Professional Documents
Culture Documents
Mecanismos Moleculares de Resistencia Bacteriana
Uploaded by
Eduardo P. BarajasOriginal Description:
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Mecanismos Moleculares de Resistencia Bacteriana
Uploaded by
Eduardo P. BarajasCopyright:
Available Formats
19
Molecular Mechanisms of Antibiotic Resistance in Bacteria
STEVEN M. OPAL | AURORA POP-VICAS
Molecular Genetics of Antibiotic Resistance
Genetic variability is essential for microbial evolution to occur. The tness of a microorganism depends on its capacity to adapt to changing environmental conditions.1 Antimicrobial agents exert strong selective pressures on bacterial populations, favoring organisms that are capable of resisting them.1,2 Genetic variability occurs through a variety of mechanisms. Point mutations may occur in a nucleotide base pair, and this is referred to as microevolutionary change. These mutations may alter enzyme substrate specicity or the target site of an antimicrobial agent, interfering with its activity. Point mutations at crucial locations on old -lactamase genes (e.g., genes for TEM-1, SHV-1) are primarily responsible for the remarkable array of newly recognized extended-spectrum -lactamases (ESBL).3,4 A second level of genomic variability in bacteria is referred to as macroevolutionary change and results in wholesale rearrangements of large segments of DNA as a single event. These rearrangements may include inversions, duplications, insertions, deletions, or transpositions of large sequences of DNA from one location of a bacterial chromosome or plasmid to another. These large-scale rearrangements of entire segments of the bacterial genome are frequently generated by specialized genetic elements called integrons, transposons, or insertion sequences, which have the capacity to insert, rearrange, and move independently from the rest of the bacterial genome.2 A third level of genetic variability in bacteria is created by the acquisition of foreign DNA carried by plasmids, bacteriophages, naked sequences of DNA, or transposable genetic elements from other bacteria (i.e., vertical transmission). Inheritance of foreign DNA further contributes to an organisms genetic variability and its capacity to respond to selection pressures imposed by antimicrobial agents.3 These mechanisms endow bacteria with the seemingly unlimited capacity to develop resistance to any antimicrobial agent (Fig. 19-1). Examples of plasmid-mediated carbapenemase-producing Klebsiella pneumoniae,5 vancomycin-resistant and daptomycin-resistant Staphylococcus aureus,6,7 multidrug-resistant (MDR) Yersinia pestis,8 and transferable quinolone resistance in enterobacteria9 attest to the capacity of microorganisms to adapt to environmental stresses such as antibiotic exposure. Once an antibiotic-resistance gene evolves, it can spread between bacteria by transformation, transduction, conjugation, or transposition. Favored clones of bacteria may proliferate in the microbial ora of patients who receive antibiotics. Evidence exists that antibiotic-resistance genes were present in the era before antibiotic therapy was available, and they probably originated from antibiotic-producing bacteria.3,10 Environmental levels of multiple classes of antimicrobial agents are now so common in soil and water samples that multiple bacterial genera have strains that subsist entirely on antibiotics as their sole carbon source.11 These bacteria express remarkably high levels of resistance to a wide array of antibiotic classes. Aquatic environments are particularly rich in bacterial populations replete with antibiotic resistance genes.12 Such environmental bacterial strains likely provide potential human pathogens with a source of novel antibiotic-resistance genes.11,12 Selection pressures placed on microbial populations by antibiotics favor the expansion of strains that have the capacity to resist the inhibitory effects of
antibiotics. These resistant populations proliferate and spread antibiotic-resistance genes vertically to subsequent generations and horizontally to susceptible strains of related bacteria, even to different species or different genera.13 Although some antibiotic-resistance genes place a metabolic burden on bacteria, many microorganisms have evolved strategies to limit this cost by repressing gene expression when it is not needed, by production of alternative gene products, or by phase variation. These adaptations allow favorable but sometimes costly antibiotic resistance to be held in reserve in the absence of antibiotic selection pressure, yet express their resistance potential on re-exposure to antibiotics.14 PLASMIDS Extrachromosomal elements were present in bacteria before the introduction of antibiotics into clinical medicine in the 20th century.10,13 Antibiotic therapy created selection pressures that favored the dissemination of resistance genes via mobile genetic elements.2,3,13 Plasmids are particularly well adapted to serve as agents of genetic exchange and resistance-gene dissemination.1,3 Plasmids are autonomously replicating genetic elements that are made of covalently closed, circular, double-stranded DNA molecules ranging from less than 10 to more than 400 kilobase pairs. They are extremely common in bacteria.13 Although multiple copies of a specic plasmid or multiple different plasmids (or both) may be found in a single bacterial cell, closely related plasmids often cannot coexist in the same cell. This observation has led to a classication scheme of plasmids based on incompatibility (Inc) groups.1,4 Plasmids may determine a wide range of functions besides antibiotic resistance, including virulence and metabolic capacities. All plasmids possess an origin for replication of DNA polymerase to bind and replicate plasmid DNA. Plasmids must also retain a set of genes that facilitate their stable maintenance in host bacteria. The transfer of plasmid DNA between bacterial species is a complex process, and the genes needed for transfer (tra genes) make conjugative plasmids larger than nonconjugative ones. Some small plasmids may be able to transfer to other bacteria by using the conjugation apparatus provided by coresident conjugative plasmids or even conjugative transposons. Many plasmid-encoded functions enable bacterial strains to persist in the environment by resisting noxious agents, such as heavy metals. Mercury released from dental llings may increase the number of antibiotic-resistant bacteria in the mouth.15 Compounds such as hexachlorophene are used as topical bacteriostatic agents, and plasmidmediated resistance to these agents has increased signicantly.16 TRANSPOSABLE GENETIC ELEMENTS Transposons can translocate as a unit from one area of the bacterial chromosome to another or between the chromosome and plasmid or bacteriophage DNA. Transposable genetic elements possess a specialized system of recombination which is independent of the generalized recombination system that classically permits recombination of largely homologous sequences of DNA through crossover events (the recA system of bacteria). The recA-independent recombination system (transposase) of transposable elements usually occurs in a random
279
280
PART I Basic Principles in the Diagnosis and Management of Infectious Diseases
Donor Tet M Transposon Conjugative plasmid Process Transformation
xx
Nonconjugative plasmid Bla PBP' Chromosome
Recipient
PBP' PBP'
PBP'
A
Transduction Phage Bla Bla
fashion between nonhomologous sequences of DNA and results in wholesale modications of large sequences of DNA as a single event (Fig. 19-2).2,5 The two types of transposable genetic elements, transposons (Tn) and insertion sequences (IS), have similar characteristics. Evidence from whole-genome sequencing projects indicates that bacterial chromosomes are replete with transposable elements.17 These mobile sequences probably play an important physiologic role in genetic variation and evolution in prokaryotic organisms. Transposons differ from insertion sequences in that they encode functional genes that mediate a recognizable phenotypic characteristic, such as an antibiotic-resistance marker. Either element can translocate as an independent unit. Both elements are anked on each end by short identical sequences of DNA in reverse order (inverted repeats). These inverted-repeat DNA termini are essential to the transposition process. Transposons and insertion sequences are incapable of autonomous self-replication and must exist on a replicon, such as the chromosome, a bacteriophage, or a plasmid, to be replicated and maintained in a bacterial population. Some transposons have the capability to move from one bacterium to another
Conjugation Mating bridge
Tet M
Tet Mtransfer
Mobilized Bla
Conjugative transposition Tet M
D
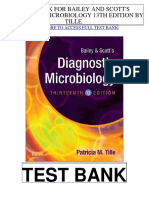
Figure 19-1 Examples of recombination events and molecular spread of antibiotic-resistance genes. The donor organism depicted here has three antibiotic-resistance genes: the rst (a low-afnity penicillin-binding protein, designated PBP) is located on the chromosome; the second (a -lactamase gene labeled Bla) on a small nonconjugative plasmid; and the third (Tet M, a tetracycline resistance determinant) on a transposon residing on a large self-conjugative plasmid. A, Genetic exchange may occur by transformation (naked DNA transfer from dying bacteria to a competent recipient). This typically results in the transfer of homologous genes located on the chromosome by recombination enzymes (recA). B, Transduction may transfer antibiotic-resistance genes (usually from small plasmids) through imprecise packaging of nucleic acids by transducing bacteriophages. C, Conjugation is an efcient method of gene transfer requiring physical contact between donor and recipient. Self-transferable plasmids mediate direct contact by forming a mating bridge between cells. Smaller nonconjugative plasmids can be mobilized in this mating process and transported into the recipient. D, Transposons are specialized sequences of DNA that possess their own recombination enzymes (transposases), allowing for transposition (hopping) from one location to another independent of the recombination enzymes of the host (recA-independent transposition). They can transpose to nonhomologous sequences of DNA and can spread antibiotic-resistance genes to multiple plasmids or genomic locations throughout the host. Some transposons possess the ability to move directly from a donor to a recipient independent of other gene transfer events (conjugative transposons).
A
TRANSPOSABLE DNA ELEMENT * * Central Flanking Flanking sequences duplicated duplicated recipient DNA Terminal repeat sequences recipient DNA on transposable element (direct or inverted)
Figure 19-2 A, Characteristic appearance of a transposon on electron microscopy, showing the stem-loop conguration. The kanamycinresistance transposon, Tn903, is inserted into a small plasmid (pSC105). After denaturation, intrastrand annealing of the complementary 1000-base-pair, inverted-repeat, terminal sequences of the transposon forms the stem structure. The kanamycin-resistance gene and the genes necessary for transposition are located in the central loop structure. B, Structure of a transposable element inserted into a recipient DNA sequence. The transposon (rectangles and wavy lines) consists of a central sequence containing the phenotypic marker gene or genes (e.g., an antibiotic-resistance gene) and the transposase genes. The terminal-repeat sequences of the transposon ank the central sequences on both sides. Insertion of the transposon results in single-strand, staggered cuts in the recipient DNA (asterisks). Subsequent gap-lling DNA synthesis and ligation results in duplication of a short sequence of recipient DNA at either end of the transposon.
19 Molecular Mechanisms of Antibiotic Resistance in Bacteria
281
without being xed within a plasmid or bacteriophage. These elements are referred to as conjugative transposons. The ubiquitous transposable element Tn916 and its derivatives are examples of conjugative transposons and have been found primarily in aerobic and anaerobic grampositive organisms, although they can also exist in gram-negative bacteria.18,19 Transposition usually results in localized replication of the transposable element from the original donor sequence of DNA and insertion of a copy of the transposable element into the recipient sequence of DNA (replicative transposition).1,2 Transposition, similar to point mutation, is a continuous, ongoing process in bacterial populations. An example of this phenomenon is the spread of a tetracycline-resistance transposon among Neisseria gonorrhoeae, Mycoplasma hominis, and Ureaplasma urealyticum.20,21 Transposons also are essential in the evolution of resistance plasmids that contain multiple antibiotic-resistance determinants.16 The recent spread of carbapenem resistance from metallo--lactamases among the Enterobacteriaceae in some European hospitals was facilitated by transposition of resistance genes on integrons to separate plasmids from different bacterial genera of gram-negative bacilli.22 High-level vancomycin resistance (vanA) in enterococci is mediated by a composite transposon that encodes a series of genes needed to express vancomycin resistance.23 Single transposons may encode multiple antibiotic-resistance determinants within their inverted-repeat termini as well.2 Genetic exchange of antibiotic-resistance genes occurs between bacteria of widely disparate species and different genera.24,25 Identical aminoglycoside-resistance genes occur in streptococci and Campylobacter,25 and enterococci apparently have acquired aminoglycoside26 and -lactam27 resistance from staphylococci. Given the highly variable environmental selection pressures created by antibiotics and the plasticity of bacterial genomes, the ongoing evolution of MDR species seems inevitable.28-30 DNA INTEGRATION ELEMENTS The structural genes that mediate antibiotic resistance often are closely linked and may exist in tandem along the bacterial chromosome or plasmid. Genetic analysis of sequences of DNA adjacent to antibioticresistance genes revealed that unique integration units often exist near promoter sites.31 These integration elements, called integrons,32 function as recombinational hot spots for site-specic recombination events between largely nonhomologous sequences of DNA. Integrons facilitate the lateral transfer and integration of antibiotic-resistance genes from mobile gene cassettes. The integron provides its own unique integrase function,33 which facilitates recA-independent recombination, and a specialized attachment and integration site consisting of a spacer sequence of highly conserved DNA, often of 59 base pairs (range, 57 to 141 base pairs). This 59-base-pair element is preserved at the 3 end of inserted antibiotic-resistance genes.34,35 Although these integration elements differ structurally and functionally from transposons,36 they seem to be widespread in bacterial populations and play an important role in the dissemination of antibiotic-resistance genes.2,21,37,38 Integrons do not transpose independently as a specic unit structure from one sequence of DNA to another. This capability of autonomous movement of large sequences of DNA is reserved primarily for transposons, insertion sequence elements, and, in some cases, bacteriophages. However, integrons may become anked by transposable elements and integrated into an existing transposon. The principal role of integrons is to provide a convenient insertion site for antibiotic-resistance genes from foreign DNA sources. There are ve classes of integrons that encode antibiotic-resistance genes, with class 1 integrons being the most common type in pathogenic microorganisms.38 A schematic representation of a class 1 integron is shown in Figure 19-3. Integrons also serve as expression cassettes for antibiotic-resistance genes in that an efcient promoter site is provided in close proximity to the 5 end of the newly inserted
5'-CS intl1 5'
IRi
P
Insertion sites for new gene cassettes
1 2
3'-CS qacE1 sul1 orf5 3'
R1
R2
R3
attl1 59 bp elements
IRt
Figure 19-3 Organization of a hypothetical class I integron. The 5 conserved sequence (5-CS) contains a site-specic integrase (intI1); an attachment site (attI1), which functions as a receptor for new gene cassettes; and two potential promoter sites, P1and P2 (white arrows). The promoter is the initiation site for the transcription of the multiple, potential, antibiotic gene cassettes (labeled R1, R2, R3) that are inserted downstream from the promoter. Repeated, variable-length, but usually 59-base-pair elements ank the central antibiotic-resistance gene cassettes. The conserved 3 end of the integron (3-CS) usually consists of a gene for resistance to quaternary ammonium compounds (qucE1), a sulfonamide-resistance gene (sul1), and an open reading frame (orf5). The outer boundaries of the integron structure are anked by a 25base-pair inverted-repeat sequence (labeled IRi and IRt).
DNA sequence. The frequency of transcription of integrated cassettes of antibiotic-resistance genes depends on the proximity of the gene to the promoter at the 5 upstream end of the integron. The level of expression of a resistance gene diminishes as the distance between the promoter and the specic antibiotic-resistance gene cassette increases.33 Numerous clusters of different antibiotic-resistance genes have been identied that have evolved through specic insertions into common integrons.34 Integrons have been found to possess ve antibiotic-resistance genes in sequence from a single integron unit.39 Complex integrons have been described that are typied by a common reading frame (orf 513) linked to the 3 end of a typical integron, which is followed by a series of inserted genes (often expanded spectrum -lactamases) and then a duplication of the 3 end of the integron. This common 3 end of type 1 integrons encode genes for resistance to quaternary ammonium compounds (qacE1), sulfonamide resistance (sul1), and an open reading frame of unknown function (orf5). These complex integrons can be mobilized and spread by adjacent insertion sequences to disseminate among bacterial populations.40
Mechanisms of Antibiotic Resistance
At least eight distinctive mechanisms of antibiotic resistance have been described in bacteria (Table 19-1). Examples of each of these mechanisms are provided in the following paragraphs. ENZYMATIC ALTERATION -Lactamases Resistance to -lactam antibiotics occurs primarily through the production of -lactamases, enzymes that inactivate these antibiotics by splitting the amide bond of the -lactam ring. -Lactamases most likely co-evolved with bacteria as mechanisms of resistance against natural antibiotics over time, and the selective pressure exerted by the widespread use of antimicrobial therapy in modern medicine may have accelerated their development and spread. -Lactamases are encoded either by chromosomal genes or by transferable genes located on plasmids and transposons. In addition, -lactamase genes (bla) frequently reside on integrons, which often carry multiple-resistance determinants. If mobilized by transposable elements, integrons can facilitate further dissemination of multidrug resistance among different bacterial species.41 -Lactamases can be classied according to their amino acid structure into four molecular classes, A through D (Table 19-2), as rst suggested by Ambler.41a Alternatively, the Bush-Jacoby-Medeiros
282
PART I Basic Principles in the Diagnosis and Management of Infectious Diseases
TABLE
19-1
Eight Major Mechanisms of Resistance by Antimicrobial Class
-Lactam Aminoglycoside Chloramphenicol Macrolide Sulfonamide Tetracycline Trimethoprim Quinolone + + (GN) + +++ + Glycopeptide ++ (GN) +++ + ++ Lincosamide, Streptogramin + (GN) +++ Rifampin +++
Mechanism
Enzymatic +++ +++ +++ + (GN) alteration Decreased + (GN) + (GN) + (GN) ++ (GN) + (GN) + (GN) permeability Efux + + + ++ +++ Alteration of ++ ++ +++ ++ + (H. pylori) +++ target site Protection of ++ target site Overproduction ++ ++ of target Bypass of + + inhibited process Bind-up antibiotic +++, most common mechanism; ++, common; +, less common; , absent; GN, gram-negative; H. pylori, Helicobacter pylori.
