You might also like
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Production and Operations ManagementDocument21 pagesProduction and Operations ManagementGaurav218100% (4)
- BHEL's Bowl Mills and Their FeaturesDocument12 pagesBHEL's Bowl Mills and Their FeaturesAbhishek KumarNo ratings yet
- Working of CNG EngineDocument10 pagesWorking of CNG EngineSardar Wasif Ashraf KhanNo ratings yet
- D51 Lubrication and Hydraulics BOBST EXPERTCUT 3Document28 pagesD51 Lubrication and Hydraulics BOBST EXPERTCUT 3DeniMestiWidianto100% (1)
- Report On Oil Types and Applications: 3 YearDocument5 pagesReport On Oil Types and Applications: 3 YearMahmoud KassabNo ratings yet
- Project MangemntDocument26 pagesProject MangemntAkash Kumar DevNo ratings yet
- Mel311 Part IIIDocument52 pagesMel311 Part IIIAkash Kumar DevNo ratings yet
- Rac ExpDocument44 pagesRac ExpAkash Kumar DevNo ratings yet
- Legacy Tcl/Tk TrainingDocument61 pagesLegacy Tcl/Tk TrainingAkash Kumar DevNo ratings yet
- TQM - Notes Anna UniversityDocument86 pagesTQM - Notes Anna UniversityMohsin AhmedNo ratings yet
- Powered by Amplitud3'Zz ... in CsDocument1 pagePowered by Amplitud3'Zz ... in CsAkash Kumar DevNo ratings yet
- Success InterviewDocument11 pagesSuccess InterviewAkash Kumar DevNo ratings yet
- Anna University Exam Paper Theory of Metal Cutting: Production EngineeringDocument3 pagesAnna University Exam Paper Theory of Metal Cutting: Production EngineeringAkash Kumar DevNo ratings yet
- TataDocument2 pagesTataAkash Kumar DevNo ratings yet
- Sample Paper InfosysDocument19 pagesSample Paper InfosysPankaj GuptaNo ratings yet
- 02MA751 Foundry Technology Dec Jan 2006Document1 page02MA751 Foundry Technology Dec Jan 2006Akash Kumar DevNo ratings yet
- Book1 HTMLDocument3 pagesBook1 HTMLAkash Kumar DevNo ratings yet
- 06 Strengthening MechanismsDocument63 pages06 Strengthening Mechanismspranavkumarparit100% (2)
- Defects PointDocument8 pagesDefects PointAnkit SenNo ratings yet
- Cast Iron Properties and Types in 40 CharactersDocument34 pagesCast Iron Properties and Types in 40 CharactersMKPashaPasha100% (1)
- New Microsoft Office PowerPoint PresentationDocument40 pagesNew Microsoft Office PowerPoint PresentationAkash Kumar DevNo ratings yet
- IEEE Copyright FormDocument2 pagesIEEE Copyright FormMatías IgnacioNo ratings yet
- PS-N AC-63 Number of Votes Vast Male Female Others Total From 7am To 9 Am 9 Am To 11 Am 11 Am To 1 PM 1 PM To 3 PM 3 PM To 5 PM 5 PM To 6 PMDocument1 pagePS-N AC-63 Number of Votes Vast Male Female Others Total From 7am To 9 Am 9 Am To 11 Am 11 Am To 1 PM 1 PM To 3 PM 3 PM To 5 PM 5 PM To 6 PMAkash Kumar DevNo ratings yet
- 1 Stress Strain SMDocument48 pages1 Stress Strain SMappuanandhNo ratings yet
- Daemon ProcessDocument1 pageDaemon ProcessAkash Kumar DevNo ratings yet
- GATE 2014: Graduate Aptitude Test in Engineering 2014Document2 pagesGATE 2014: Graduate Aptitude Test in Engineering 2014Akash Kumar DevNo ratings yet
- Behaviour of MaterialsDocument9 pagesBehaviour of MaterialsAkash Kumar DevNo ratings yet
- Principles of Ic EnginesDocument15 pagesPrinciples of Ic EnginesIvan KopićNo ratings yet
- New Text DocumentDocument3 pagesNew Text DocumentAkash Kumar DevNo ratings yet
- S S - A L: Tress AND Train Xial OadingDocument11 pagesS S - A L: Tress AND Train Xial OadingAkash Kumar DevNo ratings yet
- The Codemasters Software Company Limited Software License AgreementDocument4 pagesThe Codemasters Software Company Limited Software License AgreementJigar TrivediNo ratings yet
- Win Configure Updated Title "Recommended Settings Updated"Document2 pagesWin Configure Updated Title "Recommended Settings Updated"dams6797No ratings yet
