Professional Documents
Culture Documents
Americanas Neumo PDF
Uploaded by
Uri MoraOriginal Description:
Original Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Americanas Neumo PDF
Uploaded by
Uri MoraCopyright:
Available Formats
Preface
Anne B. Chang, MBBS, MPHTM, FRACP, PhD
Guest Editor
Hi Doc. John keeps getting respiratory infections. What should I do?
Jane has been coughing for 5 weeks and we have had little sleep. Can you give her
something to stop this cough?
Such scenarios are regularly seen by most clinicians whose practice includes
children. Indeed, children who have respiratory symptoms and signs or illness are
among the most common presentations to medical practitioners. In this issue of
Pediatric Clinics of North America, an evidence-based approach to common scenarios
in pediatric respiratory care is emphasized, because significant advances in clinical
care have occurred when long held dogma were questioned and evidence applied.
1
William Silverman eloquently articulated this in his book Wheres the Evidence?
1
He
further challenges clinicians to reflect on where the line between knowing (the
acquisition of newmedical information) and doing (the application of that newknowl-
edge) is drawn.
In this issue, authors with significant clinical and research expertise from the United
States, Europe, Asia, and Australia have utilized the GRADE
2
system for each recom-
mended approach. As these articles were written well before the British Medical Jour-
nal GRADE series were published, the short GRADE system was utilized.
2
The steps in
each article are designed to answer the questions: What is the evidence-based ap-
proach? and What is the strength of the evidence of the approach? The first five
articles focus on common respiratory symptoms that are encountered by clinicians,
such as respiratory noises and cough. The remaining articles are disease specific,
designed as an evidence-based approach to guide the clinician when a child who
has an illness such as pneumonia presents.
A significant limiting factor in almost all of the articles in this issue is the lack of
randomized controlled trials for the suggested approach taken. Indeed, even for the
very common symptoms of cough
3
or wheeze
4
in the young child, there is a glaring
lack of high level evidence, let alone for the less common but significant symptoms
of chest pain and shortness of breath. We have a long way to go to achieving complete
evidence-based medicine in the respiratory care of children. However, this issue
Common Respiratory Symptoms and Illnesses: A Graded Evidence-Based Approach
Pediatr Clin N Am 56 (2009) xvxvi
doi:10.1016/j.pcl.2008.11.001 pediatric.theclinics.com
0031-3955/08/$ see front matter 2009 Elsevier Inc. All rights reserved.
provides a succinct approach that highlights the evidence, or lack of, to managing
respiratory symptoms and conditions, which general practitioners and pediatricians
are likely to encounter in a child. I hope readers will find the articles useful in their
clinical practice and stimulate some to conduct clinical research to improve the man-
agement of common respiratory conditions in childhood. I thank the authors for their
valuable contributions to this issue.
Anne B. Chang, MBBS, MPHTM, FRACP, PhD
Child Health Division
Menzies School of Health Research
Charles Darwin University
Brisbane
Australia
Queensland Childrens Respiratory Centre
Royal Childrens Hospital
Herston Road
Herston, Brisbane
Queensland 4006
Brisbane
Australia
E-mail address:
annechang@ausdoctors.net
REFERENCES
1. Silverman WA. Wheres the evidence? Debates in modern medicine. New York:
Oxford University Press; 1999.
2. GRADE Working Group. Grading quality of evidence and strength of recommen-
dations. BMJ 2004;328:14907.
3. Chang AB, Glomb WB. Guidelines for evaluating chronic cough in pediatrics:
ACCP Evidence-Based Clinical Practice Guidelines. Chest 2006;129:S26083.
4. Brand PL, Baraldi E, Bisgaard H, et al. Definition, assessment and treatment of
wheezing disorders in preschool children: an evidence-based approach. Eur
Respir J 2008;32:1096110.
Preface xvi
Respi ratory Noi ses:
How Useful areThey
Cl i ni cal l y?
Craig Mellis, MBBS, MPH, MD, FRACP
As the parents of infants and young children will attest, noisy breathing is extremely
common in this age group. Whereas a multitude of different noises have been
described in the literature, the most frequently used terms are wheeze, rattle,
stridor, snore, and nasal snuffle/snort. Conventional wisdom, based on empiric
evidence and basic physiology, is that these noises emanate from specific anatomic
sites within the respiratory system (Table 1). Thus, correctly identifying these noises is
of major clinical relevance, in terms of localizing both the site of obstruction, and the
most likely underlying cause.
There is a vast array of underlying conditions, both congenital and acquired, that
can produce these noises. For example, in a major textbook on pediatric respiratory
disease there are more than 35 listed causes of wheeze, and a similar number for stri-
dor.