system classies the enzymes into several functional groups according to their substrate prole and susceptibility to -lactamase inhibitors such as clavulinic acid (Table 19-3).42 Class A, C, and D -lactamases hydrolyze the -lactam ring through a serine residue at their active site, whereas class B enzymes are metallo--lactamases that use zinc (Zn2+) to break the amide bond. Class C enzymes include the -lactamase determined by the chromosomal ampC gene of Escherichia coli K-12, which shares extensive sequence homology with chromosomally mediated -lactamases of Shigella and Klebsiella species. These enzymes are large proteins (molecular weight, approximately 39,000) with mainly cephalosporinase activity. They also have serine at their active site but share little homology with the class A -lactamases. The tertiary structures of class C -lactamases show striking similarities to penicillin-binding proteins (PBPs), from which they may have evolved.3 The rst -lactamase was described as a penicillinase capable of hydrolyzing penicillin in E. coli in 1940, about the same time as the rst clinical use of penicillin was reported in the literature.43 The next years witnessed the rapid spread of plasmid-encoded penicillin resistance among the majority of S. aureus clinical isolates.44,45 Among
TABLE
gram-negative organisms, the rise in ampicillin resistance in the 1960s was ascribed to the emergence of TEM-1, a plasmid-encoded -lactamase named after a Greek patient, Temoniera, in whom the rst isolate was recovered. The family of TEM -lactamases disseminated worldwide through various Enterobacteriaceae, as well as Pseudomonas aeruginosa, Haemophilus inuenzae, and N. gonorrhoeae.46,47 Similarly, both chromosomally encoded and plasmid-mediated SHV-type -lactamases, with a molecular structure related to that of the TEM enzymes, became widely prevalent among E. coli and K. pneumoniae isolates. The pharmaceutical industrys development of thirdgeneration cephalosporins, which initially were stable to the actions of TEM- and SHV-type -lactamases, was soon followed by the emergence and global spread of ESBLs, which are capable of hydrolyzing monobactam and broad-spectrum cephalosporins.3,45-48 In addition, increasing reports of the emergence and spread of carbapenemases have raised concern about the currently limited antimicrobial arsenal against infections with MDR gram-negative bacteria.47 To date, more than 600 -lactamases have been described, and their amino acid sequences can be found on the Jacoby and Bush website (www.lahey .org/studies/webt/htm, accessed February 2009).
19-2
Ambler Classication of -Lactamases Active Site Serine Enzyme Type Penicillinases Broad-spectrum Extended-spectrum (ESBL) Carbapenemases Substrates Benzylpenicillin, aminopenicillins, carboxypenicillins, ureidopenicillins, narrow-spectrum cephalosporins Substrates of broad-spectrum plus oxymino--lactams (cefotaxime, ceftazidime, ceftriaxone) and aztreonam Substrates of extended-spectrum plus cephamycins and carbapenems Substrates of extended-spectrum plus cephamycins and carbapenems Substrates of extended-spectrum plus cephamycins Examples PC1 in Staphylococcus aureus TEM-1, SHV-1 in Escherichia coli, Klebsiella pneumoniae, and other gram-negative bacteria In Enterobacteriaceae: TEM-derived, SHV-derived, CTX-Mderived; PER-1, VEB-1, VEB-2, GES-1, GES-2, IBC-2 in Pseudomonas aeruginosa KPC-1, KPC-2, KPC-3 in K. pneumoniae; NMC/IMI, SME family IMP, VIM, GIM, SPM, SIM lineages in P. aeruginosa, Acinetobacter spp. AmpC-type enzymes in Enterobacteriaceae, Acinetobacter baumannii OXA-family in P. aeruginosa OXA-derived in P. aeruginosa OXA-derived in Acinetobacter spp.
Class A
B C D
Metallo-lactamases (Zn2+) Serine Serine
Carbapenemases Cephalosporinases Oxacillinases Broad-spectrum Extended-spectrum Carbapenemases
Aminopenicillins, ureidopenicillins, cloxacillin, methicillin, oxacillin, and some narrow-spectrum cephalosporins Substrates of broad-spectrum plus oxymino--lactams and monobactam Substrates of extended-spectrum plus cephamycins and carbapenems
Adapted from Jacoby GA, Munoz-Price LS. The new -lactamases. N Engl J Med. 2005;352:380-391.
19 Molecular Mechanisms of Antibiotic Resistance in Bacteria
283
TABLE
19-3
Bush-Jacoby-Medeiros Functional Classication Scheme for -Lactamases Enzyme Type Cephalosporinase Penicillinase Broad-spectrum Extended-spectrum Inhibitor-resistant Carbenicillinase Cloxacillinase Cephalosporinase Carbapenemase Carbapenemase Penicillinase Inhibition by Clavulanate No Yes Yes Yes Diminished Yes Yes Yes Yes No No Molecular Class C A A A A A D or A A A B A Examples Enterobacter cloacae P99 (C), MIR-1 (P) Bacillus cereus, Staphylococcus aureus (B) SHV-1 (B), TEM-1 (P) Klebsiella oxytoca K1 (C), TEM-3 (P), SHV-2 (P) TEM-30 (IRT-2) (P) AER-1 (C), PSE-1 (P), CARB-3 (P) Streptomyces cacaoi (C), OXA-1 (P) Proteus vulgaris (C), FEC-1 (P) IMI-1 (C), NMC-A (C), Sme-1 (C) Stenotrophomonas maltophilia L1 (C), IMP-1 (P) Burkholderia cepacia (C), SAR-2 (P)
Group 1 2a 2b 2be 2br 2c 2d 2e 2f 3 4
B, both chromosomal and plasmid; C, chromosomal; P, plasmid. New group (derived from Bush K, Jacoby GA, Medeiros AA. A functional classication scheme for -lactamases and its correlation with molecular structure. Antimicrob Agents Chemother. 1995;39:1211-1233).
Extended-Spectrum -Lactamases TEM-Derived. TEM-1 is the most common -lactamase in gramnegative bacteria, and it can hydrolyze penicillins and narrowspectrum cephalosporins in Enterobacteriaceae, N. gonorrhoeae, and H. inuenzae.45 The extended-spectrum of activity for TEM-derived ESBLs is obtained through changes in a single or a few amino acids that alter the conguration of the enzyme at its active site, making it more accessible to the bulky R1 oxymino-side chains of third-generation cephalosporins (cefotaxime, cefpodoxime, ceftazidime, ceftriaxone) and monobactam (aztreonam).49 The rst TEM-derived ESBL, TEM-3, was reported in 1988.50 There are now more than 160 TEMderived ESBLs (see the Lahey clinic website described earlier). They are found primarily in E. coli and K. pneumoniae isolates but also in other Enterobacteriaceae such as Enterobacter aerogenes, Morganella morganii, Proteus spp., and Salmonella spp.45 The majority of TEMderived ESBLs remain susceptible to inhibition by clavulinic acid, although inhibitor-resistant TEM variants have also been described.51 SHV-Derived. The SHV-1 (or sulfhydryl variable) -lactamase has a biochemical structure similar to that of TEM-1 (68% of amino acids are shared52), and its ESBL derivatives are also produced by point mutations (one or more amino acid substitutions) at its active site. SHV-type -lactamases are found primarily in K. pneumoniae strains. A three-dimensional image of TEM-type and SHV-type ESBLs is provided in Figure 19-4. CTX-MDerived. CTX-M -lactamases are not evolutionarily related to the SHV and TEM families; they are thought to have been acquired by plasmids from the chromosomal AmpC enzymes of Kluyvera spp., environmental gram-negative rods of low pathogenic potential.53,54 In general, the CTX-M family members hydrolyze cefotaxime and ceftriaxone better than ceftazidime, and they are inhibited more by tazobactam than by clavulinic acid,45,52 although point mutations leading to increased activity against ceftazidime can occur. CTX-M enzymes have disseminated rapidly worldwide and are now among the most prevalent ESBLs in Europe and South America.55 Recent reports of community-acquired bloodstream infections with MDR CTX-M E. coli isolates from Spain and Israel are raising signicant public health concern.56,57 OXA-Derived. OXA-type -lactamases (molecular class D, functional group 2d) hydrolyze oxacillin and its derivatives very effectively and are poorly inhibited by clavulinic acid.42,45 OXA-derived ESBLs have been described mainly in P. aeruginosa, in which they confer high-level resistance to oxymino- lactams.45 AmpC Enzymes. AmpC -lactamases (molecular class C, functional group 1) are primarily chromosomal enzymes that confer resistance to penicillins, narrow-spectrum cephalosporins, oxymino-lactams, and cephamycins; they are not susceptible to -lactamase inhibitors such as clavulinic acid.58 Cefepime and aztreonam are usually poor substrates, although modulation by point mutations at
the R2 loop of the active site have been responsible for variants with increased ability to hydrolyze cefepime. AmpC production in gramnegative bacilli is normally repressed. However, a transient increase in production (10-fold to 100-fold) can occur in the presence of -lactam antibiotics in the following species that possess inducible AmpC enzymes: Enterobacter, Citrobacter freundii, Serratia, M. morganii, Providencia, and P. aeruginosa.59 AmpC -lactamase production returns to low levels after antibiotic exposure is discontinued, unless spontaneous mutations occur in the ampD locus of the gene, leading to permanent hyperproduction (derepression) in these species. Thirdgeneration cephalosporins in Enterobacter infections can therefore select for the overgrowth of these stably derepressed mutants, leading to the emergence of antibiotic resistance during treatment.58,60 More than 20 plasmid-mediated AmpC enzymes, derived from chromosomally encoded genes in Enterobacteriaceae or in Aeromonas species, have been described in E. coli, K. pneumoniae, Salmonella enterica, and Proteus mirabilis. -Lactam resistance attributable to this system appears to be increasing and confers a resistance phenotype similar to that of Enterobacter species.47
TEM
SHV
Ser Ser
Figure 19-4 Ribbon diagrams of TEM -lactamases (A) and SHV -lactamases (B). Alpha-helices are shown in yellow, beta-strands in pink, and turns in gray. The serine (Ser) residue (white arrow) involved in the hydrolysis of the -lactam antibiotic ring is shown in ball-and-stick mode in the active site at the center of each molecule. The surrounding atoms, shown in stick mode, represent various sites of amino acid substitutions (point mutations) that yield an extended-spectrum -lactamase phenotype. (Adapted with permission from Jacoby GA, Munoz-Price SL. The new beta-lactamases. N Engl J Med. 2005;352:380.)
284
PART I Basic Principles in the Diagnosis and Management of Infectious Diseases
Carbapenemases. Carbapenemases confer the largest antibiotic resistance spectrum, because they can hydrolyze not only carbapenems but also broad-spectrum penicillins, oxymino-cephalosporins, and cephamycins. The KPC enzymes are currently the most important class A serine carbapenemases. Since being initially reported from K. pneumoniae isolates in several outbreaks in the northeastern United States,61-64 KPC carbapenemases have been found worldwide in many other gram-negative species, such as E. coli, Citrobacter, Enterobacter, Salmonella, Serratia, and P. aeruginosa.5 Class B metallo--lactamases use a Zn2+ cation for hydrolysis of the -lactam ring, are susceptible to ion chelators such as ethylenediamenetetraacetic acid (EDTA), and are resistant to clavulinic acid, tazobactam, and sulbactam. They confer resistance to all -lactam antibiotics except monobactams. Chromosomally encoded metallo-lactamases are primarily found in environmental isolates of Aeromonas, Chryseobacterium, and Stenotrophomonas species and are usually of low pathogenic potential.65 Most of the clinically important metallo-lactamases belong to ve different families (IMP, VIM, SPM, GIM, and SIM). They are typically transmitted by mobile gene elements inserted into integrons and have spread through P. aeruginosa, Acinetobacter, other gram-negative nonfermenters, and enteric bacterial pathogens.22,66 Finally, class D carbapenemases have been described among four subfamilies of OXA-type -lactamases (OXA-23, OXA-24, OXA-40, OXA-58), primarily in Acinetobacter baumannii. In A. baumannii, the intrinsic weaker carbapenemase activity is augmented through coupling of the -lactamase production with an additional resistance mechanism, such as decreased membrane permeability or increased active efux.67 Anaerobic Bacteria. -Lactamases also contribute to the resistance of anaerobic bacteria to -lactam antibiotics.73,74 The -lactamases of fusobacteria and clostridia are principally penicillinases.75,76 The -lactamases produced by Bacteroides fragilis are predominantly cephalosporinases, some of which have been found to hydrolyze cefoxitin and imipenem and may be transferable.77-79 Most of the cephalosporinases are inhibited by clavulanate, sulbactam, or tazobactam. Some isolates of Bacteroides spp. produce carbapenemases, metalloenzymes inhibited by EDTA but not by clavulanate, that confer resistance to imipenem. Contribution of -Lactamases to -Lactam Antibiotic Resistance. The level of antibiotic resistance mediated by a particular -lactamase in a population of bacteria is determined by at least ve variables. The efciency of the -lactamase in hydrolyzing an antibiotic depends on (1) its rate of hydrolysis and (2) its afnity for the antibiotic; other variables are (3) the amount of -lactamase produced by the bacterial cell, (4) the susceptibility of the target protein (PBP) to the antibiotic, and (5) the rate of diffusion of the antibiotic into the periplasm of the cell. Within the bacterial cell, -lactamases contribute to antibiotic resistance in several ways. The simplest model is that of penicillinaseproducing staphylococci, in which the bacteria, on exposure to penicillin, begin to produce -lactamase, which they excrete extracellularly. Two events then take place concurrently: penicillin lyses bacteria, and -lactamase hydrolyzes penicillin. If viable bacterial cells remain after the level of penicillin has declined to less than the minimal inhibitory concentration (MIC), regrowth of bacteria occurs.39 Another model is exemplied by gram-negative bacilli, which (1) produce a -lactamase that remains trapped in the periplasmic space and (2) have no barrier to antibiotic penetration. An example is H. inuenzae strains that produce the TEM-1 -lactamase.80 In this model and the rst one discussed, a marked inoculum effect occurs: the MIC for a large inoculum (106 organisms per milliliter) may be 1000-fold greater than that for a small inoculum (102/mL). The low level of resistance of single cells has made it possible for ampicillin to cure some infections caused by -lactamase-producing strains of H. inuenzae in which the inoculum of infecting bacteria was low.
Another model is exemplied by the ampicillin resistance of E. coli strains that produce the TEM-1 -lactamase. These bacteria have a barrier to entry of -lactam molecules (the outer membrane), and they produce a -lactamase that remains localized to the periplasmic space. In this model, the kinetics are more complicated. The enzyme is situated strategically between the barrier to antibiotic penetration (outer membrane) and the antibiotic targets (PBPs on the cytoplasmic membrane). In this position, the enzyme can destroy antibiotic molecules sequentially as they make their way through the barrier, analogous to a sharpshooter with abundant ammunition who aims at targets passing through a single entry point. As a consequence, high levels of resistance occur with single bacterial cells, in contrast to the previous example.39 Variations on this model occur when the amount of -lactamase produced increases with exposure to a -lactam (induction), as occurs in Enterobacter and Pseudomonas species. High levels of -lactamase are produced only after a period of exposure to the inducing antibiotic, and resistance may be expressed late. When Enterobacter strains are exposed to two -lactam antibiotics, one of which is a potent inducer (e.g., cefamandole), antagonism between the two antibiotics may result.77 Table 19-4 lists mechanisms of resistance to -lactam antibiotics. These mechanisms often work in concert and may accumulate in a single patient. For example, over a period of 3 months, a 19-month-old child with aplastic anemia had nine blood isolates of E. coli, all derived from a common ancestor, despite multiple courses of antibiotics including ceftazidime.81 The rst isolate produced a TEM-1 -lactamase but was susceptible to ceftazidime (MIC = 0.25g/mL). A later isolate became resistant (MIC of ceftazidime = 32g/mL) by acquiring a new plasmid-determined -lactamase (SHV-1) linked to efcient promoter and by turning off the production of an outer membrane porin. An even higher level of resistance (MIC of ceftazidime 128 g/mL) occurred when the SHV-1 -lactamase mutated to form the ESBL, SHV-8, which hydrolyzes ceftazidime much more rapidly. By turning off porin production to slow the rate of entry of ceftazidime into the periplasmic space and producing an ceftazidime-inactivating ESBL, the infecting E. coli used two mechanisms synergistically to achieve a high level of resistance to ceftazidime. Aminoglycoside ResistanceModifying Enzymes Among aerobic bacteria, aminoglycoside resistance is most commonly caused by modifying enzymes that are coded by genes on plasmids or
TABLE
19-4
Mechanisms of Resistance to -Lactam Antibiotics
I. Alter target site (PBP) A. Decrease afnity of PBP for -lactam antibiotic 1. Modify existing PBP a. Create mosaic PBP (1) Insert nucleotides obtained from neighboring bacteria (e.g., penicillin-resistant Streptococcus pneumoniae) (2) Mutate structural gene or genes of PBP (e.g., ampicillinresistant -lactamasenegative Haemophilus inuenzae) 2. Import new PBP (e.g., mecA in methicillin-resistant Staphylococcus aureus) II. Destroy -lactam antibiotic A. Increase production of -lactamase 1. Acquire more efcient promoter a. Mutate existing promoter b. Import new promoter 2. Deregulate control of -lactamase production a. Mutate regulator gene (e.g., ampD in stably derepressedEnterobacter cloacae) B. Modify structure of resident -lactamase 1. Mutate its structural gene (e.g., ESBLs in Klebsiella pneumoniae) C. Import new -lactamase with different spectrum of activity III. Decrease concentration of -lactam antibiotic inside cell A. Restrict its entry (loss of porins) B. Pump it out (efux mechanisms)
ESBL, extended-spectrum -lactamase; PBP, penicillin-binding protein.
