Professional Documents
Culture Documents
Error Anestesia Espinal
Uploaded by
Juan Mantilla LinaresCopyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Error Anestesia Espinal
Uploaded by
Juan Mantilla LinaresCopyright:
Available Formats
Error anestesia espinal : los mecanismos de gestin y prevencin
1 . P. D. W. Fettes1 , *,
2 . J.-R. Jansson2 y
3 . J. A. W. Wildsmith1
+ Afiliaciones de los autores
1 . Departamento de Anestesia 1Universidad , Ninewells Hospital y la Facultad de Medicina ,
Dundee DD1 9SY , Reino Unido
2 . 2AstraZeneca I + D SE- 151 85 , Sdertlje , Suecia
1 . * Autor para correspondencia. E - mail: paulfettes@nhs.net
Aceptado el 2 de abril de 2009.
Siguiente seccin
abstracto
Aunque espinal ( subaracnoidea o intratecal ) anestesia es generalmente considerado como
uno de los tipos ms confiables de mtodos de bloques regionales , se ha reconocido desde
hace tiempo la posibilidad de fracaso . Tratar con un anestsico espinal, que es de alguna
manera inadecuada puede ser muy difcil , de modo que , la tcnica debe ser realizado de una
manera que reduce al mnimo el riesgo de la anestesia regional . Por lo tanto , los mdicos
deben tener en cuenta todos los posibles mecanismos de fallo para que, siempre que sea
posible , estos mecanismos pueden ser evitados. Esta revisin ha considerado los
mecanismos de una manera secuencial : problemas con la puncin lumbar , los errores en la
preparacin y la inyeccin de soluciones inadecuadas ; difusin de las drogas a travs del
lquido cefalorraqudeo , insuficiencia de la accin del frmaco en el tejido nervioso , y ms
dificultades relacionadas con el proceso asistencial que el bloque actual . Se discuten las
tcnicas para reducir al mnimo la posibilidad de fracaso , todos ellos requieren , en esencia,
mucha atencin al detalle. Las opciones para la gestin de un bloque inadecuada incluyen la
repeticin de la inyeccin , la manipulacin de la postura del paciente para fomentar una
mayor propagacin de la solucin inyectada , la suplementacin con la infiltracin de
anestsico local por el cirujano , el uso de la sedacin sistmica o frmacos analgsicos , y
recurrir a la anestesia general . Procedimientos de seguimiento deben incluir la
documentacin completa de lo sucedido , la provisin de una explicacin al paciente y , si est
indicado por los acontecimientos , la investigacin detallada.
palabras clave
Las tcnicas anestsicas regionales
Las tcnicas de anestesia espinal ,
Complicaciones
Dos condiciones son , por lo tanto , absolutamente necesario para producir anestesia espinal :
puncin de la duramadre y la inyeccin subaracnoidea de un agente anestsico .
Gaston Labat , 1922
Espinal ( intratecal ) anestesia es generalmente considerado como uno de los ms fiables de
los mtodos de bloques regionales : la tcnica de insercin de la aguja es relativamente
sencillo, con el lquido cefalorraqudeo (LCR ) proporciona tanto una clara indicacin de
colocacin de la aguja con xito y un medio a travs del cual la solucin anestsica local por
lo general se propaga rpidamente . Sin embargo , la posibilidad de fracaso ha sido
reconocida , la cita anterior est tomada de la obra de Gaston Labat , 24 el "padre" de la
moderna anestesia regional. Sus dos condiciones para el xito , aunque quizs un poco
simplista cuando se relaciona con los conocimientos actuales, an indican la esencia del
mtodo y proporcionar un punto de partida para la consideracin de la falta, aunque puede ser
til para definir exactamente lo que esto significa en primer lugar . Literalmente, la palabra
fracaso implica que un anestsico espinal se intent , pero que no result bloque , lo que
sucede, pero tal vez un resultado ms comn es que los resultados de un bloque, pero no es
adecuada para la operacin propuesta . Esta insuficiencia puede relacionarse con tres
componentes del bloque : el tamao, la calidad , o la duracin de la accin del anestsico local
, a menudo con ms de uno de estos siendo inadecuada . Esta opinin ha considerado las tres
eventualidades en la definicin de "fracaso" .
Los profesionales con ms experiencia se consideran la incidencia de fracaso con anestesia
espinal a ser muy baja, quizs menos de un 1% . Sin embargo , una cifra tan alta como 17 % se
ha citado de un hospital universitario estadounidense, pero la mayora de los fracasos se
consideraron ' evitables ' .28 Una encuesta en otra institucin considera que esta elevada tasa
era "inaceptable" , y grabado el mucho ms bajo, pero an significativa , la figura de un 4% ,
con los " errores de juicio " como factor.32The importante implicacin clara es que la atencin
a los detalles es vital, y se ha demostrado que la tasa de fracaso de < 1 % es alcanzable en la
vida cotidiana practice.17Minimizing la incidencia de fracaso es , obviamente, un requisito
previo para la obtencin de los beneficios de la anestesia espinal , y la prevencin debe
comenzar con el reconocimiento pleno de los peligros potenciales de modo que la prctica
clnica se puede adaptar a evitarlas .
En trminos generales , la insuficiencia bloque normalmente se atribuye a uno de los tres
aspectos : tcnica clnica , la inexperiencia ( del aprendiz sin supervisin en especial ) , y el
fracaso para apreciar la necesidad de una meticulosa approach.10 Sin embargo , tales
categoras amplias revelan poco acerca de los muchos detallada formas en las que una
inyeccin intratecal puede ir por mal camino en cada una de las cinco fases de la anestesia
espinal individual, siendo estos , en secuencia , la puncin lumbar , la inyeccin de solucin ,
la difusin del frmaco a travs CSF, la accin del frmaco sobre las races de los nervios
espinales y la mdula , y manejo del paciente posterior . Todos los problemas que estn bien
descritas en la literatura, pero por lo general hace mucho tiempo, y muchos profesionales
parecen no darse cuenta de los problemas planteados. Por ejemplo , la divisin de
neurociencia de AstraZeneca recibi informes 562 ' del producto de defectos de notificacin
"en el ao 6 y el 31 de diciembre de 2007, toda atribucin fallida anestesia espinal a la solucin
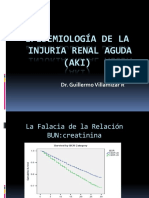
de bupivacana ineficaces (Fig. 1 ) . Casi un tercio de los informes ( 179 ) eran del Reino Unido,
pero prcticamente todos los pases donde se comercializa la droga estaba representado . Sin
embargo , el anlisis mostr que el material devuelto fue dentro de las especificaciones del
producto en cada caso para una revisin formal, basado en una bsqueda en la literatura , se
pensaba que era la pena.
Ver una versin ms grande :
En esta pgina
En una nueva ventana
Descargar como diapositivas de PowerPoint
Fig. 1
Nmero anual de informes sobre fallaron la anestesia espinal con bupivacana recibido por
AstraZeneca entre el 1 de enero de 1993 y 31 de diciembre 2008 trazadas segn las regiones
del mundo.
Los anuncios no de este sitio
Seccin Seccin anterior
estrategia de bsqueda
Para esta revisin " PubMed " bases de datos "Google" se realizaron bsquedas utilizando los
trminos "fall la anestesia regional ',' Error anestesia regional ' , ' Error anestesia espinal ' y '
error anestesia espinal . Artculos relevantes fueron recuperados al igual que todos los
papeles posiblemente pertinentes en sus listas de referencias . Bsquedas de apoyo se
realizaron en sujetos que no han sido identificadas de otro modo , los ejemplos concretos son
el volumen de LCR , ectasia dural y la compatibilidad qumica de los anestsicos locales con
adjuntos .
Adems , las bsquedas se realizan con 'Planet ' ( una base de datos interna de AstraZeneca) ,
' Biosis ' , ' Current Contents ', ' Embase ', ' PsycINFO "," Medline ", y" Medline Daily update ' ,
con los trminos " Error anestesia espinal "y" Error anestesia espinal ' como nicos trminos
de bsqueda y " anestesia raqudea " o " anestesia raqudea " o " anestesia raqudea " o "
anestesia mdula espinal " o " cable de la anestesia espinal " o " anestesia raqudea " o "
anestesia , mdula "y" fracaso del tratamiento "o" fracaso del tratamiento "y" intratecal .
Todos los documentos identificados como relevantes se incluyeron en esta revisin .
Seccin Seccin anterior
Mecanismos y su prevencin
Puncin lumbar Error
Incapacidad para obtener LCR , a veces referido como un " grifo seco ' , es la nica causa de la
falla , que es inmediatamente obvia . Una aguja con una luz bloqueada desde el principio es
una posibilidad terica , pero es muy poco probable con un equipamiento moderno . Sin
embargo, tanto la aguja y el estilete debe comprobar la exactitud de ajuste antes de su uso , y
la aguja no se debe avanzar sin el estilete en su lugar ya que el tejido o cogulo de sangre
puede obstruir fcilmente las bellas agujas calibre utilizadas ahora . De lo contrario , una
puncin lumbar fallida es casi siempre debido a ya sea un mal posicionamiento de la insercin
de la aguja del paciente o incorrecta , ambos factores estn dentro del control del anestesista .
Anomalas de la columna vertebral ( cifosis , escoliosis , la calcificacin de los ligamentos ,
consecuencias de la osteoporosis ) , la obesidad, y la ansiedad del paciente hacen que tanto el
posicionamiento de la paciente y la insercin ms difcil , especialmente en los ancianos aguja
. Textos de la anestesia regional dan amplia instruccin ms que puede ser proporcionado
aqu, y buena formacin clnica es la clave del xito , pero la mayora de dificultades se deben
a la falta de cumplimiento de las normas bsicas.
Posicionamiento
El paciente se coloca sobre una superficie firme ; las lminas y las espinas dorsales lumbares
estn ' separados ' mximamente mediante la flexin de toda la columna vertebral ( incluyendo
el cuello ) , las caderas , las rodillas y ; rotacin y la curvatura lateral de la columna vertebral
se evitan ; estos puntos se aplican a los puncin lumbar , tanto en audiencia pblica y las
posiciones horizontales laterales , el primero suele ser una opcin ms fcil en los pacientes
"difciles" , pero a veces ocurre lo contrario . El papel de la asistente en lograr y mantener al
paciente en la posicin correcta no puede ser underestimated.35
insercin de la aguja
A pesar de su identificacin precisa puede ser difcil con la tierra - marcas clnicos , lo que se
considera que es el tercer espacio intermedio lumbar se suele utilizar , pero el examen puede
indicar que otra es preferible. Sin embargo , se debe tener cuidado de no aventurarse
demasiado dao craneal y el riesgo a la mdula cord.33 Con el enfoque de la lnea media , la
insercin debe comenzar precisamente en el , a mitad de camino en la lnea media entre las
espinas posteriores , con el eje de la aguja en ngulo recto a la parte posterior en ambos
planos . Pequeos , cambios incrementales en el ngulo de la aguja se deben hacer slo si hay
resistencia al avance , y si se encuentra resistencia , angulacin ceflica debe probarse
primero , y tal angulacin puede ser apropiado desde el principio si el paciente no es capaz de
flexionar completamente ( por ejemplo, la paciente obsttrica a trmino ) . A veces se necesita
un grado de angulacin caudal , con una ligera direccin lateral que se requiera muy rara vez .