1
However, for practical purposes, most noises will be attributable to a relatively
small number of common, underlying conditions. Table 2 lists the most common
acute and persistent causes of these noises.
Although the clinical utility of these respiratory noises is often assumed, unfortu-
nately, distinguishing these noises fromeach other can be very difficult. Many children
will have multiple noises, as the obstruction to airway is often extensive (eg, inflamma-
tion involving both upper and lower airways), the noise may vary fromminute to minute,
and some noises will not clearly fit one of these simple descriptors. This difficulty in
categorizing the noise is worse when the noise is intermittent, described by the childs
parent, and not confirmed by the clinician. Further, even when heard by the clinician
agreement between clinicians on the terminology of these noises is far from perfect.
Because these noises can be considered as either a symptom (when reported on
history by a parent) or a sign (when confirmed on physical examination by a clinician)
it is crucial that we have high-quality research evidence regarding both the validity
(accuracy or closeness to the truth, when compared with a gold standard) and
Central Clinical School, Room 406, Blackburn Building D06, University of Sydney, Royal Prince
Alfred Hospital, Sydney, NSW 2006, Australia
E-mail address: c.mellis@usyd.edu.au
KEYWORDS
Noisy breathing
Validity and reliability
Wheeze
Rattle
Stridor
Pediatr Clin N Am 56 (2009) 117
doi:10.1016/j.pcl.2008.10.003 pediatric.theclinics.com
0031-3955/08/$ see front matter 2009 Elsevier Inc. All rights reserved.
the reliability (repeatability) of these symptoms and signs.
2
Reliability includes both
intraobserver reliability (ie, whether the clinician will agree with himself/herself
when observing the same sign on two separate occasions), and between-observer
reliability (ie, whether two clinicians, or parent and clinician, will agree when both
observe the same physical sign).
The purpose of this article is to appraise the published research evidence concern-
ing respiratory noises in infants and young children, with particular emphasis on the
validity and reliability of these noises, and their subsequent clinical relevance and di-
agnostic significance. Numerous textbooks and narrative reviews have comprehen-
sive descriptions of the clinical features of the conditions that can cause noisy
breathing, and these will not be elaborated on here. Rather, this review will focus on
evidence relating to validity and reliability of these noises (symptoms and signs),
and whether we can improve the utility of these reported and observed noises by
the use of technology, such as video recordings or computerized acoustic analysis.
It must be pointed out that despite noisy breathing being an extremely common clin-
ical problem, there is a paucity of high-quality clinical research evidence concerning
these key questions. The available evidence is from observational studies, and using
the Grade approach
3
is automatically assigned as low level evidence. There are also
inconsistencies and the data are sparse. Moreover, it is clear that much of the evi-
dence has come predominantly from several research groups, particularly in the
United Kingdom. Consequently, further research could have an important impact on
the conclusions drawn from the current evidence presented here.
Table1
Common noises and the site of origin
Noise Site of Origin
Wheeze Intrathoracic airways
Rattle Either or both intra- and extrathoracic airways
Stridor Extrathoracic airways
Snore Oro-naso-pharyngeal airway
Snuffle/snort Nasal passages/naso-pharynx
Grunt Alveoli/lung parenchyma
Table 2
Common clinical causes of noisy breathing
Noise Acute Persistent
Wheeze Intermittent asthma/Viral-induced
wheeze
Infants: Transient early wheeze (TEW)
Older children: Persistent asthma
Rattle Acute viral bronchitis Chronic sputum retention
(neuromuscular disorders)
Stridor Acute laryngotracheobronchitis
(or viral croup)
Laryngomalacia (or infantile larynx)
Snore Acute tonsillitis/pharyngitis Chronically enlarged tonsils and
adenoids
Snuffle Acute viral head cold (coryza) Allergic rhinitis
Mellis 2
DEFINITIONS
Wheeze
Wheeze is a high-pitched, continuous musical noise, often associated with prolonged
expiration. While predominantly heard in the expiratory phase, wheeze can occur
throughout the respiratory cycle. Basic respiratory physiology tells us that wheeze em-
anates from the intrathoracic airways, and can be produced by pathology either in the
large, central airways, or the small, peripheral airways. The intensity of the wheeze is
a poor indicator of the severity of the obstruction. Indeed, if the obstruction is ex-
tremely severe the wheeze may become inaudible.