19 Molecular Mechanisms of Antibiotic Resistance in Bacteria
285
TABLE
19-5
Aminoglycoside-Modifying Enzymes Usual Antibiotics Modied K, T, G, K K, A G T, G K, T, G K, T, A K, T, G K, T, A G, Ar G, K, T, FQ Common Genera SA, SR E, PS, SA, SR E, PS, SA, SR PR E, PS E, PS E, PS, SA E, PS SA SA, Ent E
Enzyme Phosphorylation APH(2) APH(3)I APH(3)III Acetylation AAC(2) AAC(3)I AAC(3)III, IV, or V AAC(6) Adenylation ANT(2) ANT(4) Bifunctional enzymes AAC(6)APH(2) AAC(6)Ib cr
A, amikacin; AAC, aminoglycoside acetyltransferase; ANT, aminoglycoside nucleotidyltransferase; APH, aminoglycoside phosphotransferase; Ar, arbekacin; cr, ciprooxacin resistance; E, Enterobacteriaceae; Ent, enterococci; FQ, uoroquinolone; G, gentamicin; K, kanamycin; PR, Providencia-Proteus; PS, pseudomonads; SA, staphylococci; SR, streptococci; T, tobramycin.
on the chromosome. Several aminoglycoside-modifying enzymes have been shown to be carried on transposons.82 More than 30 aminoglycoside-modifying enzymes that have been identied are capable of three general reactions: N-acetylation, O-nucleotidylation, and O-phosphorylation. For each of these reactions, there are several different enzymes that attack a specic amino or hydroxyl group. The nomenclature for these enzymes identies the molecular site where the modication occurs after the type of enzymatic activity. For example, an aminoglycoside acetyltransferase (AAC) that acts at the 3 site is designated AAC(3) (Table 19-5). Because more than one enzyme may catalyze the same reaction, roman numerals may also be necessary, as in AAC(3)IV. Enzymatic aminoglycoside resistance is achieved by modication of the antibiotic during the process of transport across the cytoplasmic membrane.83 Resistance to a particular aminoglycoside is a function of the balance between two different ratesthat of drug uptake and that of drug inactivation. An important factor in determining the level of resistance is the afnity of the modifying enzyme for the antibiotic. If an enzyme has a high afnity for the specic aminoglycoside, drug inactivation can occur at very low concentrations of the enzyme. The differences observed in the worldwide distribution of aminoglycoside-modifying enzymes may be partially a function of antibiotic selection pressures and may have had profound implications as to the choice of antibiotics used at specic medical centers. The aminoglycoside phosphotransferases APH(3) and APH(3) are distributed widely among gram-positive and gram-negative species worldwide and have led to decreased use of kanamycin and streptomycin. The gene for aminoglycoside nucleotidyltransferase ANT(2) was associated with multiple nosocomial outbreaks in the 1990s across the United States. The gene for aminoglycoside acetyltransferase AAC(6)I has been found to be more prevalent in enteric bacteria and in staphylococci in East Asia.84 The AAC(3) group of enzymes have been responsible for outbreaks of antibiotic resistance in South America, western Europe, and the United States. Although each outbreak of aminoglycosideresistant Enterobacteriaceae has its own pattern, the most typical manner of spread has been the appearance of a plasmid-carrying, aminoglycoside-resistant strain of K. pneumoniae, usually carrying the ANT(2) gene, with subsequent dissemination to other strains of the species and further spread later to other species and genera of Enterobacteriaceae.83 Major increases in plasmid-mediated aminoglycoside resistance have been noted among enterococci,85 initially in the developing
world86 but increasingly in the United States and Europe.87,88 Their clinical impact is exacerbated by the frequent cotransmission of -lactamases, which results in a loss of synergy when combination therapy is used for serious enterococcal infections. S. aureus and S. epidermidis have become increasingly resistant to aminoglycosides because of the interspecies and intraspecies dissemination of plasmidmediated, aminoglycoside-modifying enzymes.89 The two most interesting development in aminoglycoside-modifying enzymes have involved the discovery of bifunctional enzymes. The rst example is the AAC(6)APH(2) enzyme; it has two functioning active sites, one for acetylation and the other for phosphorylation of aminoglycosides. This bifunctional enzyme probably arose from a fusion event of the genes for these two enzymes. This enzyme is now widespread in staphylococci and enterococci, frequently residing on a common transposon (Tn4001) found on the chromosome and on transferable plasmids. AAC(6)APH(2) accounts for most of the high-level gentamicin and arbekacin resistance observed in methi cillin-resistant S. aureus (MRSA) isolates in many countries worldwide.90,91 The other major discovery regarding aminoglycoside-modifying enzymes is the existence of variant enzymes that can modify the structure of an entirely different class of antimicrobial agent. The rst bifunctional enzyme that was capable of modifying aminoglycosides and a uoroquinolone (ciprooxacin) was described in 2006.92 This enzyme, designated AAC(6)Ib cr, not only acetylates kanamycin, gentamicin, and tobramycin but also acetylates the piperazinyl side group of ciprooxacin. The acetylated quinolone is fourfold less active than the parent compound and may lead to clinically signicant resistance in enteric bacteria possessing other mechanisms for diminished quinolone activity. This enzyme has two important mutations in the gene for the basic AAC(6) enzyme (W102R and D179Y) and 12 unique base pairs at its 5 end that are essential to alter substrate specicity and allow ciprooxacin acetylation function for this enzyme.92 The widespread use of ciprooxacin and other uoroquinolones over the past 2 decades has changed the selection pressures on bacterial populations, promoting the development of quinolone resistance. Chloramphenicol Acetyltransferase Resistance to chloramphenicol in gram-positive and gram-negative organisms is mediated primarily by the inactivating enzyme, chloramphenicol acetyltransferase. This is an intracellular enzyme that inactivates the drug by 3-O-acetylation93 and is encoded by plasmid-borne or chromosomal genes. Despite homology at the active site of this enzyme, there is considerable diversity between chloramphenicol acetyltransferase enzymes isolated from gram-positive and from gramnegative organisms.94 Macrolide-, Lincosamide-, and StreptograminInactivating Enzymes Although resistance to erythromycin and other macrolides is frequently the result of alterations in the ribosomal target site or efux pumps, several substrate-inactivating enzymes have been characterized.95 Erythromycin esterases have been isolated from E. coli that hydrolyze the lactone ring of the antibiotic and result in its inactivation. This is a plasmid-mediated resistance determinant that is constitutively produced and results in high-level resistance to erythromycin (MIC > 2000 g/mL).96 These resistance genes limit the utility of oral erythromycin or other macrolides in reducing the aerobic gramnegative ora of the intestinal tract before gastrointestinal surgical procedures. Other plasmid-mediated resistance genes generate specic inactivating enzymes in Streptococcus hemolyticus and S. aureus that adenylate97 lincosamides or acetylate98 or hydrolyze99 streptogramins. Tetracycline Inactivation A tetracycline-inactivating enzyme called TetX has been described rarely in Bacteroides species.100 Tetracycline resistance is principally
286
PART I Basic Principles in the Diagnosis and Management of Infectious Diseases
TABLE
19-6
Mechanisms of Tetracycline Resistance Tet Determinant tetA-L, P*, V, Y, Z, otrB, tcr3, Tet 30 tetM, O, P*, Q, S, T, W, otrA tetX tetU, otrC Common Bacterial Species Enterobacteriaceae, Pseudomonas, Streptomyces, Staphylococcus, Streptococcus spp. Gram-positive and gram-negative anaerobes; Neisseria, Haemophilus, Enterococcus, Staphylococcus, Streptococcus spp. Bacteroides spp. Mycobacteria, Enterococcus spp. Helicobacter pylori
Resistance Mechanism Drug efux Ribosomal protection Enzymatic inactivation Unknown mechanism Altered ribosomal target
Resistance to nalidixic acid and other quinolones has been associated with alterations of outer membrane proteins in Serratia marcescens114 and P. aeruginosa. However, single-step, high-level mutational resistance to nalidixic acid by aerobic gram-negative bacilli occurs with a frequency of 107, whereas only low-level resistance to the newer quinolones (less than 10 times the MIC) usually is obtained with a single-step selection of less than about 109.115 Plasmid-mediated chloramphenicol resistance resulting from decreased permeability has been demonstrated in E. coli.116 Inner Membrane Permeability The rate of entry of aminoglycoside molecules into bacterial cells is a function of their binding to a usually nonsaturable anionic transporter, whereupon they retain their positive charge and subsequently are pulled across the cytoplasmic membrane by the internal negative charge of the cell.117 This process requires energy, and a threshold minimal level of internal negative charge inside the cell must be present before signicant transport occurs; this is called the proton motive force.118 The level of the internal charge that is required may depend on the actual aminoglycoside concentration at a given time. Either the energy generation or the proton motive force that is required for substrate transport into the cell may be altered in mutants resistant to aminoglycosides. Aminoglycoside-resistant isolates with altered proton motive force occur rarely but develop in the course of long-term aminoglycoside therapy.119 These isolates usually have a small colony phenotype because of their reduced rate of growth. They may be unstable and revert to a sensitive phenotype in the absence of selective aminoglycoside pressure. The clinical signicance of these isolates is not clear. They may retain some virulence120 and rarely may cause fatal bacteremia.121 Because oxidative metabolism is essential for aminoglycoside uptake action and for cell growth and development, Pseudomonas mutants have been found that are decient in specic cytochromes.122 Resistant mutants with defective electron transport systems have been described in E. coli, S. aureus, and Salmonella spp. Facultative organisms grown anaerobically are resistant to aminoglycosides because of a marked reduction in uptake of the antibiotic. PROMOTION OF ANTIBIOTIC EFFLUX Tetracyclines Active efux of antimicrobial agents is recognized increasingly as a common mechanism of resistance in many clinically relevant pathogens. Some strains of E. coli, Shigella spp., and other enteric organisms express a membrane transporter system that leads to multidrug resistance by drug efux.122 Many of these are multicomponent, regulated, energy-dependent transporter systems that promote the active efux of multiple classes of antibiotics. Specic efux pumps also exist that promote the egress of single classes of antimicrobial agents. The major mechanism of resistance to tetracyclines found in enteric gram-negative organisms is decreased accumulation of tetracycline (see Table 19-6). This reduced uptake is an energy-dependent process that is related to the generation of an inner membrane protein produced by the tetracycline-resistance determinant (designated Tet) or resistance gene products for oxytetracycline derivatives (Otr). The primary mechanism for the decreased accumulation of tetracycline is through active efux of the antibiotic across the cell membrane.123 Decreased uptake of tetracycline from the extracellular environment also accounts for decreased accumulation of tetracycline inside resistant cells. These resistance determinants may be found on the chromosome or plasmids and frequently are found on transposable genetic elements. Tetracycline-resistance genes are generally inducible by subinhibitory concentrations of tetracycline. There are almost 40 recognized tetracycline-resistance determinants, most of which mediate drug efux.124 Their genes were designated in the past by letters (e.g., tetA, tetB). Because there are now more determinants than letters in the English alphabet, new tet genes are designated by numbers (e.g., tet30).
*Tet P has two different genes that mediate different mechanisms of resistance.
mediated by other mechanisms, including efux and ribosomal protection (Table 19-6). DECREASED PERMEABILITY OF BACTERIAL MEMBRANES Outer Membrane Permeability It was recognized early in the history of antibiotic development that penicillin is effective against gram-positive bacteria but not against gram-negative bacteria.101 This difference in susceptibility to penicillin is due in large part to the outer membrane, a lipid bilayer that acts as a barrier to the penetration of many antibiotics into the cell.102 Situated outside the peptidoglycan cell wall of gram-negative bacteria, this outer membrane is absent in gram-positive bacteria. The outer portion of this lipid bilayer is composed principally of lipopolysaccharide made up of tightly bound hydrocarbon molecules that impede the entry of hydrophobic antibiotics, such as nafcillin or erythromycin.103,104 Agents that disrupt the integrity of the lipopolysaccharide layer (e.g., polymyxin) or mutations that lead to the production of defective lipopolysaccharides result in increased permeability of hydrophobic antibiotics.105 The passage of hydrophilic antibiotics through this outer membrane is facilitated by the presence of porins, proteins that are arranged so as to form water-lled diffusion channels through which antibiotics may traverse the membrane.106 Bacteria usually produce many porins; approximately 105 porin molecules are present in a single cell of E. coli. Bacteria are able to regulate the relative number of various porins in response to the osmolarity of the surrounding medium. In hyperosmolar media, E. coli may repress production of the larger porins (OmpF) while continuing to express smaller ones (OmpC).107 The rate of diffusion of antibiotics through this outer membrane is a function not only of the numbers and properties of the porin channels but also of the physicochemical characteristics of the antibiotic. In general, the larger the antibiotic molecule, the more negative the charges, and the greater the degree of hydrophobicity, the less likely it is to penetrate through the outer membrane.108 Small hydrophilic molecules with a zwitterionic charge, such as imipenem, are highly permeable. Larger, highly charged molecules, such as carbenicillin, are much less permeable. Mutations resulting in the loss of specic porins can occur in clinical isolates and determine increased resistance to -lactam antibiotics. Resistance to aminoglycosides and carbapenems emerging during therapy has been associated with a lack of production of outer membrane proteins.109,110 For example, emergence of imipenem resistance during therapy, observed in up to 25% of P. aeruginosa infections,111 has been ascribed to mutational loss of its OprD protein (also known as the D2 porin).109-113
19 Molecular Mechanisms of Antibiotic Resistance in Bacteria
287
Macrolides and Streptogramins In some strains of Streptococcus pneumoniae, Streptococcus pyogenes, S. aureus, and S. epidermidis, an active efux mechanism causes resistance to macrolides, streptogramins, and azalides.125 This efux mechanism is mediated by the mef (for macrolide efux) genes in streptococci and msr (for macrolide streptogramin resistance) genes in staphylococci.126 A similar efux system, encoded by a gene called mreA (for macrolide resistance efux A), has been described in group B streptococci.127 This mechanism of resistance is prevalent in communityacquired infections,128 and dissemination of these resistance genes among important bacterial pathogens is a considerable threat to the usefulness of macrolide antibiotics (Table 19-7). -Lactams Active efux mechanisms also may contribute to the full expression of -lactam resistance in P. aeruginosa. Multidrug efux pumps in the inner and outer membrane of P. aeruginosa act in concert with periplasmic -lactamases and membrane permeability components to protect the bacterium from -lactam agents.129,130 Fluoroquinolones Active efux of uoroquinolones has been detected in enteric bacteria131,132 and in staphylococci.128,133 This efux may be related to a multiple-antibiotic resistance transporter128 (i.e., NorA) or a specic quinolone efux pump (i.e., EmrAB, AcrAB). This mechanism of limiting access of high levels of uoroquinolones works in concert with other mechanisms (point mutations of DNA gyrases, permeability barriers, and acetylation) for full expression of quinolone resistance. ALTERED TARGET SITES Alteration of Ribosomal Target Sites Macrolides, Lincosamides, and Streptogramins. Resistance to a wide variety of antimicrobial agents, including tetracyclines, macrolides, lincosamides, streptogramins, and the aminoglycosides, may result from alteration of ribosomal binding sites. Failure of the antibiotic to bind to its target site or sites on the ribosome disrupts its ability to inhibit protein synthesis and cell growth. For macrolides, lincosamides, and streptogramin B, this is the principal mechanism of multiple-agent resistance among aerobic and anaerobic gram-positive organisms.126 Resistance is mediated by the products of the erm (erythromcyin ribosome methylation) gene: the variety of methylase enzymes (MLSB-determinant) that dimethylate adenine residues on the 23S ribosomal RNA (rRNA) of the 50S subunit of the prokaryotic ribosome, disrupting the binding of MLS to the ribosome (see Table 19-7). Different classes of this resistance determinant may be located on plasmids or on the bacterial chromosome.
