You might also like
- Psychiatric Assessment ToolDocument53 pagesPsychiatric Assessment ToolLori100% (4)
- Lecture Notes On PsychiatryDocument38 pagesLecture Notes On PsychiatryMing Wang50% (6)
- Hypnotherapy Scripts 6 Steve G Jones Ebook PDFDocument66 pagesHypnotherapy Scripts 6 Steve G Jones Ebook PDFjohannes2212100% (10)
- Physical Changes With AgingDocument8 pagesPhysical Changes With Agingjanna mae patriarcaNo ratings yet
- AO 56 S 1989 LTODocument13 pagesAO 56 S 1989 LTOmikan2No ratings yet
- NSP2 PDFDocument92 pagesNSP2 PDFIrene C. CruzNo ratings yet
- Administrative Order No 56 S 1989Document7 pagesAdministrative Order No 56 S 1989Anne Marion Perez67% (3)
- Generic DispensingDocument30 pagesGeneric Dispensingshervintancruzado83% (6)
- Medication ProfileDocument1 pageMedication ProfileKlendle Leigh Revocal100% (1)
- Unit 1. Clinical PharmacyDocument5 pagesUnit 1. Clinical PharmacyAashish BhattaraiNo ratings yet
- Dispensing Lecture Reviewer - MidtermDocument26 pagesDispensing Lecture Reviewer - Midtermapi-306968266No ratings yet
- Hospital FormularyDocument27 pagesHospital FormularyMarvin BernalesNo ratings yet
- Aiims Hospital Disaster PlanDocument6 pagesAiims Hospital Disaster PlanSujatha J JayabalNo ratings yet
- Four Humors Theory in Unani MedicineDocument4 pagesFour Humors Theory in Unani MedicineJoko RinantoNo ratings yet
- TR-Pharmacy Services NC IIIDocument135 pagesTR-Pharmacy Services NC IIIAljon Fortaleza Balanag100% (2)
- Community Pharmacy Internship Reflection PaperDocument2 pagesCommunity Pharmacy Internship Reflection PaperPeter Paul Recabo100% (2)
- Páginas Desdepharmacotherapy Casebook 10th Ed.Document61 pagesPáginas Desdepharmacotherapy Casebook 10th Ed.Glo VsNo ratings yet
- Standard Patient Counseling ScriptDocument22 pagesStandard Patient Counseling ScriptElleason Joshua G. FranciscoNo ratings yet
- Philippine Practice Standards For PharmacistsDocument8 pagesPhilippine Practice Standards For PharmacistsAgatha Rose100% (1)
- Storage of Dosage FormsDocument20 pagesStorage of Dosage FormsMeredith Kerr50% (2)
- Ao 55 1988Document10 pagesAo 55 1988Ella Riva100% (2)
- Briefer On RA 10918Document3 pagesBriefer On RA 10918Eugene UC100% (1)
- Philippine Pharmacists Advocacy Programs PDFDocument4 pagesPhilippine Pharmacists Advocacy Programs PDFFaith Gabriel100% (1)
- Standard Operating Procedure Good Storage PracticeDocument2 pagesStandard Operating Procedure Good Storage PracticeDaniel Yves IV Paez100% (1)
- Jurisprudence and EthicsDocument22 pagesJurisprudence and EthicsRozamae Magnanao100% (1)
- Dispensing and Medication CounselingDocument12 pagesDispensing and Medication CounselingLei100% (3)
- Hospital Pharmacy QA and Inventory ControlDocument9 pagesHospital Pharmacy QA and Inventory ControlChristian Rey Abuan80% (10)
- Hospital Information Management System - Cover PageDocument15 pagesHospital Information Management System - Cover Pageapi-1946401583% (6)
- Organization of NICU ServicesDocument45 pagesOrganization of NICU ServicesMonika Bagchi84% (64)
- PALS Helpful Hints 2015 Guidelines Posted Nov 2016Document5 pagesPALS Helpful Hints 2015 Guidelines Posted Nov 2016Mj Teate100% (1)
- Asthma - Case PresentationDocument56 pagesAsthma - Case Presentationsarooah199467% (6)
- Pharmaceutical Jurisprudence - Ethics Answer Key-RED PACOPDocument20 pagesPharmaceutical Jurisprudence - Ethics Answer Key-RED PACOPArk Olfato ParojinogNo ratings yet
- The Philippine Pharmacy Act: RA 10918 Submitted By: Emerald Shaine P. SamozaDocument49 pagesThe Philippine Pharmacy Act: RA 10918 Submitted By: Emerald Shaine P. Samozaemerald shaine samozaNo ratings yet
- Dr. Nelson T. TubonDocument29 pagesDr. Nelson T. TubonBS50% (2)
