Professional Documents
Culture Documents
Cardioprotective Growth Factors
Uploaded by
Abhel Calderon0 ratings0% found this document useful (0 votes)
17 views16 pagesSeveral growth factors have been shown to protect the cardiomyocyte from the detrimental effects of acute ischaemiareperfusion injury. This protective effect is due to the recruitment of specific intracellular signal transduction pathways. This article will review several of these cardioprotective growth factors with respect to their ability to confer direct myocardial protection.
Original Description:
Copyright
© © All Rights Reserved
Available Formats
PDF, TXT or read online from Scribd
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentSeveral growth factors have been shown to protect the cardiomyocyte from the detrimental effects of acute ischaemiareperfusion injury. This protective effect is due to the recruitment of specific intracellular signal transduction pathways. This article will review several of these cardioprotective growth factors with respect to their ability to confer direct myocardial protection.
Copyright:
© All Rights Reserved
Available Formats
Download as PDF, TXT or read online from Scribd
0 ratings0% found this document useful (0 votes)
17 views16 pagesCardioprotective Growth Factors
Uploaded by
Abhel CalderonSeveral growth factors have been shown to protect the cardiomyocyte from the detrimental effects of acute ischaemiareperfusion injury. This protective effect is due to the recruitment of specific intracellular signal transduction pathways. This article will review several of these cardioprotective growth factors with respect to their ability to confer direct myocardial protection.
Copyright:
© All Rights Reserved
Available Formats
Download as PDF, TXT or read online from Scribd
You are on page 1of 16
Review
Cardioprotective growth factors
Derek J. Hausenloy and Derek M. Yellon*
The Hatter Cardiovascular Institute, University College London Hospital and Medical School, 67 Chenies Mews, London WC1E
6HX, UK
Received 5 January 2009; revised 1 February 2009; accepted 9 February 2009; online publish-ahead-of-print 13 February 2009
Time for primary review: 23 days
Many of the originally identied cardiovascular growth factors have been demonstrated to exert a
diverse variety of actions within the cardiovascular system, the majority of which are unrelated to
their initially proposed mechanism of action. Interestingly, several of these growth factors have been
demonstrated to protect the cardiomyocyte from the detrimental effects of acute ischaemiareperfu-
sion injury, through the activation of a variety of cell-surface receptors and the subsequent recruitment
of a number of intracellular signal transduction pathways, which include components of the reperfusion
injury salvage kinase pathway. This article will review several of these cardioprotective growth factors
with respect to their ability to confer direct myocardial protection, focusing on the underlying signalling
pathways involved and their potential for clinical application.
KEYWORDS
Cardioprotection;
Ischaemia;
Reperfusion;
Growth factors
1. Introduction
Elucidating the mechanistic pathways underlying normal
cardiac development, growth, and differentiation has
resulted in the identication of a variety of growth
factors, each capable of exerting a diverse array of
effects, many of which appear unrelated to their originally
proposed function within the cardiovascular system.
Several of these growth factors are released by cardiomyo-
cytes during myocardial ischaemia, suggesting that they
may play a role in cardiac repair, myocardial angiogenesis,
and myocardial infarct repair. Whether their release during
myocardial ischaemia confers endogenous cardioprotection
has not been fully resolved and is the subject of ongoing
investigation.
Interestingly, the exogenous administration of several of
these growth factors has been reported to protect the myo-
cardium from the detrimental effects of acute ischaemia
reperfusion injury. This protective effect is due to the
recruitment of specic intracellular signal transduction
pathways linked to cardioprotection, which include the sig-
nalling components of the reperfusion injury salvage kinase
(RISK) pathway, a group of pro-survival kinases that include
PI3K-Akt and MEK1/2-Erk1/2, which confer powerful cardio-
protection when specically activated at the time of myo-
cardial reperfusion.
13
However, it must be appreciated
that the signal transduction pathways underlying the
effects of these cardioprotective growth factors are
complex, and a comprehensive review of all the signalling
pathways involved is beyond the scope of this review
article. Therefore, in this article, we will focus on those
growth factors which were originally identied as having
the potential to exert cardioprotection through the RISK
pathway at the onset of myocardial reperfusion, a clinically
relevant time point for acute myocardial infarction patients
undergoing reperfusion using either brinolytic therapy or
primary percutaneous coronary intervention. These include
the angiogenic growth factors such as vascular endothelial
growth factor (VEGF) and broblast growth factor (FGF),
the IL-6 family cytokine member, cardiotrophin-1 (CT-1),
insulin and insulin-like growth factor (IGF), transforming
growth factor-b (TGF-b), and the peptide hormone, urocor-
tin, which through a variety of receptor subtypes share the
ability to confer cardioprotection through the activation of
the RISK pathway. These growth factors have specic cardi-
ovascular effects separate from their cardioprotective prop-
erties which may in some cases limit their eventual clinical
application in patients with coronary heart disease. The
reader is directed to several other reviews for comprehen-
sive accounts on the cardioprotective effects of other
peptide hormones (kinins, natriuretic peptides, and adreno-
medullin),
4
erythropoietin,
5
and the adipocytokines.
6
2. The reperfusion injury salvage
kinase pathway
The initial concept that there existed pro-survival protein
kinase signalling cascades capable of mediating cardiopro-
tection at the time of myocardial reperfusion was originally
proposed by our laboratory in 1999.
7
The idea was formu-
lated following the general appreciation that apoptotic
cell death was essentially a reperfusion phenomenon and
*
Corresponding author. Tel: 44 207 380 9888; fax: 44 207 380 9505.
E-mail address: hatter-institute@ucl.ac.uk
Published on behalf of the European Society of Cardiology. All rights reserved. & The Author 2009.
For permissions please email: journals.permissions@oxfordjournals.org.
Cardiovascular Research (2009) 83, 179194
doi:10.1093/cvr/cvp062
b
y
g
u
e
s
t
o
n
J
u
l
y
2
2
,
2
0
1
2
h
t
t
p
:
/
/
c
a
r
d
i
o
v
a
s
c
r
e
s
.
o
x
f
o
r
d
j
o
u
r
n
a
l
s
.
o
r
g
/
D
o
w
n
l
o
a
d
e
d
f
r
o
m
that the activation of particular anti-apoptotic protein
kinases such as PI3K-Akt and MEK1/2-Erk1/2, specically at
the clinically relevant time of myocardial reperfusion, had
the ability to attenuate lethal myocardial reperfusion
injury and limit myocardial infarct size.
1,3,7
The original
studies which had been designed to investigate this
concept had examined the effect of growth factors (includ-
ing those reviewed in this article) that were known to acti-
vate PI3K-Akt and MEK1/2-Erk1/2 in order to determine
whether they were capable of mediating cardioprotection
when administered at the onset of myocardial reperfusion.
7
Subsequently, a diverse variety of agents including natriure-
tic peptides, statins, adipocytokines, adenosine, bradyki-
nin, opioids have been reported to target lethal
myocardial reperfusion injury and limit myocardial infarct
size when given at the time of myocardial reperfusion
(reviewed in references 1 and 3).
It is interesting to appreciate that the RISK pathway
underlies the endogenous cardioprotective strategies such
as ischaemic pre-conditioning (IPC)
8
and post-conditioning,
9
which refer to the application of brief periods of ischaemia
reperfusion to the heart either prior to the index ischaemic
event or at the onset of myocardial reperfusion, respect-
ively. Given that both of these treatment strategies
require a mechanical intervention applied directly to the
heart, which limits their clinical applicability, the pharma-
cological manipulation of the cardioprotective signal trans-
duction pathway which unites pre-conditioning and
post-conditioning at the time of myocardial reperfusion
10,11
provides an opportunity to reproduce their infarct-limiting
effects using growth factors as the clinical cardioprotective
therapy.
The mechanism underlying the cardioprotection elicited
by the Akt and Erk1/2, components of the RISK pathway, is
the subject of the ongoing investigation, and a number of
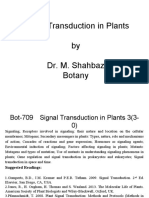
potential mechanisms have been proposed (Figure 1): (i)
the inhibition of the mitochondrial permeability transition
pore (mPTP),
12,13
a critical determinant of lethal myocardial
reperfusion injury
14
; this may be mediated through the acti-
vation of downstream GSK-3b,
12
causing the opening of the
ATP-sensitive mitochondrial potassium channel and the sub-
sequent production of mitochondrial ROS,
15
or through
another unknown mechanism; (ii) the activation of a
variety of anti-apoptotic mechanisms including the phos-
phorylation and inhibition of pro-apoptotic factors such as
BAD and BAX, and the inhibition of cytochrome C release
(reviewed in references 1 and 3); or, (iii) potentiating
calcium uptake via SERCA into the sarcoplasmic reticulum,
thereby reducing calcium-induced mPTP opening.
16
It is important to appreciate that the use of growth
factors as an acute cardioprotective strategy requires the
transient short-lived activation of the PI3K-Akt and MEK1/
2-Erk1/2 components of the RISK pathway as opposed to
their chronic activation which can result in the loss of
their cardioprotective effect
17
and lead to unwanted cardi-
ovascular effects such as cardiac hypertrophy. Furthermore,
Figure 1 This schematic provides a simplied overview of the intracellular transduction pathways underlying cardioprotection elicited by the growth factors:
transforming growth factor-b1 (TGF-b1), cardiotrophin-1 (CT-1), broblast growth factor (FGF), vascular endothelial growth factor (VEGF), insulin, insulin-like
growth factor (IGF), and urocortin. Ligand binding to their respective cell-surface receptors on the cardiomyocyte activates intracellular signalling kinase cas-
cades including Raf-Ras-Mek1/2-Erk1/2 and PI3K-Akt of the reperfusion injury salvage kinase (RISK) pathway, the JAK-STAT pathway, and various anti-apoptotic
mechanisms (including the phosphorylation and inhibition of Bax and BAD as well as the inhibition of cytochrome C release). Many of the acute cardioprotective
mechanisms manifested at the time of reperfusion converge on the mitochondria and include the inhibition of the mitochondrial permeability transition pore
(mPTP), which can be achieved through several different mechanisms including the phosphorylation and inhibition of GSK3b; the opening of the ATP-sensitive
mitochondrial potassium (Mito K
ATP
) channel by the eNOS-NO-PKG-PKC-1 cascade which produces mitochondrial ROS, which inhibits mitochondrial permeability
transition pore opening; and the intracellular calcium modulation due to augmented SERCA uptake of calcium into the sarcoplasmic reticulum. More long-term
cardioprotection may be achieved through the genetic transcription of various cardioprotective mediators such as iNOS, NFkB, MMP-1, phospholipase-1, and so on
(not shown on diagram, see text for details).
D.J. Hausenloy and D.M. Yellon 180
b
y
g
u
e
s
t
o
n
J
u
l
y
2
2
,
2
0
1
2
h
t
t
p
:
/
/
c
a
r
d
i
o
v
a
s
c
r
e
s
.
o
x
f
o
r
d
j
o
u
r
n
a
l
s
.
o
r
g
/
D
o
w
n
l
o
a
d
e
d
f
r
o
m
the concept of the RISK pathway continues to evolve as the
number of described cardioprotective agents increases and
the list of other signalling pathways such as JAK-STAT,
18,19
PKG,
20
PKC-1,
21
sphingosine kinase,
22
and so on, which are
capable of protecting at the time of myocardial reperfusion,
is expanded.
3. Cardioprotective growth factors: protein
tyrosine kinase receptors
In this section, cardioprotective growth factors which bind
to protein tyrosine kinase receptors are reviewed and
these include FGF, VEGF, insulin, and IGF. Growth factor
binding to its specic protein tyrosine kinase receptor in
the heart has the ability to activate both the PI3K-Akt and
MEK1/2-Erk1/2 signal transduction cascades of the cardio-
protective RISK pathway (Figure 1). The activation of the
protein tyrosine kinase receptor by its specic growth
factor results in the autophosphorylation of tyrosine resi-
dues, leading to the recruitment to the membrane of PI3K
(class I
A
), which is activated by directly binding to phospho-
tyrosine residues of the growth factor receptor.
23,24
PI3K
then generates the lipid product phosphatidylinositol-3,4,5-
trisphosphate, which in turn recruits to the membrane sig-
nalling proteins with pleckstrin homology domains, including
the protein serinethreonine kinases, Akt.
23
In addition,
growth factor binding to the receptor tyrosine kinases
results in the activation of Ras, leading to the recruitment
of Raf to the membrane and the subsequent activation of
the MEK1/2-Erk1/2 kinase cascade.
25
3.1 Fibroblast growth factor
In 1974, Gospodarowicz
26
isolated from bovine pituitary
extract a polypeptide which was capable of stimulating
broblast proliferation, which was termed broblast
growth factor. Subsequent investigation has identied 23
members of the FGF family, and these regulate a diverse
variety of effects including embryogenesis, angiogenesis,
growth, and cell survival, although many of the experimen-
tal studies have focused on the actions of FGF-1 (formerly
termed acidic or aFGF) and FGF-2 (formerly termed basic
or bFGF).
27,28
Both FGF-1 and FGF-2 are secreted by cardio-
myocytes in response to myocardial ischaemia and they bind
to a specic plasma membrane tyrosine kinase FGF1 recep-
tor, which is known to be present on cardiomyocytes.
27,28
There is an extensive literature on the myocardial angio-
genic/arteriogenic properties of FGF, and its therapeutic
potential for treating patients with chronic ischaemic
heart disease, a topic which is comprehensively reviewed
elsewhere.
29
In 1992, Yanagisawa-Miwa et al.
30
were the rst to demon-
strate an acute cardioprotective effect in canine hearts
using an intracoronary administration of FGF-2. In this par-
ticular study, the observed infarct-limiting effect of FGF-2
was attributed to its angiogenic properties.
30
A number of
subsequent experimental studies have since demonstrated
an acute cardioprotective effect with FGF which is indepen-
dent of its angiogenic/arteriogenic actions (Table 1). An
initial experimental study by Padua et al.
31
demonstrated
infarct limitation in the isolated rat heart pre-treated with
FGF-2, and a subsequent study using the in situ canine
hearts demonstrated infarct size reduction with
intracoronary FGF-2 in the absence of any effects on
either coronary collaterals or myocardial angiogenesis.
32
Further experimental studies have used shortened reperfu-
sion times in order to investigate the intracellular mechan-
istic pathways underlying the acute cardioprotection
elicited by FGF and are summarized in Table 1.
3.1.1 Signal transduction pathways underlying broblast
growth factor cardioprotection
FGF-1 and FGF-2 exert their cardioprotective effects by
binding to specic plasma membrane tyrosine kinase FGF
receptor (FGFR1 in the heart), which result in the recruit-
ment of a number of different signal transduction pathways
(Figure 1).
27,28
Htun et al.
33
were the rst to demonstrate that the
infarct-limiting effects of FGF-2 pre-treatment could be
abolished by non-specic pharmacological antagonists of
growth factors and tyrosine kinase, suggesting that the car-
dioprotective effect of FGF-2 may be receptor-mediated.
