You might also like
- Utmc - Utoledo.edu Depts Nursing Pdfs Basic EKG RefresherDocument210 pagesUtmc - Utoledo.edu Depts Nursing Pdfs Basic EKG RefresherTrish HồNo ratings yet
- ACLS Answer KeyDocument23 pagesACLS Answer KeyKirana Budhiarta94% (17)
- 2020 AHA Guidelines For CPR & ECCDocument42 pages2020 AHA Guidelines For CPR & ECCArun100% (1)
- ACCSAP 10 .PDF Version 1Document470 pagesACCSAP 10 .PDF Version 1Adeel Lakhiar100% (9)
- Adult Advanced Life Support: Resuscitation Council (UK)Document23 pagesAdult Advanced Life Support: Resuscitation Council (UK)Masuma SarkerNo ratings yet
- FREE 2022 ACLS Study Guide - ACLS Made Easy! PDFDocument18 pagesFREE 2022 ACLS Study Guide - ACLS Made Easy! PDFkumar23No ratings yet
- Emergency Cart ProcedureDocument20 pagesEmergency Cart ProcedureAyiessa_AJNo ratings yet
- BLS For Healthcare Providers Student ManualDocument2 pagesBLS For Healthcare Providers Student ManualdrsmiNo ratings yet
- Advanced Cardiovascular Life Support (ACLS)Document27 pagesAdvanced Cardiovascular Life Support (ACLS)Sara Ali100% (3)
- Guidelines Adult Advanced Life SupportDocument34 pagesGuidelines Adult Advanced Life SupportParvathy R NairNo ratings yet
- From MedscapeCME Clinical BriefsDocument4 pagesFrom MedscapeCME Clinical Briefssraji64No ratings yet
- Guidelines Adult Advanced Life SupportDocument35 pagesGuidelines Adult Advanced Life SupportindahNo ratings yet
- ACLS DrugsDocument4 pagesACLS DrugsEduard Espeso Chiong-Gandul Jr.No ratings yet
- Cardiopulmonary ResuscitationDocument3 pagesCardiopulmonary ResuscitationLee Liang Lee LiangNo ratings yet
- Basic Life Support and Advanced Cardiovascular Life SupportDocument90 pagesBasic Life Support and Advanced Cardiovascular Life SupportRakhshanda khan100% (1)
- CAB-CPR UpdateDocument15 pagesCAB-CPR Updatedragon66No ratings yet
- BLS & AclsDocument13 pagesBLS & AclsadamNo ratings yet
- In-Hospital AlsDocument10 pagesIn-Hospital AlsCzarian Estillore HigoyNo ratings yet
- Unit 5 Cardiac Emergencies: StructureDocument27 pagesUnit 5 Cardiac Emergencies: StructurebtaleraNo ratings yet
- Basic Life SupportDocument34 pagesBasic Life SupportEveline FebrinaNo ratings yet
- The FourDocument22 pagesThe FourInatul AuliaNo ratings yet
- Civic Welfare Training ServiceDocument13 pagesCivic Welfare Training ServiceVanessa Rose RofloNo ratings yet
- Basic Life SupportDocument6 pagesBasic Life SupportbhongskirnNo ratings yet
- Basic Cardiac Life Support 2011Document6 pagesBasic Cardiac Life Support 2011Tashfeen Bin NazeerNo ratings yet
- Basic Life Support: Submitted By: Kennedy V. Velasco Bscrim 1-AlphaDocument7 pagesBasic Life Support: Submitted By: Kennedy V. Velasco Bscrim 1-AlphaProsperJuan BelieversNo ratings yet
- Guidelines - In-Hospital ResuscitationDocument18 pagesGuidelines - In-Hospital ResuscitationparuNo ratings yet
- Advanced Life Support-RESSU CouncilDocument30 pagesAdvanced Life Support-RESSU CouncilGigel DumitruNo ratings yet
- The Rules and Changes: ACLS Guidelines 2010Document81 pagesThe Rules and Changes: ACLS Guidelines 2010Annisa Rizki Ratih PratiwiNo ratings yet
- ACLS and MegacodeDocument33 pagesACLS and MegacodeMark Joseph100% (1)
- ACLS Online Training Material: Unit One: General ConceptsDocument34 pagesACLS Online Training Material: Unit One: General ConceptsJohn JenjinsNo ratings yet
- Cardiopulmonary Resuscitation 2015Document31 pagesCardiopulmonary Resuscitation 2015Clarissa Maya TjahjosarwonoNo ratings yet
- Cardiopulmonary ResuscitationDocument10 pagesCardiopulmonary ResuscitationLilay MakulayNo ratings yet
- ACLS II Sept 25 StudentsDocument60 pagesACLS II Sept 25 StudentsLex CatNo ratings yet