- (BLUE PACOP) Pharmaceutical Jurisprudence & EthicsDocument31 pages(BLUE PACOP) Pharmaceutical Jurisprudence & EthicsDenise Yanci Demiar100% (1)
- CentralVenousCatheters PDFDocument77 pagesCentralVenousCatheters PDFHarold De Leon Malang100% (1)
- Code of Ethics and PPhADocument12 pagesCode of Ethics and PPhARaymond Godfrey DagwasiNo ratings yet
- OutputDocument1 pageOutputmsenthamizharasaNo ratings yet
- BFAD GUIDELINES LABELING DRUG PRODUCTSDocument35 pagesBFAD GUIDELINES LABELING DRUG PRODUCTSDaya Mavi Tura Gabuyo100% (2)
- Basic Iv Fluid PDFDocument77 pagesBasic Iv Fluid PDFDesi AdiyatiNo ratings yet
- Associate Professor:Ivan Bonet. Obstetric and Gynecology Associate Professor:Ivan Bonet. Obstetric and GynecologyDocument31 pagesAssociate Professor:Ivan Bonet. Obstetric and Gynecology Associate Professor:Ivan Bonet. Obstetric and Gynecologyivan0% (1)
- Ra 9711-FDA Act of 2009Document34 pagesRa 9711-FDA Act of 2009Shehana Tawasil Musahari0% (1)
- Pharmaceutical Jurisprudence and Ethics ManualDocument51 pagesPharmaceutical Jurisprudence and Ethics ManualYap JackyNo ratings yet
- Damasco - Cpi - Activity No.9Document5 pagesDamasco - Cpi - Activity No.9LDCU - Damasco, Erge Iris M.No ratings yet
- Ra 10918Document23 pagesRa 10918Colleen Ariel SandovalNo ratings yet
- Space Management in Pediatric DentistryDocument37 pagesSpace Management in Pediatric DentistryAlshammary Freah100% (3)
- (Dispensing 1 Laboratory) Review NotesDocument12 pages(Dispensing 1 Laboratory) Review NotesZen HeartNo ratings yet
- Addition and DeletionDocument10 pagesAddition and DeletionNikkaMontilNo ratings yet
- Exam PrelimDocument4 pagesExam PrelimRochelle Anne Abad BandaNo ratings yet
- Ao 99 S 1990Document2 pagesAo 99 S 1990taengoo2180% (1)
- Tablet FriabilityDocument25 pagesTablet FriabilityJean Florencondia67% (3)
- Ethical Standards for Health Product PromotionDocument14 pagesEthical Standards for Health Product PromotionKitkat CasacopNo ratings yet
- Name: Eyah Ifeanyi Godfrey Score: Year Level: 3 Date: 12/7/2020Document14 pagesName: Eyah Ifeanyi Godfrey Score: Year Level: 3 Date: 12/7/2020Jeyma Dacumos100% (1)
- PX CDocument1 pagePX CMich TolentinoNo ratings yet
- Advocacy in PharmacyDocument3 pagesAdvocacy in PharmacyZofia RanadaNo ratings yet
- Nica Chua - Hospital Pharmacy Internship Daily Activity Report-Day 33 MajorDocument5 pagesNica Chua - Hospital Pharmacy Internship Daily Activity Report-Day 33 MajorMa Victoria ChuaNo ratings yet
- Dispensing CA NotesDocument16 pagesDispensing CA NotesJohn TecsonNo ratings yet
- Clinical Pharmacy Answer Key-PINK PACOPDocument29 pagesClinical Pharmacy Answer Key-PINK PACOPKaguraNo ratings yet
- INTERN-3 Community Pharmacy ProfileDocument34 pagesINTERN-3 Community Pharmacy ProfilejadeNo ratings yet
- Republic Act No 6675Document4 pagesRepublic Act No 6675JenilynM.ChuNo ratings yet
- Internship5 12Document7 pagesInternship5 12Jerel MarquezNo ratings yet
- Exercises 8-10 (By Dr. N. Tubon) PDFDocument25 pagesExercises 8-10 (By Dr. N. Tubon) PDFLoren100% (1)
- Iinternship 13Document35 pagesIinternship 13Darwin MangabatNo ratings yet
- PhenacetinDocument16 pagesPhenacetinJericSalcedoNo ratings yet
- Apply for FDA License to Operate (LTO) in the PhilippinesDocument3 pagesApply for FDA License to Operate (LTO) in the Philippinesarkina_sunshine0% (1)
- Ra 3720 - Safety and Purity of Foods, and CosmeticsDocument70 pagesRa 3720 - Safety and Purity of Foods, and CosmeticsShehana Tawasil MusahariNo ratings yet
- Case 2Document4 pagesCase 2Patrícia Martins25% (4)
- Bronchial AsthmaDocument3 pagesBronchial AsthmaSabrina Reyes0% (1)
- CasesDocument25 pagesCasesfatemaNo ratings yet
- Cases Resp - SystemDocument12 pagesCases Resp - SystemJerin XavierNo ratings yet
- By Nawal GaletDocument54 pagesBy Nawal GaletSoia NeriyaniNo ratings yet
