You might also like
- Drug Recipes IndexDocument72 pagesDrug Recipes IndexEka Kusyanto50% (4)
- Pharmacology 3 - Management of Heart FailureDocument59 pagesPharmacology 3 - Management of Heart Failurealbatros000No ratings yet
- Drugs For Congestive Heart FailureDocument46 pagesDrugs For Congestive Heart Failuresultan khabeeb100% (1)
- Vasoconstrictors & VasodilatorsDocument37 pagesVasoconstrictors & VasodilatorsDrVarun Menon100% (1)
- Vasodilators by Hiren PatelDocument28 pagesVasodilators by Hiren PatelHiren_Patel_2427No ratings yet
- 1 Drugs For HypertensionDocument62 pages1 Drugs For HypertensionSaniNo ratings yet
- Hepatorenal Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsFrom EverandHepatorenal Syndrome, A Simple Guide To The Condition, Diagnosis, Treatment And Related ConditionsNo ratings yet
- Preps 4-61Document57 pagesPreps 4-61fianaNo ratings yet
- ObjectionableDocument9 pagesObjectionabledmtalbhogeNo ratings yet
- Business Plan To Start An Online Pharmacy BusinessDocument32 pagesBusiness Plan To Start An Online Pharmacy BusinessDiriba Alemu100% (1)
- Antihypertensive DrugsDocument37 pagesAntihypertensive Drugsleiann_jessicaNo ratings yet
- Capital Budgeting Hetero DrugsDocument100 pagesCapital Budgeting Hetero DrugsDasari Anilkumar100% (1)
- Vasodilators 1233318450814478 3Document29 pagesVasodilators 1233318450814478 3Nehal AmjadNo ratings yet
- Friabilator Operation Cleaning Handling Standard Operating ProcedureDocument8 pagesFriabilator Operation Cleaning Handling Standard Operating ProcedureKumar Galipelly100% (1)
- Foreign Body EarDocument34 pagesForeign Body EarGabriella ChafrinaNo ratings yet
- 8D - HypertensionDocument58 pages8D - Hypertensionmashe1No ratings yet
- Cardiotronic MedicationsDocument13 pagesCardiotronic MedicationsTee WoodNo ratings yet
- Calcium Channel Blockers: Mechanisms, Types, Uses & Side EffectsDocument6 pagesCalcium Channel Blockers: Mechanisms, Types, Uses & Side EffectsManyal Kutin KoakNo ratings yet
- Managing Hypertension with Drug TherapyDocument39 pagesManaging Hypertension with Drug TherapykiranstNo ratings yet
- Cardiovascular PharmacologyDocument61 pagesCardiovascular PharmacologyTeeOne920% (1)
- Thiazide and Thiazide-Like DiureticsDocument3 pagesThiazide and Thiazide-Like DiureticsYohanes SutrisnoNo ratings yet
- Cardiovascular System Pharmacology: Pharmacology Ii DR E KeziaDocument15 pagesCardiovascular System Pharmacology: Pharmacology Ii DR E KeziaJohnNo ratings yet
- Emergency Cardiac Medications for ArrhythmiasDocument14 pagesEmergency Cardiac Medications for ArrhythmiasRomzy BasañesNo ratings yet
- Anti Hypertensive 20191211Document35 pagesAnti Hypertensive 20191211helloitsmenadNo ratings yet
- Cardiac ArrhythmiaDocument101 pagesCardiac ArrhythmiaYuvraj ChauhanNo ratings yet
- عرض تقديمي2Document18 pagesعرض تقديمي2Sabrina ShalhoutNo ratings yet
- HTN EmergencyDocument11 pagesHTN EmergencyKaran ChhabraNo ratings yet
- Antihypertensive AgentsDocument52 pagesAntihypertensive Agentssameena ramzanNo ratings yet
- Heat Failure DrugsDocument8 pagesHeat Failure DrugsDaniel MwiluNo ratings yet
- Skema HipertensiDocument4 pagesSkema HipertensiAndri wijayaNo ratings yet
- Cardiotonic DrugsDocument67 pagesCardiotonic DrugsLady Mae Ramos100% (1)