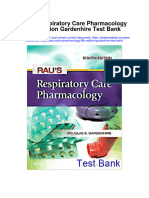
Wheeze as a result of large airways obstruction
When a structural lesion obstructs airflow in the large airways (intrathoracic trachea and
major bronchi), the resultant noise is a result of turbulent airflowat the point of narrowing
(Fig. 1). Thus, thewheezemay bequitelocalizedonauscultation, andisclassicallytermed
monophonic.
4
Although asthma is the commonest cause of wheeze, there are numer-
ous other potential causes, many of which are serious and require specific, urgent inter-
ventions. These include inhaled foreign body, endobronchial tuberculosis, and bronchial
adenoma. Extrinsic compression of a large, central airway will produce a similar type of
wheeze. Causes include rare, but important conditions, such as enlarged mediastinal
lymph nodes, benign or malignant mediastinal tumors, and achalasia.
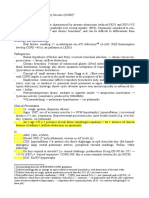
Wheeze as a result of small airways obstruction
In the presence of extensive small airway narrowing, the resultant high pleural pres-
sure swings can cause compression (inward collapse) of the large airways during ex-
piration, producing generalized expiratory wheezing (Fig. 2). The very young are
particularly prone to this because their large airways are relatively soft (floppy)
and more prone to collapse. Because the specific site of the large airway obstruction
noise is variable, the noise is termed polyphonic.
4
This is common in infants with
acute viral bronchiolitis, where the audible wheeze is usually accompanied by exten-
sive inspiratory crackles on auscultation. Abnormal floppiness of the walls of large,
central airways can produce an identical noise during normal respiration, and is char-
acteristically seen in the various forms of tracheomalacia and/or bronchomalacia.
Fig. 1. Wheeze attributable to large airways obstruction. (Adapted from Henry R. Wheezing
disorders other than asthma. In: Roberton DM, South M, editors. Practical paediatrics. 6th
edition. Edinburgh: Churchill Livingstone; 2007. p. 493; with permission.)
Respiratory Noises 3
While the now well-characterized transient early wheeze (TEW) is assumed to be
a result of congenitally abnormal small-caliber airways,
5
some studies have ques-
tioned this assumption.
6
Typically, infants with TEW wheeze persistently through the
first year, do not have inspiration crackles, are not troubled by either cough or short-
ness of breath, and cease wheezing by age 18 to 24 months.
Assessing wheeze
In evaluating a young child with parent-reported wheeze, the first step is to determine
exactly what the parents mean by that term. In particular, whether wheeze is being
used in a generic sense to describe any noise, particularly a rattly chest. Quality
of Evidence (GRADE):
3
Moderate. Data are from observational studies, which is the
appropriate study design. However, studies are predominantly small cohorts and
cross-sectional studies, with some conflicting data.
Inyoungchildrenwho, onexamination, haveacombinationof generalized, polyphonic
wheeze, asthma(or viral-inducedwheeze), islikely. Additional clinical informationshould
besought torule this inor out, suchas overinflationof thechest, prolongedexpiration, or
a trial of bronchodilator therapy (see article on asthma elsewhere in this issue).
In a young child, with either localized wheeze or monophonic wheeze, particularly if
accompanied by asymmetric breath sounds (that is, uneven air entry), a focal lesion
must be ruled out. This could include an endobronchial obstruction (eg, foreign
body) or a mass lesion compressing a major bronchus. Thus, further investigations
(eg, chest radiograph) and probable bronchoscopy are indicated. Quality of Evidence
(GRADE): Moderate to high. Appropriately, data are from observational studies, pre-
dominantly cohorts and case series.
Assessing infants with wheeze
In infants (younger than 12 months), a polyphonic wheeze on auscultation, particularly
if accompanied by generalized inspiratory crackles, indicates probable acute viral
bronchiolitis. Interventions should be considered only if there is significant breathless-
ness resulting in difficulty feeding. Apart from supplementary oxygen, adequate fluid
intake, and careful nursing care, no other intervention is of proven benefit. Quality of
evidence for no benefit: High for inhaled beta-agonists, adrenaline, and systemic
corticosteroids.
Fig. 2. Wheeze attributable to small airways obstruction. (From Henry R. Wheezing disorders
other than asthma. In: Roberton DM, South M, editors. Practical paediatrics. 6th edition. Ed-
inburgh: Churchill Livingstone; 2007. p. 493; with permission.)
Mellis 4
In infants with recurrent or persistent polyphonic wheezing, not associated with signifi-
cant cough, inspiratory crackles, or significant increase in the work of breathing, the most
likelydiagnosisisTEW. Qualityof evidence: High. Multiplebirthcohorts, consistent findings.