TABLE
MLSB resistance resulting from ribosomal methylation has been described in many species, including S. aureus, Streptococcus sanguis, B. fragilis, and Clostridium perfringens. MLS resistance may be constitutive or inducible by either older macrolides (e.g., erythromycin) or newer azalides. In S. pneumoniae, resistance is encoded by the ermB gene, which is responsible for the methylation of loop V of the 23S ribosomal subunit.134,135 In addition, point mutations in ribosomal proteins L4 and L22 of the 50S subunit have been described that render S. pneumoniae resistant to macrolides.136 Inducible resistance in streptococci is generated by a variety of lincosamides and macrolides, resulting in cross-resistance to the MLSB antibiotics. In staphylococci, only 14 to 15 numbered macrolides induce MLSB methylation, and the organisms express resistance to macrolides only. Tetracyclines. Tetracycline resistance may be mediated by a variety of mechanisms, the most common of which are efux mechanisms and ribosomal protection mechanisms (see Table 19-6).137 An additional, unusual mechanism of tetracycline resistance through alteration of the target site of action has been found in Helicobacter pylori.138 This organism can possess a mutation in its 16S rRNA that limits tetracycline binding to its target site at the 30S subunit of the bacterial ribosome. Aminoglycosides. Resistance to aminoglycosides is also mediated at the ribosomal level. In Enterobacteriaceae and nonfermenting gramnegative bacteria, methylation of the 16S rRNA (the site at which aminoglycosides bind and inhibit protein synthesis) by enzymes usually carried on plasmids is mediated by the rmtA gene and related genes (rmtB, rmtC, armA). This is now recognized as a major mechanism of resistance to all parenteral aminoglycosides that appears to be spreading globally.139 Mutations of the S12 protein of the 30S subunit have been shown to interfere with binding of streptomycin to the ribosome. Ribosomal resistance to streptomycin may be a signicant cause of streptomycin resistance among enterococcal isolates.140 Ribosomal resistance to the 2-deoxystreptamine aminoglycosides (gentamicin, tobramycin, amikacin) seems to be uncommon and may require multiple mutations in that these aminoglycosides appear to bind to several sites on the 30S and 50S subunits of the prokaryotic ribosome. Ribosomal resistance often is associated with decreased intracellular accumulation of the drug.141 Ketolides. Although ketolides were only recently introduced into clinical practice, clinical isolates of S. pneumoniae resistant to telithromycin have been reported and are caused by constitutive expression of the erm gene, mutations in domains II and V of the 23S rRNA binding sites, and mutations within ribosomal proteins L4 and L22.142
19-7
Resistance Mechanisms against the Macrolides, Lincosamides, and Streptogramins Resistance Pattern
Bacterial Species Streptococci, Enterococci
Staphylococci
Gene Designation erm (A,B) erm (A,B) mef (A or E) L4/L22 mut Inu (B) erm (A,C) erm (A,C) Msr (A or B) Vgb, vgbB Ere A or B Inu (A)
Phenotype MLSB-inducible MLSB-constitutive M M L MLSB-inducible MLSB-constitutive MSB SB M L
Resistance Mechanism Ribosomal methylation Ribosomal methylation Efux Ribosomal mutation Inactivation Ribosomal methylation Ribosomal methylation Efux Inactivation Inactivation Inactivation
14- or 15-Membered Ring* (s) I or R R I or R R S R R R S R S
16-Membered Ring (s) I or R R S R S (s) R S S R S
Clindamycin (s) I or R R S S SI (s) R S S S SI
Streptogramin B (s) I or R R S S S (s) R R R S S
*14- or 15-membered ring structures, erythromycin, clarithromycin, azithromycin. 16-membered ring structures, spiramycin. I, intermediate susceptibility; R, resistant; (s), appears susceptible in vitro but may select resistant clones in vivo; S, sensitive.
288
PART I Basic Principles in the Diagnosis and Management of Infectious Diseases
Oxazolidinones. Resistance to linezolid, the main oxazolidinone currently in clinical use, has been described in gram-positive isolates (S. aureus, Enterococcus faecium, Enterococcus faecalis, S. epidermidis) as a result of point mutations within the genes encoding the 23S rRNA of the 50S ribosomal subunit, the antibiotics main binding site.143 Specically, translocation of peptidyltransfer RNA from the A site to the P site during translation from bacterial ribosomes is inhibited through G-to-U substitutions at position 2576 or similar binding sites in the peptidyl transferase region of 23S rRNA.144 Resistance development has been observed during prolonged linezolid therapy in vancomycinresistant enterococcus (VRE) bacteremia.145 Alteration of Cell Wall Precursor Targets Vancomycin and other glycopeptide antibiotics, such as teicoplanin, bind to d-alanine-d-alanine, which is present at the termini of the steam peptide in peptidoglycan precursors. The large glycopeptide molecules prevent incorporation of the precursors into the cell wall. Resistance of enterococci to vancomycin has been classied into six varieties, based on genotype, type of target site alteration, and level of resistance to vancomycin and susceptibility or resistance to teicoplanin (Table 19-8).146,147 Strains of E. faecium and E. faecalis with high-level resistance to vancomycin and teicoplanin have class A resistance. Either vancomycin or teicoplanin can induce resistance in these strains. Class A resistance to glycopeptides transfers by conjugation from E. faecium to other gram-positive bacteria,148 including E. faecalis,149 S. pyogenes, S. sanguis, and Listeria monocytogenes. The vanA gene on the plasmid encodes an inducible protein that is related to the d-alanined-alanine ligases involved in cell wall synthesis in E. coli.150 This protein synthesizes peptidoglycan precursors that have a depsipeptide terminus (d-alanine-d-lactate) instead of the usual d-alanine-d-alanine. The modied peptidoglycan binds glycopeptide antibiotics with reduced afnity, conferring resistance to vancomycin and teicoplanin.151,152 Strains of E. faecium and E. faecalis with class B resistance have levels of resistance to vancomycin that range from high (MIC = 1024g/mL) to low (MIC = 4g/mL) and are susceptible to teicoplanin. Vancomycin, but not teicoplanin, can induce resistance to vancomycin and teicoplanin in these strains. The genes determining the VanB phenotype are self-transferable by conjugation to other Enterococcus strains.153,154 All isolates of Enterococcus gallinarum, Enterococcus casseliavus, and Enterococcus avescens possess low-level resistance to vancomycin and are susceptible to teicoplanin (class C phenotype). The resistance is mediated by chromosomal genes known as vanC1, vanC2, or vanC3.155 The vanC gene complex gives rise to resistance to vancomycin by synthesis of an alternative dipeptide, d-alanine-d-serine, in which a serine replaces the terminal alanine. Other variant genes, known as vanE and vanG, have been found in enterococcal species and also mediate various levels of glycopeptide resistance (see Table 19-8). Since 1987, reports from the United States and Japan have documented outbreaks of vancomycin-resistant S. epidermidis,156 S. haemo-
lyticus,157 and S. aureus.158 The rst vancomycin-resistant S. aureus (VRSA) isolate in the United States was recovered in 2002 from a foot ulcer in a diabetic patient who was receiving chronic hemodialysis, concurrently with a VRE strain from the same wound.159 DNA sequencing revealed identical vanA genes in both isolates, and further molecular analysis implicated plasmid-mediated transfer of resistance, through the Tn1546 genetic element encoding the vanA gene, from the enterococcus (VRE) strain into the vancomycin-susceptible MRSA strain recovered from the same patient, rendering it vancomycin resistant (VRSA).159,160 Alteration of Target Enzymes -Lactams. -Lactam antibiotics inhibit bacteria by binding covalently to PBPs in the cytoplasmic membrane. These target proteins catalyze the synthesis of the peptidoglycan that forms the cell wall of bacteria.165 Alterations of PBPs can lead to -lactam antibiotic resistance.166 In gram-positive bacteria, resistance to -lactam antibiotics may be associated with a decrease in the afnity of the PBP for the antibiotic167 or with a change in the amount of PBP produced by the bacterium.168 Multiple mechanisms seem to be present in some clinical isolates. Penicillin-resistant strains of S. pneumoniae isolated in South Africa showed several changes in PBPs: decreased afnity of some PBPs, loss of others, and appearance of PBPs not present in the more susceptible cells.169 The genes that encode these PBPs are mosaics, composed of segments from susceptible pneumococci and segments from resistant commensal streptococci.170 In S. aureus171-173 and E. faecium,174 additional PBPs may be inducible (i.e., their production is stimulated by exposure of the microorganism to the -lactam antibiotic). These inducible PBPs have a lower afnity for -lactam antibiotics, making them less susceptible to inhibition by low concentrations of drug. Changes in the types of PBPs observed in susceptible and resistant strains also have been seen with the viridans streptococcal species Streptococcus mitis.175 Methicillin. In S. aureus, methicillin resistance is conferred by the expression of the mecA gene, which encodes PBP2a, a protein with low afnity for -lactam antibiotics, conferring resistance to methicillin, nafcillin, oxacillin, and cephalosporins. The mecA gene is the structural component of the mec gene cassette, and it is inserted into the larger staphylococcal cassette chromosome mec (SCCmec), which appears to have been acquired by horizontal transfer from a coagulase-negative Staphylococcus species.176 At least ve different SCCmec types of varying genetic sequences and size have been described. Types I through III are found in health careassociated MRSA strains and tend to be larger and multidrug resistant. Types IV and V are associated with community-acquired MRSA strains; they tend to be smaller and are more susceptible to antibiotics other than -lactamases. Expression of the methicillin-resistance gene is controlled by two regulatory components of the mec gene, mecR1 and mecI, and the -lactamase genes, blaI, blaRI, and blaZ, which can downregulate mecA transcription. Although the mecA gene is present in all MRSA
TABLE
19-8
Vancomycin Resistance in Enterococci and Staphylococci A B 4 to >500 0.5 to 2 Inducible P, C d-ala-d-lac E. faecalis, E. faecium 64 to >500 16 to >500 Inducible P, C d-ala-d-lac E. faecalis, E. faecium, S. aureus C 2 to 32 0.5 to 2 Constitutive, inducible C d-ala-d-Ser E. gallinarum (C-1) E. casseliavus (C-2) E. avescens (C-3) D 64 to 128 4 to 64 Constitutive C d-ala-d-lac E. faecium E 16 0.5 Inducible C d-ala-d-ser E. faecalis G 12 to 16 0.5 ND C d-ala-d-ser E. faecalis
MIC for Vanco (g/mL) MIC for Teico (g/mL) Expression Genetic location Target alteration Common species
ala, alanine; C, chromosome; E., Enterococcus; lac, lactate; MIC, minimal inhibitory concentration; ND, not described; P, plasmid; S., Staphylococcus; ser, serine; Teico, teicoplanin; Vanco, vancomycin.
19 Molecular Mechanisms of Antibiotic Resistance in Bacteria
289
isolates, the phenotypic expression of methicillin resistance is more variable. For example, S. aureus isolates grown at 32C, rather than at 37C, are more likely to express methicillin resistance.177 The expression of methicillin resistance seems to be modied also by auxiliary genes, such as fem and aux, which are present in the staphylococcal chromosome and affect various steps in peptidoglycan synthesis.178,179 The PBPs of -lactamasenegative, penicillin-resistant strains of N. gonorrhoeae, Neisseria meningitidis, and H. inuenzae have shown reduced penicillin-binding afnity.180-183 Their PBPs seem to be encoded by hybrid genes containing segments of DNA scavenged from resistant strains of related species, similar to penicillin-resistant pneumococci.184 Mutations leading to a loss of outer membrane proteins may be associated with the acquisition of penicillin resistance in non penicillinase-producing strains of N. gonorrhoeae, suggesting that altered permeability also may contribute to the resistance.185 Permeability changes and decreased afnity of PBPs are mechanisms found jointly in clinical isolates of P. aeruginosa186 and in non-lactamase producing strains of H. inuenzae.187 Multiple mutations may be necessary to effect this type of resistance. Quinolones. DNA gyrase (also called bacterial topoisomerase II) is necessary for the supercoiling of chromosomal DNA in bacteria to accomplish efcient cell division.188 Another related enzyme, topo isomerase IV, also is required for segregation of bacterial genomes into two daughter cells during cell division. These enzymes consist of two A subunits encoded by the gyrA gene and two B subunits encoded by the gyrB gene (or parC and parE for topoisomerase IV). Although spontaneous mutation in the gyrA locus is the most common cause of resistance to multiple uoroquinolones in enteric bacteria, B-subunit alterations also may affect resistance to these drugs. Quinolone resistance may occur as a result of decreased cell wall permeability, efux, or enzyme protection mechanisms.9 DNA gyrase is the primary site of action in gram-negative bacteria, whereas topoisomerase IV is the principal target of quinolones in gram-positive bacteria, including S. aureus. Mutations in a variety of chromosomal loci have been described that result in altered DNA gyrases resistant to nalidixic acid and the newer uoroquinolones in Enterobacteriaceae and P. aeruginosa.189,190 Many of these mutations involve the substitution of single amino acids at the quinolone resistancedetermining region (QRDR; located between amino acids 67 and 106 in the gyrase A subunit), which is involved in generation of the DNA gyrasebacterial DNA complex.191,192 Clinical isolates of C. freundii in Japan were found to be highly resistant to the newer quinolones as a result of alterations in the DNA gyrase.193 Plasmid-mediated quinolone resistance has been found in various Enterobacteriaceae and is conferred by qnr-encoded proteins that bind to the DNA gyrase antibiotic target and protect it from quinolone action. Although uoroquinolone resistance associated with plasmidborne qnr genes is low-level resistance, these genes are usually linked to other antibiotic-resistance determinants carried on the same mobile element and have been associated with clinical MDR phenotypes.9,194-196 Another plasmid-derived quinolone resistance, encoded by the aac(6)Ib cr gene and derived by mutation of a plasmid-contained aminoglycoside-modifying enzyme, appears to be widely disseminated among E. coli isolates in the United States, mediating low-level ciprooxacin resistance.92 Sulfonamides. There are two common genes that mediate resistance to sulfa drugs in pathogenic bacteria: sul1 and sul2. These genes give rise to altered forms of the target enzyme for sulfonamide, dihydro pteroate synthase (DHPS).197 This enzyme is essential for folic acid synthesis in susceptible bacteria. The altered DHPS enzymes mediated by the sulfonamide-resistance genes no longer bind to sulfa, yet they continue to synthesize dihydropteroate from para-aminobenzoic acid substrate. The ubiquitous sul1 gene is part of the class 1 integron family, giving rise to widespread resistance to sulfonamides.38
Trimethoprim. Trimethoprim is a potent inhibitor of bacterial dihydrofolate reductase (DHFR). Many altered DHFR enzymes with loss of inhibition by trimethoprim have been described from genes found primarily on resistance plasmids. These altered DHFR genes are widespread in gram-negative bacteria and are found in staphylococci (dfrA gene).198,199 PROTECTION OF TARGET SITES Tetracyclines Tetracycline resistance may occur by a mechanism that interferes with the ability of tetracycline to bind to the ribosome. The ubiquitous tetM resistance gene and related tetracycline-resistance determinants protect the ribosome from tetracycline action. The precise molecular site of action of this resistance mechanism is unclear. The tetM is dispersed widely in gram-positive organisms and in Mycoplasma,124 Ureaplasma,21 Campylobacter,124 and Neisseria20 species. The tetM gene generates protein with elongation factorlike activity that stabilizes ribosome transfer RNA interactions in the presence of tetracycline molecules. Fluoroquinolones The newly recognized plasmid-mediated, antibiotic-resistance gene mediating quinolone resistance seems to function as a target protection system.9 The resistance mechanism seems to protect DNA gyrase from binding to quinolones, allowing the bacterium to resist quinolone inhibitory effects. When this low-level resistance determinant is expressed in concert with another quinolone-resistance gene, such as DNA gyrase mutations, clinical failures with the use of uoroquinolones can result. OVERPRODUCTION OF TARGET Sulfonamides and Trimethoprim Sulfonamides compete with para-aminobenzoic acid to bind the enzyme DHPS and halt the generation of pteridines and nucleic acids. Sulfonamide resistance may be mediated in some bacteria by overproduction of the synthetic enzyme DHPS. The gene responsible for DHPS is felP, and strains of bacteria that produce excess DHPS can overwhelm sulfa inhibition.197 Trimethoprim resistance may occur in a similar fashion, by production of excess amounts of DHFR from the bacterial chromosomal gene folA.198,199 BYPASS OF ANTIBIOTIC INHIBITION Another mechanism for acquiring resistance to specic antibiotics is by the development of auxotrophs, which have growth factor requirements different from those of the wild strain. These mutants require substrates that normally are synthesized by the target enzymes; if the substrates are present in the environment, the organisms are able to grow despite inhibition of the synthetic enzyme. Enterococci can be folate auxotrophs requiring environmental acquisition of folic acid for growth. They become intrinsically resistant to folic acid inhibitors (sulfa drugs or trimethoprim) in the process. Bacteria with mutations in the enzyme thymidylate synthetase can retain viability but become thymine dependent. They require exogenous supplies of thymidine to synthesize thymidylate via salvage pathways and are highly resistant to sulfa drugs and trimethoprim.200 BIND-UP ANTIBIOTIC Vancomycin-intermediate S. aureus (VISA) expresses unusually thick peptidoglycan cell walls that are less completely cross-linked together.161 The cell wall in some strains of VISA contains nonamidated glutamine precursors that provide an increased number of false binding sites to vancomycin.162,163 The vancomycin molecules are absorbed to these excess binding sites, preventing the antibiotic from reaching its target and allowing peptidoglycan synthesis in the cytoplasmic membrane to continue uninhibited.163 The specter of increasing outbreaks of vanco-
290
PART I Basic Principles in the Diagnosis and Management of Infectious Diseases
mycin-resistant staphylococci has led the U.S. Centers for Disease Control and Prevention to develop vigorous interim guidelines to mitigate the spread of this serious nosocomial problem.164 A compilation of the most frequent mechanisms of resistance used by common bacterial pathogens to inhibit the actions of antibiotics is provided in Table 19-9. Multiple mechanisms are increasingly in operation at the same time within individual bacterial cells. The problem of multiple antibiotic resistance expression is considered in the following sections.
