You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Full Download Bontragers Textbook of Radiographic Positioning and Related Anatomy 9th Edition Lampignano Test BankDocument36 pagesFull Download Bontragers Textbook of Radiographic Positioning and Related Anatomy 9th Edition Lampignano Test Bankjohn5kwillis100% (22)
- Saeed Sentence Relation and Truth (Summary)Document11 pagesSaeed Sentence Relation and Truth (Summary)Mohammad Hassan100% (1)
- Mywizard For AIOps - Virtual Agent (ChatBOT)Document27 pagesMywizard For AIOps - Virtual Agent (ChatBOT)Darío Aguirre SánchezNo ratings yet
- Integral Theory System Simplified Clinical ApproachDocument15 pagesIntegral Theory System Simplified Clinical ApproachAndrei CristeaNo ratings yet
- Integral Theory System Simplified Clinical ApproachDocument15 pagesIntegral Theory System Simplified Clinical ApproachAndrei CristeaNo ratings yet
- Public Health Mini-Guides - Alcohol Misuse - 1st Edition (2015)Document143 pagesPublic Health Mini-Guides - Alcohol Misuse - 1st Edition (2015)Andrei Cristea100% (1)
- Villar PDFDocument7 pagesVillar PDFAndrei CristeaNo ratings yet
- AN VI MG TabelDocument2 pagesAN VI MG TabelAndrei CristeaNo ratings yet
- An Enhanced RFID-Based Authentication Protocol Using PUF For Vehicular Cloud ComputingDocument18 pagesAn Enhanced RFID-Based Authentication Protocol Using PUF For Vehicular Cloud Computing0dayNo ratings yet
- Hamza Akbar: 0308-8616996 House No#531A-5 O/S Dehli Gate MultanDocument3 pagesHamza Akbar: 0308-8616996 House No#531A-5 O/S Dehli Gate MultanTalalNo ratings yet
- EVS (Yuva)Document88 pagesEVS (Yuva)dasbaldev73No ratings yet
- Montessori Vs WaldorfDocument4 pagesMontessori Vs WaldorfAbarnaNo ratings yet
- Coping Mechanism and Academic Performance Among FiDocument14 pagesCoping Mechanism and Academic Performance Among FiMary Margaret MorillaNo ratings yet
- Prelims CB em Ii5Document21 pagesPrelims CB em Ii5Ugaas SareeyeNo ratings yet
- School of Management Studies INDIRA GANDHI NATIONAL OPEN UNIVERSITY Proforma For Approval of Project Proposal (MS-100)Document12 pagesSchool of Management Studies INDIRA GANDHI NATIONAL OPEN UNIVERSITY Proforma For Approval of Project Proposal (MS-100)Pramod ShawNo ratings yet
- QFW Series SteamDocument8 pagesQFW Series Steamnikon_fa50% (2)
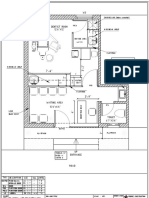
- Dental Clinic - Floor Plan R3-2Document1 pageDental Clinic - Floor Plan R3-2kanagarajodisha100% (1)
- Prevention of Power Theft Using Concept of Multifunction Meter and PLCDocument6 pagesPrevention of Power Theft Using Concept of Multifunction Meter and PLCMuhammad FarhanNo ratings yet
- Reaffirmed 1998Document13 pagesReaffirmed 1998builconsNo ratings yet
- Assignment OSDocument11 pagesAssignment OSJunaidArshadNo ratings yet
- Physical Characteristics of SoilDocument26 pagesPhysical Characteristics of SoillfpachecoNo ratings yet
- Psyche Finals: Trans 2: Psychotic Disorder: SchizophreniaDocument4 pagesPsyche Finals: Trans 2: Psychotic Disorder: SchizophreniajisooNo ratings yet
- Forlong - Rivers of LifeDocument618 pagesForlong - Rivers of LifeCelephaïs Press / Unspeakable Press (Leng)100% (15)
- Dosificación Gac007-008 Sem2Document2 pagesDosificación Gac007-008 Sem2Ohm EgaNo ratings yet
- MnemonicsDocument1 pageMnemonicsSunil Boyz-uNo ratings yet
- School Form 8 Grade 3Document20 pagesSchool Form 8 Grade 3Mimi Ng PinasNo ratings yet
- Math 10 Week 3-4Document2 pagesMath 10 Week 3-4Rustom Torio QuilloyNo ratings yet
- Maharashtra State Board of Technical Education. Academic Monitoring Department ProfileDocument14 pagesMaharashtra State Board of Technical Education. Academic Monitoring Department Profilevspd2010No ratings yet
- Fortigate System Admin 40 Mr2Document115 pagesFortigate System Admin 40 Mr2KhaleelNo ratings yet
- 60 Plan of DepopulationDocument32 pages60 Plan of DepopulationMorena Eresh100% (1)
- Test 4 MathDocument15 pagesTest 4 MathYu ChenNo ratings yet
- Chapter 4 PDFDocument26 pagesChapter 4 PDFMeloy ApiladoNo ratings yet
- Btech CertificatesDocument6 pagesBtech CertificatesSuresh VadlamudiNo ratings yet
- 1941 Iraq and The IlluminatiDocument4 pages1941 Iraq and The IlluminatiZaneWeltonNo ratings yet
- Applications PDFDocument90 pagesApplications PDFahmedNo ratings yet