You might also like
- Changes in The Sexual Function During Pregnancy: Aim. MethodsDocument10 pagesChanges in The Sexual Function During Pregnancy: Aim. MethodsYosep SutandarNo ratings yet
- Infertility and Sexual Dysfunctions: A Systematic Literature ReviewDocument8 pagesInfertility and Sexual Dysfunctions: A Systematic Literature ReviewTantonio Tri PutraNo ratings yet
- Age and Infertility:: The Biological Clock: Fact or Fiction?Document5 pagesAge and Infertility:: The Biological Clock: Fact or Fiction?Anna HamdaniNo ratings yet
- Characteristics Associated With Ever Having An Abortion: Discussion and ConclusionsDocument2 pagesCharacteristics Associated With Ever Having An Abortion: Discussion and ConclusionsbeqtinuraniNo ratings yet
- Epidemiology of Infertility and Recurrent Pregnancy Loss in Society With Fewer ChildrenDocument6 pagesEpidemiology of Infertility and Recurrent Pregnancy Loss in Society With Fewer ChildrenDavid AdityaNo ratings yet
- 06 Chapter 2Document48 pages06 Chapter 2Prakash BalagurunathanNo ratings yet
- Male and Female InfertilityDocument55 pagesMale and Female InfertilityNkopengieh Rene PochiekenNo ratings yet
- Sexual Dysfunction After Delivery: Faculty of Medicine, Menoufia UniversityDocument22 pagesSexual Dysfunction After Delivery: Faculty of Medicine, Menoufia UniversityWael GaberNo ratings yet
- Sexual - Life - and - Dysfunction - After - Maternal - Morbidi BGFNBRNDocument14 pagesSexual - Life - and - Dysfunction - After - Maternal - Morbidi BGFNBRNOctaria SaputraNo ratings yet
- Sexual Dysfunction 3Document23 pagesSexual Dysfunction 3Wael GaberNo ratings yet
- Spontaneous Abortion - Risk Factors, Etiology, Clinical Manifestations, and Diagnostic Evaluation - UpToDate PDFDocument23 pagesSpontaneous Abortion - Risk Factors, Etiology, Clinical Manifestations, and Diagnostic Evaluation - UpToDate PDFPaula Grtrs WstrmrNo ratings yet
- Lag Aert 2017Document8 pagesLag Aert 2017abdi syahputraNo ratings yet
- Bio Infertility EditedDocument9 pagesBio Infertility EditedSABARI SRINIVAS ANo ratings yet
- Fetal Death UpToDate 2feb04 196028 284 18220Document23 pagesFetal Death UpToDate 2feb04 196028 284 18220restuwidianaNo ratings yet
- Miscarriage in India: A Population-Based Study: Tervals, Because It Was Not Possible From The Data Set ToDocument3 pagesMiscarriage in India: A Population-Based Study: Tervals, Because It Was Not Possible From The Data Set ToMutianaUmminyaKhanzaNo ratings yet
- Author Information Kafaei Atrian MDocument9 pagesAuthor Information Kafaei Atrian MabdullahNo ratings yet
- Endo Met RitisDocument9 pagesEndo Met RitisabdullahNo ratings yet
- Endo Met RitisDocument9 pagesEndo Met RitisabdullahNo ratings yet
- JMB 2012 2 3 379 385 PDFDocument7 pagesJMB 2012 2 3 379 385 PDFRayhan Oemar AljaidyNo ratings yet
- Coitus Late in PregnancyDocument8 pagesCoitus Late in PregnancyabdullahNo ratings yet
- Sexual Activity Health and Well-Being The Beneficial Roles of Coitus and MasturbationDocument15 pagesSexual Activity Health and Well-Being The Beneficial Roles of Coitus and Masturbationomar.bordon0110No ratings yet
- First Page PDFDocument1 pageFirst Page PDFAmenNo ratings yet
- Examining The Number of Births A Woman (Or A Man) Has Produced by A Given Point in Time, Such As The Date of A Census or SurveyDocument17 pagesExamining The Number of Births A Woman (Or A Man) Has Produced by A Given Point in Time, Such As The Date of A Census or SurveyMayjane MicayasNo ratings yet
