You might also like
- CCRN ReviewDocument22 pagesCCRN ReviewMelissaDavis71% (7)
- Cardiovascular Anatomy and PhysiologyDocument28 pagesCardiovascular Anatomy and PhysiologyLouise Mica Lee100% (1)
- Cardiovascular System ReviewDocument9 pagesCardiovascular System ReviewsenjicsNo ratings yet
- Lecture 3 Cardiovascular System 1Document54 pagesLecture 3 Cardiovascular System 1hafiz patah100% (1)
- The HeartDocument59 pagesThe Heartapi-26587879No ratings yet
- 6th Central Pay Commission Salary CalculatorDocument15 pages6th Central Pay Commission Salary Calculatorrakhonde100% (436)
- Functional organization of the cardiovascular systemDocument19 pagesFunctional organization of the cardiovascular systemIbtesam Mohammed100% (2)
- Session 29 Foods To Fill The Energy GapDocument24 pagesSession 29 Foods To Fill The Energy Gapapi-19824701No ratings yet
- 1118 Electrical Injuries EMPDocument20 pages1118 Electrical Injuries EMPAbog Luis Guillermo Andrade FloresNo ratings yet
- The Heart: Anatomy, Chambers, Circulation & ValvesDocument14 pagesThe Heart: Anatomy, Chambers, Circulation & ValvesGary Bowen100% (1)
- Evolution of the Circulatory System: From Unicellular to MammalsDocument16 pagesEvolution of the Circulatory System: From Unicellular to MammalsSaajid AmraNo ratings yet
- PHYSIOLOGY OF THE CARDIOVASCULAR SYSTEMDocument92 pagesPHYSIOLOGY OF THE CARDIOVASCULAR SYSTEMSanti Purnama SariNo ratings yet
- The Circulatory System: Agriscience 332 Animal Science #8646-A TEKS: (C) (2) (A) and (C) (2) (B)Document111 pagesThe Circulatory System: Agriscience 332 Animal Science #8646-A TEKS: (C) (2) (A) and (C) (2) (B)brdaisyNo ratings yet
- Circulatory System: A Tutorial Study GuideFrom EverandCirculatory System: A Tutorial Study GuideRating: 5 out of 5 stars5/5 (3)
- Blood Vessels CirculationDocument11 pagesBlood Vessels CirculationChrisjohn Aster OsioNo ratings yet
- Heart Anatomy & Physiology GuideDocument56 pagesHeart Anatomy & Physiology Guidepreet kaurNo ratings yet
- Cardiac PhysiologyDocument102 pagesCardiac PhysiologyPeter Larsen100% (1)
- Management of The Sick Young Infant Age 1 Week Up To 2 MonthsDocument5 pagesManagement of The Sick Young Infant Age 1 Week Up To 2 Monthsapi-19824701No ratings yet
- CardiovascularDocument92 pagesCardiovascularRolinette DaneNo ratings yet
- Circulatory SystemDocument111 pagesCirculatory SystemYounas Bhatti100% (1)
- Internal Medicine Clinical Treatment Guidelines 9-10-2012 1Document264 pagesInternal Medicine Clinical Treatment Guidelines 9-10-2012 1ursula_ursulaNo ratings yet
- Pediatric Nursing Reviewer CardiovascularDocument4 pagesPediatric Nursing Reviewer CardiovascularnieacatleyaNo ratings yet
- Sample Exam Questions - Nuclear Medicine Technology Certification BoardDocument6 pagesSample Exam Questions - Nuclear Medicine Technology Certification BoardClauzi Rodrigo Guerini100% (3)
- Session 30 Foods To Fill The Iron and Vit A GapDocument34 pagesSession 30 Foods To Fill The Iron and Vit A Gapapi-19824701No ratings yet
- Anatomy and Physiology of HeartDocument69 pagesAnatomy and Physiology of HeartRitu Arun Kaushik100% (1)
- ANP Heart Anatomy & PhysiologyDocument3 pagesANP Heart Anatomy & PhysiologySheana Tmpl100% (1)
- 2023 UHS MDCAT Vocab 843 Words by SLMN GrammarDocument79 pages2023 UHS MDCAT Vocab 843 Words by SLMN Grammarjamil ahmedNo ratings yet
- B.Sc. MIT Revised CurriculumDocument76 pagesB.Sc. MIT Revised CurriculumGouspeer MNo ratings yet
- Wolf's AmnesiaDocument10 pagesWolf's AmnesiaJo AnneNo ratings yet
- HeartDocument72 pagesHeartfyzanfroshie100% (1)