This nding was later conrmed in an experimental study
by Jiang et al.
34
in which it was found that a mutant form
of FGF-2 with reduced afnity for the FGFR-1 tyrosine
kinase receptor failed to limit myocardial infarct size in
the intact canine heart. This mutant form of FGF-2 was
still able to bind to heparin-binding receptors and accumu-
late in the extracellular matrix, suggesting that this was
not required for the acute cardioprotective effect.
34
Subsequent experimental studies have gone on to impli-
cate other familiar mediators of cardioprotection including
PKC-1, PKC-d, Erk1/2, iNOS,
35,36
as well as gap junction
protein, connexion-43.
37
Crucially, the treatment of isolated
adult rat cardiomyocytes with FGF-2 mediated cardiopro-
tection through the activation of PKC-1, suggesting a
direct protective effect of this growth factor on the cardio-
myocyte.
36
Importantly, from a clinical perspective, it has
also been demonstrated by Cuevas et al.
35
that FGF-1 was
able to reduce myocardial infarct size in the in vivo rat
heart when administered at the onset of myocardial reper-
fusion. This cardioprotective effect elicited at the onset of
myocardial reperfusion was conrmed using FGF-2 in a sub-
sequent experimental study and was linked to the activation
of PKC isoforms a, 1, d, and z.
34,38
Importantly, the cardio-
protective effect elicited by FGF-2 was demonstrated to
be independent of its mitogenic effects, as a non-mitogenic
mutant form of FGF-2 was capable of reducing myocardial
infarct size in the perfused rat heart when administered at
the onset of myocardial reperfusion,
38
providing reassuring
evidence that an acute cardioprotective strategy using
FGF-2 may offer benecial effects in terms of infarct limit-
ation without a mitogenic effect.
The role of endogenous FGF in the context of cardiopro-
tection using gain and loss of function approaches has also
been studied. Sheikh et al.
39
demonstrated that the trans-
genic overexpression of FGF-2 in the heart conferred resist-
ance against acute myocardial ischaemiareperfusion injury
and this cardioprotective effect was associated with the
upregulation of p38 MAPK (mitogen-activated protein
kinase), JNK MAPK, and PKC (a and 1 isoforms), although
the contribution of these protein kinases to FGF cardiopro-
tection was not investigated. In contrast, it has been
reported that mice overexpressing FGF-2 are more suscep-
tible to isoproterenol-induced myocardial injury, the mech-
anism of which has been attributed to pro-inammatory
Cardioprotective growth factors 181
b
y
g
u
e
s
t
o
n
J
u
l
y
2
2
,
2
0
1
2
h
t
t
p
:
/
/
c
a
r
d
i
o
v
a
s
c
r
e
s
.
o
x
f
o
r
d
j
o
u
r
n
a
l
s
.
o
r
g
/
D
o
w
n
l
o
a
d
e
d
f
r
o
m
Table 1 Acute cardioprotection with broblast growth factor
Study Model Treatment regime Effect Mechanistic insight
Yanagisawa-Miwa
et al. (1992)
30
In vivo canine heart Intracoronary injection of FGF-2 Improved function; reduced MI size; increased myocardial
capillary density 1 week post-MI
Infarct-limiting effect attributed to angiogenesis
Padua et al. (1995)
31
Isolated perfused rat heart Pre-treatment with FGF-2 (10 mg/heart) Improved function and less CPK release after 30 min
reperfusion
FGF-2 present in blood vessels and cardiomyocytes
Horrigan et al.
(1996)
32
In vivo canine heart Intracoronary injection of FGF-2 (10 mg)
10 min into ischaemia and at
reperfusion
Reduced MI size at 1 week Infarct-limiting effect not associated with angiogenic
response at 1 week
Cuevas et al. (1997)
163
In vivo rat heart Intravenous bolus of FGF-1 at
reperfusion
Reduced myocardial injury and neutrophil activation Non-mitogenic form cardioprotective; less inammation
Cuevas et al. (1997)
164
In vivo rat heart Intravenous bolus of FGF-1 at the onset
of reperfusion
Reduced apoptotic cell death Reduced apoptosis; non-mitogenic form
cardioprotective
Htun et al. (1998)
33
In vivo porcine heart Intramyocardial injection of FGF-1 or
FGF-2 60 min prior to infarction
Reduced myocardial infarct size after 120 min reperfusion Cardioprotection receptor-mediated and requires TK
and mitogenic activity but not haemodynamic activity
Padua et al. (1998)
36
Isolated perfused rat heart Pre-treatment with FGF-2 (10 mg/heart) Improved recovery of function after 60 min reperfusion Negative inotropic effect; cardioprotection requires PKC
and is associated with the activation of PKC-1, PKC-d,
and Erk1/2
Cuevas et al. (2009)
35
In vivo rat heart Intravenous bolus of FGF-1 at the onset
of reperfusion
Improved function and reduced MI size after 24 h reperfusion Cardioprotection at the onset of reperfusion and
associated with iNOS expression
Horrigan et al.
(1999)
165
In vivo canine heart Intracoronary injection of FGF-2 (20 mg)
15 min into ischaemia
Reduced MI size after 5 min reperfusion Infarct-limiting effect not associated with change in
myocardial blood ow
Cuevas et al. (2009)
35
In vivo rat heart Intravenous FGF-1 at reperfusion Reduced CPK release after 24 h reperfusion Cardioprotection blocked by glibenclamide, suggesting
K
ATP
channel is involved
Sheikh et al. (2001)
39
Isolated perfused murine
heart
Overexpression of FGF-2 Reduced LDH release at 60 min reperfusion FGF-2 overexpression protects the hearts against
ischaemic injury and is associated with the
upregulation of PKC, JNK, and p38
Buehler et al.
(2002)
166
In vivo murine heart and
isolated cardiomyocytes
Overexpression of FGF-1 Reduced LDH/CK release; reduced MI size; increased
cardiomyocyte viability
FGF-1 overexpression protects the hearts against
ischaemic injury and Erk1/2 acts as mediator
Jiang et al. (2002)
34
In vivo and ex vivo rat
heart
In vivo: intramyocardial injection of
FGF-2 prior to infarction
In vivo: improved function and smaller MI after 24 h and 6
week reperfusion
Long-term cardioprotection with FGF-2;
cardioprotection requires binding of FGF-2 at FGFR-1
and activation of PKC
Ex vivo: FGF-2 perfused at the onset of
reperfusion
Ex vivo: activation of PKC-a, 1, z
House et al. (2003)
41
Isolated working murine
heart
Cardiac overexpression and ablation of
FGF-2
FGF-2
2/2
reduced function but no difference in MI size;
improved function and reduced MI size in mice
overexpressing FGF-2
Potential endogenous role for FGF-2 as an acute
cardioprotective growth factor
Jiang et al. (2004)
38
In vivo and ex vivo rat
heart
In vivo: intramyocardial injection of
non-mitogenic FGF-2 in
non-reperfused infarction
Improved function, reduced infarct size, PKC-a, 1, d, z
activation and less cytosolic cytochrome C
Cardioprotective effect does not require mitogenic
property of FGF-2
Ex vivo: perfusion with non-mitogenic
FGF-2 at the onset of reperfusion
Palmen et al. (2004)
167
Isolated working murine
heart
Overexpression of FGF-1 Improved function; reduced LDH release; cardioprotection
blocked by PKC and TK inhibitors
Cardioprotection elicited by FGF-1 requires PKC and TK
activation; no difference in p38 or JNK
House et al. (2005)
168
Isolated working murine
heart
Cardiac overexpression of FGF-2 Improved function; reduced MI size; Erk1/2 activation and
p38 inhibition during ischaemia and at reperfusion; MEK1/
2 inhibitor blocks protection
Cardioprotection elicited by FGF-2 requires Erk1/2
activation during ischaemia and at reperfusion
MI, myocardial infarct; CPK, creatine phosphokinase.
D
.
J
.
H
a
u
s
e
n
l
o
y
a
n
d
D
.
M
.
Y
e
l
l
o
n
1
8
2
b y g u e s t o n J u l y 2 2 , 2 0 1 2h t t p : / / c a r d i o v a s c r e s . o x f o r d j o u r n a l s . o r g /D o w n l o a d e d f r o m
myocardial injury mediated by Tcells.
40
The role of FGF-2 as
an endogenous cardioprotective growth factor was revealed
in a subsequent experimental study by House et al.
41
in
which it was reported that transgenic mice lacking cardiac-
specic FGF-2 were more susceptible to acute myocardial
ischaemiareperfusion injury with respect to myocardial
function, although there was no difference in myocardial
infarct size. However, transgenic mice overexpressing
cardiac-restricted FGF-2 that were subjected to myocardial
infarction developed smaller infarctions and had improved
function.
41
Finally, the absence of FGF-2 had a negative
impact on myocardial infarct repair and LV remodelling.
42
It is interesting to note that the PI3K-Akt component of
the RISK pathway has not been linked to the FGF cardiopro-
tection even though this pathway is known to be activated
following FGF binding to its tyrosine kinase receptor on
the cardiomyocyte.
3.1.2 Clinical application of broblast growth factor
The clinical application of FGF thus far has been restricted
to its potent ability to stimulate myocardial angiogenesis
and arteriogenesis. However, subsequent clinical studies
(AGENT1-4) which have examined the use of chronic treat-
ment using adenoviral transfection with FGF-4 in patients
with maximally treated chronic ischaemic heart disease
reported no benecial effects (reviewed in reference 29).
Whether the acute treatment with exogenous FGF has the
ability to reduce myocardial infarct size when administered
as adjunctive therapy to myocardial reperfusion in patients
presenting with an acute myocardial infarction remains to
be determined. Previous experience in patients with stable
coronary artery disease
43
using intracoronary recombinant
FGF-2 at doses ,30 mg/kg had no signicant benecial
effects in terms of reducing angina symptoms, and a signi-
cant number of patients experienced hypotension with the
single bolus infusion, which would limit its use in patients
presenting with an acute myocardial infarction unless a
safe efcacious non-hypotensive dose could be found.
3.2 Vascular endothelial growth factor
VEGF, a 45 kDa polypeptide, is a major regulator of angio-
genesis in the heart, which, like FGF, has been examined
in clinical trials as a therapeutic angiogenic strategy in
chronic ischaemic heart disease.
44
In contrast, given that
VEGF promotes angiogenesis in tumour growth, VEGF antag-
onists are also being developed as novel anti-cancer therapy.
VEGF is generated in response to myocardial ischaemia and
binds to two high-afnity tyrosine kinase receptors, the t-1
and the KDR (the human homologue of the murine k-1
receptor), which are preferentially distributed on vascular
endothelial cells but are also known to be present on cardi-
omyocytes.
44,45
VEGF also exerts a diverse variety of pleio-
tropic effects which include an acute cardioprotective
effect, and this will be the main focus of this section.
Cardiomyocytes have been demonstrated to produce
VEGF mRNA in response to hypoxia
46,47
or the inhibition of
the electron transport chain,
47
an effect which in the
human heart is mediated by the stabilization of
hypoxia-inducible factor.
48
Luo et al.
49
were the rst to
demonstrate an acute cardioprotective effect with VEGF
pre-treatment. Perfusion of isolated rat hearts with VEGF
resulted in improved functional recovery and less cardiac
enzyme release following a sustained period of ischaemia
reperfusion injury.
49
However, in this study, the cardiopro-
tective effect was attributed to a vascular effect, although
a direct myocardial effect may have been possible. Both
t-1 and KDR/k-1 VEGF receptors have been demonstrated
to be present in cardiomyocytes,
45
suggesting that VEGF
may exert a direct effect on cardiomyocytes. The activation
of the VEGF receptor is known to activate signal transduc-
tion pathways of the RISK pathway such as MEK1/2-Erk1/
2-p90
rsk
within the cardiomyocyte
50
and PI3K-Akt-eNOS
within endothelial cells,
51
which are known to mediate cyto-
protection. Therefore, one would surmise that through
these signalling cascades, VEGF would have the potential
to protect cardiomyocytes from ischaemiareperfusion
injury by acting directly on the cardiomyocyte, although
this remains to be demonstrated (Figure 1).
Interestingly, the contribution of VEGF to the endogenous
cardioprotective strategy of IPC has been investigated. It
has been demonstrated that IPC augments levels of VEGF
mRNA in cardiomyocytes in a PKC-1-dependent manner
52
and that heterozygous mice lacking the VEGF receptors
k-1
53
or t-1
54,55
sustain greater myocardial ischaemia
reperfusion injury and are resistant to the infarct-limiting
effects of IPC, a nding which may be attributed to the
downregulation of cardioprotective mediators such as Akt,
iNOS, and eNOS.
55
Therefore, further pre-clinical work is
required to determine whether VEGF is capable of mediating
a direct cardioprotective effect at the level of the cardio-
myocyte and to demonstrate whether similar pro-survival
signal transduction pathways are involved in conveying the
protective signal.
In common with FGF, the clinical application of VEGF has
until now been restricted to therapeutic angiogenesis. In
this respect, phase 1 clinical studies of patients with refrac-
tory ischaemic heart disease examining angiogenic gene
therapy using AdVEGF165
56
or AdVEGF121
57
have been com-
pleted with no safety issues. With regard to the exogenous
recombinant VEGF therapy, an intracoronary high-dose of
recombinant VEGF (50 ng/kg/min) at day 0 and three sub-
sequent intravenous infusions at days 3, 6, and 9 resulted
in signicant improvement in anginal symptoms at 120
days in patients with stable coronary artery disease unamen-
able to revascularization.
58
Whether, a single intracoronary
dose of recombinant VEGF as adjuvant reperfusion therapy
would be safe and efcacious in patients presenting with a
myocardial infarction is unknown.
3.3 Insulin
Insulin is intricately involved with growth and metabolism of
the heart and it is this inuence on cardiac metabolism
during myocardial ischaemia which rst attracted its use
as part of the glucoseinsulinpotassium (GIK) therapy in
ischaemic heart disease. There is extensive literature exam-
ining the cardioprotective potential of metabolic modu-
lation using GIK therapy in patients presenting with an
acute myocardial infarction,
59,60
and in this respect, the
reader is directed to the following reviews.
61
In this
section, the primary focus will be on those studies investi-
gating the acute cardioprotective effects of insulin when
administered alone (Table 2).
Insulin binds to its specic protein tyrosine kinase recep-
tor (IR), resulting in the autophosphorylation of intracellular
Cardioprotective growth factors 183
b
y
g
u
e
s
t
o
n
J
u
l
y
2
2
,
2
0
1
2
h
t
t
p
:
/
/
c
a
r
d
i
o
v
a
s
c
r
e
s
.
o
x
f
o
r
d
j
o
u
r
n
a
l
s
.
o
r
g
/
D
o
w
n
l
o
a
d
e
d
f
r
o
m
tyrosine residues, leading to the recruitment to the mem-
brane and the phosphorylation of the insulin receptor sub-
strate (IRS), which in turn generates Src homology 2
(SH2)-domain-binding sites for numerous effectors including
PI3K and the subsequent activation of Akt.
