You might also like
- Endocrinology Notes for Medical StudentsFrom EverandEndocrinology Notes for Medical StudentsRating: 4 out of 5 stars4/5 (1)
- Chapter 14 Red Blood CellsDocument37 pagesChapter 14 Red Blood CellsCatherine LiuNo ratings yet
- Hematology SummaryDocument9 pagesHematology SummaryJovielle Hayden100% (1)
- Summary of All AnemiaDocument2 pagesSummary of All Anemiabenlarsena93% (14)
- Hematology Tables Morphology of RBCsDocument5 pagesHematology Tables Morphology of RBCsGlydenne Glaire Poncardas GayamNo ratings yet
- HAEMOPOIESISDocument6 pagesHAEMOPOIESISDiyana ZahariNo ratings yet
- HematologyDocument5 pagesHematologyIvy Jan OcateNo ratings yet
- H1d - Microcytic Anemias ChartDocument3 pagesH1d - Microcytic Anemias ChartqselmmNo ratings yet
- Acquired Bleeding DisordersDocument1 pageAcquired Bleeding DisordersGerardLumNo ratings yet
- AnemiaDocument1 pageAnemiaindriyanti natasya ayu utami kottenNo ratings yet
- RBC Morphology and InclusionsDocument3 pagesRBC Morphology and InclusionsDeomicah SolanoNo ratings yet
- WBC Lymph Node SpleenDocument12 pagesWBC Lymph Node Spleendr brijesh TiwariNo ratings yet
- Hematologic Pathology p36-47Document12 pagesHematologic Pathology p36-47zeroun24No ratings yet
- Clinical Medicine - Lecture: - Topic: - DateDocument3 pagesClinical Medicine - Lecture: - Topic: - DateqselmmNo ratings yet
- Anemia ChartsDocument6 pagesAnemia ChartsLiz100% (1)
- RBC DisordersDocument70 pagesRBC DisordersNdor Baribolo100% (1)
- Acute and Chronic LeukemiasDocument3 pagesAcute and Chronic Leukemiaskaku100% (2)
- Decreased Levels of Iron by Diet or Hemorrhage Impaired Heme SynthesisDocument8 pagesDecreased Levels of Iron by Diet or Hemorrhage Impaired Heme SynthesisSamuel RothschildNo ratings yet
- Top 10 AnemiasDocument24 pagesTop 10 AnemiasSim M ChangNo ratings yet
- Blood FilmDocument2 pagesBlood FilmGerardLum100% (1)
- Poikilocytosis Review TableDocument5 pagesPoikilocytosis Review Tablekat100% (1)
- Interpretation of Liver Enzyme Tests - A Rapid GuideDocument3 pagesInterpretation of Liver Enzyme Tests - A Rapid Guidesserggios100% (2)
- Study Questions (Hematology)Document11 pagesStudy Questions (Hematology)tkanesNo ratings yet
- Clinical Chemistry Board ReviewDocument14 pagesClinical Chemistry Board ReviewWellaBaylasNo ratings yet
- Chart - WBC DisordersDocument1 pageChart - WBC DisordersSamuel RothschildNo ratings yet
- WBC Neoplasms Review - PathologyDocument6 pagesWBC Neoplasms Review - Pathologylas100% (6)
- Anemia Type Pathogenesis Clinical Manifestations Diagnosis Peripheral Blood Lab FindingsDocument15 pagesAnemia Type Pathogenesis Clinical Manifestations Diagnosis Peripheral Blood Lab FindingsDanielle FosterNo ratings yet
- Microcytic Hypochromic Macrocytic Normochromic Normocytic: Anemia HematocritDocument7 pagesMicrocytic Hypochromic Macrocytic Normochromic Normocytic: Anemia Hematocritjjjj31No ratings yet
- Endocrine Pathology p17-32Document16 pagesEndocrine Pathology p17-32zeroun24No ratings yet
- Component Therapy-Transfusion of TheDocument8 pagesComponent Therapy-Transfusion of TheGennelyn Ross Delos ReyesNo ratings yet
- Approach To Diagnosis of Haemolytic AnaemiasDocument2 pagesApproach To Diagnosis of Haemolytic AnaemiasGerardLumNo ratings yet
- Pathology GlomerulonephritisDocument4 pagesPathology GlomerulonephritisGerardLum100% (2)