- COMMUNITY AND MEDICAL HEALTH NURSING QUESTIONSDocument6 pagesCOMMUNITY AND MEDICAL HEALTH NURSING QUESTIONSJonathan Agcaoili KupahuNo ratings yet
- The Heart's Chambers and ValvesDocument29 pagesThe Heart's Chambers and ValvesomarNo ratings yet
- Chapter 13 - HeartDocument5 pagesChapter 13 - Heartbussniesm05No ratings yet
- Heart Anatomy GuideDocument7 pagesHeart Anatomy GuideKaryll AguilaNo ratings yet
- Heart .Which Divides Right and Left, Structures of TheDocument5 pagesHeart .Which Divides Right and Left, Structures of Thecabas114No ratings yet
- ССС 2019Document83 pagesССС 2019bekafop813No ratings yet
- Week Objectives 1-5Document295 pagesWeek Objectives 1-5qvqck4zmnnNo ratings yet
- 7.8.heart and VesselsDocument11 pages7.8.heart and Vesselssomebody_maNo ratings yet
- Cardiovascular System LectureDocument5 pagesCardiovascular System LectureMarci MunirNo ratings yet
- Acfrogb 7ik4ojriyfu8nvvwmohozvp1pcb2hjyh47jdwvhnpmnhiyornnhy - Xeyhodxnx4wlzdu5sc59 1gvhetgkpoh5ws31c2bftcevdfose32075g4qf78x9c08Document60 pagesAcfrogb 7ik4ojriyfu8nvvwmohozvp1pcb2hjyh47jdwvhnpmnhiyornnhy - Xeyhodxnx4wlzdu5sc59 1gvhetgkpoh5ws31c2bftcevdfose32075g4qf78x9c08Bala GanapathyNo ratings yet
- Anatomy Lec.6Document5 pagesAnatomy Lec.6aminqasm111No ratings yet
- THE HEART HandoutDocument61 pagesTHE HEART HandoutMitha PelangiNo ratings yet
- Anatomy and Histology of The Cardiovascular SystemDocument16 pagesAnatomy and Histology of The Cardiovascular SystemTasmiah HossainNo ratings yet
- HUMAN ANATOMY AND PHYSIOLOGY LABORATORY Cardiovascular SystemDocument12 pagesHUMAN ANATOMY AND PHYSIOLOGY LABORATORY Cardiovascular SystemZaira MangalimanNo ratings yet
- Oral RevDocument6 pagesOral RevjjolaguerNo ratings yet
- Cardiovascular PBLsDocument8 pagesCardiovascular PBLsAya SobhiNo ratings yet
- The Cardiovascular To MhsDocument25 pagesThe Cardiovascular To MhsikuwageNo ratings yet
- Anatomy and Physiolog1Document5 pagesAnatomy and Physiolog1Isabel Barredo Del MundoNo ratings yet
- Transport in Invertebrates and VertebratesDocument13 pagesTransport in Invertebrates and VertebratesJoan GalarceNo ratings yet
- Structure and Function of The Cardiovascular System PDFDocument9 pagesStructure and Function of The Cardiovascular System PDFteuuuuNo ratings yet
- 5053922cardiovascular SystemDocument7 pages5053922cardiovascular SystemHasham AhmadNo ratings yet
- Heart: Size, Form, and Location: Cardiovascular SystemDocument3 pagesHeart: Size, Form, and Location: Cardiovascular Systemskyler andradaNo ratings yet
- Common Cardiac Anomalies Seen Within The Cardiac Catheterization LabDocument23 pagesCommon Cardiac Anomalies Seen Within The Cardiac Catheterization Labapi-356406300No ratings yet
- CVSDocument184 pagesCVStee su lingNo ratings yet
- (Lecture 7) The Cardiovascular, Respiratory and Lymphatic SystemDocument32 pages(Lecture 7) The Cardiovascular, Respiratory and Lymphatic SystemKasraSrNo ratings yet
- Cardiology: Patent LumenDocument5 pagesCardiology: Patent LumenDeepthi VallabhaneniNo ratings yet
- Anatomy of The HeartDocument5 pagesAnatomy of The HeartxXjhmXxNo ratings yet
- Circulatory System FKM'12Document55 pagesCirculatory System FKM'12muhammadsudrajadNo ratings yet
- CardiovascularDocument7 pagesCardiovascularapi-294104473No ratings yet
- Anatomy and Physiology of the Cardiovascular SystemDocument64 pagesAnatomy and Physiology of the Cardiovascular SystemMathews showsNo ratings yet
- Internal Striucture of HeartDocument2 pagesInternal Striucture of HeartDhilahHarfaDhilahNo ratings yet