- Osce PDFDocument18 pagesOsce PDFMahamed Wefkey OmranNo ratings yet
- NCM 112 Rle Case Analysis: Care of Client With Alterations in Oxygenation (ASTHMA)Document2 pagesNCM 112 Rle Case Analysis: Care of Client With Alterations in Oxygenation (ASTHMA)Joegie ArioNo ratings yet
- Pediatric Asthma TBL QuestionsDocument4 pagesPediatric Asthma TBL QuestionsVladimir BasurtoNo ratings yet
- JNC 8Document14 pagesJNC 8amiwahyuniNo ratings yet
- Hipertensi AND Kemoterapi PDFDocument11 pagesHipertensi AND Kemoterapi PDFHananun ZharfaNo ratings yet
- Ich Q3C (R4)Document25 pagesIch Q3C (R4)Ravishankar NagarajanNo ratings yet
- Click To Edit Master Subtitle StyleDocument4 pagesClick To Edit Master Subtitle StyleRobertoArandaNo ratings yet
- Internasional PDFDocument10 pagesInternasional PDFHananun ZharfaNo ratings yet
- Stifar Komplemen2013Document44 pagesStifar Komplemen2013Hananun ZharfaNo ratings yet
- 232 439 1 SMDocument10 pages232 439 1 SMHananun ZharfaNo ratings yet
- 14 13 1 PB PDFDocument9 pages14 13 1 PB PDFRizki PuspitasariNo ratings yet
- How to Get Scholarships for Studying AbroadDocument15 pagesHow to Get Scholarships for Studying AbroadHananun ZharfaNo ratings yet
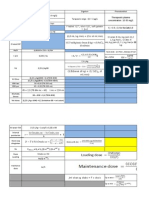
- Rumus Cp maks Cp min C toksik farmasiDocument4 pagesRumus Cp maks Cp min C toksik farmasiHananun ZharfaNo ratings yet
- Fast Dissolving Oral Films An Innovative DrugDocument8 pagesFast Dissolving Oral Films An Innovative DrugHananun ZharfaNo ratings yet
- How to Get Scholarships for Studying AbroadDocument15 pagesHow to Get Scholarships for Studying AbroadHananun ZharfaNo ratings yet
- Pembuatan Fase Gerak KKT: KarbohidratDocument4 pagesPembuatan Fase Gerak KKT: KarbohidratHananun ZharfaNo ratings yet
- Rumus Cp maks Cp min C toksik farmasiDocument4 pagesRumus Cp maks Cp min C toksik farmasiHananun ZharfaNo ratings yet
- GrafikDocument7 pagesGrafikHananun ZharfaNo ratings yet
- How to Get Scholarships for Studying AbroadDocument15 pagesHow to Get Scholarships for Studying AbroadHananun ZharfaNo ratings yet
- Analisis ParetoDocument1 pageAnalisis ParetoHananun ZharfaNo ratings yet
- Dept. of Pulmonology expertise in lung careDocument7 pagesDept. of Pulmonology expertise in lung carerohit6varma-4No ratings yet
- AtherosclerosisDocument7 pagesAtherosclerosisFaris Mufid Madyaputra100% (1)
- Emergency Contact ListDocument1 pageEmergency Contact ListthubanNo ratings yet
- Dental BS Delta 1500 PPO Benefit Summary 2018Document4 pagesDental BS Delta 1500 PPO Benefit Summary 2018deepchaitanyaNo ratings yet
- Major & Mild NCD Terminology UpdatesDocument30 pagesMajor & Mild NCD Terminology Updatesrachelle anne merallesNo ratings yet
- Health Apps - A ToolkitDocument3 pagesHealth Apps - A ToolkitAlexandra WykeNo ratings yet
- Cae Linking WordsDocument8 pagesCae Linking Wordsapi-19975062No ratings yet
- Assessment 7Document5 pagesAssessment 7api-525782290No ratings yet
- 4-5TH JANUARY 2023: Organized byDocument3 pages4-5TH JANUARY 2023: Organized byvivien kate perixNo ratings yet
- Nursing Diagnosis and Plan of Care for Anemia with Chronic DiseaseDocument6 pagesNursing Diagnosis and Plan of Care for Anemia with Chronic DiseaseChristine Joy FloresNo ratings yet
- Qip ProjectDocument13 pagesQip Projectapi-534216481No ratings yet
- Chapter 10Document45 pagesChapter 10Hannah BuquironNo ratings yet
- ATT Induced Hepatotoxicity: Dr. K. K. SharmaDocument36 pagesATT Induced Hepatotoxicity: Dr. K. K. SharmaSucharita Ray100% (1)
- Malnutrition in Critical Illness and Beyond A Narrative Review PDFDocument9 pagesMalnutrition in Critical Illness and Beyond A Narrative Review PDFEsteban DavidNo ratings yet
- F-I Drug HandbookDocument55 pagesF-I Drug HandbookGeanieveve ElnasNo ratings yet