- Hematologic Pathology p48-64Document17 pagesHematologic Pathology p48-64zeroun24100% (1)
- Hematology Anemia & Bleeding Zorko2015Document6 pagesHematology Anemia & Bleeding Zorko2015Rishi Sharma100% (1)
- CBC Reviewer Anaphy LabDocument9 pagesCBC Reviewer Anaphy LabARVINE JUSTINE CORPUZNo ratings yet
- Anemia Table283Document2 pagesAnemia Table283Bridget ParkerNo ratings yet
- DR Nilukshi Perera Consultant HaematologistDocument68 pagesDR Nilukshi Perera Consultant HaematologistThaveeshaLindsayWhiteNo ratings yet
- Hematologic Pathology p24-35Document12 pagesHematologic Pathology p24-35zeroun24100% (6)
- Leukemia - Pathophysiology of White Cells DisordersDocument10 pagesLeukemia - Pathophysiology of White Cells DisordersJacecosmozNo ratings yet
- AUB - Urine Screening For Metabolic DisordersDocument3 pagesAUB - Urine Screening For Metabolic DisordersJeanne Rodiño100% (1)
- 2021 Systemic Pathology S4T1 - RBC and Bleeding Disorders PDFDocument27 pages2021 Systemic Pathology S4T1 - RBC and Bleeding Disorders PDFAlexis Bondad100% (1)
- Urinalysis TableDocument9 pagesUrinalysis TableMegNo ratings yet
- Anti-Coagulants, Anti-Platelets, FibrinolyticsDocument1 pageAnti-Coagulants, Anti-Platelets, FibrinolyticsGerardLum100% (1)
- 33-Hemostasis and Coagulation ProfileDocument40 pages33-Hemostasis and Coagulation ProfileOsman Mohamed MuhumedNo ratings yet
- Microscopic Exam 01 - RBC, WBC, BacteriaDocument30 pagesMicroscopic Exam 01 - RBC, WBC, BacteriaBrent LagartoNo ratings yet
- RH Blood Group SystemDocument6 pagesRH Blood Group SystemUsman ChNo ratings yet
- COMPLETE BLOOD COUNT Lecture GuideDocument9 pagesCOMPLETE BLOOD COUNT Lecture GuideKaycee Gretz LorescaNo ratings yet
- LN Hematology MLT FinalDocument549 pagesLN Hematology MLT FinalMahfuzur Rahman100% (3)
- Common Plating Media For Clinical Bacteriology (From Bailey & Scott's Diagnostic Microbiology, 12th Ed)Document2 pagesCommon Plating Media For Clinical Bacteriology (From Bailey & Scott's Diagnostic Microbiology, 12th Ed)Elizabeth Enjambre HernaniNo ratings yet
- Virology - Study GuideDocument5 pagesVirology - Study GuideMatt McGlothlinNo ratings yet
- Abx FinalDocument3 pagesAbx Finalyanks1120No ratings yet
- Thalassemia TableDocument2 pagesThalassemia TableMeevie ToledoNo ratings yet
- L6-PATHO-Neoplasia (Sept2821)Document12 pagesL6-PATHO-Neoplasia (Sept2821)Erald PaderangaNo ratings yet
- Correctly: IncorrectlyDocument70 pagesCorrectly: IncorrectlyDjdjjd Siisus100% (1)
- Blood Test ResultsDocument1 pageBlood Test ResultsnindyaNo ratings yet
- Hematology Lectures 1 5 DR - TuyDocument10 pagesHematology Lectures 1 5 DR - TuyMiguel Cuevas DolotNo ratings yet
- Anemia SDocument5 pagesAnemia SGps PandetteNo ratings yet
- USMLE - Heme & Lymph PathologyDocument21 pagesUSMLE - Heme & Lymph PathologyMatt McGlothlinNo ratings yet
- Anemia EngDocument49 pagesAnemia EngingritfuryNo ratings yet
- FBC Analysers and FBC InterpretationDocument63 pagesFBC Analysers and FBC InterpretationNikkole PhalulaNo ratings yet
- 7.1. Anemia 2023Document30 pages7.1. Anemia 2023MichellyTjoaNo ratings yet
- Neonatal Hyperbilirubinemia and JaundiceDocument8 pagesNeonatal Hyperbilirubinemia and JaundiceAndreea GeorgianaNo ratings yet
