You might also like
- Curry PowderDocument8 pagesCurry PowderMahendar Vanam100% (1)
- Assertmodule 1Document9 pagesAssertmodule 1Olivera Mihajlovic TzanetouNo ratings yet
- A Systematic Review of Impression Technique For ConventionalDocument7 pagesA Systematic Review of Impression Technique For ConventionalAmar BhochhibhoyaNo ratings yet
- Afpam47 103v1Document593 pagesAfpam47 103v1warmil100% (1)
- Stress Fatigue PrinciplesDocument12 pagesStress Fatigue Principlesjinny1_0No ratings yet
- Dental Anxiety QuestionnairesDocument4 pagesDental Anxiety QuestionnairesAmar BhochhibhoyaNo ratings yet
- Jurnal AntibiotikDocument5 pagesJurnal AntibiotikSela PutrianaNo ratings yet
- Effects of Systematic Oral Care in Critically Ill PatientsDocument7 pagesEffects of Systematic Oral Care in Critically Ill PatientsCarlene AlincastreNo ratings yet
- IntroductionDocument11 pagesIntroductionshrikantNo ratings yet
- Schwartz 2007Document8 pagesSchwartz 2007adriana Ortega CastilloNo ratings yet
- Advancing Infection Control in Dental Care SettingDocument12 pagesAdvancing Infection Control in Dental Care SettingEndang SetiowatiNo ratings yet
- Evidence Based Practise of Oral MedicineDocument10 pagesEvidence Based Practise of Oral MedicineshrikantNo ratings yet
- 10.1007/s00520 013 1942 0 PDFDocument13 pages10.1007/s00520 013 1942 0 PDFhendra ardiantoNo ratings yet
- Prescribing Trends of Systemic Antibiotics by Periodontists in AustraliaDocument27 pagesPrescribing Trends of Systemic Antibiotics by Periodontists in AustraliaMohammad HarrisNo ratings yet
- Clinical Efficacy of Local Delivered Minocycline in The Treatment of Chronic Periodontitis Smoker PatientsDocument5 pagesClinical Efficacy of Local Delivered Minocycline in The Treatment of Chronic Periodontitis Smoker PatientsvivigaitanNo ratings yet
- General Practitioner Antimicrobial Stewardship Programme Study (GAPS) : Protocol For A Cluster Randomised Controlled TrialDocument9 pagesGeneral Practitioner Antimicrobial Stewardship Programme Study (GAPS) : Protocol For A Cluster Randomised Controlled TrialAlexandrahautaNo ratings yet
- A Study of Prescription Pattern of Antibiotics in Pediatric In-Patients of Mc-Gann Teaching Hospital Shivamogga Institute of Medical Sciences (SIMS), Shivamogga, Karnataka.Document5 pagesA Study of Prescription Pattern of Antibiotics in Pediatric In-Patients of Mc-Gann Teaching Hospital Shivamogga Institute of Medical Sciences (SIMS), Shivamogga, Karnataka.International Organization of Scientific Research (IOSR)No ratings yet
- Swoope1977 PDFDocument8 pagesSwoope1977 PDFKrupali JainNo ratings yet
- Oral Care Practice For The Ventilated Patients in Intensive Care Units: A Pilot SurveyDocument7 pagesOral Care Practice For The Ventilated Patients in Intensive Care Units: A Pilot SurveyRochman MujayantoNo ratings yet
- Di Susun Untuk Memenuhi Tugas Mata Kuliah Mikrobiologi Dan ParasitologiDocument5 pagesDi Susun Untuk Memenuhi Tugas Mata Kuliah Mikrobiologi Dan ParasitologiJulfianas Bekti WahyuniNo ratings yet
- Study DesignsDocument36 pagesStudy Designsz6f9cw8vwvNo ratings yet
- Venugopalan2016 PDFDocument7 pagesVenugopalan2016 PDFSyahidatul Kautsar NajibNo ratings yet
- The Prevalence of Malnutrition in Hospitals Can Be Reduced: Results From Three Consecutive Cross-Sectional StudiesDocument11 pagesThe Prevalence of Malnutrition in Hospitals Can Be Reduced: Results From Three Consecutive Cross-Sectional StudiesManlio Fabio FelixNo ratings yet
- Ab Round StewardshipDocument7 pagesAb Round StewardshipbpinsaniNo ratings yet
- Evidence-Basedprosthodontics: Fundamental Considerations, Limitations, and GuidelinesDocument17 pagesEvidence-Basedprosthodontics: Fundamental Considerations, Limitations, and GuidelinesRohan BhagatNo ratings yet
- Bell 2012Document13 pagesBell 2012badria bawazirNo ratings yet