TABLE
RESISTANCE TO NEWER, OLDER, AND MISCELLANEOUS AGENTS The major mechanisms of bacterial resistance to newer agents and to agents, such as polymyxin B and related compounds, that have experienced renewed interest in response to progressive antibiotic resistance are summarized in Table 19-10. The oxazolidinone agent linezolid is an inhibitor of initiation of bacterial translation and has proved useful in the treatment of gram-positive bacterial infections,
19-9
Resistance Mechanisms Found in Common Bacterial Pathogens Resistance Phenotype -Lactams Macrolides, lincosamides, streptogramin B Tetracycline Trimethoprim and sulfonamides Fluoroquinolones -Lactams: Penicillin -Lactams: Methicillin, oxacillin, nafcillin, and cephalosporins (MRSA) Glycopeptides: GISA Glycopeptides: GRSA -Lactams (ampicillin) Aminoglycosides Vancomycin Linezolid Quinupristin-dalfopristin Penicillins Fluoroquinolones Tetracycline Macrolides MDR -Lactams Aminoglycosides Fluoroquinolones MDR Major Resistance Mechanisms Alteration of target enzymes (PBPs) Alteration of ribosomal target sites (methylation of adenine residue in domain V of 23S rRNAermB); efux (mefE) Protection of ribosomal target site (tetM) Alteration of target enzymes (DHFR)trimethoprim; DHPS synthasesul1, sul2 in sulfonamides) Alteration of target enzymes (DNA gyrasegyrA mutations; topoisomerase IVparC mutations Enzymatic inhibition (penicillinase production) Alteration of target enzymePBP2a (mecA) Alteration of cell wall precursor targets (thickened cell wall binds drug, preventing it from reaching its target) Alteration of cell wall precursor targets (plasmid-mediated transfer of vanA genes from VRE, resulting in d-ala-d-lac peptidoglycan precursors) Alteration of target enzymes (PBP5 in E. faecium); enzymatic inhibitionrare (penicillinase in E. faecalis) Altered ribosomal target site mutations; enzymatic inhibition (high-level resistance: AMEs) Alteration of cell wall precursor targets (high-level resistance: vanA, vanB, vanD phenotypes; low-level resistance: vanC, vanE, vanG phenotypes) Alteration of ribosomal target sites (G2576U mutation in domain V of 23S rRNA) Enzymatic inhibition; efux; target modication (E. faecium) PPNG: enzymatic inhibition (plasmid-acquired penicillinase); CRNG: altered target enzymes (PBPs) Alteration of target enzymes (DNA gyrase, topoisomerase IV); efux (MtrR-CDE efux system) Protection of ribosomal target (tetM gene) Efux; alteration in ribosomal targets (C2611T mutation in domain V of the 23S rRNA) Efux (MtrR-CDE system: confers resistance to penicillin, tetracycline, macrolides) Enzymatic inhibition (ampC cephalosporinases, ESBLs, MBLs); active efux (MexAB); reduced outer membrane permeability (loss of OprD channel) Enzymatic inhibition (AMEs); efux (MexXY); alteration of ribosomal targets (ribosomal methylation) Efux (MexAB, CD, EF, XY, GH, VW); alteration of target enzymes (DNA gyrase mutationsgyrA) Overexpression of the MexA-MexB-OprM active efux system (resistance to quinolones, tetracyclines, and trimethoprim) Enzymatic inhibition (ampC cephalosporinases, plasmid-acquired -lactamases of the TEM, SHV, CTX-M, PER, VEB families; MBLs of the IMP, VIM, SIM families; and OXA-type serine carbapenemases); alteration of target enzymes (PBPs); reduced outer membrane permeability; efux pumps Enzymatic inhibition (AMEs); efux pumps Efux pumps Efux pumps Impermeable outer membrane; enzymatic inhibition (inducible MBLs L1, L2) Alteration in sulfonamide target enzymes (sul1, sul2 genesassociated with plasmids or class 1 integrons) Alteration of target enzymes (DNA gyrase mutations); efux pumps MDR efux pump (SmeDEFconfers resistance to tetracycline, erythromycin, chloramphenicol, noroxacin, ooxacin) Enzymatic inhibition (constitutive expression of penicillinases; ESBLs; KPC carbapenemases); decreased outer membrane permeability Alteration of target enzymes (DNA gyrase mutationsgyrA); efux; protection of target site (plasmid-mediated qnr genes) Enzymatic inhibition (AMEs); alteration of ribosomal targets (ribosomal methylation) Enzymatic inhibition (chromosomally encoded cepA cephalosporinases; MBLs); efux (homologues of RND pumps); alteration in drug targets (PBPs) Alteration of ribosomal targets Protection of ribosomal target (tetQ); efux Alteration of target enzymes (DNA gyrase mutationsgyrA); efux
Pathogen Streptococcus pneumoniae
Staphylococcus aureus
Enterococci
Neisseria gonorrhoeae
Pseudomonas aeruginosa
Acinetobacter baumannii
-Lactams Aminoglycosides Quinolones Tigecycline -Lactams TMP-SMX Fluoroquinolones MDR -Lactams Fluoroquinolones Aminoglycosides -Lactams Macrolides, lincosamides, streptogramin B Tetracycline Quinolones
Stenotrophomonas maltophilia
Klebsiella pneumoniae
Bacteroides spp.
ala, alanine; AMEs, aminoglycoside-modifying enzymes; CRNG, chromosomally resistant N. gonorrhoeae; DHFR, dihydrofolate reductase; DHPS, dihydropteroate synthase; E., Enterococcus; ESBL, extended-spectrum -lactamase; GISA, glycopeptide-intermediate S. aureus; GRSA, glycopeptide-resistant S. aureus; lac, lactate; MBL, metallo--lactamase; MDR, multidrug resistance; MRSA, methicillin-resistant S. aureus; PBPs, penicillin-binding proteins; PPNG, penicillinase-producing N. gonorrhoeae; RND, resistance nodulation division; rRNA, ribosomal RNA; TMP-SMX, trimethoprim-sulfamethoxazole; VRE, vancomycin-resistant enterococcus.
19 Molecular Mechanisms of Antibiotic Resistance in Bacteria
291
19-10
TABLE
Resistance Mechanisms of Newer, Older, and Other Antimicrobial Agents Polymyxin ++ ++ Daptomycin + (GN) ++ + Linezolid + (GN) + ++ Metronidazole ++ Tigecycline + ++
Mechanism Enzymatic inactivation Decreased permeability Efux Alteration of target site Protection of target site Overproduction of target Bypass of inhibited process Bind up antibiotic
+++, most common mechanism; ++, common; + less common; , absent; GN, gram-negative.
particularly those expressing resistance to standard antibiotics, such as MRSA, glycopeptide-resistant S. aureus (GRSA), and VRE. Resistance is primarily related to mutations at the 23S rRNA binding site of the antimicrobial agent.144,145,201 Efux mechanisms may also contribute to reduced activity of linezolid in some bacterial species.202 Polymyxin is a cationic peptide antibiotic that alters the permeability of the outer membrane of gram-negative bacteria. The use of polymyxin has been rekindled in light of the limited number of therapeutic options available to treat MDR bacilli. Resistance is attributable to binding up the agent to the polysaccharide capsule203 or to alterations in the afnity of binding to the outer membrane lipid target of polymyxin B.204 The lipopeptide daptomycin is now widely used for treatment of MRSA and GRSA infections. The drug induces permeability changes and loss of intracellular potassium in susceptible gram-positive bacteria. Resistance is often associated with the abnormally thick cell wall characteristic of VISA strains.205,206 Accumulation of mutations, especially with the gene mprF (encoding lysylphosphatidylglycerol synthetase) indicates that the alterations in potential cell membrane binding sites account for reduced daptomycin activity.207 Tigecycline is a glycylcycline antibiotic with a mechanism of action like that of tetracyclines but with remarkable resistance to many of the standard tetracycline-resistance mechanisms. Recent evidence indicates that some unusual efux pumps are expressed in some MDR gram-negative bacilli.208-210 Metronidazole resistance is related to loss of activity of reduced nicotinamide adenine dinucleotide phosphate (NADPH) nitroreductase through mutations of the synthetic gene rdxA. This enzyme activity is essential to covert metronidazole to its active metabolite.211 These mechanisms are summarized on Table 19-10.
those encoding topoisomerase IV or DNA gyrase targets, rendering uoroquinolones ineffective).214 The clinically important MDR efux pumps belong to several different families: (1) the resistance nodulation division (RND) family; (2) the major facilitator superfamily (MFS); (3) the staphylococcal multiresistance (SMR) family; and (4) the multidrug and toxic compound extrusion (MATE) family. Such efux pumps are widespread among prokaryotes (Fig. 19-5) and are responsible for the export of toxic substances, allowing survival in a noxious environment (e.g., the biliary system for enteric bacteria).215 They may also play a role in mediating bacterial adherence to host tissues and exporting virulence determinants, as has been described for P. aeruginosa.216 Bacteria can also acquire multidrug resistance through sequential transfer of multiple-resistance determinants located on mobile genetic elements. For example, conjugative transposons such as Tn916, which confer conferring resistance to tetracycline and chloramphenicol, can easily disseminate among bacterial species.217 Transposons often coexist with other genetic elements, such as plasmids, that may carry
Outer membrane TolC
AcrA
Multidrug-Resistance Mechanisms among Bacteria
Bacteria can express more than one mechanism of antibiotic resistance, leading to MDR phenotypes or even pan-resistance. For example, molecular analysis of P. aeruginosa isolates from a nosocomial outbreak in Belgium revealed the convergence of several strategies for antibiotic resistance: (1) overexpression of AmpC chromosomal -lactamases conferring resistance to multiple -lactam antibiotics; (2) mutational loss of OprD porin, conferring resistance to imipenem; and (3) upregulation of the MexXY efux system (a member of the RND family), which exports uoroquinolones, tetracycline, aminoglycosides, and antipseudomonal -lactam agents.212 In general, multiple antibiotic resistance in gram-negative bacteria often starts with the relatively limited outer membrane permeability to many antibiotic agents, coupled with the overexpression of MDR efux pumps, which can export multiple unrelated antibiotics.213 In addition, by reducing the intracellular concentration of the antimicrobial agent to less than the MIC required for bacterial killing, efux mechanisms may allow bacterial survival for longer periods, facilitating the accumulation of new antibiotic-resistance mutations (e.g.,
AcrB
Inner membrane Figure 19-5 Proposed structural model for the multidrug resistance AcrAB-TolC efux pump in Escherichia coli. The AcrAB-TolC efux system is the most important resistance-nodulation-division (RND) transporter in E. coli and is composed of three interconnected elements: (1) the transmembrane AcrB transporter, which protrudes from the inner membrane into the periplasm; (2) the outer membrane channel TolC, which crosses from the periplasm through the outer membrane, providing the exit route for substrates into the extracellular medium; and (3) the AcrA periplasmic accessory protein, which stabilizes the complex. The pump recognizes a wide variety of substrates, including hydrophobic organic solvents and lipids as well as anionic, cationic, and zwitterionic antimicrobials, yielding a multidrug-resistant phenotype. (Adapted with permission from Lomovoskaya O, Zgurskaya HI, Totrov M, Watkins WJ. Waltzing transporters and the dance macabre between humans and bacteria. Nat Rev Drug Discov. 2007;6:56-65.)
292
PART I Basic Principles in the Diagnosis and Management of Infectious Diseases
additional antibiotic-resistant determinants. For example, analysis of a plasmid encoding the bla(CTX-15) gene responsible for resistance to extended-spectrum cephalosporins in an E. coli outbreak in Toronto revealed a large MDR region encoding multiple transposons and numerous other resistance genes, such as bla(OXA-1), bla(TEM-1), tetA, and aminoglycoside-resistance genes aac(6)Ib and aac(3)II.218 The ability of bacteria to capture multiple antibiotic resistance genes is further illustrated by resistance integrons, which can insert resistance gene cassettes into their attI integration site and are often found on transposons carried on plasmids, with seemingly endless recombinant potential.219
Kb
~44
Control of Antibiotic Resistance
Although the emergence of antibiotic-resistant bacteria has been correlated with the rise and fall of specic antibiotic use in clinical practice, the chain of causality is not always clear-cut.220,221 Bacterial strains contain complex aggregations of genes that may be linked together. The use of one antibiotic may select for the emergence of resistance to another. Mobile genetic elements and rapidly evolving integron cassettes with multiple antibiotic-resistance genes endow bacteria with a remarkable capacity to resist antibiotics.222 Although the development of antibiotic resistance may be inevitable, the rate at which it develops can be diminished by the rational use of antibiotics.29 The wider accessibility of computers and the ability to track antibiotic-resistance genes with molecular techniques have enhanced understanding and tracking of the spread of antibiotic resistance. With the appropriate computerized surveillance, a hospital laboratory may be able to detect rapidly the emergence of a new type of resistance or the presence of a new microbial strain within a specic unit or patient population. Techniques such as restriction endonuclease digestion analyses of microbial genomes and genetic probes of antibioticresistance genes by polymerase chain reaction (PCR) make it possible to conrm the presence of new genes in the environment. This information may be correlated with the phenotypic measures determined by the clinical microbiology surveillance system (Fig. 19-6). Use of molecular techniques greatly augments surveillance data, because large data sets can obscure subtle changes (miniepidemics) that may be more amenable to the institution of stringent infection control measures. Some bacterial strains have the ability to hypermutate in stressful environments, increasing the risk of acquisition of resistance mutations.223,224 Because prokaryotic organisms all contribute to a common gene pool, favorable genes mediating antibiotic resistance may disseminate among bacterial populations. In less than a decade, newly used and inexpensive drugs such as trimethoprim have gone from being highly effective in the treatment of dysentery in developing countries to becoming unusable in several of these areas.225 The emergence of other MDR organisms has had clinical signicance in the management of outpatient and nosocomial infections. Reports of VRSA in Japan and the United States suggest that common, invasive microbial pathogens may become refractory to any chemotherapeutic agent in the future.29 Rational policies for antibiotic usage suggest curtailment of the unnecessary use of antibiotics in situations such as animal husbandry. The causal link between the use of antibiotics for animal growth promotion and augmentation of resistance in human pathogens has been disputed,226 but more recent evi6.1 5.6
A
1 2 3 4 5 6
B
1 2 3 4 5 6
Figure 19-6 A, Agarose gel of EcoRI-digested plasmids derived from four isolates (lanes 1 through 4) that contain a nosocomial trimethoprimresistance plasmid (called pBWH10) from a Boston hospital. Another nosocomial plasmid from the same hospital that does not contain tri methoprim-resistance genes (lane 5) and one in which the trimethoprimresistance and sensitive plasmids are present in the same isolate (lane 6) are also shown. B, To demonstrate that the ngerprints from the trimethoprim-resistance plasmids in lanes 1 through 4 and lane 6 contain the same gene, DNADNA hybridization of the same six plasmids was performed using a type II dihydrofolate reductase probe. The probe and the restriction endonuclease analyses helped pinpoint the location and genetic homology of this trimethoprim-resistance gene.
dence is convincing that transfer of resistance genes occurs through the foods humans consume.227-229 New drug discoveries have allowed physicians to be one step ahead of the bacterial pathogens. Nonetheless, rapid evolution of resistance has limited the duration of the effectiveness of specic agents against certain pathogens. The best hope for the future is the development of a greater understanding of how antimicrobial resistance spreads, intelligent use and development of improved bacterial vaccines, and the implementation of effective infection control strategies.230 Newer antimicrobial agents have had a substantial impact in decreasing human morbidity and mortality rates over the past half-century. It behooves us to expand our surveillance of antibiotic-resistance determinants and to exercise caution in dispensing antibiotics to maximize their continued efcacy.