- Diagnostic Report: Client Code: Client'S Name and AddressDocument3 pagesDiagnostic Report: Client Code: Client'S Name and AddressKhurram Shadab IqbalNo ratings yet
- ISBB CompilationDocument6 pagesISBB CompilationElla SalesNo ratings yet
- Haematology Assignment 1Document4 pagesHaematology Assignment 1KINGSCOMPUTERS CYBERNo ratings yet
- Table of Blood Group Systems v. 9.0 03-FEB-2021Document3 pagesTable of Blood Group Systems v. 9.0 03-FEB-2021AnthonyNo ratings yet
- Wa0038.Document9 pagesWa0038.Sambhu Nath DeyNo ratings yet
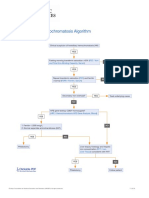
- Hereditary Hemochromatosis AlgorithmDocument1 pageHereditary Hemochromatosis AlgorithmS6b2No ratings yet
- A Study of Knowledge, Attitude and Practice About Sickle Cell Anaemia in Patients With Positive Sickle Cell Status in Bardoli TalukaDocument4 pagesA Study of Knowledge, Attitude and Practice About Sickle Cell Anaemia in Patients With Positive Sickle Cell Status in Bardoli TalukaManisa ParidaNo ratings yet
- Scales and Arpeggios FingeringsDocument2 pagesScales and Arpeggios FingeringsJames RileyNo ratings yet
- Blood Component TherapyDocument13 pagesBlood Component TherapyMohamed ElgayarNo ratings yet
- Blood Grouping and RH TypingDocument4 pagesBlood Grouping and RH TypingJeevs MusicNo ratings yet
- Blood BankingDocument10 pagesBlood BankingSheen AmboyNo ratings yet
- Blood Type Review WorksheetDocument2 pagesBlood Type Review WorksheetSofa100% (2)
- Accu-Temp® Cautery: Specialty CauterizationDocument2 pagesAccu-Temp® Cautery: Specialty CauterizationrhymenNo ratings yet
- Schwartz's Hemostasis, Surgical BleedingDocument33 pagesSchwartz's Hemostasis, Surgical BleedingArifHidayat100% (4)
- ThrombocytopeniaDocument1 pageThrombocytopeniaanum786110No ratings yet
- Coombs TestDocument6 pagesCoombs TestjnsenguptaNo ratings yet
- Blood Grouping Brochure 2013 - Priced PDFDocument8 pagesBlood Grouping Brochure 2013 - Priced PDFmwenyeweNo ratings yet
- Blood Transfusion PolicyDocument6 pagesBlood Transfusion PolicyTanisha SinghNo ratings yet
- Clinical Guide To Transfusion - Preoperative Autologous Donation (Chapter 16)Document4 pagesClinical Guide To Transfusion - Preoperative Autologous Donation (Chapter 16)Ahmed ZeyadNo ratings yet
- Iron Deficiency Anaemia: DR Mrs Stella Kanu Bmls Mbbs MSCDocument17 pagesIron Deficiency Anaemia: DR Mrs Stella Kanu Bmls Mbbs MSCDavid KanuNo ratings yet
- Collection TubeDocument6 pagesCollection TubeChristiane ReaNo ratings yet
- Gambaran Kadar Hematokrit Dan Hemoglobin Pada Kejadian Infark Miokard Akut (Ima) Di Rsup Prof. Dr. R. D. Kandou Manado Periode Januari - Agustus 2014Document7 pagesGambaran Kadar Hematokrit Dan Hemoglobin Pada Kejadian Infark Miokard Akut (Ima) Di Rsup Prof. Dr. R. D. Kandou Manado Periode Januari - Agustus 2014Elma CantikaNo ratings yet
- Types of AnaemiaDocument2 pagesTypes of AnaemiaSuhaila NaemaNo ratings yet
- LP 10 Anemia 3Document43 pagesLP 10 Anemia 3Anonymous elq7jZiSNo ratings yet
- Physical Examination For Pregnant WomanDocument31 pagesPhysical Examination For Pregnant WomanFrancia ToledanoNo ratings yet
- Pathology Consultation On Hba Methods and Interferences: Jeanne M. Rhea, PHD, and Ross Molinaro, PHDDocument12 pagesPathology Consultation On Hba Methods and Interferences: Jeanne M. Rhea, PHD, and Ross Molinaro, PHDyosefinNo ratings yet
- PDF TextDocument1 pagePDF TextBoss GuptaNo ratings yet