Todas las autoridades recomiendan que el anestesista debe tener un buen conocimiento de la
anatoma de la columna vertebral y relacionarlos con los cambios en la resistencia de los
tejidos a medida que se avanza la aguja de modo que una "imagen" mental de dnde est la
punta de la aguja se agradece.
Los puntos anteriores se aplican especficamente para el enfoque de la lnea media ; enfoques
laterales o paramediana son los preferidos por algunos, 27 especialmente si los ligamentos de
la lnea media estn muy calcificadas , pero son inherentemente tcnicas ms complejas . Sin
embargo, ante las dificultades , se aplican las mismas reglas bsicas : asegurarse de que el
paciente est en la posicin correcta y que se utilizan los ngulos correctos y la tcnica de
insercin.
adjuntos
Es ms probable que asumir y mantener la posicin correcta Una calma , paciente relajado ,
por lo que la explicacin (antes y durante el procedimiento) y apacible , sin prisas manejo de
pacientes son vitales ; premedicacin ansioltica luz contribuye mucho a la relajacin del
paciente, la infiltracin local de anestsico en la puncin el sitio debe ser eficaz sin ocultar las
seales, sino que debe incluir tanto intradrmica y sc inyeccin . El logro de la posicin
correcta es un reto especial en el paciente con dolor ( por ejemplo, de una fractura de cadera )
y la analgesia sistmica ( intravenosa o por inhalacin ) ayuda considerablemente. El objetivo
de tales adyuvantes es el de optimizar la posicin del paciente y para evitar cualquier
movimiento . Como se discutir ms adelante , slo se necesita un ligero movimiento para
desplazar la aguja de su objetivo .
Los avances en la tecnologa de ultrasonido estn llegando a la etapa en que se puede utilizar
para superar las dificultades con la puncin lumbar , pero los mdicos se siguen deben ser
conscientes de los problemas y la forma en que deben ser superados.
Puncin lumbar Pseudo - xito
La aparicin de un lquido claro en el cubo de la aguja suele ser la confirmacin definitiva de
que se ha entrado en el espacio subaracnoideo. Rara vez , sin embargo , el lquido
transparente no es CSF , pero anestsico local inyectado como un " top-up " para la anestesia
epidural que luego result insuficiente para una cesrea, o incluso difundir all desde el lumbar
plexus.26 Desafortunadamente , una prueba positiva para glucosa en el fluido no confirma que
este fluido es, sin duda porque CSF constituyentes fluidos extracelulares difunden
rpidamente en los fluidos inyectados en el espacio epidural . Otra , an ms raro , sugiri
causa de un lquido claro que aparece en la base de la aguja , pero no confirma la puncin
lumbar con xito, es un arcnido congnita cyst.39
Errores de inyeccin de solucin
La aparicin de la PPC en el cubo de la aguja es un requisito previo esencial para la anestesia
espinal , pero no garantiza el xito , que tambin requiere que una dosis plenamente eficaces
es a la vez elegido y realmente depositado en el LCR .
seleccin de dosis
Estudios de muchos factores que influyen en la propagacin de drogas intratecal han
demostrado que la dosis inyectada , dentro de la gama normalmente utilizado , tiene slo un
pequeo efecto en la medida de un anestsico espinal , pero es mucho ms importante en la
determinacin de la calidad y la duracin de block.20 general , la dosis real elegido depender
de la especfica de anestsico local utilizado , la baricidad de esa solucin , con posterioridad
la postura del paciente , el tipo de bloque destinado , y la duracin prevista de la ciruga . Por
lo tanto , el conocimiento de los factores que influyen en la propagacin de drogas por va
intratecal y la experiencia clnica con cualquier preparacin anestsica local en particular son
guas importantes para la eleccin de una dosis eficaz .
Sin embargo , la necesidad de garantizar un efecto adecuado significa que las dosis de
frmacos inyectados en tcnicas estndar de " disparo nico ' son ms grandes de lo que es
estrictamente necesario , la experiencia con el ajuste de la dosis durante la anestesia espinal
continua mostrando claramente que las dosis ms bajas son a menudo effective.21 En
intentos ya sea a minimizar la hipotensin , por ejemplo, mediante el intento de producir un
bloqueo unilateral , o la movilizacin postoperatoria velocidad , por la disminucin de la
duracin , algunos mdicos utilizan dosis ms bajas que se traditional3 ( por ejemplo, 5-10 en
lugar de 15 mg de bupivacana hiperbrica ) . Utilizado correctamente , y cuando fuera
apropiado, estas dosis pueden ser confiables , pero no significa que el margen de error se
reduce y que las consecuencias de otros problemas ( por ejemplo, prdida de la sustancia
inyectada , vea ms adelante ) sern exageradas y as correr el riesgo de un bloqueo
insuficiente . Se vuelve an ms importante asegurarse de que la totalidad de la dosis ms
baja que alcanza el lquido cefalorraqudeo y luego se extiende correctamente, recordando que
el "espacio muerto" de la aguja contendr una parte importante de lo que es un volumen
pequeo para empezar.
La prdida de la sustancia inyectada
La conexin Luer entre la jeringa y la aguja proporciona una oportunidad listo para la salida de
la solucin . Una variante particular de este problema es una fuga a travs de un defecto en la
unin del cubo de la aguja y shaft.6Given los pequeos volmenes implicados , la prdida de
incluso unas pocas gotas puede causar una disminucin significativa en la masa de alcanzar
el LCR de drogas , y por lo tanto en su eficacia . Para evitar esto, ha sido durante mucho
tiempo la enseanza convencional de que la jeringa que contiene el inyectado se debe insertar
muy firmemente en el cubo de la aguja , y que la posterior verificacin, se hace que se
produzca ninguna fuga .
inyeccin fuera de lugar
Aguja y la jeringa debe estar conectado con firmeza, pero el gran cuidado se debe tomar para
evitar cualquier desplazamiento anterior o posterior de la punta de la aguja en el espacio
epidural, subaracnoidea , donde la deposicin de una dosis de anestsico local espinal tendr
poco o ningn efecto. Aspiracin de lquido , despus de la fijacin de la jeringa, debe
confirmar el flujo libre de peste porcina clsica y , por lo tanto , que la punta de la aguja se
encuentra todava en el espacio correcto , pero tal aspiracin puede desplazar la punta menos
que se realice con cuidado, ya que la fuerza de la inyeccin de la contenido de la jeringa . Para
prevenir el desplazamiento en cualquier etapa , se ha defendido que el dorso de una mano
debe ser anclado firmemente contra la espalda del paciente y los dedos utilizados para
inmovilizar la aguja , mientras que la otra mano se utiliza para manipular las syringe.40
mayora de los practicantes recomendaran aspiracin de LCR despus de que se mantiene la
inyeccin para confirmar que la colocacin correcta , y algunos abogan por que esto se hace a
mitad de camino a travs, as aunque ninguna de estas prcticas se ha demostrado que
influyen en el resultado de la block.3240
Desplazamiento Consejo debe tener vigilancia en contra de cualquier tipo de aguja espinal ,
pero es un tema en particular con las agujas de la " punta de lpiz " ahora se utiliza
ampliamente para reducir al mnimo la incidencia de cefalea ps- puncin. La abertura en el
extremo de estas agujas es proximal a la punta , por lo que slo un menor grado de
movimiento ' hacia atrs ' durante la unin jeringa puede resultar en inyeccin epidural como
se reconoci en una etapa temprana en el uso generalizado de tales needles.12 Las distancias
involucrados son del orden de un milmetro o dos , pero ( como con fugas ) mala colocacin
de slo una pequea cantidad de solucin puede tener efectos significativos . Una cuestin
adicional con agujas de punta de lpiz es que la abertura , al ser mucho ms largo que el bisel
de una aguja de Quincke , puede " a horcajadas " de la duramadre de manera que un poco de
solucin alcanza el LCR , y algunos el espacio epidural ( fig. 2 ) .41 esto puede ser exagerada
por la duramadre que acta como una vlvula de ' colgajo ' a travs de la abertura de la aguja .
Inicialmente , la presin del LCR empuja hacia el exterior dura por lo que la aspiracin se
realiza correctamente ( fig. 3A ) , pero empuja la posterior inyeccin de la duramadre hacia
adelante y la solucin est fuera de lugar (Fig. 3B ) .
Ver una versin ms grande :
En esta pgina
En una nueva ventana
Descargar como diapositivas de PowerPoint
la figura 2
Las posibles posiciones de la punta de una aguja de punta de lpiz . Si se coloca
correctamente ( imagen superior) que toda la solucin anestsica local alcanzar el espacio
subaracnoideo , pero si ' caballo ' la apertura de la duramadre (foto inferior) alguna solucin
ser depositado en el espacio epidural.
Ver una versin ms grande :
En esta pgina
En una nueva ventana
Descargar como diapositivas de PowerPoint
Fig. 3
Para mostrar cmo la duramadre o aracnoides mater puede actuar como una vlvula de '
colgajo ' a travs de la apertura de una aguja de punta de lpiz . Durante la aspiracin ( A) de la
duramadre / aracnoides se retiraron permitiendo CSF para entrar en la aguja. Durante la
inyeccin de la duramadre ( B) o aracnoides ( C ) es empujado hacia adelante y el anestsico
local entra en el espacio epidural o subdural .
Una variante es que la punta de la aguja penetre en la duramadre , pero es la aracnoides que
acta como la vlvula de aleta de manera que los resultados de una inyeccin subdurales ( fig.
3C ) . Esta mala ubicacin, se lo suele considerar como que conduce a la propagacin
excesiva durante el bloqueo epidural , pero el fenmeno equivalente se ha descrito despus de
la inyeccin subaracnoidea previsto , 37 y es una complicacin reconocida de myelography.22
inyeccin subdural tambin ha sido identificado como la causa de un bloque fallado cuando se
destinen a epidural11 o subarachnoid15 inyeccin .
Estas eventualidades , siendo alteraciones sutiles de la colocacin, son imposibles de
identificar en el momento actual, pero la rotacin de la aguja a travs de 360 despus de la
aparicin inicial de la CSF, y antes de la llegada de aspiracin , se ha defendido como una
manera de reducir al mnimo la posibilidad de que ocurra , la teora de que la rotacin se
reduce el riesgo de los bordes de la membrana de captura en la abertura .
Diseminacin intratecal inadecuada
La difusin intratecal de un anestsico local , incluso cuando se coloca correctamente ,
realmente ha sido descrito como capricious.7 Los factores que lo afectan, son muchos, pero el
foco aqu ser en las que puede dar lugar a la propagacin inadecuada.
anormalidad anatmica
Intratecal propagacin se rige por la interaccin entre las caractersticas fsicas de soluciones
, la gravedad, y la configuracin del canal vertebral . Anormalidades anatmicas que conducen
a problemas de propagacin pueden ser a la vez abierta y encubierta . Las curvas de la
columna vertebral son parte integral de propagacin solucin y cualquier anormalidad obvia ,
la cifosis o escoliosis, pueden interferir con el proceso. El examen de la paciente debe revelar
si esto puede ocurrir , pero no es posible predecir si el efecto ser propagacin excesiva o el
fracaso .
Una posibilidad muy raro , que no es evidente en el examen , es que los ligamentos que
sostienen la mdula espinal dentro de la teca forma completa septos y actan como barreras
longitudinales o transversales a la propagacin del anestsico local . Esto puede resultar en
un bloque que es totalmente unilateral2 o de la insuficiencia de extensin ceflica . La
estenosis espinal u otras lesiones patolgicas tambin pueden limitar la propagacin , la
eficacia , o ambos , uno de estos casos se atribuye a las consecuencias de la anterior
intratecal chemotherapy.142Similarly , ciruga previa dentro del canal vertebral puede dar lugar
a adherencias que interfieren con la extensin .
