You might also like
- Drug ListsDocument10 pagesDrug ListsAmber Merritt100% (1)
- Top 300 Drugs Pocket Reference Guide (2021 Edition)From EverandTop 300 Drugs Pocket Reference Guide (2021 Edition)Rating: 5 out of 5 stars5/5 (1)
- Naplex MpjeDocument35 pagesNaplex MpjeAtlantis ManNo ratings yet
- Naplex NotesDocument226 pagesNaplex NotesløzanNo ratings yet
- Total Pharmacy Notes TPN For EEDocument1,601 pagesTotal Pharmacy Notes TPN For EEClaire Cura100% (2)
- 2006 Info For MpjeDocument28 pages2006 Info For Mpjemina75% (4)
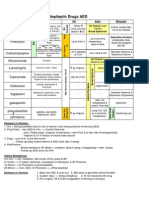
- Antiepileptic Drugs AED: D' DI Disadv SE AdvDocument1 pageAntiepileptic Drugs AED: D' DI Disadv SE Advrayooona88No ratings yet
- Pharmacy Operations: Licensure, Registration and CertifiacationsDocument5 pagesPharmacy Operations: Licensure, Registration and CertifiacationsHitomi Shiroshita100% (1)
- R: K D, M, S T: Xprep EY Rugs Nemonics Tudy IPSDocument18 pagesR: K D, M, S T: Xprep EY Rugs Nemonics Tudy IPSKNo ratings yet
- Pharmacy Laws, Medicare, Medicaid and Business Management: Copy Right ProtectedDocument8 pagesPharmacy Laws, Medicare, Medicaid and Business Management: Copy Right Protectedasas100% (1)
- @ Drug Antibiotics AntifungalDocument57 pages@ Drug Antibiotics AntifungalDr. Anil Virani SurgeonNo ratings yet
- Pedia Stickers PDFDocument8 pagesPedia Stickers PDFAshNo ratings yet
- OTC Exam 2 Study GuideDocument32 pagesOTC Exam 2 Study GuideDave WinNo ratings yet
- All Other ClassificationsDocument6 pagesAll Other ClassificationsCorey100% (1)
- IV PO Conversion CAPDocument3 pagesIV PO Conversion CAPdamondouglasNo ratings yet
- Brand Generic Class Other: NAPLEX ReviewDocument72 pagesBrand Generic Class Other: NAPLEX Reviewbapimirab654No ratings yet
- Over The Counter Drug ListDocument5 pagesOver The Counter Drug Listpradip_26No ratings yet
- Infectious Diseases IDocument7 pagesInfectious Diseases ITiff VoNo ratings yet
- Top 200 Drug ExamDocument1 pageTop 200 Drug ExamUyen V. NguyenNo ratings yet
- RX Cheat Sheet Pharmacy CrackDocument1 pageRX Cheat Sheet Pharmacy Crackramesh kumar100% (1)
- Drug of Choice and First Line of TreatmentDocument2 pagesDrug of Choice and First Line of Treatmentprinz1mendezNo ratings yet
- Chapter 35 AsthmaDocument4 pagesChapter 35 AsthmaDrashtibahen PatelNo ratings yet
- RxprepDocument1 pageRxprepSandeep KannegantiNo ratings yet
- Top Drugs: 1. ACETAMINOPHEN (Tylenol)Document12 pagesTop Drugs: 1. ACETAMINOPHEN (Tylenol)epingNo ratings yet
- Math Formulas For NAPLEX CalculationsDocument1 pageMath Formulas For NAPLEX CalculationsNasru DiinNo ratings yet
- Antipsychotics Factsheet pg2Document1 pageAntipsychotics Factsheet pg2JUSASBNo ratings yet
- Comprehensive Pharmacology SummaryDocument25 pagesComprehensive Pharmacology Summarysubash p100% (1)
- Naplex StudyDocument1 pageNaplex StudyMaxwell Bentley LeeNo ratings yet
- Study GuideDocument6 pagesStudy GuideFidelis MusicGroupNo ratings yet
- Insulin Chart: Insulin Type Onset of Action Peak Duration of ActionDocument1 pageInsulin Chart: Insulin Type Onset of Action Peak Duration of ActionGeorge ZachariahNo ratings yet
- Brad Hinton CVDocument6 pagesBrad Hinton CVapi-486072801No ratings yet
- Chapter 28 Infections: Perioperative Antimicrobial PPXDocument10 pagesChapter 28 Infections: Perioperative Antimicrobial PPXDrashtibahen PatelNo ratings yet
- Confused Drug Names-IsMPDocument9 pagesConfused Drug Names-IsMPPria Utama100% (1)
- Pharmacy Law Final Exam ReviewDocument3 pagesPharmacy Law Final Exam Reviewtiffanievo05100% (1)
- OtcDocument9 pagesOtcChrissie100% (1)