However, if the wheeze is associated with any of the above features, then asthma is
likely, and a trial of treatment appropriate (see article on asthma in this issue). In this
age group, the possibility of a rare congenital malformation of the airways also needs
to be considered.
Rattle
The current belief is that a rattle is a result of excessive secretions in the large airways,
which are presumably moving with normal respiration.
7
Rattles may be heard in either,
or both, inspiration and expiration. A research group in Yorkshire, United Kingdom,
coined the term ruttle to describe this coarse respiratory noise.
7
However, because
the term rattle is far more widely recognized, ruttle is best avoided, as there is al-
ready considerable confusion concerning the numerous terms used to describe noisy
breathing. A rapid improvement in rattles (measured objectively with acoustic analysis)
after inhalation of anticholinergics suggests these rattling noises are attributable to
coughing or clearance of sputum, rather than alterations in bronchomotor tone.
8
Par-
ents will often comment that as well as being able to hear the rattle, they can feel the
rattle (as a vibration), when placing their hands over the childs chest wall. Unfortu-
nately, parents commonly mislabel the rattle as a wheeze, resulting in overdiagnosis
of asthma (and unnecessary antiasthma treatment).
Assessing rattle
In an infant or young child with a rattle observed on examination, the most likely cause
is acute viral bronchitis. Further inquiry should be made concerning any associated
cough. No treatment is known to influence cough or rattle. Quality of evidence: Mod-
erate. One small randomized trial of inhaled anticholinergics reduced rattle.
If the child has an underlying chronic neurologic or neuromuscular condition, the
most likely explanation is inability to cough and/or swallow normal secretions, and ap-
propriate investigation to rule out pulmonary aspirations is indicated. Specific inter-
ventions are rarely indicated. Quality of evidence: Low. Paucity of data.
Stridor
In contrast to wheeze, stridor is predominantly inspiratory, and indicates obstruction
to airflow in the extrathoracic airways down to the level of the thoracic inlet. However,
wheeze and stridor can occur in both phases of respiration, particularly when the ob-
struction is severe. Because stridor is a sign of upper airway obstruction, it should
never be ignored. At this point in the respiratory tract there is only a single air passage.
Thus, if there is severe obstruction, respiratory arrest can occur, as there is no alter-
nate route for air entry.
The upper airway is a complex anatomic region, which is best divided into supra-
glottic, glottic, and subglottic areas. The supraglottic area includes the epiglottis, ar-
yepiglottic folds, and false vocal cords. Because this area is composed of soft tissue
and muscle, it is prone to inward collapse, resulting in obstruction. This typically oc-
curs in infants with laryngomalacia (infantile larynx).
9
Laryngomalacia is by far the
most common cause of stridor in infants, and is a result of collapse of the supraglottic
structure during inspiration. The noise varies in intensity depending on the respiratory
effort, typically louder with crying and feeding, softer when quietly sleeping. Although
classically causing inspiratory stridor, it is often associated with other noises such as
stertor (or clucking noise), but a normal cry (voice), and normal cough.
Respiratory Noises 5
Although acute epiglottitis (caused by Haemophilius influenzae type B) is now rare
because of widespread vaccination, the noise produced by this condition is typically
a soft vibrating snoring sound, rather than a harsh inspiratory stridor. Further, there
is usually no associated cough, and certainly no loud barking croupy cough.
The glottic area includes the true vocal cords. Typically, pathology at this level
causes a soft, hoarse cry (voice) as well as inspiratory stridor. Examples include vocal
cord paresis, laryngeal web, and laryngeal warts.
The subglottic area includes the extrathoracic trachea, down to the level of the tho-
racic inlet. Although supported by cartilage, this can collapse inwards in the presence
of large pleura pressure swings. Acute stridor at this anatomic level in infants and
young children is usually caused by viral croup (laryngotracheobronchitis).
10
Typi-
cally, the stridor is loud and harsh, together with a loud brassy, honking cough, and
signs of a viral respiratory tract infection.
Assessing stridor
In infants with persistent stridor, but no significant increase in the work of breathing, no
cough, normal cry, no apnea or cyanotic episodes, and thriving, then laryngomalacia
is the most likely cause. No further investigation is warranted apart from follow-up re-
view. Quality of evidence: High. Large observational studies with consistent findings.
If stridor is persistent and associated with any of the above features, then consider
significant upper airway pathology, and probable larangoscopy and bronchoscopy.
Quality of evidence: Moderate. Mostly from small cohorts and case series.