Un interesante ' anormalidad ' considera que han causado propagacin restringido en un solo
paciente era un volumen ms grande de lo normal de CSF en la zona lumbar theca.18 estudio
sistemtico posterior ha demostrado que el volumen de LCR lumbar es el factor ms
importante que influye en la variabilidad observada entre los individuos en se encontr que la
propagacin de una intratecal injection.9 una correlacin negativa entre el volumen de LCR
lumbar y el nivel sensorial pico alcanzado con bupivacana hiperbrica cuando la inyeccin se
realiz tanto en posicin supina y posiciones sentadas . Una variacin de este factor es
ectasia dural , que es un aumento de volumen patolgico de la duramadre visto en la mayora
de los pacientes con sndrome de Marfan y en algn otro tejido conectivo disorders.25
densidad de la solucin
Consistentemente eficaz de la anestesia espinal requiere que el practicante tiene una buena
comprensin de los factores que intervienen en la transmisin intratecal , en particular , pero
no slo , densidad de la solucin . Una solucin con una densidad en el rango normal de la del
CSF ( ' isobrica ' ) prcticamente garantizar bloque de los miembros inferiores , con poco
riesgo de bloqueo del nervio dorsal y as hypotension.43 Sin embargo , las soluciones simples
de bupivacana , aunque a menudo referido como isobrica , en realidad son de densidad
suficientemente baja para ser hipobrica , especialmente a la temperatura corporal . Como
resultado, su gama de propagacin es mucho menos predecible que el de una preparacin
verdaderamente isobrica , y de vez en cuando el bloque puede ser no mayor que la primera ,
o incluso segundos , dermatoma lumbar cuando se administra a la posicin supina no
embarazadas patient.29 Aunque el impacto de las variaciones en el volumen de LCR an no se
ha estudiado con estas soluciones , parece probable que este factor puede muy bien ser un
factor en su variabilidad .
Las soluciones con una densidad mayor que la de CSF ( hiperbrico ) se mueven muy
definitivamente bajo la influencia combinada de la gravedad y las curvas del canal vertebral .
Hace ms de cien aos, Barker, uno de los pioneros de la anestesia espinal en el Reino Unido ,
observ que la adicin de glucosa a la solucin preparada para una ms confiable effect.4 En
el escenario estndar , el de un paciente en posicin supina despus de la inyeccin de una
preparacin hiperbrica en el nivel medio -lumbar , la solucin se extienda "abajo" la
pendiente bajo el efecto de la gravedad a la piscina en el punto ' ms bajo ' de la curva torcica
, por lo que la exposicin de todas las races de los nervios hasta ese nivel a un concentracin
eficaz de anestsico local. Sin embargo , si la puncin lumbar se realiza en el cuarto lumbar o
el espacio intermedio lumbo - sacra el anestsico local puede ser ' atrapado ' por debajo de la
curva lumbar , especialmente si el paciente est en la posicin de sentado durante la inyeccin
y se mantiene en esa posicin durante un perodo a partir de entonces .
Esto se traduce en un bloque que se limita a los segmentos sacros, como se ha descrito con
un catter espinal que pasa caudally.31 prevencin se basa en evitar demasiado bajo un nivel
de inyeccin a menos que, por supuesto , tiene la intencin deliberada de un bloque ' silla ' .
Accin del frmaco ineficaz
La ltima explicacin posible para una columna vertebral no es realmente que la solucin
inyectada llega a los nervios diana , pero es inactivo o ineficaz , con una variedad de
explicaciones siendo posible .
errores de identificacin
Anestsicos espinales se suministran en solucin acuosa lista para la inyeccin y no hay
oportunidad para la confusin en la preparacin de la solucin en s misma . Sin embargo ,
otras soluciones pticamente claras , tales como un anestsico local separado para
infiltracin de la piel o adyuvantes analgsicos , se utilizan a menudo de la misma rea de
preparacin estril y la posibilidad de que confundirlos puede conducir a un bloque ineficaz
deben ser considerados . El reconocimiento de la posibilidad de tales errores de inyeccin ha
llevado al uso generalizado de etiquetado jeringa en la anestesia , pero esto no es tan fcil
dentro de un campo estril , ya que es en una estacin de trabajo de anestesia . La atencin al
detalle es esencial , pero minimizando el nmero de ampollas en la bandeja de bloque ( tales
como el uso de la misma anestsico local para ambos infiltracin de la piel y la mdula ) y
consistente uso de diferentes tamaos de jeringa para cada componente del procedimiento de
ayudar considerablemente .
incompatibilidad qumica
La mezcla de dos diferentes preparaciones farmacuticas tambin plantea la posibilidad de
ineficacia como resultado de la interaccin entre el anestsico local y el adyuvante . Los
anestsicos locales parece ser compatible con la mayora de los opioides comunes , pero ha
habido poco estudio formal de los efectos de la mezcla , y la situacin es an menos definitivo
con otros adyuvantes como la clonidina , midazolam y otras sustancias ms extremas.
Ciertamente , no hay estudios sobre la estabilidad de tres o ms de las sustancias cuando se
mezclan para uso intratecal , una prctica no desconocida en la actualidad. La reaccin
qumica puede generar un precipitado obvio , pero otra posibilidad es que el pH de la solucin
de anestsico local se vuelve an ms baja de lo que era para empezar. Esto puede reducir la
concentracin de la fraccin no ionizada que es lo que se difunde en el tejido nervioso y , a
menos que la solucin se mezcla bien con CSF , un efecto de disminucin podra resultar . Hay
al menos un informe que indica que la incidencia de fracaso es mayor despus de la adicin
de una solucin vasoconstrictora y esto podra representar un ejemplo de este effect.30
Solucin de anestsico local Inactivo
Los mayores , los anestsicos locales de tipo ster son qumicamente lbiles de modo que la
esterilizacin por calor y el almacenamiento prolongado , especialmente en solucin acuosa ,
pueden hacerlos ineficaces debido a la hidrlisis y por lo tanto necesitan un manejo muy
cuidadoso . Aunque los frmacos unida a amida ms modernas (por ejemplo, lidocana ,
bupivacana , etc ) son mucho ms estables y pueden ser esterilizado por calor en solucin y
luego almacenar durante varios aos sin prdida de potencia , ha habido una serie de informes
que atribuyen el fracaso de mdula anestsicos a drug.8163844 inactiva
Resistencia anestsico local
Muy rara vez un anestsico espinal no se ha atribuido a la "resistencia" fisiolgica a las
acciones de los frmacos anestsicos locales , aunque los informes tienden a la
anecdotal.5233645 Una historia de fallo repetido de las tcnicas anestsicas locales dentales o
de otro tipo se acompaa por la especulacin de que el problema se debe a una mutacin del
canal de sodio que hace que los medicamentos ineficaces . Sin embargo , no hay tal mutacin
se ha descrito nunca, y los informes clnicos estn incompletos , no especficamente para
tener en cuenta no slo las causas reconocidas de fracaso, sino tambin el comportamiento
de un paciente ansioso que prefieren la anestesia general como una explicacin de la
"resistencia" . Se requiere una investigacin muy detallada para la "resistencia" para ser
aceptado como una explicacin. Como acotacin al margen , cualquier paciente que da una
historia de repetidos fracasos con anestesia local debe ser administrado por un mdico con
experiencia .
La falta de gestin posterior
No todas las reclamaciones de un paciente de incomodidad o incluso dolor , durante la
anestesia espinal son el resultado de una inyeccin inadecuada. Un anestsico espinal se
realiza correctamente producir completa somtica , y un importante grado de bloqueo
autonmico , nervio en la mitad inferior del cuerpo a menos que se utilice un mtodo
especficamente restringido . Sin embargo , asegurar que se produce este bloque es slo una
parte del proceso debido a que los componentes no afectados del sistema nervioso requieren
una consideracin y gestin . En concreto , esto se relaciona con la conciencia de la relacin
clnica y de sensaciones transmitidas a travs de los nervios bloqueados , con los dos
factores posiblemente haciendo la reclamacin del paciente que el bloque ha fallado. Esta
realidad no puede ser el caso , pero el manejo del paciente ciertamente ha fallado si tal
afirmacin se hace cuando el bloque es realmente tan bueno como podra ser.
En decbito supino y despierto durante una ciruga no es una experiencia agradable, incluso
para el ms optimista de los individuos, y la ansiedad por s solo puede causar mucha
dificultad. Adems, las mesas de operaciones estn diseados para el acceso quirrgico , no
la comodidad del paciente , y estmulos intra - abdominales pueden dar lugar a impulsos
aferentes en las fibras nerviosas parasimpticas y frnico no bloqueados . El ms ansioso que
el paciente , mayor ser el impacto de estos factores y ms probable ser que el paciente no
podr hacer frente a la situacin y afirman que la anestesia no ha funcionado correctamente.
Expectativa juega un papel , y la buena orientacin de los pacientes preoperatoria seguida de
un enfoque de apoyo del anestesista durante la operacin es importante para evitar este tipo
de problemas , pero tambin lo es el uso prudente y proactiva de los medicamentos sedantes
y analgsicos sistmicos. Sedacin suficiente para producir somnolencia o incluso dormir (
con un seguimiento adecuado ) , rara vez es contraindicada , salvo en la situacin obsttrica ,
e incluso hay pequeas dosis en ocasiones pueden ser tiles .
Prueba del bloque
En los ltimos aos , se ha convertido en casi obligatorio , sin duda en el contexto obsttrico ,
para poner a prueba el nivel de bloque formalmente comienza antes de la ciruga . Esta
precaucin aparentemente sensata puede ser difcil o imposible llevar a cabo en algunos
pacientes ( por ejemplo, el paciente demente con una fractura del cuello del fmur ) . Enfoque
excesivo en la prueba tambin puede tener un impacto negativo. La mayora de los pacientes
tendrn cierta ansiedad acerca de la efectividad de la inyeccin, y esto se incrementar si la
prueba se inicia demasiado pronto. La prctica convencional es comprobar bloque motor
mediante pruebas de la capacidad de levantar las piernas , seguida por la prueba del bloqueo
sensorial a estmulos como el tacto suave , fro, o pinchazo , todos los cuales tienen sus
defensores . Es recomendable comenzar las pruebas en los segmentos ms bajos , en los que
el inicio ser ms rpido , y seguir hacia arriba . Demostrando desde el principio que hay algn
efecto fomenta la confianza del paciente ; pruebas demasiado pronto hace lo contrario .
Aunque no existe una evaluacin formal del nivel de bloque, el mdico debe estar seguro de
que un bloque adecuada se ha producido . Establecer que el nivel de bloque es apropiado para
la ciruga proyectada se toma a menudo para demostrar que la calidad de bloque es adecuada
tambin , pero esto no es siempre el caso si se utilizan fras o pinchazo estmulos . La
observacin de que el nivel de bloque superior se encuentra a pocos dermatomas anterior que
inervan el campo quirrgico (sin olvidar las estructuras ms profundas ) es un buen comienzo,
pero no garantiza que la calidad de los bloques es suficiente. Una pizca encubierta del sitio de
la incisin quirrgica propuesta puede ser un mejor indicador de la analgesia piel, y puede ser
tranquilizador si el bloque ha sido lento en el inicio . De hecho , hay mucho que decir , sobre
todo cuando el paciente est consciente, por preguntar al cirujano a hacer lo mismo con
dientes pinzas quirrgicas antes de la incisin de la piel, 10 pero subrepticiamente andwithout
hacer una pregunta capciosa , como " Esto duele? " ! El paciente est distrado por la
conversacin y el intercambio de miradas entre el cirujano y el anestesista es todo lo que se
necesita para la ciruga de comenzar.