- Hypertensive Emergencies: BY: Dr. Imtiyaz Hashim (PGR) Dr. Khalida Baloch (Ho)Document31 pagesHypertensive Emergencies: BY: Dr. Imtiyaz Hashim (PGR) Dr. Khalida Baloch (Ho)امتیاز ہاشم بزنجوNo ratings yet
- CVS PharmacologyDocument60 pagesCVS PharmacologyGølà Sèèñàà–baale irraaNo ratings yet
- 1 Antihypertensive DrugsDocument14 pages1 Antihypertensive DrugsReda SoNo ratings yet
- 2nd - Semester.lecture 3.1-Drugs Used in HypertensionDocument40 pages2nd - Semester.lecture 3.1-Drugs Used in HypertensionToader SilviaNo ratings yet
- Obat Yang Bekerja Pada Sistem KardiovaskulerDocument18 pagesObat Yang Bekerja Pada Sistem KardiovaskulerMuhammad IkbalNo ratings yet
- HCL Clonipress: 75 MCG & 150 MCG TabletDocument1 pageHCL Clonipress: 75 MCG & 150 MCG TabletShyden Taghap Billones BordaNo ratings yet
- Emergency Drugs Review: Oxygen, Epinephrine, Atropine and MoreDocument71 pagesEmergency Drugs Review: Oxygen, Epinephrine, Atropine and Moredodong skyroseNo ratings yet
- Anti HypertensionDocument62 pagesAnti HypertensionHazazi Jr Love LoverpoolNo ratings yet
- Journal 3 Diuretic in Heart FailureDocument6 pagesJournal 3 Diuretic in Heart FailureClara Nur RamadhaniNo ratings yet
- 10-11 Treatment of HypertensionDocument11 pages10-11 Treatment of HypertensionHanif GandohNo ratings yet
- Pharm CH 11 AntihypertensivesDocument42 pagesPharm CH 11 AntihypertensivesDaniel AdamsNo ratings yet
- FARMAKOGNOSI - Obat AntihipertensiDocument7 pagesFARMAKOGNOSI - Obat AntihipertensiTrianisa FebyNo ratings yet
- Antihypertensive Drugs ٠١١٦٥٨Document10 pagesAntihypertensive Drugs ٠١١٦٥٨mohnad806mNo ratings yet
- Bihs PDFDocument4 pagesBihs PDFFredrikus Lay Berkh MansNo ratings yet
- Review of Advancements in Heart Failure 81220Document65 pagesReview of Advancements in Heart Failure 81220Dr MustafaNo ratings yet
- Antihypertension: Prajogo WibowoDocument45 pagesAntihypertension: Prajogo WibowoDesti Ratna PutriNo ratings yet
- NCP and DSDocument6 pagesNCP and DSfranzcatchie100% (1)
- Heart Failure and DHF PDFDocument31 pagesHeart Failure and DHF PDFMahamed Wefkey OmranNo ratings yet
- Ecart For PrintingDocument10 pagesEcart For PrintingbluennaNo ratings yet
- Anti Hypertensive Drugs .Document6 pagesAnti Hypertensive Drugs .Baqir BroNo ratings yet
- Spironolactone: Generic Name Brand Name ClassificationDocument5 pagesSpironolactone: Generic Name Brand Name ClassificationShermalyn SalahuddinNo ratings yet
- Prepared By: Shukri Yusuf ElmiDocument17 pagesPrepared By: Shukri Yusuf ElmiabdishakurNo ratings yet
- Heart Failure Managing HF Related Peripheral Oedema in Primary CareDocument1 pageHeart Failure Managing HF Related Peripheral Oedema in Primary CareParth VinaypatilNo ratings yet
- Drugs Affecting The Cardiovascular System (Antihypertensive - Part-1)Document6 pagesDrugs Affecting The Cardiovascular System (Antihypertensive - Part-1)alialahmedy24No ratings yet
- PEDRIATICDocument17 pagesPEDRIATICMaxxdlc 16No ratings yet
- Faculty of Physical TherapyDocument15 pagesFaculty of Physical TherapyDr Abdallah BahaaNo ratings yet
- Congestive Heart FailureDocument25 pagesCongestive Heart Failureemman122392No ratings yet
- Diuretics in The Treatment of Hypertension: Michael E. Ernst, Pharmd, and Samuel J. Mann, MDDocument8 pagesDiuretics in The Treatment of Hypertension: Michael E. Ernst, Pharmd, and Samuel J. Mann, MDWawan NNo ratings yet