- Bls - Acls Update American Heart Association 2020: Ns. Anastasia Hardyati., Mkep., Sp. KMBDocument26 pagesBls - Acls Update American Heart Association 2020: Ns. Anastasia Hardyati., Mkep., Sp. KMBcelvin sohilait100% (1)
- BLS & ACLS Survey 22012021Document17 pagesBLS & ACLS Survey 22012021Muhammad RezaNo ratings yet
- Acls 2015Document9 pagesAcls 2015Andy PrasetyoNo ratings yet
- UntitledDocument11 pagesUntitledAnkita BramheNo ratings yet
- Basic Life Support (BLS) Primary Survey For Respiratory ArrestDocument6 pagesBasic Life Support (BLS) Primary Survey For Respiratory ArrestRifqi MuhammadNo ratings yet
- Adult Advanced Life SupportDocument14 pagesAdult Advanced Life SupportAnonymous TT7aEIjhuhNo ratings yet
- WHATs New in CPCRDocument4 pagesWHATs New in CPCRJessicaHernandezNo ratings yet
- CPR - Cardiopulmonary ResuscitationDocument31 pagesCPR - Cardiopulmonary ResuscitationPanji HerlambangNo ratings yet
- Wsava - Fecava - Bsava World Congress 2012 - VinDocument8 pagesWsava - Fecava - Bsava World Congress 2012 - Vinkuriakosejane6No ratings yet
- Cardiopulmonary Resuscitation (CPR)Document21 pagesCardiopulmonary Resuscitation (CPR)Cristy Guzman100% (1)
- Respi MVDocument25 pagesRespi MVtimie_reyesNo ratings yet
- Acls Course HandoutsDocument8 pagesAcls Course HandoutsRoxas CedrickNo ratings yet
- CPR in HospitalDocument9 pagesCPR in Hospitalrajnishpathak648No ratings yet
- Cardiac Arrest 191108Document9 pagesCardiac Arrest 191108anita tri hastutiNo ratings yet
- ACLSDocument39 pagesACLSJason LiandoNo ratings yet
- ACLS PEA Asystole AlgorithmDocument3 pagesACLS PEA Asystole AlgorithmSafira RNo ratings yet
- BHJD Dan BHJLDocument23 pagesBHJD Dan BHJLSyukran AbNo ratings yet
- AlsDocument4 pagesAlsFaraaz KhanNo ratings yet
- Pals 2011Document21 pagesPals 2011Saúl Chilón71% (14)
- Using The ACLS Primary Survey For A Patient in Respiratory ArrestDocument34 pagesUsing The ACLS Primary Survey For A Patient in Respiratory Arrest강기연100% (1)
- RACE 2017 MegacodeDocument33 pagesRACE 2017 MegacodemickeyNo ratings yet
- Basic Life SupportDocument4 pagesBasic Life Supportraven_claw25No ratings yet
- Cardiopulmonar Y ResuscitationDocument34 pagesCardiopulmonar Y ResuscitationRatuSitiKhadijahSarahNo ratings yet
- Cardiac ArrestDocument30 pagesCardiac ArrestagnescheruseryNo ratings yet
- 2015 NRP 7th Edition Primer PDFDocument4 pages2015 NRP 7th Edition Primer PDFWipaporn ChaengsriNo ratings yet
- Basic and Advanced Cardiac Life Support: What's New?Document6 pagesBasic and Advanced Cardiac Life Support: What's New?frakturhepatikaNo ratings yet
- Review of Respiratory ArrestDocument2 pagesReview of Respiratory ArrestsrimatsimhasaneshwarNo ratings yet
- Paediatric Advanced Life Support GuidelinesDocument31 pagesPaediatric Advanced Life Support GuidelinesEXODUSGENNo ratings yet
- UP DA TE CP R 20 15: Prof. Dr. Achsanuddin Hanafie, SP - An, KIC, KAO Dept. Anestesiologi Dan Terapi Intensif FK-USUDocument37 pagesUP DA TE CP R 20 15: Prof. Dr. Achsanuddin Hanafie, SP - An, KIC, KAO Dept. Anestesiologi Dan Terapi Intensif FK-USUAndrias OzNo ratings yet
- Essentials in Lung TransplantationFrom EverandEssentials in Lung TransplantationAllan R. GlanvilleNo ratings yet
- Advanced Cardiac Life Support Quick Study Guide 2015 Updated GuidelinesFrom EverandAdvanced Cardiac Life Support Quick Study Guide 2015 Updated GuidelinesRating: 4 out of 5 stars4/5 (6)
- Pediatric Advanced Life Support Quick Study Guide 2015 Updated GuidelinesFrom EverandPediatric Advanced Life Support Quick Study Guide 2015 Updated GuidelinesRating: 5 out of 5 stars5/5 (2)
- Paskariatne Probo - Simple Approach To Peri Operative HypertensionDocument42 pagesPaskariatne Probo - Simple Approach To Peri Operative HypertensionCupit NubillisNo ratings yet
- Early Warning Scores PDFDocument14 pagesEarly Warning Scores PDFjuliansyahjuventusNo ratings yet