Catter y tcnicas combinadas
La gran mayora de la anestesia espinal implica una sola , a travs de inyeccin de la aguja y ,
como se ha sealado , esto requiere cierto grado de certeza acerca de su eficacia para la
ciruga . Para aprovechar el inicio rpido y profundo bloque de la anestesia espinal , continua y
tcnicas espinal y epidural combinadas se han introducido para aumentar la flexibilidad . Si
los catteres se colocan correctamente , problemas de propagacin inadecuada , la calidad y
la duracin del efecto se pueden tratar con aunque muchos de los potenciales problemas
tcnicos descritos anteriormente todava se puede aplicar . Sin embargo , ambos mtodos
requieren un mayor nivel de habilidad y experiencia para utilizar , la insercin de un catter
intratecal puede ser sorprendentemente difcil de lograr en algunos pacientes y , como se ha
mencionado ya , pueden resultar en la mala direccin de la solucin de anestsico local , con
el riesgo de neurotoxicity.34 es vital dejar no ms de 2-3 cm de catter dentro de la duramadre
para evitar esto. En la tcnica combinada , es comn para inyectar un volumen relativamente
pequeo para el componente de la columna vertebral , por lo que los problemas que pueden
resultar en una proporcin no alcanzar el espacio subaracnoideo son muy relevantes , pero al
menos el catter epidural se puede utilizar en los intentos para rescatar la situacin .
Seccin Seccin anterior
Manejo de la insuficiencia
Fracaso de la anestesia espinal es un evento de gran preocupacin para el paciente y el
anestesilogo , incluso cuando es evidente de inmediato , pero puede tener consecuencias
graves ( clnica y mdico- legal) si el problema slo se hace evidente una vez la ciruga ha
comenzado. Si hay alguna duda acerca de la naturaleza o la duracin de la ciruga propuesta ,
un mtodo que no sea un anestsico espinal estndar debe ser utilizado. El anestesista
residente debe evitar el exceso de venta de la tcnica , especialmente en los primeros das de
prctica supervisada. Prometiendo que todo se puede lograr mediante una inyeccin no deja
margen de maniobra, pero que ofrece una inyeccin para reducir el dolor y una segunda para
garantizar la inconsciencia hace. Si un anestsico espinal hace fracasar de alguna manera, las
opciones de gestin son limitados , as que, la primera regla es que gastar todos los esfuerzos
en la prevencin.
Es mejor prevenir que curar
Despus de haber tomado la decisin de utilizar una anestesia espinal, el bloque se debe
realizar con una atencin meticulosa a los detalles , como se ha indicado anteriormente. Es
imposible exagerar la importancia de este punto.
El bloque fallado
La gestin precisa del bloque no depender de la naturaleza de la insuficiencia y la hora a la
que se hace evidente . Por lo tanto , algunos de vigilancia de la aparicin del bloque y la
interpretacin correcta de las observaciones son vitales . Cuanto menor sea la aparicin de
cualquier motor o bloqueo sensorial , ms probable es que el bloque es insuficiente , por lo
que cuanto ms detallada esta evaluacin debe ser. Mientras que el inicio de la anestesia
espinal es rpida en la mayora de los pacientes , puede ser lento en algunos , de modo que , '
tintura de tiempo ' debe ser siempre allowed.10 Sin embargo , si la mayor parte del bloque de
espera no ha desarrollado dentro de 15 min , alguna maniobra adicional es casi seguro que va
a ser necesario . Las posibilidades , sus explicaciones, y sugiri respuestas inmediatas son
las siguientes :
1 . No bloquear : la solucin equivocada se ha inyectado , se ha depositado en el lugar
equivocado , o es ineficaz . Repetir el procedimiento o la conversin a la anestesia general son
la nica opcin. Si , despus de la operacin , el paciente tiene prurito significativo , es
probable que slo se inyect un opioide .
2 . Bueno bloque de inadecuada extensin ceflica : el nivel de inyeccin fue muy bajo,
anormalidad anatmica ha restringido extendi , o alguna sustancia inyectada se ha
extraviado. Si se utiliz una solucin hiperbrica , flexionar las caderas y las rodillas del
paciente y la inclinacin de la cabeza de la tabla hacia abajo. Esto se endereza la curva lumbar
, pero mantiene ' pendiente ' a ceflica y permite que cualquier solucin ' atrapado ' en el sacro
para difundir an ms . Una variante con el mismo objetivo , pero tal vez ms adecuado a la
situacin obsttrica , es convertir al paciente en la posicin de lateral llenos con una
inclinacin de la cabeza hacia abajo , invirtiendo el lado despus de 2-3 min . Si se ha utilizado
una solucin simple ( y por lo general ligeramente hipobrica ) , que puede ayudar a sentar al
paciente , pero ten cuidado con acumulacin de sangre perifrica .
Si un espinales resultados de la inyeccin de catter en extensin inadecuada , la respuesta
no debe ser para inyectar ms de la misma solucin , porque la dosis tiene un efecto mnimo
sobre intratecal spread.20 cualquier postura debe ser manipulado como anteriormente, o una
baricidad diferente de la solucin debe ser juzgado , o el catter debe ser retirado antes de la
inyeccin es repeated.31
3 . Bueno , pero unilateral bloque : esto es ms probable debido a la posicin , pero es posible
que los ligamentos longitudinales de apoyo el cable han bloqueado extendi . Si la operacin
es estar en el limbo anestesiado , el cirujano debe saber que la otra pierna tiene la sensacin,
y el paciente debe estar tranquilo y supervisar atentamente . De lo contrario , girando el
paciente sobre el lado no bloqueado si se ha utilizado una solucin hiperbrica ( o la inversa
de soluciones simples ) puede facilitar extendido .
4 . reas dispersadas de bloque ( Este trmino se utiliza para describir un bloque que aparece
en la medida adecuada , pero los efectos sensoriales y motores son incompletos . ) : Causas
de bloque inadecuada son numerosas e incluyen todos los descritos anteriormente , pero la
explicacin ms probable es que el locales anestsico fue al menos parcialmente fuera de
lugar , o que la dosis administrada era inadecuada . Si esto se hace evidente antes de que
empiece la ciruga , las opciones son para repetir la inyeccin espinal o de utilizar un mayor
grado de suplementacin sistmica de lo previsto , siendo esta ltima la nica opcin despus
de la incisin de la piel . Puede que no sea necesario recurrir a la anestesia general , sedacin
, o frmacos analgsicos son a menudo suficiente , especialmente cuando la ansiedad del
paciente es un factor importante . La infiltracin de la herida y otros tejidos con anestsico
local por el cirujano tambin puede ser til en tales situaciones .
5 . Duracin inadecuada: la explicacin ms probable es que para una de varias razones una
dosis inadecuada de anestesia local se entrega a la CSF . Alternativamente , lidocana (para
infiltracin de la piel ) se confundi de bupivacana o la operacin se ha llevado ms tiempo de
lo esperado. Suplementacin sistmica o la infiltracin de anestsico local pueden marea
asuntos ms , pero a menudo la nica opcin es convertir a la anestesia general.
Repitiendo el bloque
Donde ningn efecto en absoluto ha seguido la inyeccin parece razonable que repetir el
procedimiento , prestando especial atencin a evitar los peligros potenciales. En todas las
dems situaciones , adems de fracaso total, debe haber algn anestsico local en el LCR ya,
y la ansiedad relacionados con varias cuestiones que deben tenerse en cuenta :
1 . Un bloque puede ser restringida a causa de algn factor , probablemente anatmica , lo que
impide la propagacin fsica de la solucin , y puede tener exactamente el mismo impacto en
una segunda inyeccin , lo que resulta en una alta concentracin de anestsico local en o
cerca del sitio de la inyeccin . Cauda equina lesiones se describieron despus de la anestesia
espinal continua cuando se le solicite propagacin repetir las inyecciones muy restringido en
lugar de la manipulacin de otros factores , 34 y un problema similar se ha descrito despus
de aguja repetidos injection.1419
2 . Repetir la inyeccin , especialmente en respuesta a un bloque de mala calidad , puede
conducir a la propagacin excesiva , 13 por lo que puede decirse que una dosis ms baja se
debe utilizar para reducir el riesgo de esta posibilidad .
3 . Un bloque de buena calidad , pero unilateral , que podra conducir a un intento de colocar
una segunda inyeccin en el "otro" lado de la teca , pero el riesgo de colocar la segunda dosis
en el mismo lado debe ser significativa .
4 . Barreras a repartidas en el espacio subaracnoideo tambin pueden afectar propagacin
epidural ( y viceversa ) , por lo que un intento de bloqueo epidural no puede tener xito ya sea .
5 . Un bloque de extensin ceflica inadecuada podra superarse mediante la repeticin de la
inyeccin en un nivel superior , pero tal vez slo debe ser intentado cuando la indicacin de
una tcnica regional es considerable .
6 . La ltima preocupacin , particularmente aplicable a la mencionada en ltimo lugar , pero
relevante para casi todas las situaciones en las que podra ser considerado un bloque de
repeticin , es que el tejido nervioso adyacente ya se ve afectada por la accin anestsica
local de manera que el riesgo de trauma aguja directa se incrementa .
Slo algunos de estos problemas, de hecho se han descrito , la mayora est en la categora de
las posibilidades tericas , pero tales preocupaciones no reforzar la opinin de que debe
hacerse todo lo posible para garantizar que la primera inyeccin es plenamente eficaz.
El recurso a la anestesia general
Hay muchas maneras en las que un bloque inadecuada podra ser ' rescatado ' , pero hay un
lmite a la cantidad de malestar o la angustia de un paciente puede tolerar , por lo que la
anestesia general se deben considerar si una o dos medidas simples no han rectificado las
cosas. El sentido comn y la experiencia clnica general son los mejores indicadores de
exactamente cundo va a convertir a la anestesia general , por lo que el alumno no
supervisado puede estar en desventaja . Sin embargo , es mucho mejor que tomar la decisin
ms pronto que tarde y tener que lidiar con un paciente gravemente angustiada. Por supuesto
, explicando ms adelante por qu no se haba facilitado la tcnica anticipada puede ser difcil.
Es otra razn por la prevencin ( conseguir el bloque de la derecha para empezar) es el mejor
enfoque , pero tambin es una razn para no "sobre- vender" el enfoque regional antes de la
operacin .
Si la anestesia general se indujo para complementar una parte efectiva anestesia espinal ,
cualquier grado de bloqueo del nervio simptico har hipotensin ms probable.
Iniciativas de seguimiento hasta
El seguimiento clnico
Como con cualquier complicacin anestsica , los detalles deberan documentarse
completamente en la memoria , y el paciente present con una disculpa y una explicacin
completa despus de la operacin . Dar al paciente un resumen escrito de los eventos para la
presentacin de un futuro anestesista puede ser muy til , aunque se debe tener cuidado para
evitar el recurso mdico- legal. En raras ocasiones, difusin inadecuada ha sido la primera
indicacin de la patologa dentro del canal vertebral . Por lo tanto , puede ser apropiado para
buscar sntomas y signos de enfermedad neurolgica , e implicar un neurlogo si hay
cualquier sospecha de stos estar presente .
