You might also like
- Ability Can Could Pages 1Document1 pageAbility Can Could Pages 1runnermnNo ratings yet
- Unit Test 4BDocument2 pagesUnit Test 4BrunnermnNo ratings yet
- How To Uncover Job Opportunities: Understand Your Target RoleDocument1 pageHow To Uncover Job Opportunities: Understand Your Target RolerunnermnNo ratings yet
- Notes Pages 2Document1 pageNotes Pages 2runnermnNo ratings yet
- Homework:: They Align With The Requirements For Your Target Role, You're Ready To Move Your Job Search ForwardDocument1 pageHomework:: They Align With The Requirements For Your Target Role, You're Ready To Move Your Job Search ForwardrunnermnNo ratings yet
- RM C1 Video Worksheets ContentsDocument1 pageRM C1 Video Worksheets ContentsrunnermnNo ratings yet
- The Roadmap Report: Unit 2: The Return of The Milkman Corresponds With Lesson 2ADocument2 pagesThe Roadmap Report: Unit 2: The Return of The Milkman Corresponds With Lesson 2ArunnermnNo ratings yet
- Unit Test 1ADocument2 pagesUnit Test 1Arunnermn100% (1)
- Unit Test 7BDocument2 pagesUnit Test 7BrunnermnNo ratings yet
- The Roadmap Report Teacher's Notes: Unit 1: Social Screen Time Corresponds With Lessons 1A& 1BDocument20 pagesThe Roadmap Report Teacher's Notes: Unit 1: Social Screen Time Corresponds With Lessons 1A& 1BrunnermnNo ratings yet
- Employment Law: Religious Discrimination and Racial Harassment: What Ever Happened To Marshawn Demur?Document12 pagesEmployment Law: Religious Discrimination and Racial Harassment: What Ever Happened To Marshawn Demur?runnermnNo ratings yet
- Task 1. Continuous AspectDocument1 pageTask 1. Continuous AspectrunnermnNo ratings yet
- Applying Agile Learning To Teaching English For Specific PurposesDocument22 pagesApplying Agile Learning To Teaching English For Specific PurposesrunnermnNo ratings yet
- Oxford Practice Grammar Advanced Tests Pages 5 6Document2 pagesOxford Practice Grammar Advanced Tests Pages 5 6runnermnNo ratings yet
- Acculturation TasksDocument2 pagesAcculturation TasksrunnermnNo ratings yet
- Medication Generic/Brand Classification Nursing Implications (3) Dosage Route Schedule /time Desired Effect Side Effects (3) TeachingDocument5 pagesMedication Generic/Brand Classification Nursing Implications (3) Dosage Route Schedule /time Desired Effect Side Effects (3) TeachingrunnermnNo ratings yet
- Phrasal Verbs - EnglishDocument4 pagesPhrasal Verbs - EnglishrunnermnNo ratings yet
- 5 Practical PYP TipsDocument1 page5 Practical PYP TipsrunnermnNo ratings yet
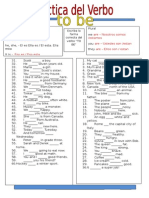
- VerbtobeDocument1 pageVerbtoberunnermnNo ratings yet
- Key Ideas: Factors That Affect Language Learning - MotivationDocument2 pagesKey Ideas: Factors That Affect Language Learning - MotivationrunnermnNo ratings yet
- Singular Plural Escriba La Forma Correcta Del Verbo "To Be": Luis LedesmaDocument1 pageSingular Plural Escriba La Forma Correcta Del Verbo "To Be": Luis LedesmarunnermnNo ratings yet
- Can and Can't: Things You Can Do and Eight Things You Can't Do. Examples: Ride A BicycleDocument1 pageCan and Can't: Things You Can Do and Eight Things You Can't Do. Examples: Ride A BicyclerunnermnNo ratings yet
- School Nurse Schedule Spring 2015: Renee Mathews 641-751-1156 Susan Gallo 641-236-2750 Gloria Dielschneider 641-366-2810Document1 pageSchool Nurse Schedule Spring 2015: Renee Mathews 641-751-1156 Susan Gallo 641-236-2750 Gloria Dielschneider 641-366-2810runnermnNo ratings yet