- Paralisis DiafragmaDocument1 pageParalisis DiafragmaCupit NubillisNo ratings yet
- PPCMDocument16 pagesPPCMCupit Nubillis100% (1)
- User Manual KED PRO Eng PDFDocument35 pagesUser Manual KED PRO Eng PDFCupit NubillisNo ratings yet
- Diagnosis and Management of CPVTDocument6 pagesDiagnosis and Management of CPVTCupit NubillisNo ratings yet
- Path FlowDocument1 pagePath FlowCupit NubillisNo ratings yet
- Dysrhythmias: Normal Electrical ActivityDocument32 pagesDysrhythmias: Normal Electrical ActivityLarisse de LeonNo ratings yet
- Nursing 202: Module B Cardiovascular System AlterationsDocument121 pagesNursing 202: Module B Cardiovascular System AlterationssenthilmnurseNo ratings yet
- ACLS DrugDocument7 pagesACLS DrugPhongsatorn Thunin100% (1)
- Superimposed ECG PDFDocument93 pagesSuperimposed ECG PDFEdalyn CapiliNo ratings yet
- MP 20-30-40!50!60 70 90 Rel. B.1 IntelliVue Patient Monitor - Configuration ... PDF Nodeid 584073&vernum 1Document130 pagesMP 20-30-40!50!60 70 90 Rel. B.1 IntelliVue Patient Monitor - Configuration ... PDF Nodeid 584073&vernum 1Juan AmaroNo ratings yet
- AclsDocument39 pagesAclstrianaamaliaNo ratings yet
- Ebook Current Diagnosis and Treatment Cardiology 5Th Edition PDF Full Chapter PDFDocument67 pagesEbook Current Diagnosis and Treatment Cardiology 5Th Edition PDF Full Chapter PDFbeth.hao417100% (31)
- Er WorksheetsDocument26 pagesEr WorksheetsThelda Mae Arteche SablanNo ratings yet
- Local Anesthetics - Blockers K+ Channel Blockers Ca2+ Channel BlockersDocument4 pagesLocal Anesthetics - Blockers K+ Channel Blockers Ca2+ Channel Blockersmed testNo ratings yet
- Management of Perioperative ArrhythmiasDocument15 pagesManagement of Perioperative Arrhythmiaszuraini_mdnoorNo ratings yet
- Ati - RN Comprehensive Predictor 2023 RemediationDocument21 pagesAti - RN Comprehensive Predictor 2023 Remediationseansdrew2No ratings yet
- Incessant VT VFDocument9 pagesIncessant VT VFTor JaNo ratings yet
- Abstract Book INAACCDocument83 pagesAbstract Book INAACCrodtobingNo ratings yet
- Arrhythmias PDFDocument29 pagesArrhythmias PDFbencleeseNo ratings yet
- Management of Cardiac ArrestDocument40 pagesManagement of Cardiac ArrestMark Francis NaniaNo ratings yet
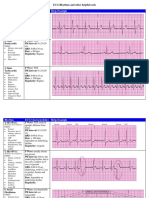
- Rhythm ECG Characteristics Strip Example: ECG Rhythms and Other Helpful ToolsDocument6 pagesRhythm ECG Characteristics Strip Example: ECG Rhythms and Other Helpful ToolsJohnildy MatiasNo ratings yet
- Cardiovascular MCQs LJDocument11 pagesCardiovascular MCQs LJYanis Yan100% (1)
- Questions & Answers: CardiologyDocument77 pagesQuestions & Answers: CardiologyDev Yadav100% (1)
- CardiacArrhythmiasPathophysiology PDFDocument1 pageCardiacArrhythmiasPathophysiology PDFNeelam Raj ThakurNo ratings yet
- 2020 Canadian Cardiovascular SocietyCanadian Heart Rhythm Society Position Statement On The Management of Ventricular Tachycardia and Fibrillation in Patients With Structural Heart Disease PDFDocument15 pages2020 Canadian Cardiovascular SocietyCanadian Heart Rhythm Society Position Statement On The Management of Ventricular Tachycardia and Fibrillation in Patients With Structural Heart Disease PDFDiego MerchánNo ratings yet
- Ventricular Tachycardia Bsn3b-Grp1Document35 pagesVentricular Tachycardia Bsn3b-Grp1Jessica RamosNo ratings yet
- ACLS AlgorithmDocument12 pagesACLS AlgorithmwildionNo ratings yet
- Morgan 2012Document5 pagesMorgan 2012aixacamila3No ratings yet
- Advanced Cardiac Life Support (ACLS)Document17 pagesAdvanced Cardiac Life Support (ACLS)Siti Rahima HarahapNo ratings yet
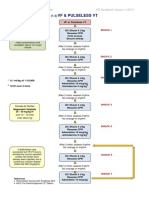
- VF & Pulseless VTDocument1 pageVF & Pulseless VTmadimadi11No ratings yet
- Admitting OrdersDocument4 pagesAdmitting OrdersRommel OliverasNo ratings yet