REFERENCES
1. Rice W, Chippindale A. Sexual recombination and the power of natural selection. Science. 2001;294:555-559. 2. Lupski JR. Molecular mechanisms for transposition of drugresistance genes and other movable genetic elements. Rev Infect Dis. 1987;9:357-368. 3. Medeiros AA. Evolution and dissemination of -lactamases accelerated by generations of -lactam antibiotics. Clin Infect Dis. 1997;24:S19-S45. 4. Gold HS, Moellering RC Jr. Antimicrobial-drug resistance. N Engl J Med. 1996;335:1445-1453. 5. Landman D, Bratu S, Kochar S, et al. Evolution of antimicrobial resistance among Pseudomonas aeruginosa, Acinetobacter baumannii, and Klebsiella pneumoniae in Brooklyn, NY. J Antimicrob Chemother. 2007;60:78-82. 6. Chang S, Sievert DM, Hageman JE, et al. Infection with vancomycin-resistant Staphylococcus aureus containing the vanA resistance gene. N Engl J Med. 2003;348:1342-1347. 7. Julian K, Kosowska-Shick K, Whitener C, et al. Characterization of a daptomycin-nonsusceptible vancomycin-intermediate Staphylococcus aureus strain in a patient with endocarditis. Antimicrob Agents Chemother. 2007;51:3445-3448 8. Galimand M, Guiyoule A, Gerbaud G, et al. Multidrug resistance in Yersinia pestis mediated by a transferable plasmid. N Engl J Med. 1997;337:677-680. 9. Tran JH, Jacoby GA. Mechanism of plasmid-mediated quinolone resistance. Proc Natl Acad Sci U S A. 2002;99:56385642. 10. Gardner P, Smith DH, Beer H, et al. Recovery of resistance factors from a drug-free community. Lancet. 1969;2:774-776. 11. Dantas G, Sommer MOA, Oluwasegun RD, et al. Bacteria subsisting on antibiotics. Science. 2008;320:100-103. 12. Cattoir V, Poirel L, Aubert C, et al. Unexpected occurrence of plasmid-mediated quinolone resistance determinants in environmental Aeromonas spp. Emerg Infect Dis. 2008;14:231-237. 13. Barlow M, Reik RA, Jacobs SD, et al. High rate of mobilization for blactx-mS. Emerg Infect Dis. 2008;14:423-428.
19 Molecular Mechanisms of Antibiotic Resistance in Bacteria
293
14. Massey RC, Buckling A, Peacock SJ. Phenotypic switching of antibiotic resistance circumvents permanent costs in Staphylococcus aureus. Curr Biol. 2001;11:1810-1814. 15. Summers AO, Wireman J, Vimy MJ, et al. Mercury released from dental silver llings provokes an increase in mercury-resistant and antibiotic-resistant bacteria in oral and intestinal oras of primates. Antimicrob Agents Chemother. 1993; 37:825-834. 16. Foster TJ. Plasmid-determined resistance to antimicrobial drugs and toxic metal ions in bacteria. Microbiol Rev. 1983;47:361-409. 17. Blattner FR, Plunkett G 3rd, Bloch CA, et al. The complete genome sequence of Escherichia coli K-12 (Comment). Science. 1997;277:1453-1474. 18. El Solh N, Allignet J, Bismuth R, et al. Conjugative transfer of staphylococcal antibiotic resistance markers in the absence of detectable plasmid DNA. Antimicrob Agents Chemother. 1986;30:161-169. 19. Salyers AA, Shoemaker NB, Stevens AM, et al. Conjugative transposons: An unusual and diverse set of integrated gene transfer elements. Microbiol Rev. 1985;49:679-690. 20. Morse SA, Johnson SR, Biddle JW, et al. High-level tetracycline resistance in Neisseria gonorrhoeae is result of acquisition of streptococcal tetM determinant. Antimicrob Agents Chemother. 1986;30:664-670. 21. Roberts MC, Kenny GE. Dissemination of the tetM tetracycline resistance determinant to Ureaplasma urealyticum. Antimicrob Agents Chemother. 1986;29:350-352. 22. Tato M, Coque TM, Ruiz-Garbajosa P, et al. Complex clonal and plasmid epidemiology in the rst outbreak of Enterobacteriaceae infection involving VIM-1 metallo--lactamase in Spain: Toward endemicity? Clin Infect Dis. 2007;45:1171-1178. 23. Arthur M, Reynolds P, Courvalin P. Glycopeptide resistance in enterococci. Trends Microbiol. 1996;4:401-407. 24. Brisson-Noel A, Arthur M, Courvalin P. Evidence for natural gene transfer from gram-positive cocci to Escherichia coli. J Bacteriol. 1988;170:1739-1745. 25. Papadopoulou B, Courvalin P. Dispersal in Campylobacter spp. of aphA-3, a kanamycin resistance determinant from grampositive cocci. Antimicrob Agents Chemother. 1988;32:945-948. 26. Courvalin P, Carlier C, Collatz E. Plasmid-mediated resistance to aminocyclitol antibiotics in group D streptococci. J Bacteriol. 1980;143:541-551. 27. Zscheck KK, Hull R, Murray BE. Restriction mapping and hybridization studies of a beta-lactamase-encoding fragment from Streptococcus (Enterococcus) faecalis. Antimicrob Agents Chemother. 1988;32:768-769. 28. Cohen ML. Epidemiology of drug resistance: Implications for a post-antimicrobial era. Science. 1992;257:1050-1055. 29. Levy SB. Antibiotic resistance: Consequences of inaction. Clin Infect Dis. 2001;3:S124-S129. 30. Hawkey PM. The origins and molecular basis of antibiotic resistance. BMJ. 1998;317:657-660. 31. Recchia GD, Hall RM. Origins of the mobile gene cassettes found in integrons. Trends Microbiol. 1997;5:389-394. 32. Stokes HW, Hall RM. A novel family of potentially mobile DNA elements encoding site-specic gene-integration functions: Integrons. Mol Microbiol. 1989;3:1669-1683. 33. Collis CM, Hall RM. Expression of antibiotic resistance genes in the integrated cassettes of integrons. Antimicrob Agents Chemother. 1995;39:155-162. 34. Ouellette M, Bissonnette L, Roy PH. Precise insertion of antibiotic resistance determinants into Tn21-like transposons: Nucleotide sequence of the OXA-1 beta-lactamase gene. Proc Natl Acad Sci U S A. 1987;84:7378-7382. 35. Paulsen IT, Littlejohn TG, Radstrom P, et al. The 3 conserved segment of integrons contains a gene associated with multidrug resistance to antiseptics and disinfectants. Antimicrob Agents Chemother. 1993;35:761-768. 36. Messier N, Roy PH. Integron integrases possess a unique additional domain necessary for activity. J Bacteriol. 2001; 183:6699-6706. 37. Hall MAL, Block HEM, Donders RT, et al. Multidrug resistance among enterobacteriaceae is strongly associated with the presence of integrons and is independent of species or isolate origin. J Infect Dis. 2003;187:251-259. 38. Recchia GD, Hall RM. Gene cassettes: A new class of mobile element. Microbiology. 1995;141:3015-3027. 39. Naas T, Mikami Y, Imai T, et al. Characterization of In53, a class 1 plasmid- and composite transposon-located integron of Escherichia coli which carries an unusual array of gene cassettes. J Bacteriol. 2001;183:235-249. 40. Fluit AC, Schmitz F-J. Resistance integrons and super-integrons. Clin Microbiol Infect. 2004;10:274-288. 41. Weldhagen GF. Integrons and beta-lactamases: A novel per spective on resistance. Int J Antimicrob Agents. 2004; 23:556-562. 41a. Ambler RP. The structure of -lactamases. Philos Trans R Soc Lond B Biol Sci. 1980;289:321-331. 42. Bush K, Jacoby GA, Medeiros AA. A functional classication scheme for -lactamases and its correlation with molecular structure. Antimicrob Agents Chemother. 1995;39:1211-1233. 43. Abraham EP, Chain E. An enzyme from bacteria able to destroy penicillin. Nature. 1940;1446:837. 44. Hawkey, PM. Molecular epidemiology of clinically signicant antibiotic resistance genes. Br J Pharmacol. 2008;153:S406S413.
45. Bradford, PA. Extended-spectrum beta-lactamases in the 21st century: Characterization, epidemiology, and detection of this important resistance threat. Clin Microbiol Rev. 2001; 14:933-951. 46. Brunton J, Clare D, Meier MA. Molecular epidemiology of antibiotic resistance plasmids of Haemophilus species and Neisseria gonorrheae. Rev Infect Dis. 1986;8:713-724 47. Babic M, Hujer AM, Bonomo RA. Whats new in antibiotic resistance? Focus on beta-lactamases. Drug Resist Updates. 2006;9:142-156 48. Knothe H, Shah P, Kremery V, et al. Transferable resistance to cefotaxime, cefoxitin, cefamandole and cefuroxime in clinical isolates of Klebsiella pneumoniae and Serratia marcescens. Infection. 1983;11:315-317 49. Philippon A, Labia R, Jacoby G. Extended-spectrum beta-lactamases. Antimicrob Agents Chemother. 1989;33:1131-1136. 50. Sougakoff W, Goussard S, Courvalin P. The TEM-3-lactamase, which hydrolyzes broad-spectrum cephalosporins, is derived from the TEM-2 penicillinase by two amino acid substitutions. FEMS Microbiol Lett. 1988;56:343348. 51. Lefon-Guibout V, Speldooren V, Heym B, et al. Epidemiological survey of amoxicillin-clavulanate resistance and corresponding molecular mechanisms in Escherichia coli isolates in France: New genetic features of blaTEM genes. Antimicrob. Agents Chemother. 2000;44:27092714. 52. Jacoby GA, Munoz-Price SL. The new beta-lactamases. N Engl J Med. 2005;352:380-391. 53. Poirel L, Kampfer P, Nordmann P. Chromosome-encoded Ambler class A beta-lactamase of Kluyvera georgiana, a probable progenitor of a subgroup of CTX-M extended-spectrum betalactamases. Antimicrob Agents Chemother. 2002;46:4038-4040. 54. Humeniuk C, Arlet G, Gautier V, et al. -Lactamases of Kluyvera ascorbata, probable progenitors of some plasmid-encoded CTX-M types. Antimicrob Agents Chemother. 2002; 46:3045-3049 55. Canton R, Coque TM. The CTX-M beta-lactamase pandemic. Curr Opin Microbiol. 2006;9:466-475. 56. Ben-Ami R, Schwaber MJ, Navon-Venezia S, et al. Inux of extended-spectrum -lactamase-producing Enterobacteriaceae into the hospital. Clin Infect Dis. 2006;42:925-934 57. Pitout JDD, Laupland KB. Extended-spectrum -lactamaseproducing Enterobacteriaceae: An emerging public-health concern. Lancet Infect Dis. 2008;8:159-166. 58. Livermore DM. Clinical signicance of beta-lactamase induction and stable derepression in gram-negative rods. Eur J Clin Microbiol. 1987;6:439-445. 59. Jones RN. Important and emerging beta-lactamase-mediated resistances in hospital-based pathogens: The Amp C enzymes. Diagn Microbiol Infect Dis. 1998;31:461-466. 60. Chow JW, Fine MJ, Shlaes DM, et al. Enterobacter bacteremia: Clinical features and emergence of antibiotic resistance during therapy. Ann Intern Med. 1991;115:585-590. 61. Bratu S, Landman D, Haag R, et al. Rapid spread of carbapenemresistant Klebsiella pneumoniae in New York City: A new threat to our antibiotic armamentarium. Arch Intern Med. 2005;165:1430. 62. Smith Moland E, Hanson ND, Herrera VL, et al. Plasmidmediated, carbapenem-hydrolysing beta-lactamase, KPC-2, in Klebsiella pneumoniae isolates. J Antimicrob Chemother. 2003;51:711. 63. Bradford PA, Bratu S, Urban C, et al. Emergence of carbapenem-resistant Klebsiella species possessing the class A carbapenem-hydrolyzing KPC-2 and inhibitor-resistant TEM-30 beta-lactamases in New York City. Clin Infect Dis. 2004;39:55-62. 64. Yigit H, Queenan AM, Anderson GJ, et al. Novel carbapenemhydrolyzing beta-lactamase, KPC-1, from a carbapenem-resistant strain of Klebsiella pneumoniae. Antimicrob Agents Chemother. 2008;52:809. 65. Walsh TR, Toleman MA, Poirel L, et al. Metallobeta-lactamases: The quiet before the storm? Clin Microbiol Rev. 2005;18 :305-325. 66. Walsh TR. The emergence and implications of metallo-lactamases in gram-negative bacteria. Clin Microbiol Infect. 2005;11(Suppl 6):2-9 67. Walther-Rasmussen J, Hoiby N. OXA-type carbapenemases. J Antimicrob Chemother. 2006;57:373-383. 68-72. References deleted. 73. Nord CE. Mechanisms of beta-lactam resistance in anaerobic bacteria. Rev Infect Dis. 1986;8(Suppl 5):S543-S548. 74. Appelbaum PC. Patterns of resistance and resistance mechanisms in anaerobes. Clin Microbiol Newslett. 1992;14:49-53. 75. Appelbaum PC, Spangler SK, Pankuch GA, et al. Characterization of a beta-lactamase from Clostridium clostridioforme. J Antimicrob Chemother. 1994;33:33-40. 76. Tuner K, Lindqvist L, Nord CE. Purication and properties of a novel beta-lactamase from Fusobacterium nucleatum. Antimicrob Agents Chemother. 1985;27:943-947. 77. Sanders CC, Sanders WE Jr, Goering RV. In vitro antagonism of beta-lactam antibiotics by cefoxitin. Antimicrob Agents Chemother. 1982;21:968-975. 78. Hedberg M, Edlund C, Lindqvist L, et al. Purication and characterization of an imipenem hydrolysing metallobeta-lactamase from Bacteroides fragilis. J Antimicrob Chemother. 1992;29:105-113. 79. Jacobs MR, Spangler SK, Appelbaum PC. Beta-lactamase production and susceptibility of US and European anaerobic gram-
negative bacilli to beta-lactams and other agents. Eur J Clin Microbiol Infect Dis. 1992;11:1081-1093. 80. Moxon ER, Medeiros AA, OBrien TF. Beta-lactamase effect on ampicillin treatment of Haemophilus inuenzae B bacteremia and meningitis in infant rats. Antimicrob Agents Chemother. 1977;12:461-464. 81. Rasheed JK, Jay C, Metchock B, et al. Evolution of extendedspectrum beta-lactam resistance (SHV-8) in a strain of Escherichia coli during multiple episodes of bacteremia. Antimicrob Agents Chemother. 1997;41:647-653. 82. Shimizu K, Kumada T, Hsieh WC, et al. Comparison of aminoglycoside resistance patterns in Japan, Formosa, and Korea, Chile, and the United States. Antimicrob Agents Chemother. 1985;28:282-288. 83. John JF Jr, Twitty JA. Plasmids as epidemiologic markers in nosocomial gram-negative bacilli: Experience at a university and review of the literature. Rev Infect Dis. 1986;8:693-704. 84. Barada K, Hanaki H, Ikeda S, et al. Trends in the gentamicin and arbekacin susceptibility of methicillin-resistant Staphylococcus aureus and the enzymes encoding aminocylcoside modiying enzymes. J Infect Chemother. 2007;13:74-78. 85. Mederski-Samoraj BD, Murray BE. High-level resistance to gentamicin in clinical isolates of enterococci. J Infect Dis. 1983;147:751-757. 86. Murray BE, Tsao J, Panida J. Enterococci from Bangkok, Thailand, with high-level resistance to currently available aminoglycosides. Antimicrob Agents Chemother. 1983;23:799802. 87. Zervos MJ, Kauffman CA, Therasse PM, et al. Nosocomial infection by gentamicin-resistant Streptococcus faecalis: An epidemiologic study. Ann Intern Med. 1987;106:687-691. 88. Hoffmann SA, Moellering RC Jr. The enterococcus: Putting the bug in our ears. Ann Intern Med. 1987;106:757-761. 89. Lyon BR, Skurray R. Antimicrobial resistance of Staphylococcus aureus: Genetic basis. Microbiol Rev. 1987;51:88-134. 90. Ichino K, Ishikawa J, Ikeda Y, et al. Characterization of a bifunctional aminoglycoside modifying enzyme with novel substrate specicity and its gene from a clinical isolate of methicillinresistant Staphylococcus aureus with high arbekacin resistance. J Antibiot. 2004;57:679-686. 91. Ardia N, Sareyyupoglu B, Ozyurt M, et al. Investigation of aminoglycoside modifying enzyme genes in methicillin-resistant staphylococci. Microbiol Res. 2006;161:49-56. 92. Robicsek A, Strahilevitz J, Jacoby EA, et al. Fluoroquinolonemodifying enzyme: A new adaptation of a common aminoglycoside acetyltransferase. Nat Med. 2006;12:83-88. 93. Gaffney DF, Foster TJ, Shaw WV. Chloramphenicol acetyl transferases determined by R-plasmids from gram negative bacteria. J Gen Microbiol. 1978;109:351-358. 94. Davies J. General mechanisms of antimicrobial resistance. Rev Infect Dis. 1979;1:23-29. 95. LeClercq R, Courvalin P. Resistance to macrolides, azalides, and streptogramins. In: Neu HC, Young LS, Zinner SH, eds. The New Macrolides, Azalides, and Streptogramins. New York: Marcel Dekker; 1993:33-40. 96. Andremont A, Gerbaud G, Courvalin P. Plasmid-mediated high level resistance to erythromycin in Escherichia coli. Antimicrob Agents Chemother. 1986;29:515-518. 97. Brisson-Noel A, Delrieu P, Samain D, et al. Inactivation of lincosamanide antibiotics in Staphylococcus: Identication of lincosaminide O-nucleotidyltransferases and comparison of the corresponding resistance genes. J Biol Chem. 1988; 263:15880-15887. 98. Le Gofc F, Capmau ML, Abbe J, et al. Plasmid-mediated pristinamycin resistance: PH1A, a pristinamycin 1A hydrolase. Ann Microbiol (Paris). 1977;128:471-474. 99. Allignet J, Loncle V, Mazodier P, et al. Nucleotide sequence of a staphylococcal plasmid gene, vgb, encoding a hydrolase inactivating the B components of virginiamycin-like antibiotics. Plasmid. 1988;20:271-275. 100. Speer BS, Bedzyj L, Salyers AA. Evidence that a novel tetracycline resistance gene found on two Bacteroides transposons encodes an NADPH-oxidoreductase. J Bacteriol. 1991; 173:176-183. 101. Fleming A. On the antibacterial action of cultures of a penicillium, with special reference to their use in the isolation of B. inuenzae. Br J Exp Pathol. 1929;10:226-236. 102. Nikaido H. Role of permeability barriers in resistance to betalactam antibiotics. Pharmacol Ther. 1985;27:197-231. 103. Labischinski H, Barnickel G, Bradaczek H, et al. High state of order of isolated bacterial lipopolysaccharide and its possible contribution to the permeation barrier property of the outer membrane. J Bacteriol. 1985;162:9-20. 104. Takeuchi Y, Nikaido H. Physical interaction between lipid A and phospholipids: A study with spin-labeled phospholipids. Rev Infect Dis. 1984;6:488-492. 105. Vaara M. Polymyxin B nonapeptide complexes with lipo polysaccharide [letter]. FEMS Microbiol Lett. 1983;18: 117-121. 106. Nikaido H, Vaara M. Molecular basis of bacterial outer membrane permeability. Microbiol Rev. 1985;49:1-32. 107. Hasegawa Y, Yamada H, Mizushima S. Interactions of outer membrane proteins 0-8 and 0-9 with peptidoglycan sacculus of Escherichia coli K-12. J Biochem (Tokyo). 1976;80:1401-1409. 108. Yoshimura F, Nikaido H. Diffusion of beta-lactam antibiotics through the porin channels of Escherichia coli K-12. Antimicrob Agents Chemother. 1985;27:84-92.
