You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Creature Loot PDF - GM BinderDocument97 pagesCreature Loot PDF - GM BinderAlec0% (1)
- Case ReportDocument28 pagesCase Reportgraceswan100% (1)
- Coriolis - Atlas CompendiumDocument62 pagesCoriolis - Atlas CompendiumSquamata100% (2)
- Primary Checkpoint - Science (0846) October 2016 Paper 2 MSDocument12 pagesPrimary Checkpoint - Science (0846) October 2016 Paper 2 MSdinakarc78% (9)
- TheSun 2008-11-04 Page16 Asian Stocks Rally Continues On Policy HopesDocument1 pageTheSun 2008-11-04 Page16 Asian Stocks Rally Continues On Policy HopesImpulsive collectorNo ratings yet
- Pathology and Genetics of Head and Neck TumoursDocument435 pagesPathology and Genetics of Head and Neck TumoursMonica MehendirattaNo ratings yet
- DKBM IndonesiaDocument25 pagesDKBM IndonesiaBagas Andriyono100% (1)
- DKBM IndonesiaDocument25 pagesDKBM IndonesiaBagas Andriyono100% (1)
- Homeroom Guidance Grade 12 Quarter - Module 4 Decisive PersonDocument4 pagesHomeroom Guidance Grade 12 Quarter - Module 4 Decisive PersonMhiaBuenafe86% (36)
- Journal Reading - AnemiaDocument31 pagesJournal Reading - AnemiagraceswanNo ratings yet
- Diskusi Topik Dr. KholisDocument29 pagesDiskusi Topik Dr. KholisgraceswanNo ratings yet
- DislocationDocument33 pagesDislocationgraceswanNo ratings yet
- Pharmacologic Treatment of Chorea in Huntington'S Disease: Drug WarningsDocument2 pagesPharmacologic Treatment of Chorea in Huntington'S Disease: Drug WarningsgraceswanNo ratings yet
- Open FractureDocument20 pagesOpen FracturegraceswanNo ratings yet
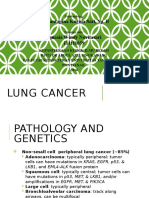
- Tumor ParuDocument20 pagesTumor ParugraceswanNo ratings yet
- 203 382 1 SMDocument9 pages203 382 1 SMNajwan Ihsan YPasNo ratings yet
- Nasopharyngeal Tumor Classification GuideDocument22 pagesNasopharyngeal Tumor Classification GuidegraceswanNo ratings yet
- Abdominal Cutaneous Nerve Entrapment Syndrome (ACNES) : A Commonly Overlooked Cause of Abdominal PainDocument8 pagesAbdominal Cutaneous Nerve Entrapment Syndrome (ACNES) : A Commonly Overlooked Cause of Abdominal PaingraceswanNo ratings yet
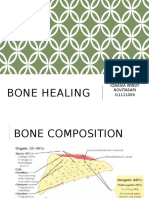
- Bone HealingDocument31 pagesBone HealinggraceswanNo ratings yet
- Chpt08 Id Characterization StreppneumoDocument14 pagesChpt08 Id Characterization StreppneumograceswanNo ratings yet
- Six Newly Recognized Types of Streptococcus PneumoniaeDocument4 pagesSix Newly Recognized Types of Streptococcus PneumoniaegraceswanNo ratings yet
- Emergence of Resistant Shigella Dysentriae Bacteria in The IDP CampsDocument2 pagesEmergence of Resistant Shigella Dysentriae Bacteria in The IDP CampsgraceswanNo ratings yet
- UnicefDocument61 pagesUnicefUgaugaaNo ratings yet
- JurnalDocument8 pagesJurnalRandy Nugraha Pratama100% (1)
- Streptococcous General MethodsDocument69 pagesStreptococcous General MethodsPraveen KumarNo ratings yet
- 1712Document2 pages1712graceswanNo ratings yet
- Seajphv 2 N 2Document60 pagesSeajphv 2 N 2graceswanNo ratings yet
- Penyakit Inf Saluran Pencernaan PDFDocument9 pagesPenyakit Inf Saluran Pencernaan PDFAde PermanaNo ratings yet
- JurnalDocument8 pagesJurnalRandy Nugraha Pratama100% (1)
- JurnalDocument13 pagesJurnalHaerul Amri HukmanNo ratings yet
- Okehasbarinda Hasan 08 24Document24 pagesOkehasbarinda Hasan 08 24graceswanNo ratings yet