62
In addition, the
SH2 domain of the growth factor receptor-bound protein-2
can activate the pre-associated GTP exchange factor Sos,
resulting in the activation of the small GTPase, Ras, which
then activates the Raf-MEK1/2-Erk1/2 signalling cascade.
62
One of the rst experimental studies to demonstrate a
direct cardioprotective effect with insulin when adminis-
tered alone was in 1999 by Baines et al.
63
In that study,
the authors demonstrated that the pre-treatment of rabbit
hearts reduced myocardial infarct size in a manner which
was dependent on the activation of PI3K and tyrosine
kinase.
63
In addition, in this study, insulin was demonstrated
to limit infarct size even when administered at the onset of
myocardial reperfusion, a clinically important time point. A
subsequent study by our laboratory demonstrated that
insulin was capable of protecting isolated neonatal cardio-
myocytes through a potential anti-apoptotic mechanistic
pathway.
64
Further experimental work has gone on to
further delineate the underlying cardioprotective signalling
cascades and has identied PI3K-Akt-p70S6K-BAD,
65
PI3K-Akt-eNOS,
66
and most recently the JAK-STAT
67
path-
ways (Table 2 and Figure 1). Interestingly, it was observed
that delayed perfusion of the isolated rat heart with
insulin after the rst 15 min of reperfusion had elapsed did
not limit infarct size, suggesting that the cardioprotective
end-effector mechanism was mediated in the rst few
minutes of myocardial reperfusion, the time-window for
preventing the opening of the mPTP, a critical mediator of
lethal myocardial reperfusion injury.
14
Subsequent studies
have identied the mPTP as a downstream target of the
PI3K-Akt pathway in insulin-induced cardioprotection.
12,13
The mechanism through which the JAK-STAT pathway
exerts acute cardioprotection at the time of myocardial
reperfusion, given its role in gene transcription, is unclear,
although it has been speculated that STAT may act directly
at the level of the mitochondria to mediate acute cardiopro-
tection (reviewed in reference 68).
Clearly, in the clinical setting, the use of insulin therapy
alone as a potential cardioprotectant is not feasible given
the risks of hypoglycaemia, although other anti-diabetic
agents such as glucagon-like peptide-1, which are capable
of stimulating insulin release without causing hypoglycae-
mia, may be used as potential cardioprotective agents in
the clinical setting.
69
3.4 Insulin-like growth factors
IGF-I and IGF-II were originally identied as somatomedin C
in 1956 and multiplication stimulatory action in 1972,
70
respectively. They preferentially bind to their respective
tyrosine kinase receptors IGF-IR and IGF-IIR, which are
present throughout the body and have been implicated in
the regulation of cell growth, differentiation, and survival
(reviewed in reference 71). IGF-I is a 72 kDa polypeptide
(comprising 70 amino acids), which is produced in the liver
in response to growth hormone, and circulates predomi-
nantly bound to IGF-binding factors.
71
In 1995, Buerke et al.
72
were the rst group to implicate
IGF-I as a cardioprotective agent, demonstrating that pre-
treatment with this growth factor reduced myocardial
necrosis, apoptosis, and neutrophil accumulation. Since
then, a variety of experimental studies have conrmed the
cardioprotective benets of IGF-I and IGF-II treatment and
have explored the underlying mechanistic pathways
(Table 3). Importantly, mice overexpressing IGF-IB (hetero-
zygous) sustained smaller myocardial infarcts, less
Table 2 Acute cardioprotection with insulin
Study Model Treatment regime Effect Mechanistic insight
Baines et al.
(1999)
63
Isolated rabbit heart Pre-treatment or treatment
at reperfusion with insulin
Reduced MI size Acute cardioprotection dependent
on TK and PI3K
Jonassen et al.
(2000)
64
Neonatal rat
cardiomyocytes
Treatment at reoxygenation
with insulin
Cell survival and less
apoptotic cell death
Anti-apoptotic effect dependent
on TK and PI3K
Jonassen et al.
(2001)
65
Isolated perfused rat
heart
Treatment at reperfusion
with insulin
Reduced MI size Protection dependent on
PI3K-Akt-p70S6K-BAD
Gao et al.
(2002)
66
In vivo perfused rat heart Treatment at reperfusion
with insulin
Reduced MI size Protection dependent on
PI3K-Akt-eNOS-NO
Gao et al.
(2004)
169
In vivo perfused rat heart Treatment at reperfusion
with insulin
Reduced MI size and less
apoptosis
Juhaszova
et al.
(2004)
12
Isolated adult rat
cardiomyocytes
Pre-treatment with insulin Less oxidative
stress-induced mPTP
opening
Protection mediated via
GSK3b-mPTP inhibition
Davidson et al.
(2006)
13
Isolated adult rat
cardiomyocytes
Pre-treatment with insulin Less oxidative
stress-induced mPTP
opening
Protection mediated via Akt-mPTP
inhibition
Fugelstag et al.
(2009)
170
Isolated rat heart Pre-treatment and treatment
at reperfusion with insulin
Smaller MI size Protection dependent on p70S6K
Fugelstag et al.
(2008)
67
Isolated rat heart and
isolated
cardiomyocytes
Pre-treatment with insulin Smaller MI size;
improved cell survival
Protection dependent on JAK-STAT
pathway upstream of Akt
MI, myocardial infarct.
D.J. Hausenloy and D.M. Yellon 184
b
y
g
u
e
s
t
o
n
J
u
l
y
2
2
,
2
0
1
2
h
t
t
p
:
/
/
c
a
r
d
i
o
v
a
s
c
r
e
s
.
o
x
f
o
r
d
j
o
u
r
n
a
l
s
.
o
r
g
/
D
o
w
n
l
o
a
d
e
d
f
r
o
m
apoptosis, and less cardiac remodelling at 7 days post-
myocardial infarction, conrming the long-term cardiopro-
tective benets of IGF-I.
73
3.4.1 Signal transduction pathways underlying
insulin-like growth factor-I cardioprotection
IGF-I exerts its cellular effects by binding to IGF-IR and acti-
vating the tyrosine kinase receptor which leads to the autop-
hosphorylation of tyrosine and serine residues and the
subsequent phosphorylation of IRS-1 and IRS-2 and down-
stream signalling pathways such as the PI3K-Akt pathway
and MEK1/2-Erk1/2.
71
The IRS-1 interacts with and activates
PI3K and the guanine-nucleotide exchange factor Grb2/SOS,
the latter of which is responsible for recruiting the Ras/Raf/
Mek1/2/Erk1/2 kinase cascade. Many of the anti-apoptotic
pathways recruited downstream of the PI3K-Akt
7476
and
MEK1/2-Erk1/2
75
pro-survival pathways have been impli-
cated in IGF-I-mediated cardioprotection (Table 3) Crucially,
the importance of Akt phosphorylation specically at the
onset of myocardial reperfusion as a mediator of
cardioprotection elicited by transgenic overexpression of
IGF-I was rst observed by Yamashita et al.
77
Many of these signal transduction pathways exert anti-
apoptotic effects by modulating the balance of anti-apoptotic
and pro-apoptotic proteins such as Bcl
2
and Bax.
78
In addition,
the majority of these signal cascades terminate on the
mitochondria, resulting in the inhibition of mPTP opening,
78
prevention of mitochondrial cytochrome C release,
78
main-
tenance of mitochondrial respiratory production and mito-
chondrial membrane potential, and less ROS production.
79
However, to be useful as a cardioprotective agent, the sys-
temic metabolic effects of IGF-I have to be overcomein
this respect, the selective adenoviral transfection of IGF-I in
the myocardium may be promising in cases where myocardial
ischaemia can be anticipated, thereby allowing cardioprotec-
tion in the absence of raised systemic levels of IGF-I.
80
3.4.2 Clinical application of insulin-like growth factor
Cardiovascular risk is doubled in patients lacking GH/IGF-I,
suggesting that this growth factor may be important for
endogenous cardioprotection (reviewed in reference 81).
Table 3 Acute cardioprotection with insulin-like growth factor
Study Model Treatment regime Effect Mechanistic insight
Buerke et al.
(1995)
72
In vivo rat heart Pre-treatment with IGF-I Reduced cardiac enzyme release;
less apoptosis; less neutrophil
accumulation
First study to demonstrate
acute cardioprotection;
anti-apoptotic and
inammatory effects
Vogt et al.
(2007)
171
In vivo porcine heart Pre-treatment via
intramyocardial
injection of IGF-II
Smaller MI size Protection dependent on
tyrosine kinase
Li et al.
(1997)
73
In vivo murine heart Mice overexpressing
IGF-I
/2
Smaller MI size, less apoptosis,
and less remodelling
Overexpression of IGF-I is
cardioprotective
Wang et al.
(2008)
172
Adult rat cardiomyocytes Pre-treatment with IGF-I
prior to serum
withdrawal or
doxorubicin treatment
Improved cell survival and less
apoptosis; reduced Bax and
Caspase 3 activation
Reduced Bax and Caspase 3
activation
Otani et al.
(2000)
173
Isolated perfused rat heart Treatment at the time of
reperfusion with IGF-I
Improved myocardial function
and less cardiac enzyme
release
Protects at reperfusion via
PI3K
Fujio et al.
(2000)
76
Neonatal cardiomyocytes Pre-treatment with IGF-I Reduced cell death, less
apoptosis
Protection dependent on
PI3K-Akt
Hong et al.
(2001)
174
H9c2 cardiac myoblasts
subjected to hydrogen
peroxide-induced stress
Pre-treatment with IGF-I Reduced cell death, less
apoptosis
Protection dependent on
PI3K-Akt and MEK1/2-Erk1/
2
Yamamura
et al.
(2001)
78
Isolated perfused rat heart Pre-treatment with IGF-I
(1224 h)
Improved function, less CK
release, and less apoptosis;
mPTP inhibition and less
cytoch C release; increased
Bcl
XL
/Bax ratio
Protection mediated by Bcl
2
/
Bax and mPTP inhibition
Yamashita
et al.
(2001)
77
Isolated perfused murine
heart
Mice overexpressing
IGF-I
/2
Less apoptosis; more PI3K-Akt
activation both pre-ischaemia
and at reperfusion
PI3K-Akt activation
pre-ischaemically and at
reperfusion important for
protection
Chao et al.
(2003)
80
Neonatal cardiomyocytes
and in vivo rat heart
Adenoviral transfection
with IGF-I vs. IGF-I
treatment
Improved cell survival, less
infarct size
More effective
cardioprotection and no
increased serum IGF-I with
adenoviral transfection
Pi et al.
(2007)
79
Adult rat cardiomyocytes Pre-treatment with IGF-I Improved mitochondrial
respiratory function,
maintained membrane
potential; less oxidative stress
Benecial effects on
mitochondrial function
MI, myocardial infarct.
Cardioprotective growth factors 185
b
y
g
u
e
s
t
o
n
J
u
l
y
2
2
,
2
0
1
2
h
t
t
p
:
/
/
c
a
r
d
i
o
v
a
s
c
r
e
s
.
o
x
f
o
r
d
j
o
u
r
n
a
l
s
.
o
r
g
/
D
o
w
n
l
o
a
d
e
d
f
r
o
m
In addition, the plasma levels of IGF-I have been reported to
be lower in patients presenting with an acute myocardial
infarction
82
and higher in patients with cardiac failure.
83
Importantly, low plasma levels of IGF-I have been linked to
worse cardiovascular outcomes.
84,85
The haemodynamic
effects of a single subcutaneous injection of exogenous
IGF-I (60 mg/kg) has been investigated in human volun-
teers
86
and patients with cardiac failure
87
and results in an
increase in stroke volume, cardiac output, ejection fraction
and reduces systemic vascular resistance, with minimal
effect of blood glucose. The inotropic effect exerted by
exogenous IGF-I may limit its clinical applicability to
patients presenting with an acute myocardial infarction
unless an appropriate cardioprotective non-inotropic dose
could be found.
4. Cardiotrophin-1: a cytokine receptor ligand
CT-1 is a member of the interleukin-6 (IL-6) family of
cytokines, which are capable of inducing cardiac hyper-
trophy by binding to cytokine receptors containing the
transmembrane signalling protein gp130. Mice lacking
gp130 exhibit severe ventricular hypoplasia, suggesting
that gp130-coupled signalling is important for the devel-
opment of the heart.
88
CT-1 was originally identied by
Pennica et al. in 1995
89
as a 21.5 kDa protein capable of
inducing hypertrophy in neonatal ventricular cardiomyo-
cytes. One year later, the same research group demon-
strated that CT-1 was required for cardiac myocyte
maturation and was capable of promoting cell survival in
neonatal rat cardiomyocytes subjected to serum depri-
vation,
90
through an anti-apoptotic pathway mediated
by MAPK, Erk1/2.
91
The rst study to demonstrate resist-
ance to ischaemiareperfusion injury with CT-1 treatment
was by Stephanou et al.
92
in 1998. In that particular study,
CT-1 treatment was associated with the upregulation of
heat shock proteins 70 and 90 in neonatal rat
cardiomyocytes and it conferred resistance against both
simulated ischaemic injury and thermal stress in terms
of improved cell survival and less apoptotic cell death.
92
Since then a variety of experimental studies have
reported treatment with CT-1 either prior to myocardial
ischaemia or at the onset of myocardial reperfusion
using cultured neonatal rat cardiomyocytes
(Table 4),
93,94
isolated perfused animal hearts,
95
the
intact animal heart, and human atrial tissue
96
(Table 2).
Importantly, it was demonstrated that CT-1 was capable
of limiting myocardial injury even when administered
at the onset of reperfusion, making the transition to clini-
cal therapy more amenable.
9395
Furthermore, CT-1 has
been reported to promote cardiomyocyte survival and
reduce apoptotic cell death following non-ischaemic
death stimuli such as angiotensin II and hydrogen
peroxide.
97
In addition, CT-1 mRNA has been identied in both the
developing and adult animal hearts, and its production is
stimulated by hypoxic stress.
98
Following a myocardial
infarction, the production of CT-1 mRNA and protein are
both enhanced in rat left and right ventricles.
99
These nd-
ings may suggest that CT-1 may play a role in endogenous
cardioprotection. However, myocardial infarct size was
found to be no different in mice lacking CT-1 compared
with the wild-type control.
100
The expression of CT-1 is also increased in the failing
animal heart
101
and human heart.
102
Myocardial stretch
from cardiac dilatation is responsible for the overexpression
of CT-1 in the failing hearts.
103
Interestingly, CT-1 has been
detected in human plasma,
104
and its levels are increased
in a variety of cardiac conditions including stable and
unstable angina,
105
acute myocardial infarction,
106
aortic
stenosis,
107
mitral regurgitation,
108
left ventricular hyper-
trophy,
109
and left ventricular systolic dysfunction.