- Hypertension Drugs Cheat Sheet: by ViaDocument3 pagesHypertension Drugs Cheat Sheet: by ViaGulzaib KhokharNo ratings yet
- Know Common Disease ManagementDocument14 pagesKnow Common Disease Managementcdx25No ratings yet
- Drug TerminologyDocument5 pagesDrug Terminologyimdaking123No ratings yet
- 2017 Comprehensive ReviewDocument26 pages2017 Comprehensive Reviewapi-364961432100% (2)
- TPN CalculationDocument3 pagesTPN CalculationSARANYANo ratings yet
- Pharm Drug ListDocument17 pagesPharm Drug Listanon_523534678No ratings yet
- What 2 StudyDocument2 pagesWhat 2 StudyWil Lester100% (1)
- NAPLEXDocument1 pageNAPLEXbaniyo100% (1)
- Drug Side EffectsDocument2 pagesDrug Side EffectsAngelic khanNo ratings yet
- Naplex 1Document7 pagesNaplex 1baniyoNo ratings yet
- Apc0271 V4 PDFDocument53 pagesApc0271 V4 PDFDrAnisha PatelNo ratings yet
- Naplex - Math FormulasDocument1 pageNaplex - Math FormulasbooseeyNo ratings yet
- NJ Mpje PDFDocument168 pagesNJ Mpje PDFPatrick Mata100% (3)
- PK Equations To Know For NaplexDocument1 pagePK Equations To Know For NaplexNasru DiinNo ratings yet
- Pharmacist ChartDocument17 pagesPharmacist Chartrajnar1962100% (1)
- 2017 April Exam CompilationDocument8 pages2017 April Exam CompilationabbasyaqobiNo ratings yet
- Quizlet PractiDocument21 pagesQuizlet Practitohomas100% (1)
- Pharmacology Drug ChartDocument50 pagesPharmacology Drug ChartEssentialForLivingNo ratings yet
- Multistate Pharmacy Jurisprudence Examination (MPJE) Study GuideDocument20 pagesMultistate Pharmacy Jurisprudence Examination (MPJE) Study GuideMcRee Learning Center100% (2)
- Antibiotic PrescribingDocument1 pageAntibiotic PrescribingJay KayNo ratings yet
- Comprehensive - Pharmacy Review For NAPLEX Practice Exams Cases and Test Prep.8thDocument63 pagesComprehensive - Pharmacy Review For NAPLEX Practice Exams Cases and Test Prep.8thRabie YahfoufiNo ratings yet
- MULTISTATE PHARMACY JURISPRUDENCE EXAMINATION (MPJE): Passbooks Study GuideFrom EverandMULTISTATE PHARMACY JURISPRUDENCE EXAMINATION (MPJE): Passbooks Study GuideNo ratings yet
- Naplex Complete Study Outline A Topic-Wise Approach DiabetesFrom EverandNaplex Complete Study Outline A Topic-Wise Approach DiabetesRating: 4 out of 5 stars4/5 (2)
- Vitamin Toxicities: NeonatalDocument29 pagesVitamin Toxicities: NeonatalfarazNo ratings yet
- Preview of Pharmacist OSCE Review BookDocument45 pagesPreview of Pharmacist OSCE Review BookChrissie100% (3)
- Pharmacy CounsellingDocument8 pagesPharmacy CounsellingChrissieNo ratings yet
- Practice Osce Scenarios PDFDocument20 pagesPractice Osce Scenarios PDFa1docNo ratings yet
- OtcDocument9 pagesOtcChrissie100% (1)
- Pharmacy Service AgreementDocument164 pagesPharmacy Service AgreementChrissieNo ratings yet
- Look Under Drugs Affecting Nutritional and Metbolic FunctionDocument1 pageLook Under Drugs Affecting Nutritional and Metbolic FunctionChrissieNo ratings yet
- Drug InteractionDocument1 pageDrug InteractionChrissieNo ratings yet
- Writing Task 1Document9 pagesWriting Task 1ChrissieNo ratings yet
- Glyceryltrinitrate: Cardiovascular PharmacologyDocument1 pageGlyceryltrinitrate: Cardiovascular PharmacologyChrissieNo ratings yet
- Processing PrescriptionsDocument24 pagesProcessing PrescriptionsChrissieNo ratings yet
- MdsMgtModule Calculations FinalDocument35 pagesMdsMgtModule Calculations FinalChrissieNo ratings yet
- Differentiating Language Difference and Language Disorder - Information For Teachers Working With English Language Learners in The Schools PDFDocument23 pagesDifferentiating Language Difference and Language Disorder - Information For Teachers Working With English Language Learners in The Schools PDFIqra HassanNo ratings yet
