You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Bill Beswick - Focused For Soccer - 2nd Edition-Human Kinetics (2010)Document216 pagesBill Beswick - Focused For Soccer - 2nd Edition-Human Kinetics (2010)juan alejandro perez quinteroNo ratings yet
- GOTTLIEB Buck - RogersDocument23 pagesGOTTLIEB Buck - Rogersvince benNo ratings yet
- Basic Clinical Massage Therapy eBookDocument3 pagesBasic Clinical Massage Therapy eBookDidik HariadiNo ratings yet
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- M1167 HMMWV Expanded Capacity TOW Missile CarrierDocument2 pagesM1167 HMMWV Expanded Capacity TOW Missile CarrierSergeant_2011100% (1)
- Tutorial1 EViews BasicsDocument20 pagesTutorial1 EViews BasicsDidik HariadiNo ratings yet
- Ajuste Valvulas Motor 336DDocument5 pagesAjuste Valvulas Motor 336Djuan sebastianNo ratings yet
- BB Head Coach Handbook 63-80 TeamsDocument18 pagesBB Head Coach Handbook 63-80 TeamsrichmondNo ratings yet
- Aprilia, BMW, Ducati and More Motorcycle SpecsDocument459 pagesAprilia, BMW, Ducati and More Motorcycle SpecsGiovaniBalzaniNo ratings yet
- Assembly Procedure VTC 254 TurbochargerDocument16 pagesAssembly Procedure VTC 254 TurbochargerMauricio MUÑOZ100% (1)
- Pe Worksheets 2Document136 pagesPe Worksheets 2api-471549637100% (6)
- The Soccer Eyeq Methodology: Section 1Document4 pagesThe Soccer Eyeq Methodology: Section 1Amin CherbitiNo ratings yet
- Extreme Sports - Exercises 0 PDFDocument2 pagesExtreme Sports - Exercises 0 PDFCarmen Herrera100% (1)
- NordicTrack C2400Document36 pagesNordicTrack C2400Guy ColvinNo ratings yet
- Odoo Functional Training v8 Pos PDFDocument9 pagesOdoo Functional Training v8 Pos PDFDidik HariadiNo ratings yet
- 694+ Illustrated Parts Catalog Revision 3.1 FROM SERIAL TRX01694CDGL11965Document549 pages694+ Illustrated Parts Catalog Revision 3.1 FROM SERIAL TRX01694CDGL11965Martín Lescano ParedesNo ratings yet
- Engargoladora de LatasDocument21 pagesEngargoladora de LatasAngel PerezNo ratings yet
- Istezanje Nakon SpavanjaDocument6 pagesIstezanje Nakon SpavanjaLaza UrosevicNo ratings yet
- Wrist and Forearm Stretches PDFDocument1 pageWrist and Forearm Stretches PDFDidik HariadiNo ratings yet
- Development of Complex Technologies For Processing of Rice BranDocument8 pagesDevelopment of Complex Technologies For Processing of Rice BranDidik HariadiNo ratings yet
- Gula Reduksi BekatulDocument6 pagesGula Reduksi BekatulDidik HariadiNo ratings yet
- 01 Introduction LabDocument27 pages01 Introduction LabChaItanya KrIshnaNo ratings yet
- Java Ee6 SlidesDocument14 pagesJava Ee6 SlidesDidik HariadiNo ratings yet
- Activation Under Serial Number (Educational License)Document4 pagesActivation Under Serial Number (Educational License)Didik HariadiNo ratings yet
- An R Programming Quick Reference: Basic Data RepresentationDocument13 pagesAn R Programming Quick Reference: Basic Data RepresentationDidik HariadiNo ratings yet
- Direct Product FormationDocument2 pagesDirect Product FormationDidik HariadiNo ratings yet
- Step by Step Guideline For Building Running Hello World Hibernate ApplicationDocument22 pagesStep by Step Guideline For Building Running Hello World Hibernate ApplicationmaripositaxNo ratings yet
- Beginning Java Ee 6 HolDocument29 pagesBeginning Java Ee 6 HolDidik HariadiNo ratings yet
- Java Ee6 SlidesDocument14 pagesJava Ee6 SlidesDidik HariadiNo ratings yet