110,111
Further work is required to determine the pathophysiologi-
cal signicance of these ndings.
Table 4 Acute cardioprotection with cardiotrophin-1
Study Model Treatment regime Effect Mechanistic insight
Stephanou
et al.
(1998)
92
Neonatal rat
cardiomyocytes
Pre-treatment with
CT-1
Improved cell survival and less
apoptotic cell death
First study to demonstrate acute
cardioprotection
Ghosh et al.
(2000)
96
Human right atrial
appendage tissue
Acute or chronic
(24 h)
pre-treatment
with CT-1
Less tissue injury following chronic
but not acute treatment; CT-1
Ab did not abrogate PC
protection
Chronic but no acute protection
with CT-1 in human atrial tissue;
PC protection not mediated
through CT-1
Brar et al.
(2001)
94
Neonatal rat
cardiomyocytes
Pre-hypoxia or at
reoxygenation
Improved cell survival and less
apoptotic cell death; protection
blocked by Erk1/2 inhibition
First study to show protection at
the time of reoxygenation;
protection is dependent upon
Erk1/2 activation
Brar et al.
(2001)
93
Neonatal rat
cardiomyocytes
Pre-hypoxia or at
reoxygenation
Improved cell survival and less
apoptotic cell death; protection
requires Erk1/2, PI3K, and Akt
Protection at the onset of
reoxygenation and is dependent
upon Erk1/2 activation
Craig et al.
(2001)
116
Neonatal rat
cardiomyocytes
Pre-treatment with
CT-1
Improved cell survival; protection
requires p38, Erk1/2, PI3K, and
NFkB
Protection dependent upon NFkB
activation
Liao et al.
(2002)
95
Adult rat
cardiomyocytes and
perfused rat heart
Pre-hypoxia or at
reoxygenation
Improved cell survival and less
apoptotic cell death; reduced
myocardial infarct size;
protection blocked by Erk1/2
inhibition
Protection in adult cardiomyocytes
and perfused heart; protection
dependent upon Erk1/2
activation
D.J. Hausenloy and D.M. Yellon 186
b
y
g
u
e
s
t
o
n
J
u
l
y
2
2
,
2
0
1
2
h
t
t
p
:
/
/
c
a
r
d
i
o
v
a
s
c
r
e
s
.
o
x
f
o
r
d
j
o
u
r
n
a
l
s
.
o
r
g
/
D
o
w
n
l
o
a
d
e
d
f
r
o
m
4.1 Signal transduction pathways underlying
cardiotrophin-1 cardioprotection
CT-1 exerts its intracellular effects by binding to a cytokine
receptor which comprises a gp130 subunit and a leukaemia
inhibitory factor (LIF) receptor subunit b which heterodi-
merize upon CT-1 binding.
112
The dimerization of the CT-1
receptor results in the recruitment of a number of signal
transduction pathways (Figure 1). The binding of CT-1 to
its cell surface receptor activates receptor-associated
Janus family tyrosine kinases (JAKs). The activation of JAK
is required for the phosphorylation of a variety of sites on
the receptor cytoplasmic domains, which in turn recruit
signal relay molecules containing src homology-2 (SH2)
and/or phosphotyrosine-binding domains. Signal relay mol-
ecules then recruit downstream signalling pathways, includ-
ing the SH2 domain-containing transcription factors (STAT),
the Ras-Raf-MEK1/2-Erk1/2 and the PI3K-Akt signal trans-
duction cascades.
113,114
Experimental studies have suggested that the cardiac
hypertrophy induced by CT-1 is mediated through the
recruitment of the JAK-STAT pathway.
91
In contrast, the
acute cardioprotection elicited by CT-1 has been associated
with the activation of several different signal transduction
pathways including (i) the activation of heat shock proteins
70 and 90
92
; (ii) the phosphorylation of the anti-apoptotic
MAPK, Erk1/2
91,93,94
; (iii) the recruitment of the anti-
apoptotic signalling cascade PI3K-Akt-BAD
93,115
; and (iv)
the phosphorylation of p38MAPK.
116
The mechanism through which these different signal
transduction pathways mediate cardioprotection is unclear,
although one study has suggested that with respect to p38,
Erk1/2, and Akt, CT-1 cardioprotection was demonstrated
to be dependent on the downstream nuclear translocation
of NFkB.
116
However, the acute cardioprotection elicited
at the time of re-oxygenation cannot be dependent on
gene transcription and may be attributed to the inhibition
of mPTP opening, although this remains to be demonstrated
with respect to CT-1 cardioprotection. Many of the signalling
cascades activate a variety of anti-apoptotic pathways with
the inhibition of various pro-apoptotic proteins such as p53,
BAX, FAS, BAD and the upregulation of anti-apoptotic pro-
teins such as Bcl
2
.
117
Interestingly, the contribution of the RISK pathway com-
ponents Erk1/2 MAPK and the PI3K-Akt pathways to CT-1
protection against serum deprivation was demonstrated to
be additive, suggesting that these two anti-apoptotic signal-
ling cascades acted in parallel to mediate cellular survi-
val.
115
However, in the context of protection from
simulated ischaemiareperfusion injury, both these pro-
survival kinase cascades appear to be required as inhibiting
either one abolished completely the cardioprotection eli-
cited by CT-1.
93
5. Urocortin: a G-protein-coupled receptor
ligand
Urocortin was rst identied in the rat mid-brain by Vaughan
et al. in 1995,
118
as a 40 amino acid peptide member of the
corticotrophin-releasing hormone (CRH) family, and was
given its name because of its homology with sh urotensin
and mammalian CRH. It binds to the G-protein-coupled
receptors, CRH-receptor 1 (CRH-R1, found predominantly
in the brain) and CRH-receptor 2 (CRH-R2, found in the per-
iphery including vascular endothelial cells and the heart),
although it acts preferentially at the latter (for comprehen-
sive reviews, please see references 119 and 120). Urocortin
has since been found to be present peripherally in various
organs, including the heart. Experimental studies have
reported peripheral vasodilation in the rat
118
and increased
cardiac contractility in sheep
121
with the systemic adminis-
tration of urocortin. These haemodynamic effects are
blunted in mice lacking CRH-R2
122
and underlie their poten-
tial utility in congestive cardiac failure (see what follows).
The rst study to demonstrate an acute cardioprotective
effect with urocortin was by Osoki et al. in 1998,
123
who
found that pre-treatment with urocortin was able to
reduce cell death and LDH release in neonatal rat cardio-
myocytes subjected to 6 h hypoxia. Subsequent studies
have demonstrated that mRNA expression of urocortin is
increased during simulated ischaemia and that it is secreted
by neonatal rat ventricular cardiomyocytes during simulated
ischaemia and released by isolated perfused rat hearts
during sublethal ischaemia (520 min),
124
suggesting that
urocortin may mediate endogenous cardioprotection.
125
Interestingly, the cardioprotective effect of bathing the neo-
natal ventricular cardiomyocytes in hypoxically pre-
conditioned medium was abolished by CRH receptor antag-
onists, suggesting that CRH peptides such as urocotin may
mediate the cardioprotective effect of IPC.
125
Since these
early publications, studies have gone on to conrm that uro-
cortin is able to reduce myocardial infarct size when admi-
nistered both prior to and at the onset of myocardial
reperfusion
126,127
(Table 5).
5.1 Signal transduction pathways underlying
urocortin cardioprotection
Urocortin exerts its cardioprotective effects by binding to
a G-protein-coupled receptor on the cardiomyocyte
called the CRH-R2b (in rat heart)
128
and CRF-R2a (in
the human heart).
129
Both urocortin mRNA and CRF-R2a
mRNA and receptors have been found in the human
heart.
130
Experimental studies have demonstrated that
the cardioprotective effect is dependent on the acti-
vation of pro-survival kinase pathways of the RISK
pathway such as the PI3K-Akt
127
and the MEK1/2-Erk1/2
cascades.
126
The binding of urocortin to its GPCR results
in the recruitment to the membrane of PI3K-g (class I
B
),
leading to the membrane recruitment and activation of
Akt.
24
In addition, PI3K-g has the ability to activate
mitogen-active protein kinases (MAPKs) such as the
MEK1/2-Erk1/2 cascade.
131
Importantly, our laboratory
132
demonstrated, using the in
vivo rat heart, that urocortin administered at the onset of
myocardial reperfusion reduced myocardial infarct size
through the specic activation of the MEK1/2-Erk1/2 pro-
survival signalling pathway. Indeed, it was in this study
that the term reperfusion injury salvage pathway was
rst described.
132
The cardioprotective effector mechan-
isms downstream of these kinase signalling pathways are
unclear and appear to converge on the cardiac mitochondria
and include the mitochondrial ATP-dependent potassium
channel,
133135
PKC activation
134
(specically the PKC-1
isoform at the level of mitochondria),
135
reduced mitochon-
drial phospholipase A,
135,136
reduced mitochondrial ROS
Cardioprotective growth factors 187
b
y
g
u
e
s
t
o
n
J
u
l
y
2
2
,
2
0
1
2
h
t
t
p
:
/
/
c
a
r
d
i
o
v
a
s
c
r
e
s
.
o
x
f
o
r
d
j
o
u
r
n
a
l
s
.
o
r
g
/
D
o
w
n
l
o
a
d
e
d
f
r
o
m
production, and prevention of mPTP opening at time of
reperfusion.
137
Interestingly, urocortin-induced cardiopro-
tection has been linked to the inhibition of Beclin-1-induced
cardiac autophagy.
138
Interestingly, cardiomyocytes isolated
from mice lacking CRF-R2 were reported to be more suscep-
tible to simulated ischaemiareperfusion injury,
139
suggesting that urocortin or its analogues urocortin II and
III may exert endogenous cardioprotection.
However, because urocortin acts at both CRH-R1 (in the
brain) and CRH-R2 (in the heart) in addition to conferring
cardioprotection, it also stimulates the production of
ACTH, which results in an increase in plasma cortisol.
However, urocortin II (stresscopin) and urocortin III
(stresscopin-related peptide), peptide analogues of uro-
cortin, bind CRH-R2 and have been reported to exert
potent cardioprotection in a similar manner to urocor-
tin,
139,140
potentially making them more useful in the clini-
cal setting.
5.2 Clinical application of urocortin
Urocortin and its cell surface (CRH-R2a) have been found in
the human heart,
130
and levels of cardiac urocortin are elev-
ated in the presence of dilated cardiomyopathy
141
and
hypertrophic cardiomyopathy.
142
In patients with mild LV
systolic heart failure, plasma levels of urocortin are elev-
ated,
143
suggesting a potential compensatory mechanism
of a failing heart given the known inotropic actions of uro-
cortin. Despite the animal studies reporting an inotropic
effect and systemic vasodilation with urocortin I, when
Table 5 Acute cardioprotection with urocortin
Study Model Treatment regime Effect Mechanistic insight
Okosi et al.
(1998)
123
Neonatal rat
cardiomyocytes
Pre-treatment with
urocortin
Improved cell survival and
less LDH release
First study to demonstrate acute
cardioprotection
Brar et al.
(1999)
125
Neonatal rat
cardiomyocytes
Pre-treatment and
treatment at the time
of reperfusion with
urocortin
Expression increased and
secretion with ischaemia;
improved cell survival and
less apoptosis
May mediate endogenous
cardioprotection; protects at
the time of reperfusion
Brar et al.
(2000)
126
Neonatal rat
cardiomyocytes and
isolated perfused rat
heart
Pre-treatment and
treatment at the time
of reperfusion with
urocortin
Improved cell survival and
less apoptosis; smaller
infarct size
Protects via Erk1/2; reduces
myocardial infarct size
Brar et al.
(2002)
127
Neonatal and adult rat
cardiomyocytes
Pre-treatment and
treatment at the time
of reperfusion with
urocortin
Improved cell survival and
less apoptosis
Protects via Akt and Erk1/2
Schulman
et al.
(2002)
132
Ex vivo and in vivo rat
hearts
Treatment at the onset of
reperfusion with
urocortin
Reduce myocardial infarct
size
Protects via Erk1/2 component of
the RISK pathway
Lawrence
et al.
(2002)
133
Neonatal rat
cardiomyocytes and
isolated perfused rat
heart
Pre-treatment with
urocortin
Improved cell survival and
less apoptosis; smaller
infarct size
Protection blocked by 5-HD
Scarabelli
et al.
(2002)
175
Isolated perfused rat
heart
Pre-treatment and
treatment at the time
of reperfusion with
urocortin
Improved function,
phosphate levels, and less
endothelial and
cardiomyocyte apoptosis
Less endothelial apoptosis;
improved phosphate levels
Chanalaris
et al.
(2003)
140
Neonatal rat
cardiomyocytes
Pre-treatment and
treatment at the time
of reperfusion with
urocortin II and III
Improved cell survival and
less apoptosis
Protects via Akt and Erk1/2
Gordon et al.
(2003)
134
Adult rat cardiomyocytes Pre-treatment with
urocortin
Less cardiac enzymes Protection blocked by 5-HD and
PKC inhibitor
Lawrence
et al.
(2003)
136
Isolated perfused rat
heart
Pre-treatment with
urocortin
Reduce infarct size Reduced phospholipase A2 gene
expression
Lawrence
et al.
(2004)
135
Neonatal rat
cardiomyocytes
Pre-treatment with
urocortin
Less mitochondrial damage Reduced mitochondrial levels of
phospholipase A2 and
increased mitochondrial levels
of Kir6.1 and PKC-1
Brar
et al.
(2004)
139
Neonatal and adult mouse
cardiomyocytes and
isolated perfused rat
heart
Pre-treatment or
treatment at the time
of reperfusion with
urocortin II and III
Improved cell survival and
small infarct sizes
Protection required Erk1/2
activation; CRH-R2
2/2
cardiomyocytes more
susceptible to injury
Cserepes
et al.
(2007)
176
Neonatal rat
cardiomyocytes
Pre-treatment or
treatment at
reperfusion with
urocortin
Less cardiac enzyme release
and less apoptosis
D.J. Hausenloy and D.M. Yellon 188
b
y
g
u
e
s
t
o
n
J
u
l
y
2
2
,
2
0
1
2
h
t
t
p
:
/
/
c
a
r
d
i
o
v
a
s
c
r
e
s
.
o
x
f
o
r
d
j
o
u
r
n
a
l
s
.
o
r
g
/
D
o
w
n
l
o
a
d
e
d
f
r
o
m
investigated in human volunteers
144
and heart failure
patients,
145
no haemodynamic effect was actually observed
and only increased levels of ACTH and cortisol were demon-
strated. It is interesting to note that urocortin is secreted in
the human heart and there are specic cell-surface recep-
tors (CRH-R2a) present on the cardiomyocyte, suggesting
that the generation of urocortin during myocardial ischae-
mia may act as an autocoid to endogenously protect the
heart in a similar manner to adenosine and bradykinin.
