You might also like
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Distillation ApparatusDocument2 pagesDistillation ApparatusStefani LarasatiNo ratings yet
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Laporan 1Document2 pagesLaporan 1Stefani LarasatiNo ratings yet
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- Supermarket CendawanDocument3 pagesSupermarket CendawanStefani LarasatiNo ratings yet
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (894)
- Molecules 18 09933 3Document16 pagesMolecules 18 09933 3Stefani LarasatiNo ratings yet
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Supermarket CendawanDocument3 pagesSupermarket CendawanStefani LarasatiNo ratings yet
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- Absen NeuroDocument6 pagesAbsen NeuroStefani LarasatiNo ratings yet
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- GWK / Uluwatu Pura??: (Jumpsuit Polkadot) (Tanktop Pink)Document1 pageGWK / Uluwatu Pura??: (Jumpsuit Polkadot) (Tanktop Pink)Stefani LarasatiNo ratings yet
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Molecules 18 09933 3Document16 pagesMolecules 18 09933 3Stefani LarasatiNo ratings yet
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
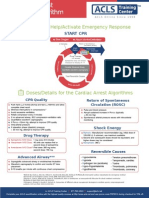
- Shout For Help/Activate Emergency Response: CPR StartDocument2 pagesShout For Help/Activate Emergency Response: CPR StartdavpierNo ratings yet
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- Confirm Booking Le Pirate Beach Club Gili Trawangan: Booking Reference NO:LPG1131Document1 pageConfirm Booking Le Pirate Beach Club Gili Trawangan: Booking Reference NO:LPG1131Stefani LarasatiNo ratings yet
- Dapus RKP Kitis 4Document1 pageDapus RKP Kitis 4Stefani LarasatiNo ratings yet
- Up Date in Head Injury ManagementDocument63 pagesUp Date in Head Injury ManagementStefani LarasatiNo ratings yet
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- Tamba HanDocument3 pagesTamba HanStefani LarasatiNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Journal Reading Tinea CapitisDocument22 pagesJournal Reading Tinea CapitisStefani LarasatiNo ratings yet
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Physical Paper +1ANNUALDocument5 pagesPhysical Paper +1ANNUALprabhnoorprimeNo ratings yet
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Bio SafetyDocument57 pagesBio SafetySatyaveer SinghNo ratings yet
- Congenital SyphilisDocument28 pagesCongenital SyphilisMeena Koushal100% (4)
- MNT For Sucrase Isomaltase DeficiencyDocument14 pagesMNT For Sucrase Isomaltase DeficiencySarah DresselNo ratings yet
- Ranula: A Review of LiteratureDocument6 pagesRanula: A Review of LiteratureNicco MarantsonNo ratings yet
- Urolithiasis PDFDocument4 pagesUrolithiasis PDFaaaNo ratings yet
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- 4446 16364 1 PBDocument8 pages4446 16364 1 PBSafira Rosyadatul AissyNo ratings yet
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- Zbornik Limes Vol 2Document354 pagesZbornik Limes Vol 2Morrigan100% (1)
- Nettle Rash Symptoms, Causes, TreatmentDocument2 pagesNettle Rash Symptoms, Causes, TreatmentArdave Laurente100% (1)
- Important Uses of Neem ExtractDocument3 pagesImportant Uses of Neem ExtractAbdurrahman MustaphaNo ratings yet
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Sas 1# - CHNDocument16 pagesSas 1# - CHNZymer Lee Perez AbasoloNo ratings yet
- Hydrocephalus IDocument52 pagesHydrocephalus IVlad Alexandra50% (2)
- Test-11 (Current Affair-2)Document86 pagesTest-11 (Current Affair-2)Pavansaikumar DasariNo ratings yet
- Angina Pectoris: Dr. Naitik D Trivedi & Dr. Upama N. TrivediDocument15 pagesAngina Pectoris: Dr. Naitik D Trivedi & Dr. Upama N. TrivediNaveen KumarNo ratings yet
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Pharmacology ReviewerDocument21 pagesPharmacology ReviewerCzairalene QuinzonNo ratings yet
- HSSC Paper PDF (8) - WatermarkDocument15 pagesHSSC Paper PDF (8) - WatermarkJitender TanwarNo ratings yet
- Epstein Barr VirusDocument13 pagesEpstein Barr VirusDianaLorenaNo ratings yet
- JUUL Labs, Inc. Class Action Complaint - January 30, 2019Document384 pagesJUUL Labs, Inc. Class Action Complaint - January 30, 2019Neil MakhijaNo ratings yet
- Vicente vs. Employees' Compensation CommissionDocument7 pagesVicente vs. Employees' Compensation CommissionAlexNo ratings yet
- BPJ Vol 9 No 2 P 827-828Document2 pagesBPJ Vol 9 No 2 P 827-828MayerNo ratings yet
- Daftar PustakaDocument3 pagesDaftar PustakaAlmira PutriNo ratings yet
- Envis Newsletter April 2014Document16 pagesEnvis Newsletter April 2014Mikel MillerNo ratings yet
- MeningitisDocument21 pagesMeningitisSonya GodwinNo ratings yet
- 5388 Tech ManualDocument198 pages5388 Tech ManualMichal SzymanskiNo ratings yet
- Progestin-Only Injectables: Characteristics and Health BenefitsDocument11 pagesProgestin-Only Injectables: Characteristics and Health BenefitsRazaria DailyneNo ratings yet
- Basics of DentistryDocument65 pagesBasics of DentistryHiba Shah100% (1)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- Information Bulletin A FMC Mbbs 2021Document27 pagesInformation Bulletin A FMC Mbbs 2021Bidyut Bikash BaruahNo ratings yet
- بنك طب نفسيDocument19 pagesبنك طب نفسيمحمد نادر100% (1)
- FCA (SA) Part I Past PapersDocument72 pagesFCA (SA) Part I Past PapersmatentenNo ratings yet
- Science Magazine, Issue 6657 (August 4, 2023)Document175 pagesScience Magazine, Issue 6657 (August 4, 2023)Kim LevrelNo ratings yet