- 7,8 - Antihypertensive DrugsDocument10 pages7,8 - Antihypertensive DrugsHusniya MehamedNo ratings yet
- Generic NameDocument8 pagesGeneric NameRosaree Mae PantojaNo ratings yet
- LECTURE 8 AntihypertensiveDocument18 pagesLECTURE 8 AntihypertensiveanaNo ratings yet
- PharmaDocument8 pagesPharma2022105340No ratings yet
- Lecture 24-25 - Antihypertensive AgentsDocument30 pagesLecture 24-25 - Antihypertensive AgentsJedoNo ratings yet
- Heart Failure: Causes, Treatments, and Dental ImplicationsDocument8 pagesHeart Failure: Causes, Treatments, and Dental Implicationsمحمد علي حميدNo ratings yet
- Pathogenesis of LeprosyDocument13 pagesPathogenesis of LeprosyNurul AinNo ratings yet
- Soal Mde Tropmed 2007Document4 pagesSoal Mde Tropmed 2007Gabriella ChafrinaNo ratings yet
- Cvs4-Clinical Aspects of Serum Cholesterol LevelDocument2 pagesCvs4-Clinical Aspects of Serum Cholesterol LevelGabriella ChafrinaNo ratings yet
- ECG Arrhythmia GraphsDocument3 pagesECG Arrhythmia GraphsGabriella ChafrinaNo ratings yet
- Rs6 Extrapulmonary TuberculosisDocument4 pagesRs6 Extrapulmonary TuberculosisGabriella ChafrinaNo ratings yet
- RS7 InfluenzaDocument6 pagesRS7 InfluenzaGabriella ChafrinaNo ratings yet
- TM3-Diagnosis and DD of MalariaDocument3 pagesTM3-Diagnosis and DD of MalariaGabriella ChafrinaNo ratings yet
- Rs6-Cervical Lymph NodeDocument6 pagesRs6-Cervical Lymph NodeGabriella ChafrinaNo ratings yet
- Lab PharmacologyDocument2 pagesLab PharmacologyGabriella ChafrinaNo ratings yet
- Rs6 Pleural TuberculosisDocument5 pagesRs6 Pleural TuberculosisGabriella ChafrinaNo ratings yet
- RS7-Acid Base BalanceDocument4 pagesRS7-Acid Base BalanceGabriella ChafrinaNo ratings yet
- RS5 PiDocument9 pagesRS5 PiGabriella ChafrinaNo ratings yet
- Rs4-Gas Exchange and TransportDocument5 pagesRs4-Gas Exchange and TransportGabriella ChafrinaNo ratings yet
- Rs4 Phop CRPDocument2 pagesRs4 Phop CRPGabriella ChafrinaNo ratings yet
- RS3 PiDocument5 pagesRS3 PiGabriella ChafrinaNo ratings yet
- Iccu (Tachycardia) : - Tutorial D-1 CVSDocument2 pagesIccu (Tachycardia) : - Tutorial D-1 CVSGabriella ChafrinaNo ratings yet
- RS5-Defense Mech of LungDocument3 pagesRS5-Defense Mech of LungGabriella ChafrinaNo ratings yet
- Macroscopic Hematuria GuideDocument3 pagesMacroscopic Hematuria GuideGabriella ChafrinaNo ratings yet
- RS1 ManagementDocument3 pagesRS1 ManagementGabriella ChafrinaNo ratings yet
- Group A Β-Hemolytic Streptococcus: - Tutorial B-1 RSDocument2 pagesGroup A Β-Hemolytic Streptococcus: - Tutorial B-1 RSGabriella ChafrinaNo ratings yet
- Iccu (Tachycardia) : - Tutorial D-1 CVSDocument2 pagesIccu (Tachycardia) : - Tutorial D-1 CVSGabriella ChafrinaNo ratings yet
- CVS5-Conduction of Cardiac Action PotentialsDocument1 pageCVS5-Conduction of Cardiac Action PotentialsGabriella ChafrinaNo ratings yet
- Lab PharmacologyDocument2 pagesLab PharmacologyGabriella ChafrinaNo ratings yet
- Deep Vein Thrombosis (DVT) : - Tutorial D-1 CVSDocument1 pageDeep Vein Thrombosis (DVT) : - Tutorial D-1 CVSGabriella ChafrinaNo ratings yet
- CVS6 Heart SoundsDocument3 pagesCVS6 Heart SoundsGabriella ChafrinaNo ratings yet
- CVS6 Page InterpretationDocument2 pagesCVS6 Page InterpretationGabriella ChafrinaNo ratings yet
- Advanced Life Support Algorithm GuideDocument1 pageAdvanced Life Support Algorithm GuideGabriella ChafrinaNo ratings yet