If stridor is acute, and associated with symptoms and signs of a viral respiratory
tract infection plus a brassy (croupy) cough, then viral croup (larynotracheobronchitis)
is most likely. If the stridor is present at rest, the obstruction should be considered
moderately severe and systemic corticosteroids or inhaled corticosteroids are indi-
cated. Quality of evidence: High. Systematic reviews.
If the acute stridor occurs in the absence of a viral respiratory tract infection, then the
possibility of a large ingested foreign body should be considered, particularly if there is
anydifficulty inswallowing. Qualityof evidence: Moderate. Small cohorts andcaseseries.
Snore
Although snoring is generally more obvious in inspiration, the noise is frequently audi-
ble throughout the respiratory cycle. The noise arises from an increase in the resis-
tance to airflow through the upper airways, predominantly in the region of the
nasopharynx and oropharynx. During rapid eye movement (REM) sleep there is relax-
ation of the oropharyngeal musculature, thus further compromising the narrowair pas-
sages, resulting in the vibratory noise we all recognize as snoring. Predictably, in
young children the usual cause is enlarged tonsils and/or adenoids.
Themajor issueclinically, is whether thesnoringis of any relevancetothechilds health.
Distinguishing primary snoring from pathologic obstructive sleep apnea-hypopnea
(OSAH) is difficult clinically.
11
If there are associated symptoms suggesting OSAH, a for-
mal sleep study may be indicated. Symptoms that suggest genuine OSAH include ob-
served apnea, excessive daytime sleepiness, and behavior or learning problems.
12
This
noise will not be discussed in detail here, as it is covered in another article in this issue.
Snuffles and Snorts
The terms snuffles and snorts are used to describe respiratory noises emanating
from the nasal passages. Snuffle has also been used to describe any discharge from
the nasal passages, and is sometimes used to describe a minor viral upper respiratory
tract infection (head cold). The term was originally used in relation to congenital
Mellis 6
syphilis. These nasal noises are frequently audible in both inspiration and expiration,
and often associated with visible secretions from the nares.
Assessing snuffles and snorts
In young infants with persistent nasal obstruction, nasal patency needs to be
assessed to rule out choanal atresia. Bilateral nasal obstruction in older children sug-
gests either perennial allergic rhinitis or, rarely, nasal polyps (usually in association
with cystic fibrosis). If persistent, purulent nasal secretions consider chronic bacterial
rhinosinusitis. Latter is suggestive of underlying presence of suppurative airways
disease (eg, cystic fibrosis, immune deficiency syndromes, and ciliary dysfunction).
Grunt
An expiratory grunt is classically seen in the presence of extensive alveolar pathology
and is considered a sign of serious disease. Grunting is particularly seen in hyaline
membrane disease (neonates) and lobar pneumonia (infants and children). However,
in both these situations, other clinical features of the underlying problem (especially
respiratory distress) are far more impressive, and of far greater diagnostic relevance,
than the noise per se. The expiratory grunt is a natural form of continuous positive air-
way pressure (CPAP), aimed at improving oxygenation, and is mechanistically similar
to pursed lips breathing in adults with chronic dyspnea.
PREVALENCE OF NOISY BREATHING
Although wheeze is well studied, there are few observational studies of infants ad-
dressing the question of how common are all forms of noisy breathing? To answer
this question Thornton and colleagues
13
studied a birth cohort of almost 300 randomly
chosen, normal-term infants in Cambridge, England. This cohort was followed longi-
tudinally from birth to 6 months. Mothers were interviewed at home about any con-
cerns they had regarding their infants health. In addition, mothers were questioned
in detail about 28 specific symptoms to determine the incidence, severity, and
duration of these specific symptoms.
Respiratory symptoms were by far the dominant concern. The commonest concern
expressed by these mothers was noisy breathing, followed by common cold symp-
toms, running nose, cough, and breathing difficulties. More than 80% of the mothers
reported1 or more of the 28 specific symptoms in the previous 24 hours. Noisy breath-
ing was reported in 30%and was second only to cold peripheries (39%). Further, of
those mothers reporting noisy breathing, 20%classified this as moderate or severe,
and almost half stated that the noisy breathing was always present. Clearly, the prev-
alence of respiratory symptoms, particularly noisy breathing, is very high in apparently
healthy, term infants.
A further observational study from the United Kingdom investigated both the
frequency of noisy breathing and the terminology used by parents to describe noisy
breathing in infants younger than 18 months of age.
7
Part of this study included a com-
munity survey, using a postal questionnaire about noisy breathing, to 200 parents of
infants. Of these 200, only 62 responded and, of these, 39 reported noisy breathing.