- Anatomi Pembuluh Darah KoronerDocument36 pagesAnatomi Pembuluh Darah KoronerenriNo ratings yet
- Vessels and CirculationDocument67 pagesVessels and CirculationTio UgantoroNo ratings yet
- Anatomy and Physiology of The HeartDocument8 pagesAnatomy and Physiology of The HeartJoan Devera100% (1)
- Cardiovascular Physiology Guide by Dr. Ahlam KadhimDocument7 pagesCardiovascular Physiology Guide by Dr. Ahlam KadhimEhab Alaa Abd Al-AmeerNo ratings yet
- WEEK 1 MEDSURG AsynchDocument12 pagesWEEK 1 MEDSURG AsynchLeigh Angelika Dela CruzNo ratings yet
- Cardiac - Lect 1Document14 pagesCardiac - Lect 1كسلان اكتب اسميNo ratings yet
- Angiology Lecture 2Document5 pagesAngiology Lecture 2আহানাফ তাহমিদ শব্দNo ratings yet
- Heart AnatomyDocument19 pagesHeart Anatomydeepika kushwahNo ratings yet
- V. Trachea: Zoology-IIDocument22 pagesV. Trachea: Zoology-IIVenkatesh JoguNo ratings yet
- Management of Clients With Problems of The Cardiovascular SystemDocument7 pagesManagement of Clients With Problems of The Cardiovascular Systemjerry smatt dumtoNo ratings yet
- القلبDocument11 pagesالقلبNajwa AbdualgaderNo ratings yet
- Cardiovascular Sys Part 1Document10 pagesCardiovascular Sys Part 1LawrenceNo ratings yet
- Anatomy and Physiology of The Heart Made Easy Part 1Document22 pagesAnatomy and Physiology of The Heart Made Easy Part 1adedayodavid860No ratings yet
- The Endocrine System: B. Pimentel, M.D. University of Makati College of NursingDocument54 pagesThe Endocrine System: B. Pimentel, M.D. University of Makati College of Nursingapi-19824701100% (1)
- The Muscular System: B. Pimentel, M.D. University of Makati - College of NursingDocument71 pagesThe Muscular System: B. Pimentel, M.D. University of Makati - College of Nursingapi-19824701No ratings yet
- Digestive SystemDocument121 pagesDigestive Systemapi-19824701100% (1)
- Session 25 Health Care PracticesDocument43 pagesSession 25 Health Care Practicesapi-19824701No ratings yet
- Endocrine ImagesDocument103 pagesEndocrine Imagesapi-19824701No ratings yet
- Session 20 Breast Conditions-fINALDocument31 pagesSession 20 Breast Conditions-fINALapi-19824701No ratings yet
- The Cell and Its FunctionDocument69 pagesThe Cell and Its Functionapi-19824701No ratings yet
- Philippine Code of Marketing of Breastmilk Substitutes (Executive Order 51)Document26 pagesPhilippine Code of Marketing of Breastmilk Substitutes (Executive Order 51)api-19824701No ratings yet
- Be It Enacted by The Senate and House of Representatives of The Philippines in Congress AssembledDocument25 pagesBe It Enacted by The Senate and House of Representatives of The Philippines in Congress Assembledapi-19824701No ratings yet
- Session 17 HIV OverviewDocument20 pagesSession 17 HIV Overviewapi-19824701No ratings yet
- Yosi BoyDocument55 pagesYosi Boyapi-19824701No ratings yet
- Session 4 Assessing A BreastfeedDocument9 pagesSession 4 Assessing A Breastfeedapi-19824701No ratings yet
- Session 3 How BF WorksDocument33 pagesSession 3 How BF Worksapi-19824701No ratings yet
- Session 15 Expressing BMDocument34 pagesSession 15 Expressing BMapi-19824701No ratings yet
- The Philippine NUrsing Act of 2002 Aka R.A. 9173Document7 pagesThe Philippine NUrsing Act of 2002 Aka R.A. 9173Rho Vince Caño MalagueñoNo ratings yet
- Republic of The PhilippinesDocument6 pagesRepublic of The Philippinesapi-19824701No ratings yet
- An Introduction To Infant and Young Child FeedingDocument15 pagesAn Introduction To Infant and Young Child Feedingapi-19824701No ratings yet