- Pre TermDocument14 pagesPre TermAnuradha DissanayakeNo ratings yet
- 1 s2.0 S0009912018302200 Main PDFDocument9 pages1 s2.0 S0009912018302200 Main PDFIvanes IgorNo ratings yet
- Overview of Infertility - UpToDateDocument16 pagesOverview of Infertility - UpToDateTaís CidrãoNo ratings yet
- Argumentative EssayDocument4 pagesArgumentative EssayHandika KiswantoroNo ratings yet
- Spontaneous AbortionDocument17 pagesSpontaneous Abortionanon_985338331No ratings yet
- Katherine J Gold Sheila M Marcus: Table 1Document4 pagesKatherine J Gold Sheila M Marcus: Table 1angelie21No ratings yet
- Chapter 1 Reproductive Health EpidemiologyyDocument13 pagesChapter 1 Reproductive Health EpidemiologyyAnnisa NurrachmawatiNo ratings yet
- Nwancho Peculiar SeminarDocument25 pagesNwancho Peculiar SeminarAzubuike ChidiNo ratings yet
- JR InfertilitasDocument15 pagesJR InfertilitasFitrahul afifahNo ratings yet
- NCM 109 JournalDocument2 pagesNCM 109 JournalAustin DiodaNo ratings yet
- Marital InfertilityDocument4 pagesMarital InfertilityasclepiuspdfsNo ratings yet
- P-342 Poster: Abstracts of The 25th Annual Meeting of ESHRE, Amsterdam, The Netherlands, 28 June - 1 July, 2009Document1 pageP-342 Poster: Abstracts of The 25th Annual Meeting of ESHRE, Amsterdam, The Netherlands, 28 June - 1 July, 2009Aby SuryaNo ratings yet
- Finaldraft AbortionDocument9 pagesFinaldraft Abortionapi-281584433No ratings yet
- High Risk WomenDocument17 pagesHigh Risk WomenamitNo ratings yet
- Dysmenorrhea in AdolescentsDocument12 pagesDysmenorrhea in AdolescentsDeff HaningNo ratings yet
- Bio Project CorrectedDocument35 pagesBio Project CorrectedSABARI SRINIVAS ANo ratings yet
- Population: The Dynamics of Biological PopulationsDocument5 pagesPopulation: The Dynamics of Biological PopulationsFred Jaff Fryan RosalNo ratings yet
- Dafpus Abortus 3Document16 pagesDafpus Abortus 3ShintungNo ratings yet
- Aging and Infertility in WomenDocument5 pagesAging and Infertility in Womendoc.GNo ratings yet
- BIOLOGY Infertility ProjectDocument6 pagesBIOLOGY Infertility ProjectSOUMYADEEP BHUINYA100% (1)
- 3.2.3. Social Causes and Consequences Social Factors That A Ect Timing of Menarche (Causes)Document24 pages3.2.3. Social Causes and Consequences Social Factors That A Ect Timing of Menarche (Causes)Azizah LindaNo ratings yet
- Studiu de CazDocument27 pagesStudiu de CazAdina TomsaNo ratings yet
- PregnantDocument10 pagesPregnantm.sandra12340No ratings yet
- In Vitro Fertilization For M6 Students: YL TsaiDocument49 pagesIn Vitro Fertilization For M6 Students: YL TsaiLee BoborasNo ratings yet
- Lec 1Document5 pagesLec 1mudassir qazalbashNo ratings yet
- Population: The Dynamics of Biological PopulationsDocument5 pagesPopulation: The Dynamics of Biological PopulationsMa Theressa Balangyao SaloNo ratings yet
- Laborinduction: Areviewof Currentmethods: Mildred M. RamirezDocument11 pagesLaborinduction: Areviewof Currentmethods: Mildred M. RamirezRolando DiazNo ratings yet
- Javon WitherspoonDocument6 pagesJavon Witherspoonapi-445367279No ratings yet
- Faktor Risiko 3 Dan PemeriksaanDocument19 pagesFaktor Risiko 3 Dan PemeriksaanNidhaSavitriNo ratings yet
- Author Information Kafaei Atrian MDocument9 pagesAuthor Information Kafaei Atrian MabdullahNo ratings yet
- Sexual DysfunctionDocument21 pagesSexual DysfunctionWael GaberNo ratings yet
