You might also like
- Role of Transcranial Approaches in The Treatment of Sellar and Suprasellar LesionsDocument28 pagesRole of Transcranial Approaches in The Treatment of Sellar and Suprasellar LesionsVenansius Ratno KurniawanNo ratings yet
- ARTICULODocument4 pagesARTICULOALFREDO JUNIOR LEON ALEJONo ratings yet
- Protective Dural Flap For Bone Drilling at The Paraclinoid Region and Porus AcusticusDocument3 pagesProtective Dural Flap For Bone Drilling at The Paraclinoid Region and Porus AcusticusVenansius Ratno KurniawanNo ratings yet
- Cerebral Arterial Gas Embolism in A Professional Diver With A Persistent Foramen OvaleDocument3 pagesCerebral Arterial Gas Embolism in A Professional Diver With A Persistent Foramen OvaleVenansius Ratno KurniawanNo ratings yet
- Bubble-Induced Platelet Aggregation in A Rat Model of Decompression SicknessDocument5 pagesBubble-Induced Platelet Aggregation in A Rat Model of Decompression SicknessVenansius Ratno KurniawanNo ratings yet
- Immersive Surgical Anatomy of The Pterional ApproachDocument25 pagesImmersive Surgical Anatomy of The Pterional ApproachVenansius Ratno KurniawanNo ratings yet
- Biomolecules 10 00389 v2Document19 pagesBiomolecules 10 00389 v2Venansius Ratno KurniawanNo ratings yet
- AboutHydrocephalus-A Book For Families Dec08Document40 pagesAboutHydrocephalus-A Book For Families Dec08rudy.langeNo ratings yet
- Definitions of Intracranial Aneurysm Size and Morphology - A Call For StandardizationDocument7 pagesDefinitions of Intracranial Aneurysm Size and Morphology - A Call For StandardizationVenansius Ratno KurniawanNo ratings yet
- Corticotropinoma (Cushing's Disease)Document2 pagesCorticotropinoma (Cushing's Disease)Venansius Ratno KurniawanNo ratings yet
- Altitude Illness - Risk Factors, Prevention, Presentation, and TreatmentDocument8 pagesAltitude Illness - Risk Factors, Prevention, Presentation, and TreatmentVenansius Ratno KurniawanNo ratings yet
- Cardiovascular Problems in DiversDocument2 pagesCardiovascular Problems in DiversVenansius Ratno KurniawanNo ratings yet
- Risk of Neurological Decompression Sickness in The Diver With A Right-To-Left Shunt - Literature Review and Meta-AnalysisDocument5 pagesRisk of Neurological Decompression Sickness in The Diver With A Right-To-Left Shunt - Literature Review and Meta-AnalysisVenansius Ratno KurniawanNo ratings yet
- Arterial Gas Embolism and DCSDocument6 pagesArterial Gas Embolism and DCSVenansius Ratno KurniawanNo ratings yet
- Cardiovascular Parameter in A Mixed-Sex Swine Study of Severe Dcs Sickness Treated With The Emulsified Perfluorocarbon OxycyteDocument9 pagesCardiovascular Parameter in A Mixed-Sex Swine Study of Severe Dcs Sickness Treated With The Emulsified Perfluorocarbon OxycyteVenansius Ratno KurniawanNo ratings yet
- Pathogenesis of Dengue Viral InfectionsDocument7 pagesPathogenesis of Dengue Viral InfectionsVenansius Ratno KurniawanNo ratings yet
- Biophysical Basis For Inner Ear Decompression SicknessDocument6 pagesBiophysical Basis For Inner Ear Decompression SicknessVenansius Ratno KurniawanNo ratings yet
- An Autopsy Case of Decompression Sickness - Hemorrhages in The Fat Tissue and Fat EmbolismDocument4 pagesAn Autopsy Case of Decompression Sickness - Hemorrhages in The Fat Tissue and Fat EmbolismVenansius Ratno KurniawanNo ratings yet
- Sanofi Pasteur CYD14 Full Results 11 July FINAL enDocument4 pagesSanofi Pasteur CYD14 Full Results 11 July FINAL enVenansius Ratno KurniawanNo ratings yet
- A Case of Decompression Illness During Saturation DivingDocument2 pagesA Case of Decompression Illness During Saturation DivingVenansius Ratno KurniawanNo ratings yet
- Decompression Sickness Treatment: First AidDocument8 pagesDecompression Sickness Treatment: First AidVenansius Ratno KurniawanNo ratings yet
- AKI Due To DCSDocument3 pagesAKI Due To DCSVenansius Ratno KurniawanNo ratings yet
- The Mechanism of Decompression IllnessDocument4 pagesThe Mechanism of Decompression IllnessVenansius Ratno KurniawanNo ratings yet
- Vaccine DengueDocument9 pagesVaccine DengueVenansius Ratno KurniawanNo ratings yet
- Asthma During Pregnancy - Mechanisms and Treatment ImplicationsDocument20 pagesAsthma During Pregnancy - Mechanisms and Treatment ImplicationsVenansius Ratno KurniawanNo ratings yet
- Adenomyosis and ReproductionDocument3 pagesAdenomyosis and ReproductionVenansius Ratno KurniawanNo ratings yet
- EDH Is Surgery Alway Mandatory ?Document6 pagesEDH Is Surgery Alway Mandatory ?Venansius Ratno KurniawanNo ratings yet
- Pathopysiology of AdenomyosisDocument11 pagesPathopysiology of AdenomyosisVenansius Ratno KurniawanNo ratings yet