294
PART I Basic Principles in the Diagnosis and Management of Infectious Diseases
109. Goldstein FW, Gutmann L, Williamson R, et al. In vivo and in vitro emergence of simultaneous resistance to both beta-lactam and aminoglycoside antibiotics in a strain of Serratia marcescens. Ann Microbiol. 1983;134A:329-337. 110. Quinn JP, Dudek EJ, DiVincenzo CA, et al. Emergence of resistance to imipenem during therapy for Pseudomonas aeruginosa infections. J Infect Dis. 1986;154:289-293. 111. Carmeli Y, Troillet N, Eliopoulos GN, et al. Emergence of antibiotic-resistant Pseudomonas aeruginosa: Comparison of risks associated with different antipseudomonal agents. Antimicrob Agents Chemother. 1999;43:1379-1382 112. Bonomo RA, Szabo D. Mechanisms of multidrug resistance in Acinetobacter species and Pseudomonas aeruginosa. Clin Infect Dis. 2006;43:S49-S56. 113. Livermore DM. Interplay of impermeability and chromosomal beta-lactamase activity in imipenem-resistant Pseudomonas aeruginosa. Antimicrob Agents Chemother. 1992;36:2046-2048. 114. Sanders BC, Sanders WE Jr, Goering RV, et al. Selection of multiple antibiotic resistance by quinolones, beta-lactams, and aminoglycosides with special refercence to cross resistance between unrelated drug classes. Antimicrob Agents Chemother. 1984;306:797-801. 115. Hooper DC, Wolfson JS, Ng EY, et al. Mechanisms of action of and resistance to ciprooxacin. Am J Med. 1987;82:12-20. 116. Gaffney DF, Cundliffe E, Foster TJ. Chloramphenicol resistance that does not involve chloramphenicol acetyltransferase encoded by plasmids from gram-negative bacteria. J Gen Microbiol. 1981;125:113-121. 117. Bryan LE, Kwan S. Roles of ribosomal binding, membrane potential, and electron transport in bacterial uptake of streptomycin and gentamicin. Antimicrob Agents Chemother. 1983;23:835-845. 118. Mates SM, Eisenberg ES, Mandel LJ, et al. Membrane potential and gentamicin uptake in Staphylococcus aureus. Proc Natl Acad Sci U S A. 1982;79:6693-6697. 119. Rusthoven JJ, Davies TA, Lerner SA. Clinical isolation and characterization of aminoglycoside-resistant small colony variants of Enterobacter aerogenes. Am J Med. 1979;67:702-706. 120. Musher DM, Baughn RE, Merrell GL. Selection of small-colony variants of Enterobacteriaceae by in vitro exposure to aminoglycosides: Pathogenicity for experimental animals. J Infect Dis. 1979;140:209-214. 121. Funada H, Hattori KI, Kosakai N. Catalase-negative Escherichia coli isolated from blood. J Clin Microbiol. 1978;7:474-478. 122. Williams JB. Drug efux as a mechanism of resistance. Br J Biomed Sci. 1996;53:290-293. 123. McMurry L, Petrucci RE Jr, Levy SB. Active efux of tetracycline encoded by four genetically different tetracycline resistance determinants in Escherichia coli. Proc Natl Acad Sci U S A. 1980;77:3974-3977. 124. Levy SB, McMurry LM, Barbosa TM, et al. Nomenclature for new tetracycline resistance determinants. Antimicrob Agents Chemother. 1999;43:1523-1524. 125. Sutcliffe J, Tait-Kamradt A, Wandrack L. Streptococcus pneumoniae and Streptococcus pyogenes resistant to macrolide but sensitive to clindamycin: A common resistance pattern made by an efux system. Antimicrob Agents Chemother. 1996;40:1817-1824. 126. Leclercq R. Mechanisms of resistance to macrolides and lincosamides: Nature of the resistance elements and their clinical implications. Clin Infect Dis. 2002;34:482-492. 127. Clancy J, Dib-Hajj F, Petitpas JW, et al. Cloning and characterizatococcus tion of a novel macrolide efux gene, mreA, from Strep agalactiae. Antimicrob Agents Chemother. 1997;41:2719-2723. 128. Levy SB: Active efux, a common mechanism for biocide and antibiotic resistance. J Appl Microbiol. 2002;92(Suppl 1):65S71S. 129. Srikumar R, Li XZ, Poole K. Inner membrane efux components are responsible for -lactam specicity of multidrug efux pumps in Pseudomonas aeruginosa. J Bacteriol. 1997; 179:7875-7881. 130. Masuda N, Sakagawa E, Ohya S, et al. Contribution of the MexX-MexY-oprM efux system to intrinsic resistance in Pseudomonas aeruginosa. Antimicrob Agents Chemother. 2000; 44:2242-2246. 131. Ghosh AS, Ahamed J, Chauhan KK, et al. Involvement of an efux system in high-level uoroquinolone resistance of Shigella dysenteriae. Biochem Biophys Res Commun. 1998;242:54-56. 132. Cohen SP, Hooper DC, Wolfson JS, et al. Endogenous active efux of noroxacin in susceptible Escherichia coli. Antimicrob Agents Chemother. 1988;32:1187-1191. 133. Brown MH, Skurray RA: Staphylococcal multidrug efux protein QacA. J Mol Microbiol Biotechnol. 2001;3:163-170. 134. Corso, A, Severina, EP, Petruk, VF, et al. Molecular characterization of penicillin-resistant Streptococcus pneumoniae isolates causing respiratory disease in the United States. Microb Drug Resist. 1998;4:325. 135. Shortridge, VD, Doern, GV, Brueggemann, AB, et al. Prevalence of macrolide resistance mechanisms in Streptococcus pneumoniae isolates from a multicenter antibiotic resistance surveillance study conducted in the United States in 1994-1995. Clin Infect Dis. 1999;29:1186 136. Tait-Kamradt X, Davies T, Appelbaum PC, et al. Two new mechanisms of macrolide resistance in clinical strains of Streptococcus pneumoniae from Eastern Europe and North America. Antimicrob Agents Chemother. 2000;44:3395-3401. 137. Roberts, MC. Update on acquired tetracycline resistance genes.
FEMS Microbiol Lett. 2005;245:195-203 138. Trieber GA, Taylor DE. Mutations in the 16S rRNA genes of Helicobacter pylori mediate resistance to tetracycline. J Bacteriol. 2002;184:2131-2140. 139. Yamane K, Wachino J, Doi Y, et al. Global spread of aminoglycoside resistance genes. Emerg Infect Dis. 2005;11:951-953. 140. Eliopoulos GM, Farber BF, Murray BE, et al. Ribosomal resistance of clinical enterococcal isolates to streptomycin isolates. Antimicrob Agents Chemother. 1984;25:398-399. 141. Ahmad MH, Rechenmacher A, Bock A. Interaction between aminoglycoside uptake and ribosomal resistance mutations. Antimicrob Agents Chemother. 1980;18:798-806. 142. Hisanaga T, Hoban DJ, Zhanel GG. Mechanisms of resistance to telithromycin in Streptococcus pneumoniae. J Antimicrob Chemother. 2005;56:447-450. 143. Meka VG, Gold HS. Antimicrobial resistance to Linezolid. Clin Infect Dis. 2004;39 :1010-1015. 144. Kloss P, Xiong L, Shinabarger DL, et al. Resistance mutations in 23 S rRNA identify the site of action of the protein synthesis inhibitor linezolid in the ribosomal peptidyl transferase center. J Mol Biol. 1999;294:93-101 145. Raad II, Hanna HA, Hachem RY, et al. Clinical-use-associated decrease in susceptibility of vancomycin-resistant Enterococcus faecium to linezolid: A comparison with quinupristin-dalfopristin. Antimicrob Agents Chemother. 2004;48:3583-3585. 146. Dutka-Malen S, LeClercq R, Coutant V, et al. Phenotypic and genotypic heterogeneity of glycopeptide resistance determinants in gram-positive bacteria. Antimicrob Agents Chemother. 1990;34:1875-1879. 147. McKessar SJ, Barry AM, Bell JM, et al. Genetic characterization of vanG, a novel vancomycin resistance locus for Enterococcus faecalis. Antimicrob Agents Chemother. 2000;44:3224-3228. 148. LeClercq R, Derlot E, Weber M, et al. Transferable vancomycin and teicoplanin resistance in Enterococcus faecium. Antimicrob Agents Chemother. 1989;33:10-15. 149. Shlaes DM, Bouvet A, Devine C, et al. Inducible, transferable resistance to vancomycin in Enterococcus faecalis A256. Antimicrob Agents Chemother. 1989;33:198-203. 150. Centers for Disease Control and Prevention. Vancomycin-resistant Staphylococcus aureusPennsylvania, 2002. MMWR Morb Mortal Wkly Rep. 2002;51:902. 151. Nicas TI, Cole CT, Preston DA, et al. Activity of glycopeptides against vancomycin-resistant gram-positive bacteria. Antimicrob Agents Chemother. 1989;33:1477-1481. 152. Bugg TD, Wright GD, Dutka-Malen S, et al. Molecular basis for vancomycin resistance in Enterococcus faecium BM4147: Biosynthesis of a depsipeptide peptidoglycan precursor by vancomycin resistance proteins VanH and VanA. Biochemistry. 1991;30:10, 408-410, 415. 153. LeClercq R, Dutka-Malen S, Brissonnoel A, et al. Resistance of enterococci to aminoglycosides and glycopeptides. Clin Infect Dis. 1992;15:495-501. 154. Quintiliani R, Evers S, Courvalin P. The vanB gene confers various levels of self-transferable resistance to vancomycin in enterococci. J Infect Dis. 1993;167:1220-1223. 155. Fluit AC, Visser MR, Schmitz FJ. Molecular detection of antimicrobial resistance. Clin Microbiol Rev. 2001;14:836-871. 156. Schwalbe RS, Stapleton JT, Gilligan PH. Emergence of vancomycin resistance in coagulase-negative staphylococci. N Engl J Med. 1987;316:927-931. 157. Biavasco F, Vignaroli C, Lazzarini R, Varaldo PE. Glycopeptide susceptibility proles of Staphylococcus haemolyticus blood stream isolates. Antimicrob Agents Chemother. 2000; 44:3122-3126. 158. Centers for Disease Control and Prevention. Reduced susceptibility of Staphylococcus aureus to vancomycinJapan, 1996. MMWR Morb Mortal Wkly Rep. 1997;46:624-635. 159. Clark NC, Weigel LM, Patel JB, et al. Comparison of Tn1546-like elements in vancomycin-resistant Staphylococcus aureus isolates from Michigan and Pennsylvania. Antimicrob Agents Chemother. 2005;49:470-472 160. Courvalin P. Vancomycin resistance in gram-positive cocci. Clin Infect Dis. 2006;42(Suppl 1):S25-S34. 161. Geisel R, Schmitz FJ, Fluit AC, et al. Emergence, mechanism, and clinical implications of reduced glycopeptide susceptibility in Staphylococcus aureus. Eur J Clin Microbiol Infect Dis. 2001;20:685-697. 162. Cui L, Murakami H, Kuwahara-Arai K, et al. Contribution of a thickened cell wall and its glutamine nonamidated component to the vancomycin resistance expressed by Staphylococcus aureus M450. Antimicrob Agents Chemother. 2000;44:2276-2285. 163. Cui L, Iwamoto A, Lian JO, et al. Novel mechanism of antibitioc resistance originating in vancomycin-intermediate Staphylococcus aureus. Antimicrob Agents Chemother. 2006;50:428-438. 164. Hospital Infection Control Practices Advisory Committee (HICPAC). Recommendations for preventing the spread of vancomycin resistance. Infect Control Hosp Epidemiol. 1995;16:105-113. 165. Waxman DJ, Strominger JL. Penicillin-binding proteins and the mechanism of action of beta-lactam antibiotics. Ann Rev Biochem. 1983;52:825-869. 166. Malouin F, Bryan LE. Modication of penicillin-binding proteins as mechanisms of beta-lactam resistance. Antimicrob Agents Chemother. 1986;30:1-5. 167. Williamson R. Resistance of Clostridium perfringens to betalactam antibiotics mediated by a decreased afnity of a single essential penicillin-binding protein. J Gen Microbiol. 1983;
129:2339-2342. 168. Giles AF, Reynolds RE. Bacillus megaterium resistance to cloxacillin accompanied by a compensatory change in penicillin binding proteins. Nature. 1979;280:167-168. 169. Hakenbeck R, Tarpay M, Tomasz A. Multiple changes of penicillin-binding proteins in penicillin-resistant clinical isolates of Streptococcus pneumoniae. Antimicrob Agents Chemother. 1980;17:364-371. 170. Spratt BG, Dowson CG, Zhang Q-Y, et al. Mosaic genes, hybrid penicillin-binding proteins, and the origins of penicillin resistance in Neisseria meningitidis and Streptococcus pneumoniae. In: Pardee A, Campisi J, eds. Perspectives on Cellular Regulation: From Bacteria to Cancer. New York: Wiley-Liss; 1991:73-83. 171. Hartman BJ, Tomasz A. Low-afnity penicillin-binding protein associated with beta-lactam resistance in Staphylococcus aureus. J Bacteriol. 1984;158:513-516. 172. Ubukata K, Yamashita N, Konno M. Occurrence of a betalactam-inducible penicillin-binding protein in methicillinresistant staphylococci. Antimicrob Agents Chemother. 1985; 27:851-857. 173. Fontana R. Penicillin-binding proteins and the intrinsic resistance to beta-lactams in gram-positive cocci. J Antimicrob Chemother. 1985;16:412-416. 174. Fontana R, Grossato A, Rossi L, et al. Transition from resistance to hypersusceptibility to beta-lactam antibiotics associated with loss of a low-afnity penicillin-binding protein in a Streptococcus faecium mutant highly resistant to penicillin. Antimicrob Agents Chemother. 1985;28:678-683. 175. Farber BF, Eliopoulos GM, Ward JI, et al. Multiply resistant viridans streptococci: Susceptibility to beta-lactam antibiotics and comparison of penicillin-binding protein patterns. Antimicrob Agents Chemother. 1983;24:702-705. 176. Lambert PA. Bacterial resistance to antibiotics: Modied target sites. Adv Drug Deliv Rev. 2005;57:1471-1485. 177. Sabath LD. Chemical and physical factors inuencing methicillin resistance of Staphylococcus aureus and Staphylococcus epidermidis. J Antimicrob Chemother. 1977;3(Suppl C):47-51. 178. Song MD, Wachi M, Doi M, et al. Evolution of an inducible penicillin-target protein in methicillin-resistant Staphylococcus aureus by gene fusion. FEBS Lett. 1987;221:167-171. 179. Berger-Bachi B, Barberis-Maino L, Strassle A, et al. FemA, a host-mediated factor essential for methicillin resistance in Staphylococcus aureus: Molecular cloning and characterization. Mol Gen Genet. 1989;219:263-269. 180. Dougherty TJ, Koller AE, Tomasz A. Penicillin-binding proteins of penicillin-susceptible and intrinsically resistant Neisseria gonorrhoeae. Antimicrob Agents Chemother. 1980;18:730737. 181. Mendelman PM, Chafn DO, Kalaitzoglou G. Penicillin-binding proteins and ampicillin resistance in Haemophilus inuenzae. J Antimicrob Chemother. 1990;25:525-534. 182. Dougherty TJ. Genetic analysis and penicillin-binding protein alterations in Neisseria gonorrhoeae with chromosomally mediated resistance. Antimicrob Agents Chemother. 1986; 30:649-652. 