Es durante el seguimiento de un paciente en el que se obtuvo ningn bloque , la posibilidad de
anestsico local "resistencia" puede parecer una explicacin atractiva. Como ya se ha
sealado , se necesita mucho ms amplia consideracin de las posibilidades , con el apoyo de
investigacin muy detallada , que ha sido el caso en los informes anteriores .
Investigar la eficacia anestsica local
La anestesia espinal suele ser una tcnica sencilla y eficaz, pero el "fracaso" puede ocurrir en
cualquier momento y en las manos de cualquier mdico , sin importar la experiencia . Sin
embargo , si el procedimiento ha , aparentemente , habido preocupaciones de rutina y directo
pueden surgir que el suministro de corriente de anestsico local es defectuoso ,
especialmente si se producen dos o ms de tales fallos en el mismo hospital dentro de un
corto perodo de tiempo . Las preparaciones que se han visto ms implicados son los de
bupivacana hiperbrica (probablemente porque es el medicamento que se usa ms
comnmente en la actualidad ), con drogas de ambos proveedores principales , Abbott38 y
AstraZeneca, 81.644 estn involucrados .
De hecho , la estabilidad qumica de los medicamentos de amida y las normas modernas de
fabricacin farmacutica significa que la inactividad de drogas es una causa ms probable de
un anestsico espinal fallado , pero sigue siendo una posibilidad de que al menos tiene que
ser eliminado .
Como se ha sugerido , la realizacin de infiltracin de la piel con un poco de la solucin
destinada a la inyeccin espinal debe demostrar que es eficaz . Si el problema contina la sala
de operaciones , los registros del departamento de farmacia y anestesia deben ser cotejados
para ver si otros mdicos en el hospital han tenido ningn problema . Del mismo modo , los
distribuidores deben ser capaces de comprobar si otros hospitales que han sido
suministrados con el material del mismo lote han informado de dificultades . Si estas
investigaciones revelan que otros estn usando el mismo material con buenos resultados , el
mdico debe tener en cuenta la opinin de estos dos grandes autoridades , Lee y Atkinson,
sobre " La mdula que no tiene ' :
Todos los trabajadores experimentados han encontrado esta vez a pesar de procedimiento
aceptado aparentemente ha sido seguido . La reflexin , sin embargo , por lo general revela un
defecto en la tcnica . En 1907 Alfred E. Barker escribi que para el xito de la analgesia
espinal es necesario ' para entrar en el saco dural lumbar eficazmente con el punto de la aguja
, y para descargar a travs de esta , toda la dosis prevista de la droga , directa y libremente en
el cefalorraqudeo fluido , por debajo de la terminacin del cable ' ( Barker , 1907 ) . El
incumplimiento de los detalles de este consejo es la causa ms comn de un pobre result.27
Failed spinal anaesthesia: mechanisms, management, and
prevention
1. P. D. W. Fettes1,
*
,
2. J.-R. Jansson2 and
3. J. A. W. Wildsmith1
+Author Affiliations
1.
1
University Department of Anaesthesia, Ninewells Hospital & Medical School, Dundee DD1 9SY, UK
2.
2
AstraZeneca R&D SE-151 85, Sodertalje, Sweden
1.
*
Corresponding author. E-mail: paulfettes@nhs.net
Accepted April 2, 2009.
Next Section
Abstract
Although spinal (subarachnoid or intrathecal) anaesthesia is generally regarded as one of the most reliable types of
regional block methods, the possibility of failure has long been recognized. Dealing with a spinal anaesthetic which is
in some way inadequate can be very difficult; so, the technique must be performed in a way which minimizes the risk
of regional block. Thus, practitioners must be aware of all the possible mechanisms of failure so that, where possible,
these mechanisms can be avoided. This review has considered the mechanisms in a sequential way: problems with
lumbar puncture; errors in the preparation and injection of solutions; inadequate spreading of drugs through
cerebrospinal fluid; failure of drug action on nervous tissue; and difficulties more related to patient management than
the actual block. Techniques for minimizing the possibility of failure are discussed, all of them requiring, in essence,
close attention to detail. Options for managing an inadequate block include repeating the injection, manipulation of
the patients posture to encourage wider spread of the injected solution, supplementation with local anaesthetic
infiltration by the surgeon, use of systemic sedation or analgesic drugs, and recourse to general anaesthesia. Follow-up
procedures must include full documentation of what happened, the provision of an explanation to the patient and, if
indicated by events, detailed investigation.
Key words
anaesthetic techniques, regional
anaesthetic techniques, spinal
complications
Two conditions are, therefore, absolutely necessary to produce spinal anesthesia: puncture of the dura mater and
subarachnoid injection of an anesthetic agent.
Gaston Labat, 1922
Spinal (intrathecal) anaesthesia is generally regarded as one of the most reliable of regional block methods: the needle
insertion technique is relatively straightforward, with cerebrospinal fluid (CSF) providing both a clear indication of
successful needle placement and a medium through which local anaesthetic solution usually spreads readily. However,
the possibility of failure has long been recognized, the above quote being taken from the work of Gaston Labat,24 the
father of modern regional anaesthesia. His two conditions for success, although perhaps a little simplistic when
related to current knowledge, still indicate the essence of the method and provide a starting point for the consideration
of failure, although it may be helpful to define exactly what this means first. Literally, the word failure implies that a
spinal anaesthetic was attempted, but that no block resulted; this happens, but perhaps a commoner outcome is that a
block results, but is inadequate for the proposed surgery. Such inadequacy may relate to three components of the
block: the extent, quality, or duration of local anaesthetic action, often with more than one of these being inadequate.
This review has considered all three eventualities within the definition of failure.
Most experienced practitioners would consider the incidence of failure with spinal anaesthesia to be extremely low,
perhaps less than 1%. However, a figure as high as 17% has been quoted from an American teaching hospital, yet
most of the failures were judged to be avoidable.28 A survey at another such institution considered that this high rate
was unacceptable, and recorded the much lower, but still significant, figure of 4%, with errors of judgement as the
major factor.32The clear implication is that careful attention to detail is vital, and it has been shown that a failure rate
of <1% is attainable in everyday practice.17Minimizing the incidence of failure is obviously a pre-requisite for
gaining the benefits of spinal anaesthesia, and prevention must start with full recognition of the potential pitfalls so
that clinical practice can be tailored to their avoidance.
In general terms, block failure is usually ascribed to one of three aspects: clinical technique, inexperience (of the
unsupervised trainee especially), and failure to appreciate the need for a meticulous approach.10 However, such broad
categories reveal little about the many detailed ways in which an intrathecal injection can go astray within each of the
five phases of an individual spinal anaesthetic, these being, in sequence, lumbar puncture, solution injection,
spreading of drug through CSF, drug action on the spinal nerve roots and cord, and subsequent patient management.
All of the problems involved are well described in the literature, but usually long ago, and many practitioners seem
unaware of the issues involved. For instance, the neuroscience division of AstraZeneca received 562 Product Defect
Notification reports in the 6 yr to December 31, 2007, all ascribing failed spinal anaesthetics to ineffective
bupivacaine solution (Fig. 1). Nearly one-third of reports (179) were from the UK, but virtually every country where
the drug is marketed was represented. However, analysis showed that the returned material was within the products
specification in every case so a formal review, based on a literature search, was thought to be worthwhile.
View larger version:
In this page
In a new window
Download as PowerPoint Slide
Fig 1
Annual numbers of reports of failed spinal anaesthesia with bupivacaine received by AstraZeneca between January 1,
1993 and December 31, 2008 plotted according to region of the world.
Ads not by this site
Previous SectionNext Section
Search strategy
For this review PubMed and Google databases were searched using the terms failed regional anaesthesia, failed
regional anesthesia, failed spinal anaesthesia, and failed spinal anesthesia. Relevant articles were retrieved as were
any possibly relevant papers in their reference lists. Supporting searches were performed on subjects that may not
have been otherwise identified, specific examples being CSF volume, dural ectasia, and the chemical compatibility of
local anaesthetics with adjuncts.
In addition, searches were made using Planet (an AstraZeneca internal database), Biosis, Current Contents,
Embase, PsycINFO, Medline, and Medline Daily update, using the terms Failed Spinal Anaesthesia and
Failed Spinal Anesthesia as sole search terms and spinal anesthesia or spinal anaesthesia or spinal anesthetic or
spinal cord anesthesia or spinal cord anaesthesia or anesthesia, spinal or anaesthesia, spinal and treatment
failure or therapy failure, and Intrathecal. All papers identified as relevant are included in this review.
Previous SectionNext Section
Mechanisms and their prevention
Failed lumbar puncture
Inability to obtain CSF, sometimes referred to as a dry tap, is the only cause of failure which is immediately
obvious. A needle with a lumen blocked at the outset is a theoretical possibility, but is most unlikely with modern
equipment. However, both needle and stylet must be checked for correctness of fit before use, and the needle should
not be advanced without the stylet in place because tissue or blood clot can easily obstruct the fine bore needles used
now. Otherwise, a failed lumbar puncture is virtually always because of either poor positioning of the patient or
incorrect needle insertion, both factors being within the control of the anaesthetist. Abnormalities of the spine
(kyphosis, scoliosis, calcification of ligaments, consequences of osteoporosis), obesity, and patient anxiety make both
positioning the patient and needle insertion more difficult, especially in the elderly. Texts of regional anaesthesia give
more extensive instruction than can be provided here, and good clinical training is the key to success, but most
difficulties are attributable to lack of adherence to the basic rules.
Positioning
The patient is placed on a firm surface; the lumbar laminae and spines are separated maximally by flexing the whole
spine (including the neck), the hips, and knees; rotation and lateral curvature of the spine are avoided; these points
apply to lumbar puncture in both sitting and lateral horizontal positions; the former is usually an easier option in
difficult patients, but sometimes the reverse is true. The role of the assistant in achieving and maintaining the patient
in the correct position cannot be underestimated.35
Needle insertion
Although its accurate identification can be difficult using clinical land-marks, what is judged to be the third lumbar
inter-space is used usually, but examination may indicate that another is preferable. However, care should be taken not
to venture too cephalad and risk damage to the spinal cord.33 With the midline approach, insertion should start
precisely in the mid-line, mid-way between the posterior spines, with the needle shaft at right angles to the back in
both planes. Small, incremental changes in needle angle should be made only if there is resistance to advancement; if
resistance is met, cephalad angulation should be tried first, and such angulation may be appropriate from the start if
the patient is unable to flex fully (e.g. the obstetric patient at term). A degree of caudad angulation is sometimes
needed, with a slight lateral direction being required very rarely. All authorities recommend that the anaesthetist
should have a good knowledge of spinal anatomy and relate these to changes in tissue resistance as the needle is
advanced so that a mental picture of where the needle tip lies is appreciated.
The above points apply specifically to the midline approach; lateral or paramedian approaches are preferred by
some,27 especially if the mid-line ligaments are heavily calcified, but they are inherently more complex techniques.
However, in the face of difficulty, the same basic rules apply: make sure that the patient is in the correct position and
that the correct angles and insertion technique are used.
Adjuncts
A calm, relaxed patient is more likely to assume and maintain the correct position, so explanation (before and during
the procedure) and gentle, unhurried patient handling are vital; light anxiolytic premedication contributes much to
relaxing the patient; local anaesthetic infiltration at the puncture site must be effective without obscuring the
landmarks, but must include both intradermal and s.c. injection. Achieving the correct position is a particular
challenge in the patient in pain (e.g. from a fractured hip) and systemic analgesia (i.v. or inhalation) helps
considerably. The aim of such adjuncts is to optimize the patients position and to prevent any movement. As will be
discussed later, it takes only slight movement to displace the needle from its target.