- Oral Care in Ventilation MechanicDocument8 pagesOral Care in Ventilation MechanicRusida LiyaniNo ratings yet
- Patient Perceptions of The Role of Nutrition For Pressure Ulcer Prevention in HospitalDocument7 pagesPatient Perceptions of The Role of Nutrition For Pressure Ulcer Prevention in HospitalSher UmarNo ratings yet
- Contents DCLDocument3 pagesContents DCLpopy ApriliaNo ratings yet
- Antibiotic Prescribing and Resistance:: Views From Low-And Middle-Income Prescribing and Dispensing ProfessionalsDocument42 pagesAntibiotic Prescribing and Resistance:: Views From Low-And Middle-Income Prescribing and Dispensing ProfessionalsFaozan FikriNo ratings yet
- Evid Based Nurs 2000 Treatment 75Document2 pagesEvid Based Nurs 2000 Treatment 75Dyana Fitri EningsihNo ratings yet
- 18factores Asociados Al Llamado Por Tto Oncologico Monestime Page 2020Document8 pages18factores Asociados Al Llamado Por Tto Oncologico Monestime Page 2020Milizeth VmNo ratings yet
- Knowledgeartyku PDFDocument9 pagesKnowledgeartyku PDFAhmed Abdulleh Al Hada'aNo ratings yet
- EBM of DyspepsiaDocument228 pagesEBM of DyspepsiaxcalibursysNo ratings yet
- Epic3 National Evidence-Based Guidelines For Preventing HCAI in NHSEDocument70 pagesEpic3 National Evidence-Based Guidelines For Preventing HCAI in NHSECarmen VarodiNo ratings yet
- ADA Adult Acute Dental Pain Guideline 2023Document25 pagesADA Adult Acute Dental Pain Guideline 2023Elaf AlBoloshiNo ratings yet
- Validity Two Methods For Assessing Oral Health Status of PopulationsDocument9 pagesValidity Two Methods For Assessing Oral Health Status of PopulationsSyarifah HaizanNo ratings yet
- Antibiotic Dosage Prescribed in Oral Implant Surgery: A Meta-Analysis of Cross-Sectional SurveysDocument16 pagesAntibiotic Dosage Prescribed in Oral Implant Surgery: A Meta-Analysis of Cross-Sectional SurveysShounak GhoshNo ratings yet
- Knowledge, Attitudes, Practices and Status of Oral Health Among Diabetic Patients at Kikuyu HospitalDocument2 pagesKnowledge, Attitudes, Practices and Status of Oral Health Among Diabetic Patients at Kikuyu HospitalNthie UnguNo ratings yet
- Williams Et Al-2019-Cochrane Database of Systematic ReviewsDocument4 pagesWilliams Et Al-2019-Cochrane Database of Systematic ReviewsErlinda AlfaNo ratings yet
- Emergency Dental Treatment Among Patients Waitlisted For The Operating RoomDocument5 pagesEmergency Dental Treatment Among Patients Waitlisted For The Operating RoomnatalyaNo ratings yet
- 17Document7 pages17bie2xNo ratings yet
- Compliance With Universal Precautions in A Medical Practice With A High Rate of HIV InfectionDocument6 pagesCompliance With Universal Precautions in A Medical Practice With A High Rate of HIV InfectionDirga Rasyidin LNo ratings yet
- Artigo - Compliance Oral Nutrition Supplement - ReviewDocument20 pagesArtigo - Compliance Oral Nutrition Supplement - ReviewFrancielle A.RNo ratings yet
- The Need For Pharmaceutical Care in An Intensive Care Unit at A Teaching Hospital in South AfricaDocument4 pagesThe Need For Pharmaceutical Care in An Intensive Care Unit at A Teaching Hospital in South AfricaAdibaNo ratings yet
- G AntibiotictherapyDocument3 pagesG AntibiotictherapyJavangula Tripura PavitraNo ratings yet
- Gibson 2010Document19 pagesGibson 2010fiora.ladesvitaNo ratings yet
- 0300060517740813Document13 pages0300060517740813Putu Ayu Krisna Sutrisni21No ratings yet
- The Use of Fibre OpticcarioDocument3 pagesThe Use of Fibre OpticcarioNelly AndriescuNo ratings yet
- Determinants Impacting The Use of Antibiotics Among Patients Visiting The Dental Clinic at Kampala International University Teaching Hospital in Bushenyi-Ishaka Municipality, WesteDocument15 pagesDeterminants Impacting The Use of Antibiotics Among Patients Visiting The Dental Clinic at Kampala International University Teaching Hospital in Bushenyi-Ishaka Municipality, WesteKIU PUBLICATION AND EXTENSIONNo ratings yet