Clearly, with this low response rate, the 63% prevalence is an overestimate of the
true prevalence, and further high-quality research on this question is needed.
On the other hand, rates of wheeze in infants have been the subject of numerous
birth cohorts, the most notable being that from Tucson, Arizona.
5
The latter study in-
troduced the now commonly used term transient early wheeze (TEW) to describe
otherwise healthy infants who wheeze in infancy but cease wheezing by age 3 years.
Most studies of TEW indicate that theses infants have abnormal lung function from
Respiratory Noises 7
birth (ie, smaller than normal-caliber airways). Large birth cohort studies froma number
of countries including the United Kingdom,
14,15
Sweden,
16
France,
17
and Brazil
18
have
been studied to ascertain the rate of parent-reported wheeze (or whistling from the
chest). Although rates vary slightly, most indicate that approximately 30% to 40%
of parents report infant wheeze; however, few studies have validated these parental
reports.
One of the few studies that compared parent reported respiratory illness in infants
with clinical diagnosis was from New Mexico.
19
An active illness surveillance system
was established over the first year of life in a large birth cohort (n 5 1200). This
included a daily symptom diary kept by parents plus a telephone interview every
2 weeks. If a respiratory illness was reported, infants were visited at home by a nurse
practitioner and specimens for virology collected. Each child contributed an average
of 429 observation days. Most respiratory illnesses diagnosed by the nurse practi-
tioner as lower respiratory (LRI) were accompanied by a parent report of either
wheeze or wet cough. LRI with wheeze was less frequent than LRI with wet cough
(6% versus 33%). Thus, in infancy coughing illnesses are far more frequent than
wheezing illnesses. However, as many of the infants with LRI and wet cough had
a rattly, bubbly chest, parents are likely to have reported the noise as wheeze
(if they had not been seen, and confirmed as non-wheeze, by a clinician). These
results highlight the likely overdiagnosis of parent-reported wheeze in infants.
Reported rates of wheeze in older children has also been extensively studied. By
far the best data currently available are from the International Study of Asthma and
Allergies in Childhood (ISAAC) study.
20
This is a worldwide, systematic study using
identical methodology to measure the rates of reported wheeze in both younger
(6- to 7-year-olds) and older children (13- to 14-year-olds). For the younger children,
rates of recent wheeze were as reported by parents (ie, Has your child had
wheezing or whistling in the chest in the past 12 months?), and for the older chil-
dren, self-reported rates of recent wheeze (ie, Have you had wheezing or whis-
tling in the chest in the past 12 months?). To assess time trends, these studies
have now been repeated. The results are available from the most recent cross-sec-
tional questionnaire survey of almost 200,000 6- to 7-year-olds in 37 countries and
over 300,000 13- to 14-year-olds in 56 countries. For 6- to 7-year-olds, parent-re-
ported rates of recent wheeze varied from a low of 2.8% (Indonesia) to a high of
37.6% (Costa Rica). High rates were also reported in New Zealand (22.2%), United
Kingdom (20.9%), Australia (20%), and North America (Canada, 18.2%). For 13- to
14-year-olds, self-reported rates of recent wheeze were in a similar range, with
a low of 3.4% (Albania) and a high of 31.2% (Isle of Man). High rates were again re-
ported for Costa Rica (27.3%), New Zealand (26.7%), United Kingdom (24.7%), and
North America (United States, 22.3%).
However, a major question with all these questionnaire studies is exactly what do
parents and/or children understand by the term wheeze? In particular, whether
many of those with reported wheeze have other respiratory noises (such as rattle,
stridor, or snore) which is being misinterpreted as a wheeze.
WHAT DO PARENTS UNDERSTAND BY WHEEZE?
This question was addressed in a hospital-based observational study of older chil-
dren.
21
A total of 139 children (aged 4 months to 15 years, median 2.5 years) were as-
sessed in the emergency department (ED) to measure the agreement between clinician
and parent report on the noise. There was a less than 50% agreement between a clini-
cians finding wheeze and parents report of wheeze. That is, in children presenting to
Mellis 8
ED with wheeze (or asthma), where the doctor finds wheeze, 39% of the parents use
words other than wheeze (particularly cough and/or difficult breathing). Also, when
the doctor does not find wheeze (especially with upper airway noises), 14% of parents
use the termwheeze to describe this noise. Clearly, parents and clinicians differ widely
in the use of the term wheeze in children with acute symptoms in an ED setting.