Advances in ultrasound technology are reaching the stage where it can be used to overcome difficulties with lumbar
puncture, but clinicians will still need to be aware of the problems and how they should be overcome.
Pseudo-successful lumbar puncture
The appearance of clear fluid at the needle hub is usually the final confirmation that the subarachnoid space has been
entered. Rarely, however, the clear fluid is not CSF, but local anaesthetic injected as a top-up for an epidural which
then proved inadequate for a Caesarean section, or even spreading there from the lumbar plexus.26 Unfortunately, a
positive test for glucose in the fluid does not confirm that this fluid is definitely CSF because extracellular fluid
constituents diffuse rapidly into fluids injected into the epidural space. Another, even rarer, suggested cause of clear
fluid appearing at the needle hub, but not confirming successful lumbar puncture, is a congenital arachnoid cyst.39
Solution injection errors
The appearance of CSF in the needle hub is an essential pre-requisite for spinal anaesthesia, but it does not guarantee
success, which also requires that a fully effective dose is both chosen and actually deposited in the CSF.
Dose selection
Studies of many factors influencing intrathecal drug spread have shown that the dose injected, within the range
normally used, has only a small effect on the extent of a spinal anaesthetic, but is far more important in determining
the quality and duration of block.20 Overall, the actual dose chosen will depend on the specific local anaesthetic used,
the baricity of that solution, the patients subsequent posture, the type of block intended, and the anticipated duration
of surgery. Thus, knowledge of the factors influencing intrathecal drug spread and clinical experience with any
particular local anaesthetic preparation are important guides to choosing an effective dose.
However, the need to guarantee an adequate effect means that the doses of drugs injected in standard single shot
techniques are larger than is strictly necessary, experience with dose titration during continuous spinal anaesthesia
showing clearly that lower doses are often effective.21 In attempts to either minimize hypotension, for example by
attempting to produce a unilateral block, or speed postoperative mobilization, by decreasing duration, some
practitioners use lower doses than is traditional3 (e.g. 510 rather than 15 mg of hyperbaric bupivacaine). Used
correctly, and in appropriate situations, such doses can be reliable, but they do mean that the margin for error is
reduced and that the consequences of other problems (e.g. Loss of injectatesee below) will be exaggerated and so
risk an inadequate block. It becomes even more important to ensure that the whole of that lower dose reaches the CSF
and then spreads properly, remembering that the dead space of the needle will contain a significant proportion of
what is a small volume to start with.
Loss of injectate
The Luer connection between syringe and needle provides a ready opportunity for leakage of solution. A particular
variant of this problem being a leak through a defect at the junction of needle hub and shaft.6Given the small volumes
involved, the loss of even a few drops may cause a significant decrease in the mass of drug reaching the CSF, and thus
in its effectiveness. To avoid this, it has long been conventional teaching that the syringe containing the injectate must
be inserted very firmly into the hub of the needle, and that a subsequent check is made that no leakage occurs.
Misplaced injection
Needle and syringe must be connected firmly, but great care should be taken to avoid either anterior or posterior
displacement of the needle tip from subarachnoid to epidural space, where deposition of a spinal dose of local
anaesthetic will have little or no effect. Fluid aspiration, after attachment of the syringe, should confirm free flow of
CSF and, thus, that the needle tip is still in the correct space, but such aspiration may displace the tip unless performed
carefully, as may the force of the injection of the syringe contents. To prevent displacement at any stage, it has been
advocated that the dorsum of one hand should be anchored firmly against the patients back and the fingers used to
immobilize the needle, while the other hand is used to manipulate the syringe.40 Most practitioners would recommend
aspiration for CSF after the injection to confirm that correct placement is maintained, and some advocate that this is
done half way through as well although neither of these practices has been shown to influence the outcome of the
block.3240
Tip displacement must be guarded against with any type of spinal needle, but it is a particular issue with the pencil
point needles now used widely to minimize the incidence of post-dural puncture headache. The opening at the end of
these needles is proximal to the tip, so only a minor degree of backward movement during syringe attachment may
result in epidural injection as was recognized at an early stage in the widespread use of such needles.12 The distances
involved are of the order of a millimetre or two, but (as with leakage) misplacement of only a small amount of
solution can have significant effects. An additional issue with pencil-point needles is that the opening, being much
longer than the bevel of a Quincke needle, may straddle the dura so that some solution reaches the CSF, and some
the epidural space (Fig. 2).41 This may be exaggerated by the dura acting as a flap valve across the needle opening.
Initially, CSF pressure pushes the dura outwards so that aspiration is successful (Fig. 3A), but subsequent injection
pushes the dura forward and the solution is misplaced (Fig. 3B).
View larger version:
In this page
In a new window
Download as PowerPoint Slide
Fig 2
Possible positions of the tip of a pencil-point needle. If it is correctly placed (upper picture) all of the local anaesthetic
solution will reach the subarachnoid space, but if the opening straddles the dura (lower picture) some solution will
be deposited in the epidural space.
View larger version:
In this page
In a new window
Download as PowerPoint Slide
Fig 3
To show how the dura or arachnoid mater may act as a flap valve across the opening of a pencil point needle. During
aspiration (A) the dura/arachnoid are pulled back allowing CSF to enter the needle. During injection the dura (B) or
arachnoid (C) is pushed forward and the local anaesthetic enters the epidural or subdural space.
A variant is that the needle tip penetrates the dura, but it is the arachnoid mater that acts as the flap valve so that a
subdural injection results (Fig. 3C). This misplacement is usually thought of as leading to excessive spread during
epidural block, but the equivalent phenomenon has been described after intended subarachnoid injection,37 and is a
recognized complication of myelography.22 Subdural injection has also been identified as the cause of a failed block
when either epidural11 or subarachnoid15 injection was intended.
These eventualities, being subtle abnormalities of placement, are impossible to identify at the actual time, but rotation
of the needle through 360 after the initial appearance of CSF, and before check aspiration, has been advocated as a
way of minimizing the possibility of them occurring, the theory being that the rotation reduces the risk of the
membrane edges catching on the opening.
Inadequate intrathecal spread
The intrathecal spread of a local anaesthetic solution, even when correctly placed, has truly been described as
capricious.7 The factors that affect it are many, but the focus here will be on those that may result in inadequate
spread.
Anatomical abnormality
Intrathecal spread is governed by interplay between solution physical characteristics, gravity, and the configuration of
the vertebral canal. Anatomical abnormalities that lead to problems with spread can be both overt and covert. The
curves of the vertebral column are integral to solution spread and any obvious abnormality, kyphosis, or scoliosis,
may interfere with the process. Examination of the patient should reveal whether this might occur, but it is not
possible to predict whether the effect will be excessive spread or failure.
A very rare possibility, which is not apparent on examination, is that the ligaments that support the spinal cord within
the theca form complete septae and act as longitudinal or transverse barriers to local anaesthetic spread. This can
result in a block that is entirely unilateral2 or of insufficient cephalad spread. Spinal stenosis or other pathological
lesions might also limit spread, effectiveness, or both, one such case being attributed to the consequences of previous
intrathecal chemotherapy.142Similarly, previous surgery within the vertebral canal may result in adhesions that
interfere with spread.
An interesting abnormality considered to have caused restricted spread in a single patient was a larger than usual
volume of CSF in the lumbar theca.18 Subsequent systematic study has shown that lumbar CSF volume is the most
important factor influencing the variability seen between individuals in the spread of an intrathecal injection.9 A
negative correlation was found between lumbar CSF volume and the peak sensory level achieved with hyperbaric
bupivacaine when the injection was performed in both supine and sitting positions. A variation of this factor is dural
ectasia, which is a pathological enlargement of the dura seen in the majority of patients with Marfans syndrome and
in some other connective tissue disorders.25
Solution density
Consistently effective spinal anaesthesia requires that the practitioner has a good understanding of the factors that
affect intrathecal spread, particularly, but not only, solution density. A solution with a density within the normal range
of that of CSF (isobaric) will virtually guarantee block of the lower limbs with little risk of thoracic nerve block and
thus hypotension.43 However, plain solutions of bupivacaine, although often referred to as isobaric, are actually of
sufficiently lower density to be hypobaric, especially at body temperature. As a result their range of spread is much
less predictable than that of a truly isobaric preparation, and occasionally the block may be no higher than the first, or
even second, lumbar dermatome when administered to the non-pregnant supine patient.29 Although the impact of
variations in CSF volume has yet to be studied with these solutions, it seems likely that this factor may well be a
factor in their variability.
Solutions with a density greater than that of CSF (hyperbaric) move very definitively under the combined influence of
gravity and the curves of the vertebral canal. Over a hundred years ago, Barker, one of the early pioneers of spinal
anaesthesia in the UK, observed that the addition of glucose to the solution made for a more reliable effect.4 In the
standard scenario, that of a patient placed supine after the injection of a hyperbaric preparation at the mid-lumbar
level, the solution will spread down the slope under the effect of gravity to pool at the lowest point of the thoracic
curve, so exposing all nerve roots up to that level to an effective concentration of local anaesthetic. However, if
lumbar puncture is performed at the fourth lumbar or the lumbo-sacral interspace the local anaesthetic may be
trapped below the lumbar curve, especially if the patient is in the sitting position during injection and maintained in
that position for a period thereafter.
This results in a block that is restricted to the sacral segments, just as has been described with a spinal catheter that
passes caudally.31 Prevention relies on avoiding too low an injection level unless, of course, a deliberate saddle
block is intended.
Ineffective drug action
The last possible explanation for a failed spinal is that the solution actually injected reaches the target nerves, but is
inactive or ineffective, with a variety of explanations being possible.
Identification errors
Spinal anaesthetics are supplied in aqueous solution ready for injection and there is no opportunity for confusion in
the preparation of the solution itself. However, other optically clear solutions, such as a separate local anaesthetic for
skin infiltration or analgesic adjuvants, are often used from the same sterile preparation area and the possibility that
confusing them may lead to an ineffective block must be considered. Recognition of the possibility of such injection
errors has led to the widespread use of syringe labelling in anaesthesia, but this is not as easy within a sterile field as it
is on an anaesthetic work station. Attention to detail is essential, but minimizing the number of ampoules on the block
tray (such as using the same local anaesthetic for both skin infiltration and spinal) and consistent use of different sizes
of syringe for each component of the procedure help considerably.
Chemical incompatibility
The mixing of two different pharmaceutical preparations also raises the possibility of ineffectiveness as a result of
interaction between local anaesthetic and adjuvant. Local anaesthetics seem to be compatible with most of the
common opioids, but there has been little formal study of the effects of mixing them, and the situation is even less
definitive with other adjuvants such as clonidine, midazolam, and other more extreme substances. Certainly, there are
no studies of the stability of three or more substances when mixed together for intrathecal use, a not unknown practice
today. Chemical reaction might generate an obvious precipitate, but another possibility is that the pH of the local
anaesthetic solution becomes even lower than it was to start with. This would decrease the concentration of the un-
ionized fraction that is what diffuses into nerve tissue and, unless the solution mixes well with CSF, a decreased effect
could result. There is at least one report indicating that the incidence of failure is greater after the addition of a
vasoconstrictor solution and this could represent an example of this effect.30
Inactive local anaesthetic solution
The older, ester-type local anaesthetics are chemically labile so that heat sterilization and prolonged storage,
particularly in aqueous solution, can make them ineffective because of hydrolysis and hence they need very careful
handling. Although the more modern amide-linked drugs (e.g. lidocaine, bupivacaine, etc.) are much more stable and
can be heat sterilized in solution and then stored for several years without loss of potency, there have been a number
of reports attributing failure of spinal anaesthetics to inactive drug.8163844
Local anaesthetic resistance
Very rarely a failed spinal anaesthetic has been attributed to physiological resistance to the actions of local
anaesthetic drugs, although the reports tend to the anecdotal.5233645 A history of repeated failure of dental or other
local anaesthetic techniques is accompanied by speculation that the problem is because of a sodium-channel mutation
that renders the drugs ineffective. However, no such mutation has ever been described, and the clinical reports are
incomplete, specifically failing to consider not only the recognized causes of failure, but also the behaviour of an
anxious patient preferring general anaesthesia as an explanation for the resistance. Very detailed investigation would
be required for resistance to be accepted as an explanation. As an aside, any patient giving a history of repeated
failures with local anaesthesia should be managed by an experienced clinician.
