You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Long-Term Effects of Intensive Glucose Lowering On Cardiovascular OutcomesDocument20 pagesLong-Term Effects of Intensive Glucose Lowering On Cardiovascular OutcomesLutfi MalefoNo ratings yet
- Effects of Medical Therapies On Retinopathy Progression in Type 2 DiabetesDocument12 pagesEffects of Medical Therapies On Retinopathy Progression in Type 2 DiabetesLutfi MalefoNo ratings yet
- "Management Insomnia": Review ArticlesDocument1 page"Management Insomnia": Review ArticlesSri Ulandari A TaufanNo ratings yet
- Chronic Kidney DiseaseDocument16 pagesChronic Kidney DiseaseLutfi MalefoNo ratings yet
- Pi Is 0190962209008214Document1 pagePi Is 0190962209008214Lutfi MalefoNo ratings yet
- DKA ManagementDocument7 pagesDKA ManagementbababrijeshNo ratings yet
- PutriDocument15 pagesPutriHusni IrchyNo ratings yet
- Anemia in CHF PDFDocument10 pagesAnemia in CHF PDFLutfi MalefoNo ratings yet
- "Management Insomnia": Review ArticlesDocument1 page"Management Insomnia": Review ArticlesSri Ulandari A TaufanNo ratings yet
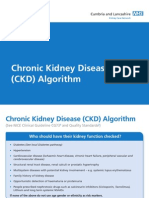
- CKD Assessment AlgorithmDocument2 pagesCKD Assessment AlgorithmLutfi MalefoNo ratings yet
- Edema ParuDocument34 pagesEdema ParuLutfi MalefoNo ratings yet
- CKD Pocket GuideDocument2 pagesCKD Pocket GuideLutfi MalefoNo ratings yet
- Jemi D.atopikDocument8 pagesJemi D.atopikLutfi MalefoNo ratings yet
- Jurnal 4Document7 pagesJurnal 4Lutfi MalefoNo ratings yet
- Treatment of Seborrheic Dermatitis: The Efficiency of Sertaconazole 2% Cream vs. Tacrolimus 0.03% CreamDocument5 pagesTreatment of Seborrheic Dermatitis: The Efficiency of Sertaconazole 2% Cream vs. Tacrolimus 0.03% CreamLutfi MalefoNo ratings yet
- Jemi D.atopikDocument8 pagesJemi D.atopikLutfi MalefoNo ratings yet
- Jurnal PsikiatriDocument7 pagesJurnal PsikiatriLutfi MalefoNo ratings yet
- Jurnal 4Document7 pagesJurnal 4Lutfi MalefoNo ratings yet
- Jurnal 1Document9 pagesJurnal 1Lutfi MalefoNo ratings yet
- Jurnal 1Document9 pagesJurnal 1Lutfi MalefoNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Rutter's Child and Adolescent Psychiatry PDF - Căutare GoogleDocument1 pageRutter's Child and Adolescent Psychiatry PDF - Căutare GoogleMihaela EvaNo ratings yet
- Schizoaffective Disorder in The DSM 5 PDFDocument5 pagesSchizoaffective Disorder in The DSM 5 PDFpipiitopandabamboo247No ratings yet
- Delusional Disorder - An OverviewDocument12 pagesDelusional Disorder - An Overviewdrrlarry100% (1)
- Mental Health: PDHPE Stage 5 Lesson PlanDocument24 pagesMental Health: PDHPE Stage 5 Lesson Planapi-298566801No ratings yet
- 3-курс №4Document3 pages3-курс №4НургулNo ratings yet
- FAKTOR SOSIO EKONOMI PADA PENYALAHGUNAAN NAPZA DI KALANGAN REMAJADocument11 pagesFAKTOR SOSIO EKONOMI PADA PENYALAHGUNAAN NAPZA DI KALANGAN REMAJAsetyanhariNo ratings yet
- Understanding Bipolar DisorderDocument24 pagesUnderstanding Bipolar DisorderdoscribeNo ratings yet
- Differential Diagnosis and Management of HallucinationsDocument6 pagesDifferential Diagnosis and Management of HallucinationsHipsipilasNo ratings yet
- Emergency Psych Referrals in Teaching HospitalDocument4 pagesEmergency Psych Referrals in Teaching Hospitalsubham kumarNo ratings yet
- Human BehaviorDocument5 pagesHuman Behaviorjetlee estacionNo ratings yet
- Binge Eating Scale: Brief DescriptionDocument3 pagesBinge Eating Scale: Brief DescriptionBrîndușaPetcariuNo ratings yet
- Stages of Addiction from Experimentation to Full DependencyDocument1 pageStages of Addiction from Experimentation to Full DependencyHuy PhamNo ratings yet
- 9 Tips for Communicating with Individuals on the Autism SpectrumDocument5 pages9 Tips for Communicating with Individuals on the Autism SpectrumSweet'nSpicy LabNo ratings yet
- Research Essay Final OutlineDocument7 pagesResearch Essay Final Outlineapi-251704489No ratings yet
- Speech Outline Mental IllnessDocument5 pagesSpeech Outline Mental IllnessMiss D79% (19)
- Violence Risk Assessment Part IDocument9 pagesViolence Risk Assessment Part IBZia135100% (1)
- Therapy for NPD SufferersDocument8 pagesTherapy for NPD SufferershopeIshanzaNo ratings yet
- Beck Youth Inventories™ - Second Edition (BYI™-II)Document2 pagesBeck Youth Inventories™ - Second Edition (BYI™-II)Sana Khan50% (2)
- PsychopathologyDocument86 pagesPsychopathologyLouieAmadoGutierrezNo ratings yet
- Creativity in Persons At-Risk For Bipolar Disorder - A Pilot StudyDocument8 pagesCreativity in Persons At-Risk For Bipolar Disorder - A Pilot Studysonia498No ratings yet
- Substance AbuseDocument15 pagesSubstance AbuseDivij SaxenaNo ratings yet
- Case Study-1 Personality Psychology About This Assignment: Questions For DiscussionDocument6 pagesCase Study-1 Personality Psychology About This Assignment: Questions For DiscussionLakshmi NarayanaNo ratings yet
- The Aftermath of Trauma: Nadya Natasha - A11180004Document3 pagesThe Aftermath of Trauma: Nadya Natasha - A11180004NadNo ratings yet
- Brief Intensive CBT For Pediatric OCD With E Therapy Maintenance - Farrell 2016 PDFDocument10 pagesBrief Intensive CBT For Pediatric OCD With E Therapy Maintenance - Farrell 2016 PDFLaura HdaNo ratings yet
- Sleep-Wake Disorders Fact Sheet PDFDocument2 pagesSleep-Wake Disorders Fact Sheet PDFAle M. MartinezNo ratings yet
- Study of thoughts, feelings and behaviour in forensic psychologyDocument2 pagesStudy of thoughts, feelings and behaviour in forensic psychologyRiley TudorNo ratings yet
- Seeking SafetyDocument17 pagesSeeking Safetyapi-24985177880% (5)
- Psychology Disorders Terms Worksheet PDFDocument2 pagesPsychology Disorders Terms Worksheet PDF12345678user100% (1)
- Psych Nursing LectureDocument448 pagesPsych Nursing LectureCherry Ann Garcia DuranteNo ratings yet
- Nca - Psychiatric NursingDocument416 pagesNca - Psychiatric NursingJemimah A. MangalindanNo ratings yet