You might also like
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Joint ECDC WHO Interim Advice On RCCE For Monkeypox 2 June 2022Document7 pagesJoint ECDC WHO Interim Advice On RCCE For Monkeypox 2 June 2022Francisca BallesterosNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- 2ECDC WHO Risk Communication Community Engagement Monkeypox Outbreak EuropeDocument11 pages2ECDC WHO Risk Communication Community Engagement Monkeypox Outbreak EuropeFrancisca BallesterosNo ratings yet
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Variable Dictionary VaccineTracker-04!11!2021Document3 pagesVariable Dictionary VaccineTracker-04!11!2021Francisca BallesterosNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- 1considerations For Contact Tracing MPX June 2022Document13 pages1considerations For Contact Tracing MPX June 2022Francisca BallesterosNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- ROA Salmonella-Enteritidis-ST11 2022 FinalDocument19 pagesROA Salmonella-Enteritidis-ST11 2022 FinalFrancisca BallesterosNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- 3interim Advice For Public Health Authorities On Summer Events MPXDocument6 pages3interim Advice For Public Health Authorities On Summer Events MPXFrancisca BallesterosNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- 5communicable Disease Threats Report 30 Jul 2022 PublicDocument28 pages5communicable Disease Threats Report 30 Jul 2022 PublicFrancisca BallesterosNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Use of Antibody Tests For SARS COV 2 in The Context of Digital Green CertificatesDocument5 pagesUse of Antibody Tests For SARS COV 2 in The Context of Digital Green CertificatesFrancisca BallesterosNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- COVID 19 in Children and The Role of School Settings in Transmission Second UpdateDocument37 pagesCOVID 19 in Children and The Role of School Settings in Transmission Second UpdateFrancisca BallesterosNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- 2021-01-13 Variable Dictionary and Disclaimer National Weekly DataDocument1 page2021-01-13 Variable Dictionary and Disclaimer National Weekly DataFrancisca BallesterosNo ratings yet
- Interim Public Health Considerations For COVID 19 Vaccination of AdolescentsDocument19 pagesInterim Public Health Considerations For COVID 19 Vaccination of AdolescentsFrancisca BallesterosNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- COVID 19 Considerations For Booster Doses in Adolescents Feb 2022Document14 pagesCOVID 19 Considerations For Booster Doses in Adolescents Feb 2022Francisca BallesterosNo ratings yet
- Description and Disclaimer Daily ReportingDocument1 pageDescription and Disclaimer Daily ReportingFrancisca BallesterosNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- Hiv and Aids: Surveillance ReportDocument7 pagesHiv and Aids: Surveillance ReportFrancisca BallesterosNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Zika Virus Safety of Substances of Human Origin Update 2017 WebDocument35 pagesZika Virus Safety of Substances of Human Origin Update 2017 WebFrancisca BallesterosNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Variable Dictionary VaccineTracker-20-08-2021Document3 pagesVariable Dictionary VaccineTracker-20-08-2021Francisca BallesterosNo ratings yet
- Agenda EAAD - European-Level Launch EventDocument1 pageAgenda EAAD - European-Level Launch EventFrancisca BallesterosNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Antimicrobial Resistance Europe 2015Document120 pagesAntimicrobial Resistance Europe 2015Francisca BallesterosNo ratings yet
- Who Ccsivd Meetingreport SangreDocument31 pagesWho Ccsivd Meetingreport SangreFrancisca BallesterosNo ratings yet
- Communicable Disease Threats Report 16 Jun 2018Document11 pagesCommunicable Disease Threats Report 16 Jun 2018Francisca BallesterosNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Communicable Disease Threats Report 26 Aug 2017Document9 pagesCommunicable Disease Threats Report 26 Aug 2017Francisca BallesterosNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
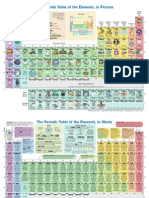
- The Periodic Table of Elements, in PicturesDocument2 pagesThe Periodic Table of Elements, in Picturesrustyy88100% (1)
- Ecdc Infographics2015 Measles Is SeriousDocument1 pageEcdc Infographics2015 Measles Is SeriousFrancisca BallesterosNo ratings yet
- Communicable Disease Threats Report 29 Jul 2017Document13 pagesCommunicable Disease Threats Report 29 Jul 2017Francisca BallesterosNo ratings yet
- ECDC - ECDC Policy Briefing - Preparing For Zika in The EUDocument1 pageECDC - ECDC Policy Briefing - Preparing For Zika in The EUFrancisca BallesterosNo ratings yet
- ECDC Epidemiological SituationDocument1 pageECDC Epidemiological SituationFrancisca BallesterosNo ratings yet
- ECDC - Public Consultation - Expert Opinion On Rotavirus Vaccination in InfancyDocument1 pageECDC - Public Consultation - Expert Opinion On Rotavirus Vaccination in InfancyFrancisca BallesterosNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- ECDC - Systematic Review On Hepatitis B and C Prevalence in The EU-EEADocument1 pageECDC - Systematic Review On Hepatitis B and C Prevalence in The EU-EEAFrancisca BallesterosNo ratings yet
- ECDC Policy BriefingsDocument1 pageECDC Policy BriefingsFrancisca BallesterosNo ratings yet
- ECDC - Examples of Interventions To Manage Tuberculosis in Vulnerable GroupsDocument2 pagesECDC - Examples of Interventions To Manage Tuberculosis in Vulnerable GroupsFrancisca BallesterosNo ratings yet
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)