Failure of subsequent management
Not all of a patients claims of discomfort, or even pain, during a spinal anaesthetic are the result of an inadequate
injection. A properly performed spinal anaesthetic will produce complete somatic, and a major degree of autonomic,
nerve block in the lower half of the body unless a specifically restricted method is used. However, ensuring that this
block occurs is only part of the process because the unaffected components of the nervous system require
consideration and management. Specifically, this relates to conscious awareness of the clinical setting and of
sensations transmitted through unblocked nerves, with both factors possibly making the patient claim that the block
has failed. This may not actually be the case, but patient management certainly has failed if such a claim is made
when the block is actually as good as it could be.
Lying supine and wide awake while undergoing surgery is not a pleasant experience, even for the most sanguine of
individuals, and anxiety alone can cause much difficulty. Further, operating tables are designed for surgical access,
not patient comfort; and intra-abdominal stimuli may result in afferent impulses in unblocked parasympathetic and
phrenic nerve fibres. The more anxious the patient, the greater will be the impact of these factors and the more likely
will it be that the patient will fail to cope with the situation and claim that the anaesthetic has not worked properly.
Expectation plays a part, and good preoperative patient counselling followed by a supportive approach from the
anaesthetist during the operation is important in avoiding such problems, but so is the judicious, and pro-active use
of systemic sedative and analgesic drugs. Sufficient sedation to produce drowsiness, or even sleep (with appropriate
monitoring), is rarely contra-indicated other than in the obstetric situation, and even there small doses may
occasionally be useful.
Testing the block
In recent years, it has become almost mandatory, certainly in the obstetric setting, to test the level of block formally
before surgery commences. This apparently sensible precaution may be difficult or impossible to undertake in some
patients (for example the demented patient with a fractured neck of femur). Excessive focus on testing can also have a
negative impact. Most patients will have some anxiety about the effectiveness of the injection, and this will be
increased if testing is started too soon. Conventional practice is to check motor block by testing the ability to lift the
legs, followed by testing of sensory block to stimuli such as soft touch, cold, or pin prick, all of which have their
proponents. It is advisable to start testing in the lower segments, where onset will be fastest, and work upwards.
Proving early on that there is some effect encourages patient confidence; testing too soon does the opposite.
Even if there is no formal assessment of the level of block, the clinician must be confident that an adequate block has
been produced. Establishing that the level of block is appropriate for the projected surgery is often taken to
demonstrate that the quality of block is adequate also, but this is not always the case if cold or pin-prick stimuli are
used. The observation that the upper block level is a few dermatomes above which innervate the surgical field (not
forgetting the deeper structures) is a good start, but it does not guarantee that the quality of block is sufficient. A
covert pinch of the site of the proposed surgical incision may be a better indicator of skin analgesia, and can be
reassuring if the block has been slow in onset. Indeed, there is much to be said, particularly when the patient is
conscious, for asking the surgeon to do the same with a toothed surgical forceps before incising the skin,10 but
surreptitiously andwithout asking a loaded question such as Does that hurt?! The patient is distracted by
conversation and an exchange of glances between surgeon and anaesthetist is all that is needed for surgery to begin.
Catheter and combined techniques
The great majority of spinal anaesthetics involve a single, through needle injection and, as has been noted, this
requires some certainty about its effectiveness for surgery. To take advantage of the rapid onset and profound block of
spinal anaesthesia, both continuous and combined spinalepidural techniques have been introduced to increase
flexibility. If the catheters are correctly placed, problems of inadequate spread, quality, and duration of effect can be
dealt with although many of the potential technical problems outlined above can still apply. However, both methods
require a greater level of skill and experience to use, the insertion of an intrathecal catheter can be surprisingly
difficult to achieve in some patients and, as has been mentioned already, can result in the misdirection of the local
anaesthetic solution, with the risk of neurotoxicity.34 It is vital to leave no more than 23 cm of catheter within the
dura to avoid this. In the combined technique, it is common to inject a relatively small volume for the spinal
component, so the problems that can result in a proportion not reaching the subarachnoid space are very relevant, but
at least the epidural catheter can be used in attempts to rescue the situation.
Previous SectionNext Section
Management of failure
Failure of a spinal anaesthetic is an event of significant concern for both patient and anaesthetist even when it is
immediately apparent, but it can have serious consequences (clinical and medico-legal) if the problem only becomes
evident once surgery has started. If there is any doubt about the nature or duration of the proposed surgery, a method
other than a standard spinal anaesthetic should be used. The trainee anaesthetist should avoid over-selling the
technique, especially in the early days of unsupervised practice. Promising that all will be achieved by one injection
leaves no room for manoeuvre, but offering one injection to reduce pain and a second to ensure unconsciousness does.
If a spinal anaesthetic does fail in some way, the management options are limited; so, the first rule is to expend every
effort in prevention.
Prevention is better than cure
Having made the decision to use a spinal anaesthetic, the block should be performed with meticulous attention to
detail as has been indicated above. It is impossible to over-emphasize this point.
The failed block
The precise management of the failed block will depend on the nature of the inadequacy and the time at which it
becomes apparent. Thus, some monitoring of the onset of the block and correct interpretation of the observations are
both vital. The slower the onset of either motor or sensory block, the more likely is the block to be inadequate, so the
more detailed this assessment should be. While the onset of spinal anaesthesia is rapid in most patients, it can be slow
in some; so, tincture of time should always be allowed.10 However, if most of the expected block has not developed
within 15 min, some additional manoeuvre is almost certainly going to be needed. The possibilities, their
explanations, and suggested immediate responses are as follows:
1. No block: the wrong solution has been injected, it has been deposited in the wrong place, or it is ineffective.
Repeating the procedure or conversion to general anaesthesia are the only option. If, after operation, the
patient has significant pruritus, it is likely that only an opioid was injected.
2. Good block of inadequate cephalad spread: the level of injection was too low, anatomical abnormality has
restricted spread, or some injectate has been misplaced. If a hyperbaric solution was used, flex the patients
hips and knees and tilt the table head down. This straightens out the lumbar curve, but maintains a cephalad
slope and allows any solution trapped in the sacrum to spread further. A variation with the same aim, but
perhaps better suited to the obstetric situation, is to turn the patient to the full lateral position with a head
down tilt, reversing the side after 23 min. If a plain (and usually slightly hypobaric) solution has been used,
it may help to sit the patient up, but beware of peripheral pooling of blood.
If a spinal catheter injection results in inadequate spread, the response should not be to inject more of the
same solution because dose has minimal effect on intrathecal spread.20 Either posture should be manipulated
as above, or a different baricity of solution should be tried, or the catheter should be withdrawn before the
injection is repeated.31
3. Good, but unilateral block: this is most likely because of positioning, but it is possible that longitudinal
ligaments supporting the cord have blocked spread. If the operation is to be on the anaesthetized limb, then
the surgeon should know that the other leg has sensation, and the patient should be reassured and closely
monitored. Otherwise, turning the patient onto the unblocked side if a hyperbaric solution was used (or the
reverse for plain solutions) may facilitate spread.
4. Patchy block (This term is used to describe a block that appears adequate in extent, but the sensory and
motor effects are incomplete.): causes of inadequate block are numerous and include all those discussed
above, but the most likely explanation is that the local anaesthetic was at least partially misplaced, or that the
dose given was inadequate. If this becomes apparent before surgery starts, the options are to repeat the spinal
injection or to use a greater degree of systemic supplementation than was planned, the latter being the only
option after skin incision. It may not be necessary to recourse to general anaesthesia, sedation, or analgesic
drugs often being sufficient especially when patient anxiety is a major factor. Infiltration of the wound and
other tissues with local anaesthetic by the surgeon may also be useful in such situations.
5. Inadequate duration: the most likely explanation is that for one of several reasons an inadequate dose of
local anaesthetic was delivered to the CSF. Alternatively, lidocaine (intended for skin infiltration) was
confused for bupivacaine, or the operation has taken longer than expected. Systemic supplementation or
infiltration of local anaesthetic may tide matters over, but often the only option is to convert to general
anaesthesia.
Repeating the block
Where no effect at all has followed the injection it seems reasonable to repeat the procedure, paying close attention to
avoiding the potential pitfalls. In all other situations besides total failure, there must be some local anaesthetic in the
CSF already, and anxieties relating to several issues have to be taken into account:
1. A restricted block may be because of some factor, probably anatomical, impeding the physical spread of the
solution, and it may have exactly the same impact on a second injection, resulting in a high concentration of
local anaesthetic at or close to the site of injection. Cauda equina lesions were described after continuous
spinal anaesthesia when very restricted spread prompted repeat injections rather than the manipulation of
other factors,34 and a similar problem has been described after repeated needle injection.1419
2. Repeat injection, especially in response to a poor quality block, may lead to excessive spread,13 so it may be
argued that a lower dose should be used to reduce the risk of this possibility.
3. A good quality, but unilateral block, might lead to an attempt to place a second injection into the other side
of the theca, but the risk of placing the second dose in the same side must be significant.
4. Barriers to spread within the subarachnoid space may also affect epidural spread (and vice versa), so an
attempt at epidural block may not succeed either.
5. A block of inadequate cephalad spread might be overcome by repeating the injection at a higher level, but
should perhaps only be attempted when the indication for a regional technique is considerable.
6. The final concern, particularly applicable to the last mentioned, but relevant to nearly all situations where a
repeat block might be considered, is that the adjacent nerve tissue is already affected by local anaesthetic
action so that the risk of direct needle trauma is increased.
Only some of these problems have actually been described, most being in the category of theoretical possibilities, but
such concerns do reinforce the view that every effort must be made to ensure that the first injection is fully effective.
Recourse to general anaesthesia
There are many ways in which an inadequate block might be rescued, but there is a limit to how much discomfort or
distress an individual patient can tolerate, so general anaesthesia must be considered if one or two simple measures
have not rectified matters. Common sense and clinical experience are usually the best indicators of exactly when to
convert to general anaesthesia, so the unsupervised trainee can be at a disadvantage. However, it is far better to make
the decision sooner rather than later and have to deal with a seriously distressed patient. Of course, explaining later
why the anticipated technique had not been provided can be difficult. It is another reason why prevention (getting the
block right to start with) is the best approach, but it is also a reason for not over-selling the regional approach before
operation.
If general anaesthesia is induced to supplement a partially effective spinal anaesthetic, any degree of sympathetic
nerve block will make hypotension more likely.
Follow-up initiatives
Clinical follow-up
As with any anaesthetic complication, the details should be documented fully in the notes, and the patient provided
with an apology and a full explanation after operation. Giving the patient a written summary of events for presentation
to a future anaesthetist can be very helpful, although care should be taken to prevent medico-legal recourse. Rarely,
inadequate spread has been the first indication of pathology within the vertebral canal. Therefore, it may be
appropriate to look for symptoms and signs of neurological disease, and involve a neurologist if there is any suspicion
of these being present.