Clearly, the use of exogenously administered urocortin as
an acutely cardioprotective agent in patients presenting
with an acute myocardial infarction will be hampered by
the accompanying haemodynamic effects in the case of uro-
cortin II,
146,147
which has been demonstrated to increase
cardiac output, heart rate, ejection fraction and to induce
systemic vasodilation, making it ideal therapy for cardiac
failure. Urocortin I, which has been reported to have no
haemodynamic effects, may be an alternative agent to use
in this setting, although its hormonal effects in terms of
ACTH production may be problematic.
144,145
6. Transforming growth factor-b
TGF-b refers to a superfamily of cytokines comprising nearly
40 members which have been implicated in a diverse variety
of cellular processes including cardiac development, vascu-
lar brosis, apoptosis, inammation among others (reviewed
in references 148 and 149). The TGF-b1 isoform is the one
most widely distributed within the cardiovascular system.
TGF-b1 is secreted as an inactive latent form which is
then activated within the extracellular space. Active
TGF-b1 binds to the type II TGF-b1 receptor (TbR-II),
which then recruits and dimerizes with TGF-b1 receptor
type I (TbR-I), forming a heterotrimeric complex which
results in the activation of TbR-II and TbR-I intracellular
serinethreonine kinases, leading to the stimulation of and
the Smad pathway, and the PI3K-Akt and MAPKs such as
MEK1/2-Erk1/2 kinase cascades, p38 and JNK.
Initial experimental studies in the early 1990s by Lefer
et al.
150,151
rst identied TGF-b1 as a mediator of acute
cardioprotection. In the rst study, these authors demon-
strated that TGF-b1 pre-treatment of the in vivo or ex
vivo rat heart reduced myocardial injury,
150
whereas in a
subsequent second study, they found that administering
TGF-b1 after the onset of myocardial ischaemia and
30 min before myocardial reperfusion reduced myocardial
infarct size in the in vivo feline heart subjected to 1.5 h
ischaemia and 4.5 h reperfusion.
151
The mechanism of cardi-
oprotection was attributed in these early studies to attenu-
ating two major proponents of myocardial reperfusion
injury, namely endothelial dysfunction and neutrophil acti-
vation. An additional study reported protective effects at
the level of the coronary endothelium.
152
Later studies
demonstrated that TGF-b1 was capable of protecting iso-
lated cardiomyocytes (in the absence of endothelium and
neutrophils).
153,154
Our group was the rst to report that
TGF-b1 could target lethal myocardial reperfusion injury
and limit myocardial infarct size when administered at the
time of myocardial reperfusion.
154
However, subsequent
investigations have described direct cardioprotective
effects on the myocardium through the recruitment of intra-
cellular signal transduction pathways including the MEK1/
2-Erk1/2 component of the RISK pathway (Table 6). Some-
what surprisingly, Chen et al.
155
found that the pre-
treatment of adult rat cardiomyocytes with TGF-b1
improved cell survival following simulated ischaemiareper-
fusion injury and this protective effect was associated with
less Akt and iNOS phosphorylation but greater levels of eNOS
phosphorylation compared with control. Interestingly, the
same group also found that the modulation of cardiomyo-
cyte TGF-b1 mediated the cardioprotection elicited by
nitric oxide donors although the mechanism linking the
two is unclear.
156
7. Stem cell therapy and growth factors
Accumulating evidence supports a paracrine mode of action
in order to explain the benecial effects of adult stem cell
therapy on post-myocardial infarction improvements in
cardiac function, with the secretion by adult stem cells of
Table 6 Acute cardioprotection with transforming growth factor-b1
Study Model Treatment regime Effect Mechanistic insight
Lefer et al.
(1990)
150
In vivo and ex vivo rat
heart
Pre-treatment with TGF-b1 Less myocardial injury First study to demonstrate acute
cardioprotection
Lefer et al.
(1993)
151
In vivo feline heart Pre-treatment with TGF-b1 Reduce myocardial infarct
size
Protection due to less endothelial
dysfunction and neutrophil
activation
Yang et al.
(1999)
153
Adult rat
cardiomyocytes
Pre-treatment with TGF-b1 Reduced cell death, less LDH
release, and less apoptosis
Direct cardioprotection on adult
cardiomyocyte
Mehta et al.
(1999)
177
Isolated perfused rat
heart
Pre-treatment with TGF-b1 Improved myocardial
function
Baxter et al.
(2001)
154
Neonatal rat
cardiomyocytes and
isolated perfused
rat heart
Treatment at the time of
reoxygenation at the
onset of reperfusion
with TGF-b1
Improved cell survival, less
apoptosis, smaller infarct
size
Protection requires activation of
Mek1/2-ERK1/2
Chen et al.
(2001)
155
Adult rat
cardiomyocytes
Pre-treatment with TGF-b1 Reduced cell death and less
apoptosis
Protection associated with less Akt/
iNOS and more eNOS
phosphorylation
Chen et al.
(2003)
178
In vivo rat heart Pre-treatment with TGF-b1 Reduced myocardial infarct
size
Protection associated with less MMP-1
Cardioprotective growth factors 189
b
y
g
u
e
s
t
o
n
J
u
l
y
2
2
,
2
0
1
2
h
t
t
p
:
/
/
c
a
r
d
i
o
v
a
s
c
r
e
s
.
o
x
f
o
r
d
j
o
u
r
n
a
l
s
.
o
r
g
/
D
o
w
n
l
o
a
d
e
d
f
r
o
m
cardioprotective and anti-apoptotic growth factors which
include FGF-2, VEGF, TGF-b, and IGF-1, contributing to the
benecial effects of stem cell therapy, rather than the
engraftment and transdifferentiation of adult stem cells
(reviewed in reference 157). Improving the therapeutic ef-
cacy of stem cell therapy in myocardial regeneration follow-
ing an acute myocardial infarction is a key objective.
Priming stem cells by pre-treatment with growth factors
has emerged as an innovative treatment strategy for enhan-
cing the cytoprotective abilities of stem cells for myocardial
repair. Several growth factors, including FGF-2,
158
IGF-1,
159
and bone morphogenetic protein-2 (BMP-2),
160,161
have been
implicated as promoting cardiomyocyte differentiation and
the cytoprotective potential in stem cells. Hahn et al.
162
demonstrated that the pre-treatment of rat mesenchymal
stems cells with a cocktail comprising FGF-2, IGF-1, and
BMP-2 increased gap-junction formation and improved the
cytoprotective abilities of the stem cells. Whether these
growth factors can be used in a similar manner to improve
the therapeutic efcacy of stem cell therapy in the clinical
setting of an acute myocardial infarction remains to be
seen.
8. Summary and conclusions
There are a number of growth factors which exert a diverse
array of cardiovascular effects including the ability to confer
acute cardioprotection. Interestingly, many of these growth
factors are released by the cardiomyocyte during myocardial
ischaemia, suggesting that they may play a role in endogen-
ous cardioprotection. In this respect, genetic ablation
studies suggest that some of these growth factors which
include FGF-2, VEGF, and urocortin may actually confer
endogenous protection against acute ischaemiareperfusion
injury. These particular growth factors protect the heart by
activating different receptors including protein tyrosine
kinase receptors, cytokines receptors, G-protein-coupled
receptors, and serinethreonine receptors present on the
cardiomyocyte plasma membrane, which then recruit a
number of cardioprotective intracellular signal transduction
pathways including the RISK pathway, many of which termi-
nate on the mitochondria. Importantly, these growth factors
are cardioprotective when administered both prior to myo-
cardial ischaemia and after the onset of ischaemia and at
the time of myocardial reperfusion, making them suitable
for patients undergoing planned cardiac surgery and for
those presenting with an acute myocardial infarction who
are undergoing reperfusion using brinolytic therapy or
primary percutaneous coronary angioplasty. Although many
of the growth factors have been safely used in the clinical
setting for different indications such as cardiac failure, the
challenge will be to rst establish the correct dosing
regimen capable of mediating cardioprotection with the
minimal haemodynamic disturbance, particularly in acute
myocardial infarction patients.
Conict of interest: none declared.
Funding
We would like thank the British Heart Foundation for the
ongoing support. This work was undertaken at UCLH/UCL,
which received a proportion of funding from the Department
of Healths NIHR Biomedical Research Centres funding
scheme.
References
1. Hausenloy DJ, Yellon DM. New directions for protecting the heart against
ischaemia-reperfusion injury: targeting the Reperfusion Injury Salvage
Kinase (RISK)-pathway. Cardiovasc Res 2004;61:448460.
2. Hausenloy DJ, Yellon DM. Survival kinases in ischemic preconditioning
and postconditioning. Cardiovasc Res 2006;70:240253.
3. Hausenloy DJ, Yellon DM. Reperfusion injury salvage kinase signalling:
taking a RISK for cardioprotection. Heart Fail Rev 2007;12:217234.
4. Burley DS, Hamid SA, Baxter GF. Cardioprotective actions of peptide
hormones in myocardial ischemia. Heart Fail Rev 2007;12:279291.
5. Riksen NP, Hausenloy DJ, Yellon DM. Erythropoietin: ready for prime-
time cardioprotection. Trends Pharmacol Sci 2008;29:258267.
6. Karmazyn M, Purdham DM, Rajapurohitam V, Zeidan A. Signalling mech-
anisms underlying the metabolic and other effects of adipokines on the
heart. Cardiovasc Res 2008;79:279286.
7. Yellon DM, Baxter GF. Reperfusion injury revisited: is there a role for
growth factor signaling in limiting lethal reperfusion injury? Trends Car-
diovasc Med 1999;9:245249.
8. Murry CE, Jennings RB, Reimer KA. Preconditioning with ischemia: a
delay of lethal cell injury in ischemic myocardium. Circulation 1986;
74:11241136.
9. Zhao ZQ, Corvera JS, Halkos ME, Kerendi F, Wang NP, Guyton RA et al.
Inhibition of myocardial injury by ischemic postconditioning during
reperfusion: comparison with ischemic preconditioning. Am J Physiol
Heart Circ Physiol 2003;285:H579H588.
10. Hausenloy DJ, Yellon DM. Preconditioning and postconditioning: united
at reperfusion. Pharmacol Ther 2007;116:173191.
11. Hausenloy DJ, Wynne AM, Yellon DM. Ischemic preconditioning targets
the reperfusion phase. Basic Res Cardiol 2007;102:445452.
12. Juhaszova M, Zorov DB, Kim SH, Pepe S, Fu Q, Fishbein KW et al. Glyco-
gen synthase kinase-3beta mediates convergence of protection signaling
to inhibit the mitochondrial permeability transition pore. J Clin Invest
2004;113:15351549.
13. Davidson SM, Hausenloy D, Duchen MR, Yellon DM. Signalling via the
reperfusion injury signalling kinase (RISK) pathway links closure of the
mitochondrial permeability transition pore to cardioprotection. Int J
Biochem Cell Biol 2006;38:414419.
14. Hausenloy DJ, Yellon DM. The mitochondrial permeability transition
pore: its fundamental role in mediating cell death during ischaemia
and reperfusion. J Mol Cell Cardiol 2003;35:339341.
15. Costa AD, Jakob R, Costa CL, Andrukhiv K, West IC, Garlid KD. The mech-
anism by which the mitochondrial ATP-sensitive K channel opening and
H2O2 inhibit the mitochondrial permeability transition. J Biol Chem
2006;281:2080120808.
16. Abdallah Y, Gkatzoia A, Gligorievski D, Kasseckert S, Euler G,
Schluter KD et al. Insulin protects cardiomyocytes against
reoxygenation-induced hypercontracture by a survival pathway target-
ing SR Ca2 storage. Cardiovasc Res 2006;70:346353.
17. Mensah K, Mocanu MM, Yellon DM. Failure to protect the myocardium
against ischemia/reperfusion injury after chronic atorvastatin treat-
ment is recaptured by acute atorvastatin treatment: a potential role
for phosphatase and tensin homolog deleted on chromosome ten?
J Am Coll Cardiol 2005;45:12871291.
18. Lecour S, Suleman N, Deuchar GA, Somers S, Lacerda L, Huisamen B
et al. Pharmacological preconditioning with tumor necrosis factor-alpha
activates signal transducer and activator of transcription-3 at reperfu-
sion without involving classic prosurvival kinases (Akt and extracellular
signal-regulated kinase). Circulation 2005;112:39113918.
19. Boengler K, Buechert A, Heinen Y, Roeskes C, Hilker-Kleiner D,
Heusch G et al. Cardioprotection by ischemic postconditioning is lost
in aged and STAT3-decient mice. Circ Res 2008;102:131135.
20. Garlid KD, Costa AD, Cohen MV, Downey JM, Critz SD. Cyclic GMP and
PKG activate mito K(ATP) channels in isolated mitochondria. Cardiovasc
J S Afr 2004;15:S5.
21. Zatta AJ, Kin H, Lee G, Wang N, Jiang R, Lust R et al. Infarct-sparing
effect of myocardial postconditioning is dependent on protein kinase
C signalling. Cardiovasc Res 2006;70:315324.
22. Jin ZQ, Karliner JS, Vessey DA. Ischaemic postconditioning protects iso-
lated mouse hearts against ischaemia/reperfusion injury via sphingosine
kinase isoform-1 activation. Cardiovasc Res 2008;79:134140.
D.J. Hausenloy and D.M. Yellon 190
b
y
g
u
e
s
t
o
n
J
u
l
y
2
2
,
2
0
1
2
h
t
t
p
:
/
/
c
a
r
d
i
o
v
a
s
c
r
e
s
.
o
x
f
o
r
d
j
o
u
r
n
a
l
s
.
o
r
g
/
D
o
w
n
l
o
a
d
e
d
f
r
o
m
23. Cantley LC. The phosphoinositide 3-kinase pathway. Science 2002;296:
16551657.
24. Oudit GY, Sun H, Kerfant BG, Crackower MA, Penninger JM, Backx PH.
The role of phosphoinositide-3 kinase and PTEN in cardiovascular physi-
ology and disease. J Mol Cell Cardiol 2004;37:449471.
25. Murphy LO, Blenis J. MAPK signal specicity: the right place at the right
time. Trends Biochem Sci 2006;31:268275.
26. Gospodarowicz D. Localisation of a broblast growth factor and its
effect alone and with hydrocortisone on 3T3 cell growth. Nature
1974;249:123127.
27. Detillieux KA, Sheikh F, Kardami E, Cattini PA. Biological activities of
broblast growth factor-2 in the adult myocardium. Cardiovasc Res
2003;57:819.
28. Kardami E, Detillieux K, Ma X, Jiang Z, Santiago JJ, Jimenez SK et al.
Fibroblast growth factor-2 and cardioprotection. Heart Fail Rev 2007;
12:267277.
29. Kapur NK, Rade JJ. Fibroblast growth factor 4 gene therapy for chronic
ischemic heart disease. Trends Cardiovasc Med 2008;18:133141.
30. Yanagisawa-Miwa A, Uchida Y, Nakamura F, Tomaru T, Kido H, Kamijo T
et al. Salvage of infarcted myocardium by angiogenic action of basic
broblast growth factor. Science 1992;257:14011403.