- This Study Resource Was: MCV4U Exam ReviewDocument9 pagesThis Study Resource Was: MCV4U Exam ReviewNathan WaltonNo ratings yet
- Jo - Mc.Donough. ESP in Perspective A Practical Guide. London. Collin ELT. 1984. p.3Document6 pagesJo - Mc.Donough. ESP in Perspective A Practical Guide. London. Collin ELT. 1984. p.3Falihatul Kholidiyah100% (1)
- Device InfoDocument3 pagesDevice InfoGrig TeoNo ratings yet
- Ielts Reading Actual Tests With Suggested Answers Oct 2021 JDocument508 pagesIelts Reading Actual Tests With Suggested Answers Oct 2021 JHarpreet Singh JohalNo ratings yet
- GTAG-14 Edited With Ad 05-20-20101 PDFDocument32 pagesGTAG-14 Edited With Ad 05-20-20101 PDFpiornelNo ratings yet
- Month Puzzle Two VariableDocument6 pagesMonth Puzzle Two VariableNayan KaithwasNo ratings yet
- Lecture Planner - Chemistry - MANZIL For JEE 2024Document1 pageLecture Planner - Chemistry - MANZIL For JEE 2024Rishi NairNo ratings yet
- Bach Polonaise G Min BWV 119 A4Document1 pageBach Polonaise G Min BWV 119 A4vincenzovaiaNo ratings yet
- CIT 811 TMA 4 Quiz QuestionDocument3 pagesCIT 811 TMA 4 Quiz QuestionjohnNo ratings yet
- Structural Engineering Formulas Second EditionDocument224 pagesStructural Engineering Formulas Second Editionahmed_60709595194% (33)
- Cisco Nexus 7000 Introduction To NX-OS Lab GuideDocument38 pagesCisco Nexus 7000 Introduction To NX-OS Lab Guiderazzzzzzzzzzz100% (1)
- 2 TolentinoDocument12 pages2 TolentinoMA. ANGELINE GRANADANo ratings yet
- ADAPT-Builder 2019 GUI Quick Reference GuideDocument103 pagesADAPT-Builder 2019 GUI Quick Reference GuideephremNo ratings yet
- Ericsson AXE 810: Switch (ROTD)Document4 pagesEricsson AXE 810: Switch (ROTD)Kao Sun HoNo ratings yet
- Manual Daily Calorie Log: MyfitnesspalDocument4 pagesManual Daily Calorie Log: MyfitnesspalAzariah Burnside100% (2)
- STRESS HealthDocument40 pagesSTRESS HealthHajra KhanNo ratings yet
- Solow 5e Web SolutionsDocument58 pagesSolow 5e Web SolutionsOscar VelezNo ratings yet
- Week 1 Macro (DDR)Document49 pagesWeek 1 Macro (DDR)Stevie Sean100% (1)
- Dell Inspiron 5547 15Document7 pagesDell Inspiron 5547 15Kiti HowaitoNo ratings yet
- Algorithm Design: Figure 1. Architecture Diagram For Greykite Library's Main Forecasting Algorithm, SilverkiteDocument3 pagesAlgorithm Design: Figure 1. Architecture Diagram For Greykite Library's Main Forecasting Algorithm, Silverkitesiper34606No ratings yet
- 2 MercaptoEthanolDocument8 pages2 MercaptoEthanolMuhamad ZakyNo ratings yet
- MODULE 1 - Contemporary WorldDocument4 pagesMODULE 1 - Contemporary WorldaapNo ratings yet
- Soal PTS Vii BigDocument6 pagesSoal PTS Vii Bigdimas awe100% (1)
- KRPL Shahjahanpur Check List For Arc Welding MachineDocument1 pageKRPL Shahjahanpur Check List For Arc Welding MachineA S YadavNo ratings yet
- Liquid Process Piping - Part 1 General Piping Design PDFDocument33 pagesLiquid Process Piping - Part 1 General Piping Design PDFnitin guptaNo ratings yet
- Introduction of Woman Role in SocietyDocument12 pagesIntroduction of Woman Role in SocietyApple DogNo ratings yet
- English Lesson Plan Form 4 (Literature: "The Living Photograph")Document2 pagesEnglish Lesson Plan Form 4 (Literature: "The Living Photograph")Maisarah Mohamad100% (3)
- Test Bank Bank For Advanced Accounting 1 E by Bline 382235889 Test Bank Bank For Advanced Accounting 1 E by BlineDocument31 pagesTest Bank Bank For Advanced Accounting 1 E by Bline 382235889 Test Bank Bank For Advanced Accounting 1 E by BlineDe GuzmanNo ratings yet
- 32 Forms of God GaneshaDocument16 pages32 Forms of God Ganeshasudhakarpk2011100% (2)