You might also like
- F DiagramDocument1 pageF DiagramBunga P.75% (4)
- Situation Analysis of Children in Timor-LesteDocument194 pagesSituation Analysis of Children in Timor-LesteBunga P.No ratings yet
- I 1380 e 00Document241 pagesI 1380 e 00Alexandre Rodrigues50% (2)
- Manual of Antimicrobial Susceptibility TestingDocument241 pagesManual of Antimicrobial Susceptibility TestingEndale Balcha100% (4)
- Build It Back Better - Deconstructing Food Security For Improved Measurement and ActionDocument7 pagesBuild It Back Better - Deconstructing Food Security For Improved Measurement and ActionBunga P.100% (1)
- Food Additives 2edDocument953 pagesFood Additives 2edarzach8885100% (13)
- In This Guide... : Getting ThereDocument3 pagesIn This Guide... : Getting ThereBunga P.No ratings yet
- 970730-Guidelines of Agricultural Policies in TaiwanDocument25 pages970730-Guidelines of Agricultural Policies in TaiwanBunga P.No ratings yet
- LSH Ln-11 Nov 2010 (Lppom Mui)Document34 pagesLSH Ln-11 Nov 2010 (Lppom Mui)Bunga P.No ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Antibiotic Selection in SepsisDocument4 pagesAntibiotic Selection in SepsisIndah AmisaniNo ratings yet
- Generalov-II - Medical Microbiology Virology Immunology - Pt-2 - 2016 PDFDocument392 pagesGeneralov-II - Medical Microbiology Virology Immunology - Pt-2 - 2016 PDFMohammad YasirNo ratings yet
- Microbiology ComplexDocument31 pagesMicrobiology ComplexAkbar WadwaniyaNo ratings yet
- Lab Manual Mic 316-Sep 2018Document15 pagesLab Manual Mic 316-Sep 2018aisyah fauziNo ratings yet
- What Is EbolaDocument3 pagesWhat Is EbolaDian Kurnia AnggraenyNo ratings yet
- HistologyDocument77 pagesHistologyRahul0% (1)
- Blood TypesDocument2 pagesBlood TypesThess Tecla Zerauc AzodnemNo ratings yet
- Un1529648 BDocument2 pagesUn1529648 BCB NitrideNo ratings yet
- Infectious Disease Catalogue LRDocument80 pagesInfectious Disease Catalogue LRKetevan MigriauliNo ratings yet
- Aso Test For Semester2Document3 pagesAso Test For Semester2Tarun AroraNo ratings yet
- DgReportingVF PDFDocument2 pagesDgReportingVF PDFRamani DantuluriNo ratings yet
- HbA1C, RBS AND FBS DATADocument2 pagesHbA1C, RBS AND FBS DATASamwel GachokaNo ratings yet
- Experiment 7: RH Typing (Tube Method) : Pre-Analytical PhaseDocument4 pagesExperiment 7: RH Typing (Tube Method) : Pre-Analytical PhasesummerNo ratings yet
- Case 4 - Diagnostic and Laboratory ProceduresDocument7 pagesCase 4 - Diagnostic and Laboratory ProceduresChristine Pialan SalimbagatNo ratings yet
- FormulationDocument9 pagesFormulationInternational Journal of Innovative Science and Research TechnologyNo ratings yet
- USP 51 Antimicrobial Effectiveness TestDocument4 pagesUSP 51 Antimicrobial Effectiveness TestAki Espaldon100% (1)
- IGCSE Bio - Blood DonationDocument13 pagesIGCSE Bio - Blood DonationTroy CampbellNo ratings yet
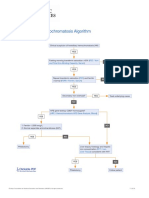
- Hereditary Hemochromatosis AlgorithmDocument1 pageHereditary Hemochromatosis AlgorithmS6b2No ratings yet
- TyphoidDocument3 pagesTyphoidShivam Tomar83% (6)
- Certificate of Analysis, Quality and Conformity: Certified: ISO 9001:2008, ISO 13485-2003 and WHO GMPDocument2 pagesCertificate of Analysis, Quality and Conformity: Certified: ISO 9001:2008, ISO 13485-2003 and WHO GMPsagor sagorNo ratings yet
- BSC Microbiology Syllabus Periyar UniversityDocument33 pagesBSC Microbiology Syllabus Periyar UniversityGopi RaviNo ratings yet
- Culture Media FinalDocument25 pagesCulture Media FinalRaghu KumarNo ratings yet
- Viruses, Viroids, and PrionsDocument45 pagesViruses, Viroids, and PrionsJillian LaoNo ratings yet
- Fowl Cholera 19 1995Document6 pagesFowl Cholera 19 1995Christian VillarrealNo ratings yet
- The RH Factor: How It Can Affect Your PregnancyDocument3 pagesThe RH Factor: How It Can Affect Your PregnancyTedd CamilingNo ratings yet
- Sonu 26S00230050665Document1 pageSonu 26S00230050665Rakesh KoliNo ratings yet
- Dog Blood TypesDocument10 pagesDog Blood Typespuscas16ramona7105100% (2)
- CTK Biotech-USA - Rapid Test - TradeDocument1 pageCTK Biotech-USA - Rapid Test - Tradeabdalazeez20122013No ratings yet
- Red Blood Cell Phenotyping of Blood Donors in Islamabad, PakistanDocument5 pagesRed Blood Cell Phenotyping of Blood Donors in Islamabad, PakistanAHNS123No ratings yet