It is during the follow-up of a patient in whom no block was obtained, the possibility of local anaesthetic resistance
may seem an attractive explanation. As has already been noted, much wider consideration of the possibilities,
supported by very detailed investigation, is needed than has been the case in previous reports.
Investigating local anaesthetic effectiveness
Spinal anaesthesia is usually a simple and effective technique, but failure can occur at any time and in the hands of
any clinician, no matter how experienced. However, if the procedure has, apparently, been routine and straightforward
concerns can arise that the current supply of local anaesthetic is defective, especially if two or more such failures
occur in the same hospital within a short period of time. The preparations which have been most implicated are those
of hyperbaric bupivacaine (probably because it is the drug used most commonly at present), with drug from both
major suppliers, Abbott38 and AstraZeneca,81644 being involved. In fact, the chemical stability of the amide drugs
and modern standards of pharmaceutical manufacture mean that drug inactivity is a most unlikely cause of a failed
spinal anaesthetic, but it remains a possibility which at least has to be eliminated.
As has been suggested, performing skin infiltration with some of the solution intended for the spinal injection should
demonstrate that it is effective. If the concern continues the operating theatre, pharmacy and anaesthetic department
records should be cross-checked to see whether other practitioners in the hospital have experienced any problems.
Similarly, distributors should be able to check whether other hospitals which have been supplied with material from
the same batch have reported difficulty. If such enquiries reveal that others are using the same material to good effect,
the clinician should consider the advice of those two great authorities, Lee and Atkinson, on The spinal that does not
take:
All experienced workers have encountered this occasionally even though accepted procedure has apparently been
followed. Reflection, however, usually discloses some flaw in technique. In 1907 Alfred E. Barker wrote that for
successful spinal analgesia it is necessary to enter the lumbar dural sac effectually with the point of the needle, and to
discharge through this, all the contemplated dose of the drug, directly and freely into the cerebrospinal fluid, below
the termination of the cord (Barker, 1907). Failure to follow the details of this advice is the commonest cause of a
poor result.27
The Author [2009]. Published by Oxford University Press on behalf of The Board of Directors of the British Journal of Anaesthesia. All rights
reserved. For Permissions, please email: journals.permissions@oxfordjournal.org
Ads not by this site
You might also like
- Artritis Reumatoide, Epidemiología, Fisiopatología, Criterios Diagnósticos y TratamientoDocument9 pagesArtritis Reumatoide, Epidemiología, Fisiopatología, Criterios Diagnósticos y TratamientoErandy BetsabeNo ratings yet
- 052 Simple Future Tense Using Will Ejercicios DownloadDocument2 pages052 Simple Future Tense Using Will Ejercicios DownloadJuan Mantilla LinaresNo ratings yet
- Protocolo Analgesia PostoperatoriaDocument66 pagesProtocolo Analgesia PostoperatoriaChurrunchaNo ratings yet
- 053 Simple Future Tense Using Going To Ejercicios DownloadDocument2 pages053 Simple Future Tense Using Going To Ejercicios DownloadJuan Mantilla LinaresNo ratings yet
- Guia Clinica Sobre El Tratamiento Del DoDocument110 pagesGuia Clinica Sobre El Tratamiento Del DoJuan Mantilla LinaresNo ratings yet
- 051 Whats Your Name Listening Practice Ejercicios DownloadDocument2 pages051 Whats Your Name Listening Practice Ejercicios DownloadJuan Mantilla LinaresNo ratings yet
- Guia de Practica AmazonasDocument44 pagesGuia de Practica AmazonasJuan Mantilla LinaresNo ratings yet
- La Metodologia de Estudio Denominado Test Class o Prueba de PracticaDocument2 pagesLa Metodologia de Estudio Denominado Test Class o Prueba de PracticaJuan Mantilla LinaresNo ratings yet
- Los Corticoides Epidurales en El Tratamiento de La Hernia DiscalDocument8 pagesLos Corticoides Epidurales en El Tratamiento de La Hernia DiscalJuan Mantilla LinaresNo ratings yet
- MatrimonioDocument40 pagesMatrimonioJuan Mantilla LinaresNo ratings yet
- Guia Auditoria Certificaciones Medicas Maternidad 2016Document36 pagesGuia Auditoria Certificaciones Medicas Maternidad 2016Juan Mantilla LinaresNo ratings yet
- Arritmias VentricularesDocument42 pagesArritmias VentricularesJesus David Tobias BallesterosNo ratings yet
- Esteroide Epid Lumbalgia CronicaDocument6 pagesEsteroide Epid Lumbalgia CronicaJuan Mantilla LinaresNo ratings yet
- Epidemiología de La Injuria Renal Aguda (AKI) : Dr. Guillermo Villamizar RDocument28 pagesEpidemiología de La Injuria Renal Aguda (AKI) : Dr. Guillermo Villamizar RJuan Mantilla LinaresNo ratings yet
- Anestesia Subaracnoidea PediatriaDocument16 pagesAnestesia Subaracnoidea PediatriaJuan Mantilla LinaresNo ratings yet
- Ecografía Aplicada A A Vía AéreaDocument9 pagesEcografía Aplicada A A Vía AéreaJuan Mantilla LinaresNo ratings yet
- Ecografia Portatil Paciente Disnea AgudaDocument87 pagesEcografia Portatil Paciente Disnea AgudaCastillo JaimeNo ratings yet
- Actualización de La Guìa de RCP en Niños 2010Document62 pagesActualización de La Guìa de RCP en Niños 2010Benjamin CalispaNo ratings yet
- Liquidos y Electrolitos en Pediatria... KvO!!!Document59 pagesLiquidos y Electrolitos en Pediatria... KvO!!!Kevin FloresNo ratings yet
- RAE CBM-BF Aspectos Básicos Del Manejo de La Vía Aérea PDFDocument10 pagesRAE CBM-BF Aspectos Básicos Del Manejo de La Vía Aérea PDFManuel MesaNo ratings yet
- Cma 054 FDocument10 pagesCma 054 Fdiego_b_mdNo ratings yet
- Articulo Erc 2017 PDFDocument5 pagesArticulo Erc 2017 PDFedward_10No ratings yet
- 3451 4034 2 PB PDFDocument24 pages3451 4034 2 PB PDFJuan Mantilla LinaresNo ratings yet
- Ecograf Identif Colocac TETDocument8 pagesEcograf Identif Colocac TETJuan Mantilla LinaresNo ratings yet
- Analg y Sedac Niño Con VMDocument10 pagesAnalg y Sedac Niño Con VMJuan Mantilla LinaresNo ratings yet
- 20180821110844Document1 page20180821110844Juan Mantilla LinaresNo ratings yet
- VENT MEC J. Blanco. 2Document35 pagesVENT MEC J. Blanco. 2Juan Mantilla LinaresNo ratings yet
- Ensayo AdministracionDocument4 pagesEnsayo AdministracionJuan Mantilla LinaresNo ratings yet
- Canales Iónicos: Ciertos Iones SelectividadDocument27 pagesCanales Iónicos: Ciertos Iones SelectividadJosué Hidalgo BustamanteNo ratings yet
- Ruggiero Regionalus 130106100208 Phpapp01 PDFDocument78 pagesRuggiero Regionalus 130106100208 Phpapp01 PDFJuan Mantilla LinaresNo ratings yet
- AnestesiaDocument2 pagesAnestesiaAnestesiologia IrenNo ratings yet
- Metodos de Captura, Manejo y AnestesiaDocument28 pagesMetodos de Captura, Manejo y AnestesiaMerlin GuzmánNo ratings yet
- Anestesia en El Animal de Laboratorio. Parte 4Document6 pagesAnestesia en El Animal de Laboratorio. Parte 4Claudiita LopezNo ratings yet
- Riesgos Ambientales QuirurgicaDocument8 pagesRiesgos Ambientales QuirurgicaDee Dee Weasley SmithNo ratings yet
- Historia de La CirugiaDocument23 pagesHistoria de La CirugiaKarol NarvNo ratings yet
- Sufrimiento Fetal AgudoDocument42 pagesSufrimiento Fetal AgudoElided Garcia CamposNo ratings yet
- Taller Cuidados de Enfermeria en Fase TransDocument2 pagesTaller Cuidados de Enfermeria en Fase TransJUAN MIGUEL BEDOYA MIRANDANo ratings yet
- Repaso de Farma 3er NuevoDocument37 pagesRepaso de Farma 3er NuevoIƨabel Mora ﭢNo ratings yet
- Iii Reunion Sacar - Dipticos PDFDocument2 pagesIii Reunion Sacar - Dipticos PDFSacar AnestesiologiaNo ratings yet
- Anestesia General y SedaciónDocument6 pagesAnestesia General y Sedaciónalejandro la portaNo ratings yet
- Catalogo de ProductosDocument22 pagesCatalogo de ProductosJackE.LozanoFernandezNo ratings yet
- Introducion A La CirugiaDocument47 pagesIntroducion A La CirugiaMirian VerdesNo ratings yet
- Cirugía AmbulatoriaDocument32 pagesCirugía AmbulatoriaGABRIELA YAZMIN SANCHEZ ZARATENo ratings yet
- Diagrama de Flujo 4 FarmaDocument2 pagesDiagrama de Flujo 4 FarmaXJuliox Cesar0% (1)
- BarbituricosDocument26 pagesBarbituricosOlenk LMNo ratings yet
- Practica 7Document12 pagesPractica 7Carlos NovoaNo ratings yet
- Intoxicacion Por Anestesicos LocalesDocument15 pagesIntoxicacion Por Anestesicos LocalesRodrigo MéridaNo ratings yet
- Monitorización Perioperatoria Del Oxígeno y CO2Document11 pagesMonitorización Perioperatoria Del Oxígeno y CO2agostina210% (1)
- Administración de AnestesiaDocument5 pagesAdministración de Anestesiapatricio sobarzoNo ratings yet
- Anestesiologia PediatricaDocument65 pagesAnestesiologia PediatricaAbel Aruquipa MarcaNo ratings yet
- Vaporizadores ExpoDocument9 pagesVaporizadores ExpoCarlos Alberto SacsaNo ratings yet
- Tecnicas de AnestesiaDocument18 pagesTecnicas de AnestesiaGissela López50% (2)
- Mapa ConceptualDocument1 pageMapa Conceptualafrc297100% (1)
- Vet Flu RaneDocument9 pagesVet Flu RaneEpic ProcrackNo ratings yet
- Anestesia Dra. Ivon Mares VelezDocument75 pagesAnestesia Dra. Ivon Mares VelezamandamissNo ratings yet
- Anestesia Regional Vs Anestesia GeneralDocument11 pagesAnestesia Regional Vs Anestesia GeneralPatylu OrdónezNo ratings yet
- Informe de Anestesia 2023Document2 pagesInforme de Anestesia 2023leo ArceNo ratings yet
- Medicamentos en CirugiaDocument50 pagesMedicamentos en CirugiaAlexandra MarinNo ratings yet
- Manual Usuario Cardiotecnica ECGDocument46 pagesManual Usuario Cardiotecnica ECGMaria Soledad PetrinoNo ratings yet
- Silabo Cirugía I 2019-Ii - 20190810183902 PDFDocument29 pagesSilabo Cirugía I 2019-Ii - 20190810183902 PDFMartin Rivera TorresNo ratings yet