31. Padua RR, Sethi R, Dhalla NS, Kardami E. Basic broblast growth factor
is cardioprotective in ischemia-reperfusion injury. Mol Cell Biochem
1995;143:129135.
32. Horrigan MC, MacIsaac AI, Nicolini FA, Vince DG, Lee P, Ellis SG et al.
Reduction in myocardial infarct size by basic broblast growth factor
after temporary coronary occlusion in a canine model. Circulation
1996;94:19271933.
33. Htun P, Ito WD, Hoefer IE, Schaper J, Schaper W. Intramyocardial infu-
sion of FGF-1 mimics ischemic preconditioning in pig myocardium.
J Mol Cell Cardiol 1998;30:867877.
34. Jiang ZS, Padua RR, Ju H, Doble BW, Jin Y, Hao J et al. Acute protection
of ischemic heart by FGF-2: involvement of FGF-2 receptors and protein
kinase C. Am J Physiol Heart Circ Physiol 2002;282:H1071H1080.
35. Cuevas P, Carceller F, Martinez-Coso V, Cuevas B, Fernandez-Ayerdi A,
Reimers D et al. Cardioprotection from ischemia by broblast growth
factor: role of inducible nitric oxide synthase. Eur J Med Res 1999;4:
517524.
36. Padua RR, Merle PL, Doble BW, Yu CH, Zahradka P, Pierce GN et al.
FGF-2-induced negative inotropism and cardioprotection are inhibited
by chelerythrine: involvement of sarcolemmal calcium-independent
protein kinase C. J Mol Cell Cardiol 1998;30:26952709.
37. Doble BW, Chen Y, Bosc DG, Litcheld DW, Kardami E. Fibroblast growth
factor-2 decreases metabolic coupling and stimulates phosphorylation
as well as masking of connexin43 epitopes in cardiac myocytes. Circ
Res 1996;79:647658.
38. Jiang ZS, Srisakuldee W, Soulet F, Bouche G, Kardami E. Non-angiogenic
FGF-2 protects the ischemic heart from injury, in the presence or
absence of reperfusion. Cardiovasc Res 2004;62:154166.
39. Sheikh F, Sontag DP, Fandrich RR, Kardami E, Cattini PA. Overexpression
of FGF-2 increases cardiac myocyte viability after injury in isolated
mouse hearts. Am J Physiol Heart Circ Physiol 2001;280:H1039H1050.
40. Meij JT, Sheikh F, Jimenez SK, Nickerson PW, Kardami E, Cattini PA.
Exacerbation of myocardial injury in transgenic mice overexpressing
FGF-2 is T cell dependent. Am J Physiol Heart Circ Physiol 2002;282:
H547H555.
41. House SL, Bolte C, Zhou M, Doetschman T, Klevitsky R, Newman G et al.
Cardiac-specic overexpression of broblast growth factor-2 protects
against myocardial dysfunction and infarction in a murine model of
low-ow ischemia. Circulation 2003;108:31403148.
42. Virag JA, Rolle ML, Reece J, Hardouin S, Feigl EO, Murry CE. Fibroblast
growth factor-2 regulates myocardial infarct repair: effects on cell pro-
liferation, scar contraction, and ventricular function. Am J Pathol 2007;
171:14311440.
43. Simons M, Annex BH, Laham RJ, Kleiman N, Henry T, Dauerman H et al.
Pharmacological treatment of coronary artery disease with recombinant
broblast growth factor-2: double-blind, randomized, controlled clini-
cal trial. Circulation 2002;105:788793.
44. Ahn A, Frishman WH, Gutwein A, Passeri J, Nelson M. Therapeutic angio-
genesis: a new treatment approach for ischemic heart diseasepart I.
Cardiol Rev 2008;16:163171.
45. Takahashi N, Seko Y, Noiri E, Tobe K, Kadowaki T, Sabe H et al. Vascular
endothelial growth factor induces activation and subcellular transloca-
tion of focal adhesion kinase (p125FAK) in cultured rat cardiac myo-
cytes. Circ Res 1999;84:11941202.
46. Ladoux A, Frelin C. Hypoxia is a strong inducer of vascular endothelial
growth factor mRNA expression in the heart. Biochem Biophys Res
Commun 1993;195:10051010.
47. Levy AP, Levy NS, Loscalzo J, Calderone A, Takahashi N, Yeo KT et al.
Regulation of vascular endothelial growth factor in cardiac myocytes.
Circ Res 1995;76:758766.
48. Lee SH, Wolf PL, Escudero R, Deutsch R, Jamieson SW,
Thistlethwaite PA. Early expression of angiogenesis factors in acute
myocardial ischemia and infarction. N Engl J Med 2000;342:626633.
49. Luo Z, Diaco M, Murohara T, Ferrara N, Isner JM, Symes JF. Vascular
endothelial growth factor attenuates myocardial ischemia-reperfusion
injury. Ann Thorac Surg 1997;64:993998.
50. Seko Y, Takahashi N, Tobe K, Ueki K, Kadowaki T, Yazaki Y. Vascular endo-
thelial growth factor (VEGF) activates Raf-1, mitogen-activated protein
(MAP) kinases, and S6 kinase (p90rsk) in cultured rat cardiac myocytes.
J Cell Physiol 1998;175:239246.
51. Gerber HP, McMurtrey A, Kowalski J, Yan M, Keyt BA, Dixit V et al. Vas-
cular endothelial growth factor regulates endothelial cell survival
through the phosphatidylinositol 3
0
-kinase/Akt signal transduction
pathway. Requirement for Flk-1/KDR activation. J Biol Chem 1998;
273:3033630343.
52. Kawata H, Yoshida K, Kawamoto A, Kurioka H, Takase E, Sasaki Y et al.
Ischemic preconditioning upregulates vascular endothelial growth
factor mRNA expression and neovascularization via nuclear transloca-
tion of protein kinase C epsilon in the rat ischemic myocardium. Circ
Res 2001;88:696704.
53. Thirunavukkarasu M, Addya S, Juhasz B, Pant R, Zhan L, Surrey S et al.
Heterozygous disruption of Flk-1 receptor leads to myocardial ischaemia
reperfusion injury in mice: application of affymetrix gene chip analysis.
J Cell Mol Med 2008;12:12841302.
54. Addya S, Shiroto K, Turoczi T, Zhan L, Kaga S, Fukuda S et al. Ischemic
preconditioning-mediated cardioprotection is disrupted in heterozygous
Flt-1 (VEGFR-1) knockout mice. J Mol Cell Cardiol 2005;38:345351.
55. Thirunavukkarasu M, Juhasz B, Zhan L, Menon VP, Tosaki A, Otani H et al.
VEGFR1 (Flt-1/2) gene knockout leads to the disruption of VEGF-
mediated signaling through the nitric oxide/heme oxygenase pathway
in ischemic preconditioned myocardium. Free Radic Biol Med 2007;42:
14871495.
56. Kastrup J, Jorgensen E, Ruck A, Tagil K, Glogar D, Ruzyllo Wet al. Direct
intramyocardial plasmid vascular endothelial growth factor-A165 gene
therapy in patients with stable severe angina pectoris. A randomized
double-blind placebo-controlled study: the Euroinject One trial. J Am
Coll Cardiol 2005;45:982988.
57. Fuchs S, Dib N, Cohen BM, Okubagzi P, Diethrich EB, Campbell A et al. A
randomized, double-blind, placebo-controlled, multicenter, pilot study
of the safety and feasibility of catheter-based intramyocardial injection
of AdVEGF121 in patients with refractory advanced coronary artery
disease. Catheter Cardiovasc Interv 2006;68:372378.
58. Henry TD, Annex BH, McKendall GR, Azrin MA, Lopez JJ, Giordano FJ
et al. The VIVA trial: Vascular endothelial growth factor in Ischemia
for Vascular Angiogenesis. Circulation 2003;107:13591365.
59. Sodi-Pallares D, Testelli MR, Fishleder BL, Bisteni A, Medrano GA,
Friedland C et al. Effects of an intravenous infusion of
potassium-insulin-glucose solution on the electrocardiographic signs of
myocardial infarction. A preliminary clinical report. Am J Cardiol
1962;9:166181.
60. Opie LH. Metabolism of free fatty acids, glucose and catecholamines in
acute myocardial infarction. Relation to myocardial ischemia and
infarct size. Am J Cardiol 1975;36:938953.
61. Sack MN, Yellon DM. Insulin therapy as an adjunct to reperfusion after
acute coronary ischemia: a proposed direct myocardial cell survival
effect independent of metabolic modulation. J Am Coll Cardiol 2003;
41:14041407.
62. DeBosch BJ, Muslin AJ. Insulin signaling pathways and cardiac growth.
J Mol Cell Cardiol 2008;44:855864.
63. Baines CP, Wang L, Cohen MV, Downey JM. Myocardial protection by
insulin is dependent on phospatidylinositol 3-kinase but not protein
kinase C or KATP channels in the isolated rabbit heart. Basic Res
Cardiol 1999;94:188198.
64. Jonassen AK, Brar BK, Mjos OD, Sack MN, Latchman DS, Yellon DM.
Insulin administered at reoxygenation exerts a cardioprotective effect
in myocytes by a possible anti-apoptotic mechanism. J Mol Cell
Cardiol 2000;32:757764.
65. Jonassen AK, Sack MN, Mjos OD, Yellon DM. Myocardial protection by
insulin at reperfusion requires early administration and is mediated
Cardioprotective growth factors 191
b
y
g
u
e
s
t
o
n
J
u
l
y
2
2
,
2
0
1
2
h
t
t
p
:
/
/
c
a
r
d
i
o
v
a
s
c
r
e
s
.
o
x
f
o
r
d
j
o
u
r
n
a
l
s
.
o
r
g
/
D
o
w
n
l
o
a
d
e
d
f
r
o
m
via Akt and p70s6 kinase cell-survival signaling. Circ Res 2001;89:
11911198.
66. Gao F, Gao E, Yue TL, Ohlstein EH, Lopez BL, Christopher TA et al. Nitric
oxide mediates the antiapoptotic effect of insulin in myocardial
ischemia-reperfusion: the roles of PI3-kinase, Akt, and endothelial
nitric oxide synthase phosphorylation. Circulation 2002;105:14971502.
67. Fuglesteg BN, Suleman N, Tiron C, Kanhema T, Lacerda L, Andreasen TV
et al. Signal transducer and activator of transcription 3 is involved in the
cardioprotective signalling pathway activated by insulin therapy at
reperfusion. Basic Res Cardiol 2008:444453.
68. Boengler K, Hilker-Kleiner D, Drexler H, Heusch G, Schulz R. The myo-
cardial JAK/STAT pathway: from protection to failure. Pharmacol Ther
2008;120:172185.
69. Hausenloy DJ, Yellon DM. GLP-1 therapy: beyond glucose control. Circu-
lation Heart Failure 2008;1:147149.
70. Pierson RW Jr, Temin HM. The partial purication from calf serum of a
fraction with multiplication-stimulating activity for chicken broblasts
in cell culture and with non-suppressible insulin-like activity. J Cell
Physiol 1972;79:319330.
71. Suleiman MS, Singh RJ, Stewart CE. Apoptosis and the cardiac action of
insulin-like growth factor I. Pharmacol Ther 2007;114:278294.
72. Buerke M, Murohara T, Skurk C, Nuss C, Tomaselli K, Lefer AM. Cardio-
protective effect of insulin-like growth factor I in myocardial ischemia
followed by reperfusion. Proc Natl Acad Sci USA 1995;92:80318035.
73. Li Q, Li B, Wang X, Leri A, Jana KP, Liu Yet al. Overexpression of insulin-
like growth factor-1 in mice protects from myocyte death after
infarction, attenuating ventricular dilation, wall stress, and cardiac
hypertrophy. J Clin Invest 1997;100:19911999.
74. Kulik G, Klippel A, Weber MJ. Antiapoptotic signalling by the insulin-like
growth factor I receptor, phosphatidylinositol 3-kinase, and Akt. Mol
Cell Biol 1997;17:15951606.
75. Parrizas M, Saltiel AR, LeRoith D. Insulin-like growth factor 1 inhibits
apoptosis using the phosphatidylinositol 3
0
-kinase and mitogen-
activated protein kinase pathways. J Biol Chem 1997;272:154161.
76. Fujio Y, Nguyen T, Wencker D, Kitsis RN, Walsh K. Akt promotes survival
of cardiomyocytes in vitro and protects against ischemia-reperfusion
injury in mouse heart. Circulation 2000;101:660667.
77. Yamashita K, Kajstura J, Discher DJ, Wasserlauf BJ, Bishopric NH,
Anversa P et al. Reperfusion-activated Akt kinase prevents apoptosis
in transgenic mouse hearts overexpressing insulin-like growth
factor-1. Circ Res 2001;88:609614.
78. Yamamura T, Otani H, Nakao Y, Hattori R, Osako M, Imamura H. IGF-I dif-
ferentially regulates Bcl-xL and Bax and confers myocardial protection
in the rat heart. Am J Physiol Heart Circ Physiol 2001;280:
H1191H1200.
79. Pi Y, Goldenthal MJ, Marin-Garcia J. Mitochondrial involvement in IGF-1
induced protection of cardiomyocytes against hypoxia/reoxygenation
injury. Mol Cell Biochem 2007;301:181189.
80. Chao W, Matsui T, Novikov MS, Tao J, Li L, Liu H et al. Strategic advan-
tages of insulin-like growth factor-I expression for cardioprotection.
J Gene Med 2003;5:277286.
81. Kaplan RC, Strickler HD, Rohan TE, Muzumdar R, Brown DL. Insulin-like
growth factors and coronary heart disease. Cardiol Rev 2005;13:3539.
82. Conti E, Andreotti F, Sciahbasi A, Riccardi P, Marra G, Menini E et al.
Markedly reduced insulin-like growth factor-1 in the acute phase of
myocardial infarction. J Am Coll Cardiol 2001;38:2632.
83. Al Obaidi MK, Hon JK, Stubbs PJ, Barnes J, Amersey RA, Dahdal M et al.
Plasma insulin-like growth factor-1 elevated in mild-to-moderate but
not severe heart failure. Am Heart J 2001;142:E10.
84. Juul A, Scheike T, Davidsen M, Gyllenborg J, Jorgensen T. Low serum
insulin-like growth factor I is associated with increased risk of ischemic
heart disease: a population-based case-control study. Circulation 2002;
106:939944.
85. Petretta M, Colao A, Sardu C, Scopacasa F, Marzullo P, Pivonello R et al.
NT-proBNP, IGF-I and survival in patients with chronic heart failure.
Growth Horm IGF Res 2007;17:288296.
86. Donath MY, Jenni R, Brunner HP, Anrig M, Kohli S, Glatz Y et al. Cardio-
vascular and metabolic effects of insulin-like growth factor I at rest and
during exercise in humans. J Clin Endocrinol Metab 1996;81:40894094.