- A Nurse Educator Is Reviewing With A Group of Nursing Students The Actions and Thought ProcessesDocument4 pagesA Nurse Educator Is Reviewing With A Group of Nursing Students The Actions and Thought ProcessesrunnermnNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (588)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5795)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (895)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (345)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (400)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (74)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (266)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2259)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1091)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (121)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Emergency Medicine EbookDocument642 pagesEmergency Medicine Ebookgulsoomro100% (1)
- Lopez 2021Document9 pagesLopez 2021toaldoNo ratings yet
- Iron Deficiency Anemia Fact SheetDocument2 pagesIron Deficiency Anemia Fact SheetCandace MorinNo ratings yet
- Nursing InformaticsDocument5 pagesNursing InformaticsDanica BonNo ratings yet
- CorticosteroidsDocument8 pagesCorticosteroidsAkuMrW100% (1)
- Nes Mental Pharmacy - FinalDocument271 pagesNes Mental Pharmacy - FinalJ Carlos ChambiNo ratings yet
- Lab YogurtDocument6 pagesLab YogurtSikin Sikin0% (1)
- Tooth DecayDocument28 pagesTooth DecayRyan Carlo CondeNo ratings yet
- Nursing Care PlanDocument4 pagesNursing Care Planjopearl1889% (9)
- Polymyalgia RheumaticaDocument19 pagesPolymyalgia Rheumaticaapi-676787384No ratings yet
- Cast Metal RestorationDocument48 pagesCast Metal RestorationRosa Faraon EspeñaNo ratings yet
- 10 D125 Document Compliance Matrix 2020Document7 pages10 D125 Document Compliance Matrix 2020Chetan PrakashNo ratings yet
- Paper PresentationDocument7 pagesPaper PresentationDuan GonmeiNo ratings yet
- Formularium 2014 - RS. Elisabeth PwkertoDocument53 pagesFormularium 2014 - RS. Elisabeth PwkertoayuNo ratings yet
- Operating Room & Surgical CaseDocument7 pagesOperating Room & Surgical CaseHappy DealNo ratings yet
- Solid Waste Management Presentation - Asnani - July 19, 2016Document22 pagesSolid Waste Management Presentation - Asnani - July 19, 2016Saga Gold Saint100% (1)
- August 5, 2016 Strathmore TimesDocument24 pagesAugust 5, 2016 Strathmore TimesStrathmore TimesNo ratings yet
- 10th 1001126 - B1 QP English CommuDocument12 pages10th 1001126 - B1 QP English CommuvidyapostNo ratings yet
- Wicksall: ExperienceDocument2 pagesWicksall: Experienceapi-451678594No ratings yet
- Sports DrinksDocument2 pagesSports DrinksMustofaNo ratings yet
- Suspected Adverse Drug Reaction Reporting Form: CdscoDocument2 pagesSuspected Adverse Drug Reaction Reporting Form: CdscoNaveen Kumar G TNo ratings yet
- Into To Balance Method ImagingDocument8 pagesInto To Balance Method ImagingSkorman7No ratings yet
- Water Quality and Irrigation Water StandardsDocument31 pagesWater Quality and Irrigation Water StandardsThe TruthNo ratings yet
- Toxicology: WEEK 6-8Document29 pagesToxicology: WEEK 6-8Cariza Anda0% (1)
- 1 s2.0 S014067362300569X MainDocument11 pages1 s2.0 S014067362300569X MainAldo Amed Montaño SalinasNo ratings yet
- Minorities in PT SchoolDocument12 pagesMinorities in PT SchoolMichael MakherNo ratings yet
- AK Lab Manual For Fwinter 2019Document192 pagesAK Lab Manual For Fwinter 2019luckyNo ratings yet
- Sodium Lignosulfonate MSDS: Section 1: Chemical Product and Company IdentificationDocument5 pagesSodium Lignosulfonate MSDS: Section 1: Chemical Product and Company IdentificationYasdiOKNo ratings yet
- Ok Ok Notes PediaDocument14 pagesOk Ok Notes PediaChristian PasicolanNo ratings yet
- A Guide To Valplast DenturesDocument2 pagesA Guide To Valplast DenturesAdelia Putri Kharisma DewiNo ratings yet