- 1-6 Amos Catherine UlummaAmosDocument83 pages1-6 Amos Catherine UlummaAmosmrpboss1No ratings yet
- Author Information Kafaei Atrian MDocument9 pagesAuthor Information Kafaei Atrian MabdullahNo ratings yet
- Blighted OvumDocument9 pagesBlighted OvumAdes Desrita CarmeliaNo ratings yet
- Teenage PregnancyDocument1 pageTeenage PregnancyDiianaMorenoNo ratings yet
- Healthcare 11 00033Document12 pagesHealthcare 11 00033ALEXANDRA PAMELA BALLADARES MARMANILLONo ratings yet
- Fashion Design Drawing 12Document9 pagesFashion Design Drawing 12Ioan-ovidiu CordisNo ratings yet
- Food GuidelinesDocument0 pagesFood Guidelinesmukesh8981No ratings yet
- Euro4 6Document11 pagesEuro4 6Ioan-ovidiu CordisNo ratings yet
- Final Program Mandela PDFDocument7 pagesFinal Program Mandela PDFIoan-ovidiu CordisNo ratings yet
- Mahatma Gandhi: His Life and LegacyDocument0 pagesMahatma Gandhi: His Life and LegacyMohammad PiraniNo ratings yet
- Clothing and Age - A Critical Review PDFDocument21 pagesClothing and Age - A Critical Review PDFIoan-ovidiu CordisNo ratings yet
- How To MeditateDocument51 pagesHow To MeditateIoan-ovidiu CordisNo ratings yet
- 5.selected Quotes MandelaDocument3 pages5.selected Quotes MandelaunmasallaNo ratings yet
- Mandela Quotes Publicity Guidelines1Document29 pagesMandela Quotes Publicity Guidelines1shahriarf15No ratings yet
- Time and Kalachakra PDFDocument23 pagesTime and Kalachakra PDFIoan-ovidiu Cordis100% (1)
- Mandela in His Own WordsDocument40 pagesMandela in His Own WordsUN Information Service GenevaNo ratings yet
- Mahatma Gandhi: His Life and LegacyDocument0 pagesMahatma Gandhi: His Life and LegacyMohammad PiraniNo ratings yet
- Final Program Mandela PDFDocument7 pagesFinal Program Mandela PDFIoan-ovidiu CordisNo ratings yet
- Gandhi Mohandas Karamchand MahatmaDocument16 pagesGandhi Mohandas Karamchand MahatmaMohan RangaNo ratings yet
- The Secret of The Golden FlowerDocument5 pagesThe Secret of The Golden FlowerIoan-ovidiu Cordis67% (3)
- Gandhi Quotes PDFDocument3 pagesGandhi Quotes PDFIoan-ovidiu CordisNo ratings yet
- 5.selected Quotes MandelaDocument3 pages5.selected Quotes MandelaunmasallaNo ratings yet
- Zen BasicsDocument33 pagesZen Basicsgavinsomething100% (1)
- Secret of The Golden Flower SampleDocument60 pagesSecret of The Golden Flower SampleIoan-ovidiu CordisNo ratings yet
- Gandhi Quotes PDFDocument3 pagesGandhi Quotes PDFIoan-ovidiu CordisNo ratings yet
- How To Practice Zazen: PpendixDocument0 pagesHow To Practice Zazen: PpendixBrent Cullen100% (1)
- Taoist Yoga For Women by OLEG TCHERNEDocument241 pagesTaoist Yoga For Women by OLEG TCHERNEIoan-ovidiu Cordis100% (4)
- Secret of The Golden Flower SampleDocument60 pagesSecret of The Golden Flower SampleIoan-ovidiu CordisNo ratings yet
- Alchemy The Secret of ImmortalityDocument73 pagesAlchemy The Secret of ImmortalityIoan-ovidiu Cordis100% (2)
- The Secret of The Golden FlowerDocument5 pagesThe Secret of The Golden FlowerIoan-ovidiu Cordis67% (3)
- The Secret of The Golden Flower: Jung andDocument38 pagesThe Secret of The Golden Flower: Jung andIoan-ovidiu CordisNo ratings yet
- Transmissiononline OrgDocument3 pagesTransmissiononline OrgIoan-ovidiu CordisNo ratings yet
- The Secret of The Golden Flower: Jung andDocument38 pagesThe Secret of The Golden Flower: Jung andIoan-ovidiu CordisNo ratings yet