87. Donath MY, Sutsch G, Yan XW, Piva B, Brunner HP, Glatz Y et al. Acute
cardiovascular effects of insulin-like growth factor I in patients with
chronic heart failure. J Clin Endocrinol Metab 1998;83:31773183.
88. Yoshida K, Taga T, Saito M, Suematsu S, Kumanogoh A, Tanaka T et al.
Targeted disruption of gp130, a common signal transducer for the inter-
leukin 6 family of cytokines, leads to myocardial and hematological dis-
orders. Proc Natl Acad Sci USA 1996;93:407411.
89. Pennica D, King KL, Shaw KJ, Luis E, Rullamas J, Luoh SM et al.
Expression cloning of cardiotrophin 1, a cytokine that induces cardiac
myocyte hypertrophy. Proc Natl Acad Sci USA 1995;92:11421146.
90. Sheng Z, Pennica D, Wood WI, Chien KR. Cardiotrophin-1 displays early
expression in the murine heart tube and promotes cardiac myocyte sur-
vival. Development 1996;122:419428.
91. Sheng Z, Knowlton K, Chen J, Hoshijima M, Brown JH, Chien KR. Cardio-
trophin 1 (CT-1) inhibition of cardiac myocyte apoptosis via a mitogen-
activated protein kinase-dependent pathway. Divergence from down-
stream CT-1 signals for myocardial cell hypertrophy. J Biol Chem
1997;272:57835791.
92. Stephanou A, Brar B, Heads R, Knight RD, Marber MS, Pennica D et al.
Cardiotrophin-1 induces heat shock protein accumulation in cultured
cardiac cells and protects them from stressful stimuli. J Mol Cell
Cardiol 1998;30:849855.
93. Brar BK, Stephanou A, Pennica D, Latchman DS. CT-1 mediated cardio-
protection against ischaemic re-oxygenation injury is mediated by PI3
kinase, Akt and MEK1/2 pathways. Cytokine 2001;16:9396.
94. Brar BK, Stephanou A, Liao Z, OLeary RM, Pennica D, Yellon DM et al.
Cardiotrophin-1 can protect cardiac myocytes from injury when added
both prior to simulated ischaemia and at reoxygenation. Cardiovasc
Res 2001;51:265274.
95. Liao Z, Brar BK, Cai Q, Stephanou A, OLeary RM, Pennica D et al.
Cardiotrophin-1 (CT-1) can protect the adult heart from injury when
added both prior to ischaemia and at reperfusion. Cardiovasc Res
2002;53:902910.
96. Ghosh S, Ng LL, Talwar S, Squire IB, Galinanes M. Cardiotrophin-1 pro-
tects the human myocardium from ischemic injury. Comparison with
the rst and second window of protection by ischemic preconditioning.
Cardiovasc Res 2000;48:440447.
97. Lopez N, Diez J, Fortuno MA. Characterization of the protective effects
of cardiotrophin-1 against non-ischemic death stimuli in adult cardio-
myocytes. Cytokine 2005;30:282292.
98. Hishinuma S, Funamoto M, Fujio Y, Kunisada K, Yamauchi-Takihara K.
Hypoxic stress induces cardiotrophin-1 expression in cardiac myocytes.
Biochem Biophys Res Commun 1999;264:436440.
99. Aoyama T, Takimoto Y, Pennica D, Inoue R, Shinoda E, Hattori R et al.
Augmented expression of cardiotrophin-1 and its receptor component,
gp130, in both left and right ventricles after myocardial infarction in
the rat. J Mol Cell Cardiol 2000;32:18211830.
100. Gritman K, Van Winkle DM, Lorentz CU, Pennica D, Habecker BA. The
lack of cardiotrophin-1 alters expression of interleukin-6 and leukemia
inhibitory factor mRNA but does not impair cardiac injury response.
Cytokine 2006;36:916.
101. Jougasaki M, Leskinen H, Larsen AM, Luchner A, Cataliotti A, Tachibana I
et al. Ventricular cardiotrophin-1 activation precedes BNP in exper-
imental heart failure. Peptides 2003;24:889892.
102. Zolk O, Ng LL, OBrien RJ, Weyand M, Eschenhagen T. Augmented
expression of cardiotrophin-1 in failing human hearts is accompanied
by diminished glycoprotein 130 receptor protein abundance. Circulation
2002;106:14421446.
103. Pan J, Fukuda K, Saito M, Matsuzaki J, Kodama H, Sano M et al. Mechan-
ical stretch activates the JAK/STAT pathway in rat cardiomyocytes. Circ
Res 1999;84:11271136.
104. Asai S, Saito Y, Kuwahara K, Mizuno Y, Yoshimura M, Higashikubo C et al.
The heart is a source of circulating cardiotrophin-1 in humans. Biochem
Biophys Res Commun 2000;279:320323.
105. Talwar S, Squire IB, Downie PF, Davies JE, Ng LL. Plasma N terminal pro-
brain natriuretic peptide and cardiotrophin 1 are raised in unstable
angina. Heart 2000;84:421424.
106. Talwar S, Squire IB, OBrien RJ, Downie PF, Davies JE, Ng LL. Plasma
cardiotrophin-1 following acute myocardial infarction: relationship
with left ventricular systolic dysfunction. Clin Sci (Lond) 2002;102:
914.
107. Talwar S, Downie PF, Squire IB, Davies JE, Barnett DB, Ng LL. Plasma N-
terminal pro BNP and cardiotrophin-1 are elevated in aortic stenosis.
Eur J Heart Fail 2001;3:1519.
108. Talwar S, Squire IB, Davies JE, Ng LL. The effect of valvular regurgita-
tion on plasma Cardiotrophin-1 in patients with normal left ventricular
systolic function. Eur J Heart Fail 2000;2:387391.
109. Gonzalez A, Lopez B, Martin-Raymondi D, Lozano E, Varo N, Barba J
et al. Usefulness of plasma cardiotrophin-1 in assessment of left ventri-
cular hypertrophy regression in hypertensive patients. J Hypertens
2005;23:22972304.
110. Talwar S, Downie PF, Squire IB, Barnett DB, Davies JD, Ng LL. An immu-
noluminometric assay for cardiotrophin-1: a newly identied cytokine is
D.J. Hausenloy and D.M. Yellon 192
b
y
g
u
e
s
t
o
n
J
u
l
y
2
2
,
2
0
1
2
h
t
t
p
:
/
/
c
a
r
d
i
o
v
a
s
c
r
e
s
.
o
x
f
o
r
d
j
o
u
r
n
a
l
s
.
o
r
g
/
D
o
w
n
l
o
a
d
e
d
f
r
o
m
present in normal human plasma and is increased in heart failure.
Biochem Biophys Res Commun 1999;261:567571.
111. Talwar S, Squire IB, Downie PF, OBrien RJ, Davies JE, Ng LL. Elevated
circulating cardiotrophin-1 in heart failure: relationship with par-
ameters of left ventricular systolic dysfunction. Clin Sci (Lond) 2000;
99:8388.
112. Pennica D, Shaw KJ, Swanson TA, Moore MW, Shelton DL, Zioncheck KA
et al. Cardiotrophin-1. Biological activities and binding to the leukemia
inhibitory factor receptor/gp130 signaling complex. J Biol Chem 1995;
270:1091510922.
113. Carpenter CL, Auger KR, Chanudhuri M, Yoakim M, Schaffhausen B,
Shoelson S et al. Phosphoinositide 3-kinase is activated by phosphopep-
tides that bind to the SH2 domains of the 85-kDa subunit. J Biol Chem
1993;268:94789483.
114. Gu H, Maeda H, Moon JJ, Lord JD, Yoakim M, Nelson BH et al. New role
for Shc in activation of the phosphatidylinositol 3-kinase/Akt pathway.
Mol Cell Biol 2000;20:71097120.
115. Kuwahara K, Saito Y, Kishimoto I, Miyamoto Y, Harada M, Ogawa E et al.
Cardiotrophin-1 phosphorylates akt and BAD, and prolongs cell survival
via a PI3K-dependent pathway in cardiac myocytes. J Mol Cell Cardiol
2000;32:13851394.
116. Craig R, Wagner M, McCardle T, Craig AG, Glembotski CC. The cytopro-
tective effects of the glycoprotein 130 receptor-coupled cytokine,
cardiotrophin-1, require activation of NF-kappa B. J Biol Chem 2001;
276:3762137629.
117. Ruixing Y, Dezhai Y, Jiaquan L. Effects of cardiotrophin-1 on hemody-
namics and cardiomyocyte apoptosis in rats with acute myocardial
infarction. J Med Invest 2004;51:2937.
118. Vaughan J, Donaldson C, Bittencourt J, Perrin MH, Lewis K, Sutton S
et al. Urocortin, a mammalian neuropeptide related to sh urotensin I
and to corticotropin-releasing factor. Nature 1995;378:287292.
119. Takahashi K, Totsune K, Murakami O, Shibahara S. Urocortins as cardio-
vascular peptides. Peptides 2004;25:17231731.
120. Davidson SM, Rybka AE, Townsend PA. The powerful cardioprotective
effects of urocortin and the corticotropin releasing hormone (CRH)
family. Biochem Pharmacol 2009;77:141150.
121. Parkes DG, Vaughan J, Rivier J, Vale W, May CN. Cardiac inotropic
actions of urocortin in conscious sheep. Am J Physiol 1997;272:
H2115H2122.
122. Coste SC, Kesterson RA, Heldwein KA, Stevens SL, Heard AD, Hollis JH
et al. Abnormal adaptations to stress and impaired cardiovascular func-
tion in mice lacking corticotropin-releasing hormone receptor-2. Nat
Genet 2000;24:403409.
123. Okosi A, Brar BK, Chan M, Dsouza L, Smith E, Stephanou A et al.
Expression and protective effects of urocortin in cardiac myocytes.
Neuropeptides 1998;32:167171.
124. Knight RA, Chen-Scarabelli C, Yuan Z, McCauley RB, Di Rezze J,
Scarabelli GM et al. Cardiac release of urocortin precedes the occur-
rence of irreversible myocardial damage in the rat heart exposed to
ischemia/reperfusion injury. FEBS Lett 2008;582:984990.
125. Brar BK, Stephanou A, Okosi A, Lawrence KM, Knight RA, Marber MS
et al. CRH-like peptides protect cardiac myocytes from lethal ischaemic
injury. Mol Cell Endocrinol 1999;158:5563.
126. Brar BK, Jonassen AK, Stephanou A, Santilli G, Railson J, Knight RA et al.
Urocortin protects against ischemic and reperfusion injury via a MAPK-
dependent pathway. J Biol Chem 2000;275:85088514.
127. Brar BK, Stephanou A, Knight R, Latchman DS. Activation of protein
kinase B/Akt by urocortin is essential for its ability to protect cardiac
cells against hypoxia/reoxygenation-induced cell death. J Mol Cell
Cardiol 2002;34:483492.
128. Stenzel P, Kesterson R, Yeung W, Cone RD, Rittenberg MB,
Stenzel-Poore MP. Identication of a novel murine receptor for
corticotropin-releasing hormone expressed in the heart. Mol Endocrinol
1995;9:637645.
129. Chen R, Lewis KA, Perrin MH, Vale WW. Expression cloning of a human
corticotropin-releasing-factor receptor. Proc Natl Acad Sci USA 1993;
90:89678971.
130. Kimura Y, Takahashi K, Totsune K, Muramatsu Y, Kaneko C, Darnel AD
et al. Expression of urocortin and corticotropin-releasing factor recep-
tor subtypes in the human heart. J Clin Endocrinol Metab 2002;87:
340346.
131. Bondeva T, Pirola L, Bulgarelli-Leva G, Rubio I, Wetzker R, Wymann MP.
Bifurcation of lipid and protein kinase signals of PI3Kgamma to the
protein kinases PKB and MAPK. Science 1998;282:293296.
132. Schulman D, Latchman DS, Yellon DM. Urocortin protects the heart from
reperfusion injury via upregulation of p42/p44 MAPK signaling pathway.
Am J Physiol Heart Circ Physiol 2002;283:H1481H1488.
133. Lawrence KM, Chanalaris A, Scarabelli T, Hubank M, Pasini E,
Townsend PA et al. K(ATP) channel gene expression is induced by urocor-
tin and mediates its cardioprotective effect. Circulation 2002;106:
15561562.
134. Gordon JM, Dusting GJ, Woodman OL, Ritchie RH. Cardioprotective
action of CRF peptide urocortin against simulated ischemia in adult
rat cardiomyocytes. Am J Physiol Heart Circ Physiol 2003;284:
H330H336.
135. Lawrence KM, Townsend PA, Davidson SM, Carroll CJ, Eaton S, Hubank M
et al. The cardioprotective effect of urocortin during ischaemia/reper-
fusion involves the prevention of mitochondrial damage. Biochem
Biophys Res Commun 2004;321:479486.
136. Lawrence KM, Scarabelli TM, Turtle L, Chanalaris A, Townsend PA,
Carroll CJ et al. Urocortin protects cardiac myocytes from ischemia/
reperfusion injury by attenuating calcium-insensitive phospholipase A2
gene expression. FASEB J 2003;17:23132315.
137. Townsend PA, Davidson SM, Clarke SJ, Khaliulin I, Carroll CJ,
Scarabelli TM et al. Urocortin prevents mitochondrial permeability tran-
sition in response to reperfusion injury indirectly by reducing oxidative
stress. Am J Physiol Heart Circ Physiol 2007;293:H928H938.
138. Valentim L, Laurence KM, Townsend PA, Carroll CJ, Soond S,
Scarabelli TM et al. Urocortin inhibits Beclin1-mediated autophagic
cell death in cardiac myocytes exposed to ischaemia/reperfusion
injury. J Mol Cell Cardiol 2006;40:846852.
139. Brar BK, Jonassen AK, Egorina EM, Chen A, Negro A, Perrin MH et al.
Urocortin-II and urocortin-III are cardioprotective against ischemia
reperfusion injury: an essential endogenous cardioprotective role for
corticotropin releasing factor receptor type 2 in the murine heart.
Endocrinology 2004;145:2435.
140. Chanalaris A, Lawrence KM, Stephanou A, Knight RD, Hsu SY, Hsueh AJ
et al. Protective effects of the urocortin homologues stresscopin (SCP)
and stresscopin-related peptide (SRP) against hypoxia/reoxygenation
injury in rat neonatal cardiomyocytes. J Mol Cell Cardiol 2003;35:
12951305.
141. Nishikimi T, Miyata A, Horio T, Yoshihara F, Nagaya N, Takishita S et al.
Urocortin, a member of the corticotropin-releasing factor family, in
normal and diseased heart. Am J Physiol Heart Circ Physiol 2000;279:
H3031H3039.
142. Ikeda K, Tojo K, Tokudome G, Ohta M, Sugimoto K, Tamura T et al.
Cardiac expression of urocortin (Ucn) in diseased heart; preliminary
results on possible involvement of Ucn in pathophysiology of cardiac dis-
eases. Mol Cell Biochem 2003;252:2532.