- Advance Life Support (American Heart Association 2010) : - Tutorial D-1 CVSDocument1 pageAdvance Life Support (American Heart Association 2010) : - Tutorial D-1 CVSGabriella ChafrinaNo ratings yet
- List of high alert medications at Husada HospitalDocument5 pagesList of high alert medications at Husada HospitalCHRISTINE EriskaNo ratings yet
- Antibiotics in OMFSDocument20 pagesAntibiotics in OMFSAmit GaurNo ratings yet
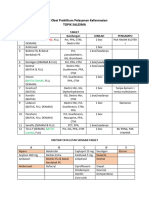
- Daftar Obat Praktikum Pelayanan Kefarmasian OretDocument4 pagesDaftar Obat Praktikum Pelayanan Kefarmasian OretRiza AsariNo ratings yet
- 5.1.4. Microbiological Quality of Non-Sterile Pharmaceutical Preparations and Substances For Pharmaceutical UseDocument1 page5.1.4. Microbiological Quality of Non-Sterile Pharmaceutical Preparations and Substances For Pharmaceutical UseCik ApaiNo ratings yet
- Medicine List by AmirDocument39 pagesMedicine List by AmirNomAn JuTtNo ratings yet
- Diabetic Foot Infections: by Scott Bergman, Pharm.D., BCPS-AQ ID and Punit J. Shah, Pharm.D., BCPSDocument20 pagesDiabetic Foot Infections: by Scott Bergman, Pharm.D., BCPS-AQ ID and Punit J. Shah, Pharm.D., BCPSPrashant LokhandeNo ratings yet
- Harga Prolanis (Data Dari Apotek Online)Document74 pagesHarga Prolanis (Data Dari Apotek Online)Orin Tri WulanNo ratings yet
- Tablet and CapsulesDocument101 pagesTablet and CapsulesTamer HassanNo ratings yet
- Cipla General Overview & SWOT AnalysisDocument5 pagesCipla General Overview & SWOT Analysisakanksha morghadeNo ratings yet
- AN ALTERNATIVE TO CODEINE AND HYDROCODONE - Management of Persistent CoughDocument2 pagesAN ALTERNATIVE TO CODEINE AND HYDROCODONE - Management of Persistent CoughAnna LiachenkoNo ratings yet
- NemeraDocument5 pagesNemeraFransisca FortunataNo ratings yet
- Hilton - Maher - SeltoDocument21 pagesHilton - Maher - Seltoareep94No ratings yet
- IT 10 - Farmakologi Obat - Obat Di Bidang Endokrin - TEODocument34 pagesIT 10 - Farmakologi Obat - Obat Di Bidang Endokrin - TEOtattosssNo ratings yet
- CephalexinDocument4 pagesCephalexinCHIEF DOCTOR MUTHUNo ratings yet
- Maharashtra Board Pharmacology Model AnswerDocument19 pagesMaharashtra Board Pharmacology Model AnswerJyoti MangtaniNo ratings yet
- 16 10 25 Decarboxylation of THCA To Active THC PDFDocument3 pages16 10 25 Decarboxylation of THCA To Active THC PDFRafael Ignacio Leal QuijónNo ratings yet
- Alims - Approved Terminology - Routes and Methods of Administration - October 2014Document2 pagesAlims - Approved Terminology - Routes and Methods of Administration - October 2014Katarina R.M.No ratings yet
- Chapter 1. Intro To DrugsDocument10 pagesChapter 1. Intro To DrugsLyka Milo AvilaNo ratings yet
- Jujube FruitDocument5 pagesJujube FruitnasmiNo ratings yet
- Gina Shenoda, BS, MBADocument3 pagesGina Shenoda, BS, MBACristian RamirezNo ratings yet
- Brain O MaticDocument5 pagesBrain O MaticshemoomiNo ratings yet
- Lozenges Troches Sticks and SuppositoriesDocument21 pagesLozenges Troches Sticks and SuppositoriesABC.DEFNo ratings yet
- Clinical Pharmacology and Clinical PharmacyDocument8 pagesClinical Pharmacology and Clinical PharmacyRowena Concepcion Penafiel100% (1)
- Phytochemical and Antibacterial Studies On Peperomia Pellucida (L.) H.B.KDocument3 pagesPhytochemical and Antibacterial Studies On Peperomia Pellucida (L.) H.B.KSonia Virgawati PratiwiNo ratings yet