- Transmissiononline OrgDocument3 pagesTransmissiononline OrgIoan-ovidiu CordisNo ratings yet
- L So I Empty Vessel MagazineDocument4 pagesL So I Empty Vessel MagazineIoan-ovidiu CordisNo ratings yet
- HannaDocument3 pagesHannaMagda FrutasNo ratings yet
- Perdarahan ObstetryDocument43 pagesPerdarahan ObstetryPutri EffendyNo ratings yet
- Supports of UterusDocument16 pagesSupports of UterusinnyNo ratings yet
- Assisted Reproductive Technologies (ART) : Doaa HegabDocument23 pagesAssisted Reproductive Technologies (ART) : Doaa HegabLinguum100% (1)
- MGM Bill Tri-Fold BrochureDocument2 pagesMGM Bill Tri-Fold BrochureMatthew Hess100% (1)
- Female and Male GenitaliaDocument5 pagesFemale and Male GenitaliaMary Mae BuellaNo ratings yet
- Male Physical and Sexual Changes: Happening To An IndividualDocument2 pagesMale Physical and Sexual Changes: Happening To An IndividualMarian Licuasen Ab-aboNo ratings yet
- VIA (Visual Inspection With Acetic Acid Aplication) Preparation of StepsDocument20 pagesVIA (Visual Inspection With Acetic Acid Aplication) Preparation of StepsIndonesian Journal of Cancer100% (1)
- Alongamento Do Pénis em Pacientes Que Têm HipogonadismoDocument1 pageAlongamento Do Pénis em Pacientes Que Têm Hipogonadismovacextensor1050% (2)
- DysmenorrheaDocument35 pagesDysmenorrheaAs-sifa KharismaNo ratings yet
- Pid XureDocument8 pagesPid XureMary Karen Rose BorjaNo ratings yet
- 1 Anatomy and Physiology of ReproductionDocument31 pages1 Anatomy and Physiology of Reproductionjose mari chanNo ratings yet
- TOG Vaginal HysterectomyDocument6 pagesTOG Vaginal HysterectomyYasmin AlkhatibNo ratings yet
- Pelvis FrozenDocument23 pagesPelvis FrozenPetar PribicNo ratings yet
- PP-MIR-US-0477-1 Mirena Patient Brochure DigitalDocument13 pagesPP-MIR-US-0477-1 Mirena Patient Brochure DigitalimtariqueNo ratings yet
- Biology IGCSE NotesDocument3 pagesBiology IGCSE NotesCharxd zzNo ratings yet
- Biology 101 Reproductive HealthDocument7 pagesBiology 101 Reproductive HealthNeelam Yadav100% (1)
- The Future For The GynaecologistDocument2 pagesThe Future For The GynaecologistwmogtNo ratings yet
- LaparosDocument3 pagesLaparosMurtaz BokhuaNo ratings yet
- WPR22220 Cervical PolypsDocument2 pagesWPR22220 Cervical PolypsSri Wahyuni SahirNo ratings yet
- Daft Arp Us TakaDocument3 pagesDaft Arp Us Takaudinamin1007No ratings yet
- Critical Appraisal Obsgin AditDocument19 pagesCritical Appraisal Obsgin AditGuruh PanjiNo ratings yet
- Genitals and Inguinal Assessment-FemaleDocument19 pagesGenitals and Inguinal Assessment-Femalemalyn1218No ratings yet
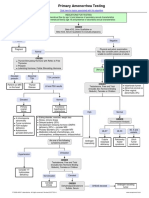
- Primary Amenorrhea Testing AlgorithmDocument1 pagePrimary Amenorrhea Testing AlgorithmfarmasiNo ratings yet
- Mestrual CycleDocument15 pagesMestrual CycleMary-Ann SanchezNo ratings yet
- Disease Definisi Etiologi Manfes/findingDocument3 pagesDisease Definisi Etiologi Manfes/findingRiani KusumadewiNo ratings yet
- Obg - 9.4.20 (Forenoon) Unit 12 - Infertility and Its ManagementDocument81 pagesObg - 9.4.20 (Forenoon) Unit 12 - Infertility and Its ManagementElakkiyaanu64 Elakkiyaanu64No ratings yet
- Disorders of Sexual FunctioningDocument5 pagesDisorders of Sexual FunctioningDhaneanne Marie ChanNo ratings yet
- Vaginal DischargeDocument1 pageVaginal DischargeRAHMANo ratings yet
- Abnormal Uterine BleedingDocument44 pagesAbnormal Uterine BleedingBezza Mae Roche CruzNo ratings yet