- Child poverty disparities IndonesiaDocument300 pagesChild poverty disparities IndonesiagraceswanNo ratings yet
- Kuliah & Praktikum Modul Gastrointestinal: Windy Novita I11111059Document1 pageKuliah & Praktikum Modul Gastrointestinal: Windy Novita I11111059graceswanNo ratings yet
- 1712Document2 pages1712graceswanNo ratings yet
- aCTION PLAN IN HEALTHDocument13 pagesaCTION PLAN IN HEALTHCATHERINE FAJARDONo ratings yet
- 457 PDFDocument8 pages457 PDFAbbey Joy CollanoNo ratings yet
- A Study On Consumer Buying Behaviour Towards ColgateDocument15 pagesA Study On Consumer Buying Behaviour Towards Colgatebbhaya427No ratings yet
- Assignment - Stocks and CBDocument2 pagesAssignment - Stocks and CBGhulam HassanNo ratings yet
- Canary TreatmentDocument117 pagesCanary TreatmentRam KLNo ratings yet
- Rozgar Sutra EnglishDocument105 pagesRozgar Sutra EnglishRisingsun PradhanNo ratings yet
- Amino AcidsDocument17 pagesAmino AcidsANAND sNo ratings yet
- Anna University CTDocument3 pagesAnna University CTprayog8No ratings yet
- Lecture-3 Sources of Bioelectric PotentialDocument13 pagesLecture-3 Sources of Bioelectric PotentialMurali krishnan.MNo ratings yet
- GF26.10-S-0002S Manual Transmission (MT), Function 9.7.03 Transmission 716.6 in MODEL 639.601 /603 /605 /701 /703 /705 /711 /713 /811 /813 /815Document2 pagesGF26.10-S-0002S Manual Transmission (MT), Function 9.7.03 Transmission 716.6 in MODEL 639.601 /603 /605 /701 /703 /705 /711 /713 /811 /813 /815Sven GoshcNo ratings yet
- OWASP Dependency-Check Plugin: DescriptionDocument10 pagesOWASP Dependency-Check Plugin: DescriptionFelipe BarbosaNo ratings yet
- Entrepreneurship: Ali Raza (Ph.D. Scholar, Near East University, North Cyprus, Mersin 10, Turkey)Document35 pagesEntrepreneurship: Ali Raza (Ph.D. Scholar, Near East University, North Cyprus, Mersin 10, Turkey)Ameen KolachiNo ratings yet
- The Diffusion of Microfinance: An Extended Analysis & Replication ofDocument33 pagesThe Diffusion of Microfinance: An Extended Analysis & Replication ofNaman GovilNo ratings yet
- PENGARUH CYBERBULLYING BODY SHAMING TERHADAP KEPERCAYAAN DIRIDocument15 pagesPENGARUH CYBERBULLYING BODY SHAMING TERHADAP KEPERCAYAAN DIRIRizky Hizrah WumuNo ratings yet
- SBLO Jepp Charts PDFDocument12 pagesSBLO Jepp Charts PDFElton CacefoNo ratings yet
- Documentation Control HandbookDocument9 pagesDocumentation Control Handbookcrainvictor 45No ratings yet
- Chapter 20: Sleep Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionDocument4 pagesChapter 20: Sleep Garzon Maaks: Burns' Pediatric Primary Care, 7th EditionHelen UgochukwuNo ratings yet
- GTA Max Profit Bunker Locations Update v1.4Document1 pageGTA Max Profit Bunker Locations Update v1.4Sam FarrelNo ratings yet
- New Pacific Timber v. Señeris, 101 SCRA 686Document5 pagesNew Pacific Timber v. Señeris, 101 SCRA 686Ishmael AbrahamNo ratings yet
- 01 Lab ManualDocument5 pages01 Lab ManualM Waqar ZahidNo ratings yet
- Chapter - 2 Fish MongeryDocument10 pagesChapter - 2 Fish MongeryKrishna ChaudharyNo ratings yet
- ReadingDocument6 pagesReadingakhyar sanchiaNo ratings yet
- Regional Office X: Republic of The PhilippinesDocument2 pagesRegional Office X: Republic of The PhilippinesCoreine Imee ValledorNo ratings yet
- Base Is OkDocument84 pagesBase Is OkajaydevmalikNo ratings yet