183. Mendelman PM, Campos J, Chafn DO, et al. Relative penicillin G resistance in Neisseria meningitidis and reduced afnity of penicillin-binding protein 3. Antimicrob Agents Chemother. 1988;32:706-709. 184. Spratt BG, Zhang Q-Y, Jones DM, et al. Recruitment of a penicillin-binding protein gene from Neisseria avescens during the emergence of penicillin resistance in Neisseria meningitidis. Proc Natl Acad Sci U S A. 1989;86:8988-8992. 185. Faruki H, Kohmescher RN, McKinney WP, et al. A communitybased outbreak of infection with penicillin-resistant Neisseria gonorrhoeae not producing penicillinase (chromosomally mediated resistance). N Engl J Med. 1985;313:607-611. 186. Mirelman D, Nuchamowitz Y, Rubinstein E. Insensitivity of peptidoglycan biosynthetic reactions to beta-lactam antibiotics in a clinical isolate of Pseudomonas aeruginosa. Antimicrob Agents Chemother. 1981;19:687-695. 187. Parr TR Jr, Bryan LE. Mechanism of resistance of an ampicillinresistant, beta-lactamase-negative clinical isolate of Haemophilus inuenzae type b to beta-lactam antibiotics. Antimicrob Agents Chemother. 1984;25:747-753. 188. Wolfson JS, Hooper DC. The uoroquinolones: Structures, mechanisms of action and resistance, and spectra of activity in vitro. Antimicrob Agents Chemother. 1985;28:581-586. 189. Hane MW, Wood TH. Escherichia coli K-12 mutants resistant to nalidixic acid: Genetic mapping and dominance studies. J Bacteriol. 1969;99:238-241. 190. Robillard NJ, Scarpa AL. Genetic and physiological characterization of ciprooxacin resistance in Pseudomonas aeruginosa PAO. Antimicrob Agents Chemother. 1988;32:535-539. 191. Schmitz FJ, Higgins P, Meyer S, et al. Activity of quinolones against gram-positive cocci: mechanisms of drug action and bacterial resistance. Eur J Clin Microbiol Infect Dis. 2002;21:647-659. 192. Schmitz FJ, Jones ME, Hofmann B, et al. Characterization of grlA, grlB, gyrA and gyrB mutations in 116 unrelated isolates of Staphylococcus aureus in relation to minimal inhibitory concentrations of ciprooxacin. Antimicrob Agents Chemother. 1998;42:1249-1252. 193. Aoyama H, Fujimaki K, Sato K, et al. Clinical isolate of Citrobacter freundii highly resistant to new quinolones. Antimicrob Agents Chemother. 1988;32:922-924. 194. Martinez-Martinez L, Pascual A, Jacoby GA. Quinolone resis-
19 Molecular Mechanisms of Antibiotic Resistance in Bacteria
295
tance from a transferable plasmid. Lancet. 1998;351:797-799. 195. Nakamura S, Nakamura M, Kojima T, et al. gyrA and gyrB mutations in quinolone-resistant strains of Escherichia coli. Antimicrob Agents Chemother. 1989;33:254-255. 196. Cullen ME, Wyke AW, Kuroda R, et al. Cloning and characterization of a DNA gyrase A gene from Escherichia coli that confers clinical resistance to 4-quinolones. Antimicrob Agents Chemother. 1989;33:886-894. 197. Enne VI, King A, Livermore DM, et al. Sulfonamide resistance in Haemophilus inuenzae mediated by acquisition of sul2 or a short insertion in chromosomal folP. Antimicrob Agents Chemother. 2002;46:1934-1939. 198. Huovinen P. Trimethoprim resistance. Antimicrob Agents Chemother. 1987;31:1451-1456. 199. Steen R, Skold O. Plasmid-borne or chromosomally mediated resistance by Tn7 is the most common response to ubiquitous use of trimethoprim. Antimicrob Agents Chemother. 1985;27: 933-937. 200. Maskell R, Okubadejo OA, Payne RH, et al. Human infections with thymine-requiring bacteria. J Med Microbiol. 1978;11:33-45. 201. Zhu W, Tenover FC, Limor J, et al. Use of pyrosequencing to identify point mutations in domain V of 23S rRNA genes of linezolid-resistant Staphylococcus aureus and Staphylococcus epidermidis. Eur J Clin Microbiol Infect Dis. 2006;26:161-165. 202. Escribano I, Rodrguez JC, Llorca B, et al. Importance of the efux pump systems in the resistance of Mycobacterium tuberculosis to uoroquinolones and linezolid. Chemotherapy. 2007;53:397-401. 203. Campos MA, Vargas MA, Regueiro V, et al. Capsule polysaccharide mediates bacterial resistance to antimicrobial peptides. Infect Immun. 2004;72:7107-7114. 204. Kwon DH, Lu CD. Polyamines induce resistance to cationic peptide, aminoglycoside, and quinolone antibiotics in Pseudomonas aeruginosa PAO1. Antimicrob Agents Chemother. 2006;50:1615-1622. 205. Longzhu C, Tominaga E, Neoh H, et al. Correlation between reduced daptomycin susceptibility and vancomycin resistance in vancomycin-intermediate Staphylococcus aureus. Antimicrob Agents Chemother. 2006;50:1079-1082. 206. Sakoulas G, Alder J, Thauvin-Eliopoulos C, et al. Induction of
207. 208. 209.
210. 211. 212. 213. 214. 215. 216. 217. 218.
daptomycin heterogeneous susceptibility in Staphylococcus aureus by exposure to vancomycin. Antimicrob Agents Chemother. 2006;50:1581-1585. Friedman L, Alder JD, Silverman JA. Genetic changes that correlate with reduced susceptibility to daptomycin in Staphylococcus aureus. Antimicrob Agents Chemother. 2006;50:2137-2145. Iredell J, Thomas L, Power D, et al. Tigecycline resistance in Australian antibiotic-resistant gram-negative bacteria. J Antimicrob Chemother. 2007;59:816-818. McAleese F, Petersen P, Ruzin A, et al. A novel MATE family efux pump contributes to the reduced susceptibility of laboratory-derived Staphylococcus aureus mutants to tigecycline. Antimicrob Agents Chemother. 2005;49:1865-1871. Peleg AY, Potoski BA, Rea R, et al. Acinetobacter baumannii bloodstream infection while receiving tigecycline: A cautionary report. J Antimicrob Chemother. 2007;59:128-131. van der Wouden EJ, Thijs JC, Kusters JG, et al. Mechanism and clinical signicance of metronidazole resistance in Helicobacter pylori. Scand J Gastroenterol Suppl. 2001;(234):10-14. Deplano A, Denis O, Poirel L, et al. Molecular characterization of an epidemic clone of panantibiotic-resistant Pseudomonas aeruginosa. J Clin Microbiol. 2005;43:1198-2004. Poole K. Outer membranes and efux: The path to multidrug resistance in gram-negative bacteria. Curr Pharm Biotechnol. 2002;3:77-98. Piddock L. Clinically relevant chromosomally encoded multidrug resistance efux pumps in bacteria. Clin Microbiol Rev. 2006;19:382-402. Lin J, Sahin O, Michael LO, et al. Critical role of multidrug efux pump CmeABC in bile resistance and in vivo colonization of Campylobacter jejuni. Infect Immun. 2003;71:4250-4259. Hirakata Y, Srikumar R, Poole K, et al. Multidrug efux systems play an important role in the invasiveness of Pseudomonas aeruginosa. J Exp Med. 2002;196:109-118. Rice, LB. Tn916 family conjugative transposons and dissemination of antimicrobial resistance determinants. Antimicrob Agent Chemother. 1998;42:1871-1877. Boyd DA, Tyler S, Christianson S, et al. Complete nucleotide sequence of a 92-kilobase plasmid harboring the CTX-15 extended-spectrum beta-lactamase involved in an outbreak in long-term-care facililites in Toronto, Canada. Antimicrob Agents
Chemother. 2004;48:3758-3764 219. Bennet PM. Plasmid encoded antibiotic resistance: Acquisition and transfer of antibiotic resistance genes in bacteria. Br J Pharmacol. 2008;153:S347-S357. 220. Whitney CG, Farley MM, Hadler J, et al. Increasing prevalence of multidrug-resistant Streptococcus pneumoniae in the United States. N Engl J Med. 2000;343:1917-1924. 221. Hogan D, Kolter R. Why are bacteria refractory to antimicrobials? Curr Opin Microbiol. 2002;5:472-477. 222. Partridge SR, Brown HJ, Hall RM. Characterization and movement of the class I integron known as Tn2521 and Tn1405. Antimicrob Agents Chemother. 2002;46:1288-1294. 223. Rainey PB, Moxon ER. When being hyper keeps you t. Science. 2000;288:1186-1187. 224. Tompkins JD, Nelson JL, Hazel JC, et al. Error-prone polymerase, DNA polymerase IV, is responsible for transient hypermutation during adaptive mutation in Escherichia coli. J Bacteriol. 2003;185:3469-3472. 225. Murray BE, Alvarado T, Kim KH, et al. Increasing resistance to trimethoprim-sulfamethoxazole among isolates of Escherichia coli in developing countries. J Infect Dis. 1985;152:1107-1113. 226. Banerjee SN, Emori TG, Culver DH, et al. Secular trends in nosocomial primary bloodstream infections in the United States, 1980-1989. National Nosocomial Infections Surveillance System. Am J Med. 1991;91:86S-89S. 227. White DG, Shao S, Sudler R, et al. The isolation of antibioticresistant Salmonella from retail ground meats. N Engl J Med. 2001;345:1147-1154. 228. Srenson TL, Blom M, Monnet DL, et al. Transient intestinal carriage after ingestion of antibiotic-resistant Enterococcus faecium from chicken and pork. N Engl J Med. 2001;345:1161-1166. 229. McDonald LC, Rossiter S, Mackinson C, et al. Quinupristindalfopristin-resistant Enterococcus faecium on chicken and in human stool specimens. N Engl J Med. 2001;345:1155-1160. 230. McGowan JE Jr, Tenover FC. Control of antimicrobial resistance in the health care system. Infect Dis Clin North Am. 1997;11:297-311.
You might also like
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The Mitochondrion - A Trojan Horse That Kicks Off InflammationDocument3 pagesThe Mitochondrion - A Trojan Horse That Kicks Off InflammationEduardo P. BarajasNo ratings yet
- Fisiopatología de La Pre-EclamsiaDocument15 pagesFisiopatología de La Pre-EclamsiaJosue Jimenez VargasNo ratings yet
- The Cell-Based Model of CoagulationDocument8 pagesThe Cell-Based Model of CoagulationJuan Francisco100% (1)
- Failure Differentiation Mano IIDocument19 pagesFailure Differentiation Mano IIEduardo P. BarajasNo ratings yet
- ABC of Clinical HematologyDocument82 pagesABC of Clinical Hematologydokice100% (1)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Nature Magazine 7170 - 2007-11-29Document189 pagesNature Magazine 7170 - 2007-11-29Roberto KlesNo ratings yet
- Mobile Genetic Elements and TransposonsDocument106 pagesMobile Genetic Elements and TransposonsPandit JiNo ratings yet
- BP605T Unit 4-6Document482 pagesBP605T Unit 4-6Gyampoh SolomonNo ratings yet
- Gene Transfer Questions-2021Document4 pagesGene Transfer Questions-2021Kaif AliNo ratings yet
- Source Document Controls ValidationDocument18 pagesSource Document Controls ValidationCarla Jean CuyosNo ratings yet
- The Role of Chromosomal Change in Plant Evolution PDFDocument241 pagesThe Role of Chromosomal Change in Plant Evolution PDFFabio SantosNo ratings yet
- Sleeping Beauty Transposon: System User ManualDocument7 pagesSleeping Beauty Transposon: System User ManualNicole AbiNo ratings yet
- Behavior Genetics and Postgenomics PDFDocument84 pagesBehavior Genetics and Postgenomics PDFvkarmoNo ratings yet
- Melt ManualDocument32 pagesMelt ManualSaikat ChakrabortyNo ratings yet
- Codon Populations in Single-Stranded Whole Human Genome DNA Are Fractal and Fine-Tuned by The Golden Ratio 1.618Document13 pagesCodon Populations in Single-Stranded Whole Human Genome DNA Are Fractal and Fine-Tuned by The Golden Ratio 1.618Jean-claude PerezNo ratings yet
- Brown Et Al. 2009 Tribolium A Model For Developmental and Pest BiologyDocument9 pagesBrown Et Al. 2009 Tribolium A Model For Developmental and Pest BiologyAneel Nizar AliNo ratings yet
- Bailey Scotts Diagnostic Microbiology 13th Tille Test BankDocument9 pagesBailey Scotts Diagnostic Microbiology 13th Tille Test BankRamiqqNo ratings yet
- Biology Exam Notes by ConstantinDocument120 pagesBiology Exam Notes by ConstantinbnvjNo ratings yet
- Molecular Evolution: Genetic Change and Innovations: Alberts (2015) Molecular Biology Edition, Figure 1-19Document38 pagesMolecular Evolution: Genetic Change and Innovations: Alberts (2015) Molecular Biology Edition, Figure 1-19anon_695632385No ratings yet
- The C-Value Paradox, Junk DNA, and ENCODEDocument6 pagesThe C-Value Paradox, Junk DNA, and ENCODEMartina RajnovicNo ratings yet
- Origin of VirusesDocument11 pagesOrigin of VirusesKyle Uy100% (3)
- Basic Cell and Molecular Biology 4e - What We Know and How Found ODocument629 pagesBasic Cell and Molecular Biology 4e - What We Know and How Found Oмакс100% (1)
- Human Molecular Genetics, 4th Edition PDFDocument704 pagesHuman Molecular Genetics, 4th Edition PDFLi Luo100% (5)
- M.SC Biochem Semester Pattern With Scheme Final NAGPUR UNIVERSITYDocument27 pagesM.SC Biochem Semester Pattern With Scheme Final NAGPUR UNIVERSITYupendramolmedNo ratings yet
- DNA Monthly Vol 1 No 6 NovDec05Document16 pagesDNA Monthly Vol 1 No 6 NovDec05piboNo ratings yet
- Gerald Crabtree - Trends in Genetics. Our Fragile IntellectDocument6 pagesGerald Crabtree - Trends in Genetics. Our Fragile IntellectDemocracia real YA100% (1)
- Chapter 7Document40 pagesChapter 7NurulJannah ARNo ratings yet
- Chapter 21 Genomes and Their EvolutionDocument8 pagesChapter 21 Genomes and Their Evolution蔡旻珊No ratings yet
- Dhiraj Kumar, Chengliang Gong-Trends in Insect Molecular Biology and Biotechnology-Springer International Publishing (2018) PDFDocument376 pagesDhiraj Kumar, Chengliang Gong-Trends in Insect Molecular Biology and Biotechnology-Springer International Publishing (2018) PDFAndres Felipe Arias MosqueraNo ratings yet
- Dna ST N FXNDocument11 pagesDna ST N FXNJyoti JoshiNo ratings yet
- Principles of Population GeneticsDocument7 pagesPrinciples of Population GeneticsGiulia Magri RibeiroNo ratings yet
- Cell 100806Document188 pagesCell 100806PrasathNo ratings yet
- MSC Genetics SyllabusDocument36 pagesMSC Genetics SyllabusMohak SahuNo ratings yet
- Chapter 18 AP Bio Study GuideDocument6 pagesChapter 18 AP Bio Study GuideHolly SullivanNo ratings yet
- Genetics: Analysis of Genes and Genomes, Ninth Edition: Includes Navigate 2 Advantage AccessDocument7 pagesGenetics: Analysis of Genes and Genomes, Ninth Edition: Includes Navigate 2 Advantage AccessVims BatchNo ratings yet