In the same study, 160 parents attending the outpatient chest clinic, because of
wheeze, were asked, What do you understand by wheeze, and howdo you recognize
wheeze in your child? Terms used by parents to describe the noise included hissing,
squeaking, whistle, and rasp. Surprisingly, almost a quarter of these parents did not
equate wheeze with a noise. Forty percent of parents stated they used nonauditory
cues when asked, How do they know when your child is wheezy? It is clear that
for a substantial proportion of parents, wheeze has a very different meaning to that
used by clinicians.
The implication of these findings on the accuracy of numerous pediatric epidemiol-
ogy studies that routinely report the rates of Has your child wheezed in the past
12 months? or Has your child ever wheezed? as asthma symptoms are obvious.
VALIDATION OF RESPIRATORYQUESTIONNAIRE TO MEASURE WHEEZE
A study from Brazil attempted to validate a questionnaire on wheeze in infancy.
22
In
this study of young children presenting to the ED with an acute respiratory illness, par-
ents answered a questionnaire on wheezing (adapted from the International Study of
Wheezing in Infants).
22
A total of 209 infants aged 12 to 15 months were assessed.
Fifty-six of these were reported to be currently wheezing and this was confirmed in
43. A further 153 parents reported no current wheeze and this absence of wheeze
was confirmed clinically in 146.
Assuming the ED clinician is the gold standard, the sensitivity and specificity of
parent-reported wheeze was 0.86 and 0.92 respectively (that is, a positive likelihood
ratio of >10). This is considerably more accurate than that seen in most other similar
studies in infants and toddlers. This suggests that using a questionnaire can be more
accurate than simply asking the parent to nominate a single termto describe the noise.
COMPARING THE SEVERITYOF PARENT-REPORTED WHEEZE WITH CLINICIAN-CONFIRMED
WHEEZE
One observational study measured the lung function of children with confirmed (by
clinicians) with unconfirmed (parent-reported) wheeze.
23
This study was part of
a large UK birth cohort (n 5 1000) and describes a subgroup of 454 children followed
to the age of 3 years. A total of 186 (41%) of these children had parent-reported
wheeze, and in 130 (29%) the wheeze was confirmed by a clinician. Specific airway
resistance (sRaw) was measured at the age of 3 by plethysmography. The major find-
ing was that sRawwas significantly higher (reflecting greater airflow limitation) in those
children with clinician confirmed wheeze, compared with children who had never
wheezed, and those with parent-reported wheeze. In short, children with clinically
confirmed wheeze in the first 3 years of life have more abnormal lung function, sug-
gesting a more clinically relevant degree of airway pathology, than those with par-
ent-reported wheezing (and those who have never wheezed).
UTILITYOF VIDEOS AS AGOLD STANDARD
An observational study fromthe United Kingdom investigated the terminology used by
parents to describe noisy breathing in infants younger than 18 months of age.
7
The
Respiratory Noises 9
parents of approximately 100 infants with noisy breathing were interviewed. These in-
fants were from three separate populations: hospital inpatients (n 5 44), hospital out-
patients (n 5 19), and a community sample (n 5 29). Almost half the parents used the
term wheeze (or whistle/musical sound) to describe noisy breathing initially, while
the term rattle (or ruttle/ bubbly chest) was used almost as frequently. The terms
stridor (5%), snuffly (5%), and snore (3%) were far less commonly used.
To evaluate the accuracy of these terms, the parents of 72 of these infants were
shown a series of videos specifically displaying footage of infants with typical wheeze,
rattle, or stridor. After viewing these videos, parents were then asked to choose the
term that best matched their childs noisy breathing. Approximately a third of the par-
ents changed fromtheir initial termwheeze, to rattle. If we assume the video is the
gold standard, these numbers translate to a sensitivity of 0.63 and a specificity of
0.68 for parents use of the term wheeze. That is, a false positive rate of 32%,
and false negative rate of 37%. For parent-reported rattle, the corresponding figures
are 0.45 and 0.81 (sensitivity and specificity respectively), or a false positive rate of
20% and false negative rate of 55%! An additional finding fromthis study was that giv-
ing parents a list of terms to describe their infants noise was unhelpful. Although these
parents reported that an adult imitating the noise was of limited value, they found the
video clips of infants with specific, single noises to be the most useful method of as-
sessing their infants respiratory noises.