143. Ng LL, Loke IW, OBrien RJ, Squire IB, Davies JE. Plasma urocortin in
human systolic heart failure. Clin Sci (Lond) 2004;106:383388.
144. Davis ME, Pemberton CJ, Yandle TG, Lainchbury JG, Rademaker MT,
Nicholls MG et al. Urocortin-1 infusion in normal humans. J Clin Endocri-
nol Metab 2004;89:14021409.
145. Davis ME, Pemberton CJ, Yandle TG, Lainchbury JG, Rademaker MT,
Nicholls MG et al. Effect of urocortin 1 infusion in humans with stable
congestive cardiac failure. Clin Sci (Lond) 2005;109:381388.
146. Davis ME, Pemberton CJ, Yandle TG, Fisher SF, Lainchbury JG,
Frampton CM et al. Urocortin 2 infusion in healthy humans: hemody-
namic, neurohormonal, and renal responses. J Am Coll Cardiol 2007;
49:461471.
147. Davis ME, Pemberton CJ, Yandle TG, Fisher SF, Lainchbury JG,
Frampton CM et al. Urocortin 2 infusion in human heart failure. Eur
Heart J 2007;28:25892597.
148. Hermonat PL, Li D, Yang B, Mehta JL. Mechanism of action and delivery
possibilities for TGFbeta1 in the treatment of myocardial ischemia. Car-
diovasc Res 2007;74:235243.
149. Ruiz-Ortega M, Rodriguez-Vita J, Sanchez-Lopez E, Carvajal G, Egido J.
TGF-beta signaling in vascular brosis. Cardiovasc Res 2007;74:
196206.
150. Lefer AM, Tsao P, Aoki N, Palladino MA Jr. Mediation of cardioprotection
by transforming growth factor-beta. Science 1990;249:6164.
151. Lefer AM, Ma XL, Weyrich AS, Scalia R. Mechanism of the cardioprotec-
tive effect of transforming growth factor beta 1 in feline myocardial
ischemia and reperfusion. Proc Natl Acad Sci USA 1993;90:10181022.
152. Keller M, Kong Y, Robertson AD, Horwitz L. Prevention of coronary vas-
cular abnormalities early in reperfusion with TGF-beta may not
prevent late coronary vascular injury. J Cardiovasc Pharmacol 1997;
30:197204.
Cardioprotective growth factors 193
b
y
g
u
e
s
t
o
n
J
u
l
y
2
2
,
2
0
1
2
h
t
t
p
:
/
/
c
a
r
d
i
o
v
a
s
c
r
e
s
.
o
x
f
o
r
d
j
o
u
r
n
a
l
s
.
o
r
g
/
D
o
w
n
l
o
a
d
e
d
f
r
o
m
153. Yang BC, Zander DS, Mehta JL. Hypoxia-reoxygenation-induced apopto-
sis in cultured adult rat myocytes and the protective effect of platelets
and transforming growth factor-beta(1). J Pharmacol Exp Ther 1999;
291:733738.
154. Baxter GF, Mocanu MM, Brar BK, Latchman DS, Yellon DM. Cardioprotec-
tive effects of transforming growth factor-beta1 during early reoxy-
genation or reperfusion are mediated by p42/p44 MAPK. J Cardiovasc
Pharmacol 2001;38:930939.
155. Chen H, Li D, Saldeen T, Mehta JL. TGF-beta(1) modulates NOS
expression and phosphorylation of Akt/PKB in rat myocytes exposed to
hypoxia-reoxygenation. Am J Physiol Heart Circ Physiol 2001;281:
H1035H1039.
156. Mehta JL, Chen HJ, Li DY. Protection of myocytes from
hypoxia-reoxygenation injury by nitric oxide is mediated by modulation
of transforming growth factor-beta1. Circulation 2002;105:22062211.
157. Gnecchi M, Zhang Z, Ni A, Dzau VJ. Paracrine mechanisms in adult stem
cell signaling and therapy. Circ Res 2008;103:12041219.
158. Rosenblatt-Velin N, Lepore MG, Cartoni C, Beermann F, Pedrazzini T.
FGF-2 controls the differentiation of resident cardiac precursors into
functional cardiomyocytes. J Clin Invest 2005;115:17241733.
159. Kodis T, de Bruin JL, Yamane T, Balsam LB, Lebl DR, Swijnenburg RJ
et al. Insulin-like growth factor promotes engraftment, differentiation,
and functional improvement after transfer of embryonic stem cells for
myocardial restoration. Stem Cells 2004;22:12391245.
160. Ghosh-Choudhury N, Abboud SL, Mahimainathan L, Chandrasekar B,
Choudhury GG. Phosphatidylinositol 3-kinase regulates bone morpho-
genetic protein-2 (BMP-2)-induced myocyte enhancer factor
2A-dependent transcription of BMP-2 gene in cardiomyocyte precursor
cells. J Biol Chem 2003;278:2199822005.
161. Schultheiss TM, Burch JB, Lassar AB. A role for bone morphogenetic pro-
teins in the induction of cardiac myogenesis. Genes Dev 1997;11:
451462.
162. Hahn JY, Cho HJ, Kang HJ, Kim TS, Kim MH, Chung JH et al. Pre-
treatment of mesenchymal stem cells with a combination of growth
factors enhances gap junction formation, cytoprotective effect on car-
diomyocytes, and therapeutic efcacy for myocardial infarction. J Am
Coll Cardiol 2008;51:933943.
163. Cuevas P, Carceller F, Cuevas B, Gimenez-Gallego G, Martinez-Coso V. A
non-mitogenic form of acidic broblast growth factor reduces neutro-
phil inltration in rat ischemic reperfused heart. Eur J Med Res 1997;
2:139143.
164. Cuevas P, Reimers D, Carceller F, Martinez-Coso V, Redondo-Horcajo M,
Saenz de Tejada I et al. Fibroblast growth factor-1 prevents myocardial
apoptosis triggered by ischemia reperfusion injury. Eur J Med Res 1997;
2:465468.
165. Horrigan MC, Malycky JL, Ellis SG, Topol EJ, Nicolini FA. Reduction in
myocardial infarct size by basic broblast growth factor following
coronary occlusion in a canine model. Int J Cardiol 1999;68(Suppl. 1):
S85S91.
166. Buehler A, Martire A, Strohm C, Wolfram S, Fernandez B, Palmen M
et al. Angiogenesis-independent cardioprotection in FGF-1 transgenic
mice. Cardiovasc Res 2002;55:768777.
167. Palmen M, Daemen MJ, De Windt LJ, Willems J, Dassen WR, Heeneman S
et al. Fibroblast growth factor-1 improves cardiac functional recovery
and enhances cell survival after ischemia and reperfusion: a broblast
growth factor receptor, protein kinase C, and tyrosine kinase-dependent
mechanism. J Am Coll Cardiol 2004;44:11131123.
168. House SL, Branch K, Newman G, Doetschman T, Schultz JJ. Cardiopro-
tection induced by cardiac-specic overexpression of broblast growth
factor-2 is mediated by the MAPK cascade. Am J Physiol Heart Circ
Physiol 2005;289:H2167H2175.
169. Gao F, Tao L, Yan W, Gao E, Liu HR, Lopez BL et al. Early anti-apoptosis
treatment reduces myocardial infarct size after a prolonged reperfu-
sion. Apoptosis 2004;9:553559.
170. Fuglesteg BN, Tiron C, Jonassen AK, Mjos OD, Ytrehus K. Pre-treatment
with insulin before ischemia reduces infarct size in Langendorff per-
fused rat hearts. Acta Physiol (Oxf) 2009;195:273282.
171. Vogt AM, Htun P, Kluge A, Zimmermann R, Schaper W. Insulin-like growth
factor-II delays myocardial infarction in experimental coronary artery
occlusion. Cardiovasc Res 1997;33:469477.
172. Wang L, Ma W, Markovich R, Chen JW, Wang PH. Regulation of cardio-
myocyte apoptotic signaling by insulin-like growth factor I. Circ Res
1998;83:516522.
173. Otani H, Yamamura T, Nakao Y, Hattori R, Kawaguchi H, Osako M et al.
Insulin-like growth factor-I improves recovery of cardiac performance
during reperfusion in isolated rat heart by a wortmannin-sensitive
mechanism. J Cardiovasc Pharmacol 2000;35:275281.
174. Hong F, Kwon SJ, Jhun BS, Kim SS, Ha J, Kim SJ et al. Insulin-like growth
factor-1 protects H9c2 cardiac myoblasts from oxidative stress-induced
apoptosis via phosphatidylinositol 3-kinase and extracellular signal-
regulated kinase pathways. Life Sci 2001;68:10951105.
175. Scarabelli TM, Pasini E, Stephanou A, Comini L, Curello S, Raddino R
et al. Urocortin promotes hemodynamic and bioenergetic recovery
and improves cell survival in the isolated rat heart exposed to ische-
mia/reperfusion. J Am Coll Cardiol 2002;40:155161.
176. Cserepes B, Jancso G, Gasz B, Racz B, Ferenc A, Benko L et al. Cardio-
protective action of urocortin in early pre- and postconditioning. Ann NY
Acad Sci 2007;1095:228239.
177. Mehta JL, Yang BC, Strates BS, Mehta P. Role of TGF-beta1 in platelet-
mediated cardioprotection during ischemia-reperfusion in isolated rat
hearts. Growth Factors 1999;16:179190.
178. Chen H, Li D, Saldeen T, Mehta JL. TGF-beta 1 attenuates myocardial
ischemia-reperfusion injury via inhibition of upregulation of MMP-1.
Am J Physiol Heart Circ Physiol 2003;284:H1612H1617.
D.J. Hausenloy and D.M. Yellon 194
b
y
g
u
e
s
t
o
n
J
u
l
y
2
2
,
2
0
1
2
h
t
t
p
:
/
/
c
a
r
d
i
o
v
a
s
c
r
e
s
.
o
x
f
o
r
d
j
o
u
r
n
a
l
s
.
o
r
g
/
D
o
w
n
l
o
a
d
e
d
f
r
o
m
You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Mitochondrial Dysfunction and Biotransformation of Bet-Carboline AlkaloidsDocument11 pagesMitochondrial Dysfunction and Biotransformation of Bet-Carboline AlkaloidsAbhel CalderonNo ratings yet
- Alicia B. Pomilio Et Al - Ayahoasca: An Experimental Psychosis That Mirrors The Transmethylation Hypothesis of SchizophreniaDocument23 pagesAlicia B. Pomilio Et Al - Ayahoasca: An Experimental Psychosis That Mirrors The Transmethylation Hypothesis of SchizophreniaPoloGreenNo ratings yet
- A Clockwork Web Circadian Timing in BrainDocument13 pagesA Clockwork Web Circadian Timing in BrainAbhel CalderonNo ratings yet
- Conexiones Entre Sistema Nervioso y Sistema InmuneDocument29 pagesConexiones Entre Sistema Nervioso y Sistema InmuneAbhel CalderonNo ratings yet
- Abnormal Energy Regulation in Early LifeDocument9 pagesAbnormal Energy Regulation in Early LifeAbhel CalderonNo ratings yet
- A Model of Global Cerebral IschemiaDocument8 pagesA Model of Global Cerebral IschemiaSociedad Peruana De Fisiología FisiopatologíaNo ratings yet
- Acute Phase ProteinsDocument4 pagesAcute Phase ProteinsAbhel CalderonNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Biochemistry of HormonesIDocument24 pagesBiochemistry of HormonesIStephie GhassanNo ratings yet
- Mechanism of Action of Thyroid HormoneDocument4 pagesMechanism of Action of Thyroid HormonejaleelkabdulNo ratings yet
- Molecular Basis of Type 2 DiabetesDocument22 pagesMolecular Basis of Type 2 DiabetespimpellerNo ratings yet
- Molecular and Cellular Mechanisms of BiosignalingDocument86 pagesMolecular and Cellular Mechanisms of BiosignalingJon QNo ratings yet
- MCQ of Neurochemistry and Signal Transduction-2022-FinalDocument6 pagesMCQ of Neurochemistry and Signal Transduction-2022-FinalKaif AliNo ratings yet
- Enzymes As Targets of Drug Action: An Overview: ArticleDocument13 pagesEnzymes As Targets of Drug Action: An Overview: ArticleSalehuddin Karaeng MattawangNo ratings yet
- Medical Complications of Type 2 DiabetesDocument422 pagesMedical Complications of Type 2 DiabetesMayracpp.16No ratings yet
- Jurnal Tirosin Kinase 4Document13 pagesJurnal Tirosin Kinase 4Maya SariNo ratings yet
- General Types of Hormone Receptors:: Receptors Function and Signal TransductionDocument12 pagesGeneral Types of Hormone Receptors:: Receptors Function and Signal Transductionmamoun mufarraqNo ratings yet
- Cell and Molecular Biology: Gerald KarpDocument53 pagesCell and Molecular Biology: Gerald Karppat ongNo ratings yet
- Biology 10Th Edition Raven Test Bank Full Chapter PDFDocument36 pagesBiology 10Th Edition Raven Test Bank Full Chapter PDFlewis.barnes1000100% (12)
- Chapter 2 Systemic Response To Injury and Metabolic Support PDFDocument28 pagesChapter 2 Systemic Response To Injury and Metabolic Support PDFGian Carlo RabagoNo ratings yet
- Protein KinasesDocument494 pagesProtein KinaseslguerreroNo ratings yet
- Cell Communication PDFDocument109 pagesCell Communication PDFediaz_956003100% (1)
- Drug Receptor TheoryDocument9 pagesDrug Receptor TheoryFish YanNo ratings yet
- Mechanisms of Signal Transduction: Growth Factors Back To The TopDocument10 pagesMechanisms of Signal Transduction: Growth Factors Back To The TopAichsaniarNo ratings yet
- Enzyme Linked Receptors LectureDocument52 pagesEnzyme Linked Receptors LectureJason PastisNo ratings yet
- Durruty, Et Al (2019) Pathogenesis of Type 2 DiabetesDocument19 pagesDurruty, Et Al (2019) Pathogenesis of Type 2 Diabetestantry puspitasariNo ratings yet
- Insulin and GlucagonDocument11 pagesInsulin and GlucagonNaman GuptaNo ratings yet
- Signal Transduction in Prokaryotes and Eukaryotes-FinalDocument66 pagesSignal Transduction in Prokaryotes and Eukaryotes-FinalAsif gill0% (1)
- Doctors in Trailing Step 1Document473 pagesDoctors in Trailing Step 1Aneesha Chopra100% (2)
- NAD+ Replenishment Improves Lifespan and Healthspan in Ataxia Telangiectasia Models Via Mitophagy and DNA RepairDocument47 pagesNAD+ Replenishment Improves Lifespan and Healthspan in Ataxia Telangiectasia Models Via Mitophagy and DNA Repairender000100% (1)