- What Decides the Outcome of Viral Infection: Host or VirusDocument23 pagesWhat Decides the Outcome of Viral Infection: Host or VirusVenansius Ratno KurniawanNo ratings yet
- Differentiating Dengue Virus Infection From Scrub Typhus in Thai Adults With FeverDocument3 pagesDifferentiating Dengue Virus Infection From Scrub Typhus in Thai Adults With FeverVenansius Ratno KurniawanNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5784)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (72)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Report SampleDocument11 pagesReport SampleArvis ZohoorNo ratings yet
- ......... NCP CaseDocument34 pages......... NCP Casevipnikally80295% (19)
- Wellness massage exam questionsDocument3 pagesWellness massage exam questionsElizabeth QuiderNo ratings yet
- Case Report: Communication Strategies For Empowering and Protecting ChildrenDocument9 pagesCase Report: Communication Strategies For Empowering and Protecting ChildrennabilahNo ratings yet
- Cyclone Shelter Construction Maintenance and Management Policy 2011Document21 pagesCyclone Shelter Construction Maintenance and Management Policy 2011MAHABUBUR RAHAMANNo ratings yet
- BS EN 752-2 Drains & Sewer PDFDocument21 pagesBS EN 752-2 Drains & Sewer PDFsefaz50% (2)
- SGLGB Form 1 Barangay ProfileDocument3 pagesSGLGB Form 1 Barangay ProfileMark Lenon Par Mapaye100% (1)
- SImOS Nano-Tera 2013Document35 pagesSImOS Nano-Tera 2013nanoteraCHNo ratings yet
- Radiographic Cardiopulmonary Changes in Dogs With Heartworm DiseaseDocument8 pagesRadiographic Cardiopulmonary Changes in Dogs With Heartworm DiseaseputriwilujengNo ratings yet
- Gurr2011-Probleme Psihologice Dupa Atac CerebralDocument9 pagesGurr2011-Probleme Psihologice Dupa Atac CerebralPaulNo ratings yet
- MBSR Standards of Practice 2014Document24 pagesMBSR Standards of Practice 2014wasdunichtsagst100% (1)
- A6013 v1 SD Influenza Ag BrochureDocument2 pagesA6013 v1 SD Influenza Ag BrochureYunescka MorenoNo ratings yet
- FreezingDocument59 pagesFreezingManoj Rathod100% (1)
- Handbook of Laboratory Animal Science - Vol IIIDocument319 pagesHandbook of Laboratory Animal Science - Vol IIICarlos AlmeidaNo ratings yet
- Experential and Relationship Oriented Approaches 1Document12 pagesExperential and Relationship Oriented Approaches 1Mary Ann CabalejoNo ratings yet
- Management of Class I Type 3 Malocclusion Using Simple Removable AppliancesDocument5 pagesManagement of Class I Type 3 Malocclusion Using Simple Removable AppliancesMuthia DewiNo ratings yet
- GIGITAN ULAR BERBISA: GEJALA, PENANGANAN DAN JENIS ULAR PALING BERBISADocument19 pagesGIGITAN ULAR BERBISA: GEJALA, PENANGANAN DAN JENIS ULAR PALING BERBISAYudhistira ArifNo ratings yet
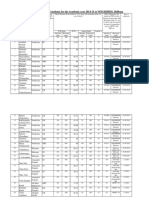
- Admission For 1st Year MBBS Students For The Academic Year 2014-2015Document10 pagesAdmission For 1st Year MBBS Students For The Academic Year 2014-2015Guma KipaNo ratings yet
- Labcorp: Patient ReportDocument4 pagesLabcorp: Patient ReportAsad PrinceNo ratings yet
- Hubungan Pengetahuan Sikap Penderita Penyakit Malaria FalciparumDocument63 pagesHubungan Pengetahuan Sikap Penderita Penyakit Malaria FalciparumEsty GulsanNo ratings yet
- College Women's Experiences With Physically Forced, Alcohol - or Other Drug-Enabled, and Drug-Facilitated Sexual Assault Before and Since Entering CollegeDocument12 pagesCollege Women's Experiences With Physically Forced, Alcohol - or Other Drug-Enabled, and Drug-Facilitated Sexual Assault Before and Since Entering CollegeGlennKesslerWP100% (1)
- 11 - Chapter 7 PDFDocument41 pages11 - Chapter 7 PDFRakesh RakiNo ratings yet
- Drug StudyDocument11 pagesDrug StudyHennah Reblando100% (3)
- As 2550.5-2002 Cranes Hoists and Winches - Safe Use Mobile CranesDocument8 pagesAs 2550.5-2002 Cranes Hoists and Winches - Safe Use Mobile CranesSAI Global - APACNo ratings yet
- Week 6 - LP Modeling ExamplesDocument36 pagesWeek 6 - LP Modeling ExamplesCharles Daniel CatulongNo ratings yet
- Influence of Social Capital On HealthDocument11 pagesInfluence of Social Capital On HealthHobi's Important BusinesseuNo ratings yet
- Wto Unit-2Document19 pagesWto Unit-2Anwar KhanNo ratings yet
- Municipal Ordinance No. 05-2008Document5 pagesMunicipal Ordinance No. 05-2008SBGuinobatan100% (2)
- Design and Estimation of Rain Water Harvesting Scheme in VIVA Institute of TechnologyDocument4 pagesDesign and Estimation of Rain Water Harvesting Scheme in VIVA Institute of TechnologyVIVA-TECH IJRINo ratings yet
- Roberts Race Gender DystopiaDocument23 pagesRoberts Race Gender DystopiaBlythe TomNo ratings yet