100% (1)