- Litecalc4D UKDocument94 pagesLitecalc4D UKDidik HariadiNo ratings yet
- Manufacturing WorkflowDocument1 pageManufacturing WorkflowDidik HariadiNo ratings yet
- Keynote - Odoo Strategy 2015Document37 pagesKeynote - Odoo Strategy 2015Didik HariadiNo ratings yet
- Beginning Java Ee 6 HolDocument29 pagesBeginning Java Ee 6 HolDidik HariadiNo ratings yet
- Calico PDFDocument6 pagesCalico PDFDidik HariadiNo ratings yet
- Think CSpyDocument288 pagesThink CSpyapi-3713317No ratings yet
- OdoodevbasicDocument42 pagesOdoodevbasicDidik HariadiNo ratings yet
- Understanding The TurboFLOORPLAN CatalogDocument3 pagesUnderstanding The TurboFLOORPLAN CatalogDidik HariadiNo ratings yet
- Hands OnPythonTutorialDocument191 pagesHands OnPythonTutorialtdysarz100% (1)
- Infor SunSystems For Oil and Gas BrochureDocument4 pagesInfor SunSystems For Oil and Gas BrochureDidik HariadiNo ratings yet
- Openerp Sales Strategy: How To Sell Openerp !Document31 pagesOpenerp Sales Strategy: How To Sell Openerp !Didik HariadiNo ratings yet
- Infor FMS SunSystemsDocument4 pagesInfor FMS SunSystemsDidik HariadiNo ratings yet
- Process Mapping in Successful ERP Implementations: Michael D. Okrent and Robert J. VokurkaDocument7 pagesProcess Mapping in Successful ERP Implementations: Michael D. Okrent and Robert J. VokurkaDidik HariadiNo ratings yet
- Common Irregular Verb ListDocument4 pagesCommon Irregular Verb Listapi-27488371100% (1)
- GV26 Acupuncture Emergency PointDocument4 pagesGV26 Acupuncture Emergency PointJosé Mário100% (1)
- ROADMDocument21 pagesROADMDereje SeyoumNo ratings yet
- To English 2223Document8 pagesTo English 2223andrians13No ratings yet
- Spice Girls 15th Anniversary SpecialDocument4 pagesSpice Girls 15th Anniversary SpecialjoanluckyNo ratings yet
- 3024C Crankshaft - InstallDocument2 pages3024C Crankshaft - Installmiguel_catNo ratings yet
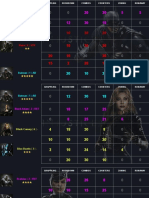
- Injustice 2 character stats and buildsDocument11 pagesInjustice 2 character stats and buildsMatija KneževićNo ratings yet
- Lesson 3:: Safety Protocol To Avoid Emergencies During An ExerciseDocument3 pagesLesson 3:: Safety Protocol To Avoid Emergencies During An ExerciseJerwin SamsonNo ratings yet
- Manual de Partes Dominar 400Document82 pagesManual de Partes Dominar 400Cesar Yriarte CastilloNo ratings yet
- Lastexception 63733199203Document19 pagesLastexception 63733199203The GadiatorNo ratings yet
- Kbox4 Performance GlobalDocument2 pagesKbox4 Performance Globalchrysomall_georgNo ratings yet
- Fostech Product Catalog 2017Document24 pagesFostech Product Catalog 2017KenshironokenNo ratings yet
- catcrochets.com-Moomin PatternDocument5 pagescatcrochets.com-Moomin PatternDebra EdelmannNo ratings yet
- Tong-Its - Wikipedia, The Free EncyclopediaDocument3 pagesTong-Its - Wikipedia, The Free EncyclopediaAnsel SotnasNo ratings yet
- Lesson Plan GonzaloDocument2 pagesLesson Plan Gonzaloapi-252176454No ratings yet
- English Week ActivitiesDocument1 pageEnglish Week ActivitiesNur Afizah SulaimanNo ratings yet
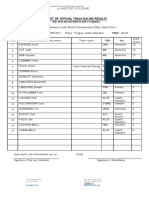
- FIM Speedway Youth World Championship 250cc Semi Final 1Document1 pageFIM Speedway Youth World Championship 250cc Semi Final 1Алексей ПолянцевNo ratings yet
- PE NotesDocument20 pagesPE NotesAlma C WalshNo ratings yet
- 2009-2010 HDK CATALOGUE Vol.12 - копияDocument125 pages2009-2010 HDK CATALOGUE Vol.12 - копияAbigail Raymond50% (4)