- PERTAMINA - SEBANA P SeriesDocument1 pagePERTAMINA - SEBANA P SeriesapriambadhaNo ratings yet
- Eco Equivalency ChartDocument1 pageEco Equivalency ChartEstakoza GoldNo ratings yet
- Harga-PelumasDocument9 pagesHarga-PelumasEndry BurhanuddinNo ratings yet
- Step 50800 50900Document3 pagesStep 50800 50900hansiiiNo ratings yet
- Tabela de Óleos LubrificantesDocument2 pagesTabela de Óleos LubrificantesAlbert MesquitaNo ratings yet
- Marine Transmissions List of Lubricants TE-ML 04Document16 pagesMarine Transmissions List of Lubricants TE-ML 04Rodrigues1392No ratings yet
- Price Quotation-Harga OliDocument2 pagesPrice Quotation-Harga OliRidwan KurniawanNo ratings yet
- Engine Tribology - Faculty of Engineering - University of LeedsDocument2 pagesEngine Tribology - Faculty of Engineering - University of LeedssbhariNo ratings yet
- Lubricants For Trucks: Reliability and Efficiency To Reach Your DestinationDocument19 pagesLubricants For Trucks: Reliability and Efficiency To Reach Your DestinationAMAZING AGNo ratings yet
- Corolla / Auris: Zre, NreDocument2 pagesCorolla / Auris: Zre, NreJavier Paredes FloresNo ratings yet
- Premium: SAE 20W-50 Motor OilDocument2 pagesPremium: SAE 20W-50 Motor OilengerbethNo ratings yet
- MAK Lubricants Price ListDocument4 pagesMAK Lubricants Price Listhajari100% (3)
- Equivalent Produk Oli & Grease Pertamina, Shell, Conoco & Total 2009Document1 pageEquivalent Produk Oli & Grease Pertamina, Shell, Conoco & Total 2009franz.xoithNo ratings yet
- Catalog BravaDocument6 pagesCatalog BravaPerformance Lubricants, C.A.No ratings yet
- Uporedna Tabela Addinol MazivaDocument2 pagesUporedna Tabela Addinol MazivaBane RadovicNo ratings yet
- BMW Operating Fluids Manual Transmission (2009.04.23)Document3 pagesBMW Operating Fluids Manual Transmission (2009.04.23)Master XeotoNo ratings yet
- Tribology - Interdisciplinary Approach and Economic BenefitsDocument22 pagesTribology - Interdisciplinary Approach and Economic BenefitsDr Junaid Hassan MasoodiNo ratings yet
- Lol Te ML 03 enDocument17 pagesLol Te ML 03 enGoudjilNo ratings yet
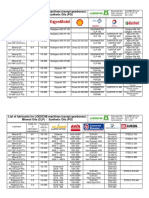
- List of Lubricants For LOESCHE-machines (Except Gearboxes) : Mineral Oils (CLP) / Synthetic Oils (PG)Document8 pagesList of Lubricants For LOESCHE-machines (Except Gearboxes) : Mineral Oils (CLP) / Synthetic Oils (PG)MossaabSelaimiaNo ratings yet
- TCC - AMSOIL Synthetic Chaincase & Gear OilDocument2 pagesTCC - AMSOIL Synthetic Chaincase & Gear OilamsoildealerNo ratings yet
- Competitive Cross-Reference ClarionDocument2 pagesCompetitive Cross-Reference ClarionHugo PinargoteNo ratings yet
- SAE Viscosity Grades Viscosity Table and ChartDocument3 pagesSAE Viscosity Grades Viscosity Table and ChartmaniNo ratings yet
- JP U JOINT KIT IDENTIFICATION CatalogDocument20 pagesJP U JOINT KIT IDENTIFICATION CatalogAlvaro Patricio Etcheverry TroncosoNo ratings yet
- Oil stock card monitoring systemDocument33 pagesOil stock card monitoring systemAndo Wibowo TariganNo ratings yet
- Box Color Guide: Motorcycle Engine OilDocument2 pagesBox Color Guide: Motorcycle Engine OilAndi Septian Eka SetiawanNo ratings yet
- Product Groups Lubricant Classes For Service Fill Ecolife Offroad For Special Vehicles and Stationary ApplicationsDocument7 pagesProduct Groups Lubricant Classes For Service Fill Ecolife Offroad For Special Vehicles and Stationary ApplicationsMOHAMED GamalNo ratings yet
- Maximum Retail Price: 2T Specification 20 40 60 250 500 1 5Document2 pagesMaximum Retail Price: 2T Specification 20 40 60 250 500 1 5Nitansh GuptaNo ratings yet