- Angela M Berry 2011Document6 pagesAngela M Berry 2011M Farid AzNo ratings yet
- DyspepsiaDocument228 pagesDyspepsiaamal.fathullah100% (1)
- Editorials: Evidence Based Medicine: What It Is and What It Isn'tDocument4 pagesEditorials: Evidence Based Medicine: What It Is and What It Isn'tDanymilosOroNo ratings yet
- JIndianSocPedodPrevDent344348-3624096 100400Document6 pagesJIndianSocPedodPrevDent344348-3624096 100400drkameshNo ratings yet
- How Decisions Are Made Antibiotic Stewardship in DentistryDocument6 pagesHow Decisions Are Made Antibiotic Stewardship in DentistryMuhammad SdiqNo ratings yet
- Corresponding Author: Mojtaba Vaismoradi, Faculty of Professional Studies, Nord UniversityDocument24 pagesCorresponding Author: Mojtaba Vaismoradi, Faculty of Professional Studies, Nord UniversityTeddy Kurniady ThaherNo ratings yet
- JP Journals 10024 2084Document8 pagesJP Journals 10024 2084darwinNo ratings yet
- 747-Article Text-1365-1-10-20200430Document6 pages747-Article Text-1365-1-10-20200430Yogita DhurandharNo ratings yet
- Infection Control & Hospital EpidemiologyDocument9 pagesInfection Control & Hospital EpidemiologyRianNo ratings yet
- Research ArticleDocument7 pagesResearch ArticleMohammed Falih HassanNo ratings yet
- The Timeliness of Patients Reporting The Side Effects of ChemotherapyDocument8 pagesThe Timeliness of Patients Reporting The Side Effects of ChemotherapyChristine SiburianNo ratings yet
- New Oral Care With ClorhedineDocument10 pagesNew Oral Care With ClorhedineZil FadilahNo ratings yet
- Advances in Managing Fistulizing Crohn’s Disease: A Multidisciplinary ApproachFrom EverandAdvances in Managing Fistulizing Crohn’s Disease: A Multidisciplinary ApproachNo ratings yet
- Groper's ApplianceDocument4 pagesGroper's Appliancejinny1_0No ratings yet
- E Adaproceedings-Child AbuseDocument64 pagesE Adaproceedings-Child Abusejinny1_0No ratings yet
- AAPD Policy On - FluorideUseDocument2 pagesAAPD Policy On - FluorideUsejinny1_0No ratings yet
- GicDocument5 pagesGicmrnitin82No ratings yet
- G - TMD-pedo MNGMT PDFDocument6 pagesG - TMD-pedo MNGMT PDFjinny1_0No ratings yet
- Pulp Therapy-Guideline AapdDocument8 pagesPulp Therapy-Guideline Aapdjinny1_0No ratings yet
- EEL 7 SpeakingDocument20 pagesEEL 7 SpeakingSathish KumarNo ratings yet
- Mucosa in Complete DenturesDocument4 pagesMucosa in Complete Denturesspu123No ratings yet
- Article-PDF-Amit Kalra Manish Kinra Rafey Fahim-25Document5 pagesArticle-PDF-Amit Kalra Manish Kinra Rafey Fahim-25jinny1_0No ratings yet
- Spacer Design Jips 2005 PDFDocument5 pagesSpacer Design Jips 2005 PDFjinny1_0No ratings yet
- GoldsDocument11 pagesGoldsjinny1_0No ratings yet
- DisinfectionDocument5 pagesDisinfectionjinny1_0No ratings yet
- KurthDocument18 pagesKurthjinny1_0No ratings yet
- Die HardnerDocument4 pagesDie Hardnerjinny1_0No ratings yet
- ResinDocument8 pagesResinjinny1_0No ratings yet
- Denture Base Resin CytotoxityDocument7 pagesDenture Base Resin Cytotoxityjinny1_0No ratings yet
- Oral Mucosal Lesions Associated With The Wearing of Removable DenturesDocument17 pagesOral Mucosal Lesions Associated With The Wearing of Removable DenturesnybabyNo ratings yet
- Implant AngulationDocument17 pagesImplant Angulationjinny1_0No ratings yet
- 7Document8 pages7jinny1_0No ratings yet
- Patient-Assessed Security Changes When Replacing Mandibular Complete DenturesDocument7 pagesPatient-Assessed Security Changes When Replacing Mandibular Complete Denturesjinny1_0No ratings yet
- 3Document7 pages3jinny1_0No ratings yet
- Avg Vs NormalDocument1 pageAvg Vs Normaljinny1_0No ratings yet
- AlginateDocument5 pagesAlginatejinny1_0No ratings yet