- PD603 - Child - Youth WelfareDocument7 pagesPD603 - Child - Youth Welfareapi-19824701100% (1)
- Ra 7160 PDFDocument259 pagesRa 7160 PDFFrederick Barillo83% (6)
- Philippines Annex3 Packaging and Advertising2003Document14 pagesPhilippines Annex3 Packaging and Advertising2003genellemaarteNo ratings yet
- Session 2 Why BF Is ImptDocument14 pagesSession 2 Why BF Is Imptapi-19824701No ratings yet
- PD996 Compulsory ImzDocument2 pagesPD996 Compulsory Imzapi-19824701No ratings yet
- FamilywithpicsDocument26 pagesFamilywithpicsapi-19824701No ratings yet
- RA6365 PopcomDocument4 pagesRA6365 Popcomapi-19824701No ratings yet
- Creating A National Nutrition Council and For Other PurposesDocument4 pagesCreating A National Nutrition Council and For Other Purposesapi-19824701No ratings yet
- Conduction System of The Heart PPT 2Document12 pagesConduction System of The Heart PPT 2leigh angelaNo ratings yet
- Study ProtocolDocument18 pagesStudy ProtocolTirthesh PatelNo ratings yet
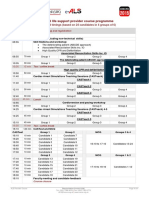
- E-ALS Programme IO ARS (March 2016)Document1 pageE-ALS Programme IO ARS (March 2016)Florentina GasttiNo ratings yet
- 5 Step EKG InterpretationDocument1 page5 Step EKG InterpretationSibel ErtuğrulNo ratings yet
- Yr 9 PASS The Body in Action PowerpointDocument77 pagesYr 9 PASS The Body in Action PowerpointKellie GuestNo ratings yet
- E363 FullDocument4 pagesE363 FullRamadhyanNo ratings yet
- Evaluation of The Relationship Between Peripheral Pulse Palpation and Doppler Systolic Blood Pressure in Dogs Presenting To An Emergency ServiceDocument6 pagesEvaluation of The Relationship Between Peripheral Pulse Palpation and Doppler Systolic Blood Pressure in Dogs Presenting To An Emergency ServiceYissette Bautista CarrilloNo ratings yet
- Answer Key-Health & Skill Related FitnessDocument3 pagesAnswer Key-Health & Skill Related Fitnessking ryan angelo jasperNo ratings yet
- Millers Anesthesia - Sixth Edition - Chapter 66 - Anesthesia For Robotic Surgery - 233Document44 pagesMillers Anesthesia - Sixth Edition - Chapter 66 - Anesthesia For Robotic Surgery - 233Adriana VickNo ratings yet
- Cardiovascular System: Blood Vessels and Circulation: Student Learning OutcomesDocument10 pagesCardiovascular System: Blood Vessels and Circulation: Student Learning Outcomeslily1liang-1No ratings yet
- Steps of CPR ProcedureDocument8 pagesSteps of CPR ProcedureKrupa Jyothi PerumallaNo ratings yet
- This Is No Way To Treat An Aorta.: Edwards EZ Glide Aortic CannulaDocument5 pagesThis Is No Way To Treat An Aorta.: Edwards EZ Glide Aortic CannulaAhmadNo ratings yet
- V.Sowndharya MeeraDocument22 pagesV.Sowndharya MeeraGopi NathNo ratings yet
- Organ Systems Practice TestDocument8 pagesOrgan Systems Practice TestChristine RomanillosNo ratings yet
- Newborn Pulmonary Hypertension Causes and TreatmentDocument10 pagesNewborn Pulmonary Hypertension Causes and TreatmentWali MoralesNo ratings yet
- Assent Template for Child StudyDocument4 pagesAssent Template for Child Studydotaadik11No ratings yet
- Course Name: Biomedical Instrumentation Course Code: MC1652: Wednesday, March 30, 2016 1Document214 pagesCourse Name: Biomedical Instrumentation Course Code: MC1652: Wednesday, March 30, 2016 1Sachin GuptaNo ratings yet
- Negative Physiological Changes of AgingDocument27 pagesNegative Physiological Changes of AgingShaharyar100% (1)
- Case ReviewDocument20 pagesCase ReviewEdwin OkonNo ratings yet
- HAP Chapterwise MCQ For 2nd Sessional PDFDocument6 pagesHAP Chapterwise MCQ For 2nd Sessional PDFsaurav prasadNo ratings yet