- 11Document7 pages11jinny1_0No ratings yet
- Long-Term Cytotoxicity of Dental Casting AlloysDocument8 pagesLong-Term Cytotoxicity of Dental Casting Alloysjinny1_0No ratings yet
- Kalitantra-Shava Sadhana - WikipediaDocument5 pagesKalitantra-Shava Sadhana - WikipediaGiano BellonaNo ratings yet
- ELS 15 Maret 2022 REVDocument14 pagesELS 15 Maret 2022 REVhelto perdanaNo ratings yet
- PresentationDocument6 pagesPresentationVruchali ThakareNo ratings yet
- Proposal For A Working Procedure To Accurately Exchange Existing and New Calculated Protection Settings Between A TSO and Consulting CompaniesDocument9 pagesProposal For A Working Procedure To Accurately Exchange Existing and New Calculated Protection Settings Between A TSO and Consulting CompaniesanonymNo ratings yet
- EVS (Yuva)Document88 pagesEVS (Yuva)dasbaldev73No ratings yet
- Project 2 Analysis of Florida WaterDocument8 pagesProject 2 Analysis of Florida WaterBeau Beauchamp100% (1)
- Competent Testing Requirements As Per Factory ActDocument3 pagesCompetent Testing Requirements As Per Factory Actamit_lunia100% (1)
- Mat101 w12 Hw6 SolutionsDocument8 pagesMat101 w12 Hw6 SolutionsKonark PatelNo ratings yet
- Test Bank For Global Marketing Management 6th Edition Masaaki Mike Kotabe Kristiaan HelsenDocument34 pagesTest Bank For Global Marketing Management 6th Edition Masaaki Mike Kotabe Kristiaan Helsenfraught.oppugnerp922o100% (43)
- New Horizon Public School, Airoli: Grade X: English: Poem: The Ball Poem (FF)Document42 pagesNew Horizon Public School, Airoli: Grade X: English: Poem: The Ball Poem (FF)stan.isgod99No ratings yet
- Review Test 1: Circle The Correct Answers. / 5Document4 pagesReview Test 1: Circle The Correct Answers. / 5XeniaNo ratings yet
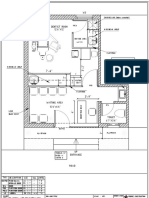
- Dental Clinic - Floor Plan R3-2Document1 pageDental Clinic - Floor Plan R3-2kanagarajodisha100% (1)
- M 995Document43 pagesM 995Hossam AliNo ratings yet
- Design of Ka-Band Low Noise Amplifier Using CMOS TechnologyDocument6 pagesDesign of Ka-Band Low Noise Amplifier Using CMOS TechnologyEditor IJRITCCNo ratings yet
- Manual ML 1675 PDFDocument70 pagesManual ML 1675 PDFSergio de BedoutNo ratings yet
- 3.1.1 - Nirmaan Annual Report 2018 19Document66 pages3.1.1 - Nirmaan Annual Report 2018 19Nikhil GampaNo ratings yet
- Recent Advances in Dielectric-Resonator Antenna TechnologyDocument14 pagesRecent Advances in Dielectric-Resonator Antenna Technologymarceloassilva7992No ratings yet
- Hamza Akbar: 0308-8616996 House No#531A-5 O/S Dehli Gate MultanDocument3 pagesHamza Akbar: 0308-8616996 House No#531A-5 O/S Dehli Gate MultanTalalNo ratings yet
- Alliance For ProgressDocument19 pagesAlliance For ProgressDorian EusseNo ratings yet
- MGN815: Business Models: Ajay ChandelDocument38 pagesMGN815: Business Models: Ajay ChandelSam RehmanNo ratings yet
- LADP HPDocument11 pagesLADP HPrupeshsoodNo ratings yet
- Alexander Fraser TytlerDocument4 pagesAlexander Fraser Tytlersbr9guyNo ratings yet
- Mywizard For AIOps - Virtual Agent (ChatBOT)Document27 pagesMywizard For AIOps - Virtual Agent (ChatBOT)Darío Aguirre SánchezNo ratings yet
- Encephalopathies: Zerlyn T. Leonardo, M.D., FPCP, FPNADocument50 pagesEncephalopathies: Zerlyn T. Leonardo, M.D., FPCP, FPNAJanellee DarucaNo ratings yet
- Vishakha BroadbandDocument6 pagesVishakha Broadbandvishakha sonawaneNo ratings yet
- Paper 11-ICOSubmittedDocument10 pagesPaper 11-ICOSubmittedNhat Tan MaiNo ratings yet
- The Life Cycle of Brent FieldDocument21 pagesThe Life Cycle of Brent FieldMalayan AjumovicNo ratings yet
- Annual Report 2022 2Document48 pagesAnnual Report 2022 2Dejan ReljinNo ratings yet
- Kaibigan, Kabarkada, Kaeskwela: Pinoy Friendships and School LifeDocument47 pagesKaibigan, Kabarkada, Kaeskwela: Pinoy Friendships and School LifeGerald M. LlanesNo ratings yet