Clearly, the terminology used by parents is very prone to misclassification. Thus, it is
essential that clinicians and epidemiologists attempt to clarify what parents really
mean by these commonly used terms, such as wheeze and rattle. Evidence suggests
the term wheeze is overused by parents, while the term rattle is underused. Add-
ing to the difficulty, it is apparent that some infants will have, simultaneously, both
a wheeze and a rattle. Moreover, infants will switch over time from a predominant
wheeze (eg, early in the course of viral bronchitis with wheeze) to a predominant
rattle (eg, resolving stage of viral bronchitis). The major clinical implication of these
data is that clinicians should not equate wheeze (particularly wheeze reported by
parents, and unconfirmed by a clinician) with asthma. When assessing children with
parent-reported wheeze, clinicians need to question further as to what the parents
are really describing as a wheeze.
In a further attempt to evaluate the accuracy of parents descriptions of noisy breath-
ing, Cane and McKenzie
24
assessed the utility of video clips of children demonstrating
noisy breathing. These videos included both typical wheeze and other noises, such as
stridor, snore, and stertor (ie, a clucking hen noise). The parents of 190 children youn-
ger than 8 years were shown these videos. Parents were a mix of those with andwithout
achildwithasthma(or other respiratory complaints). Videos wereshowntoparents who
were then asked what word they would use to describe these noises. In addition, par-
ents were asked where they believed these noises were coming from, ie, chest, throat,
or nose. The first major finding was the difficulty the authors hadwith clinicians agreeing
on what the actual video noises were demonstrating. Agreement among clinicians was
poorin only 10 of the 15 videos was there unanimous agreement on the termused to
describe the noise. This was despite the videos demonstrating a distinct, typical single
sound, which is obviously far removed from real life, clinical situations.
As with the previous study using videos, 30% of the parents (whether they had
a wheezy child or not) used terms other than wheeze to describe the video of
wheezing. A further 30% of these parents falsely labeled other sounds (stridor, snore,
or stertor) as wheeze. Although parents reports of symptoms were in poor agree-
ment with clinicians, the ability of parents to identify the origin (or location) of the noise
was in relatively good agreement with the clinicians. This study supports other studies
Mellis 10
indicating that video clips are a method of improving the accuracy of parental terms
used to describe noisy breathing, especially wheeze.
Video questionnaires have been used to validate measures of wheeze in older chil-
dren. The ISAAC written and video questionnaires were compared in 317,000 adoles-
cents (aged 13 to 14 years old) in 40 countries.
25
As expected, responses to the video
gave lower prevalences of wheeze symptoms. Chance corrected agreement (Kappa)
was also generally low. Initial pilot studies, using hypertonic saline bronchial chal-
lenges in 393 school children (age 13 to 15 years) to validate the ISAAC questionnaire
found low sensitivity (47%), but high specificity (92%) when compared with a positive
response to the question regarding current wheeze.
26
Similar results were found for
a 6-minute exercise challenge (sensitivity 5 46%; specificity 5 88%). Similar findings
have been published more recently from Germany as part of the ISAAC Phase II
study.
27
Although the high specificity is encouraging (to rule asthma in), a bronchial
challenge test is not generally considered an adequate gold standard for the diag-
nosis of wheeze or asthma.
NATURAL HISTORY/PROGNOSIS OF NOISY BREATHING
An important question is whether early respiratory noises predict subsequent wheeze.
The study by Turner and colleagues
28
described the natural history of the full range of
these early respiratory noises. This observational study was part of a large Scottish
birth cohort of approximately 2000 infants. A respiratory questionnaire (modified
ISAAC questionnaire) was administered at the age of 2 and 5 years. The key findings
were the following: children with a whistle at age 2 were more likely to wheeze
(73%), and were more likely to be receiving asthma treatment (40%) at age 5 years,
compared with children with a rattle at 2 years (34% and 11% respectively), or
who purred (39% and 18% respectively). Further, children with a whistle at 2
years are more likely to have a mother with asthma (38%). Children with a rattle
or a purr at 2 years are more likely to have been exposed to tobacco smoke at
home, compared with those with either a whistle, or no noise at 2 years. This is in
keeping with the belief that a rattle is attributable to hypersecretion of mucus and/or
recurrent or persistent bronchitis, possibly related to exposure to environmental to-
bacco smoke.
While rattle and purr (at 2 years) resolved in the majority by age 5 years, of real
concern is that approximately half of these children (with a rattle or a purr) were diag-
nosed as having asthma. On the other hand, whistle (or wheeze) at 2 years persisted in
a substantial proportion at 5 years, and proved to be a strong predictor of ongoing
wheeze and subsequent need for asthma treatment. These authors also made the im-
portant observation that most parents seem to think that wheeze is any respiratory
noise, of which a whistle is one sub-set [of wheeze].
28
The natural history of wheeze in infancy has been studied extensively, particularly by
Martinez and colleagues.
5
This birth cohort from Tucson, Arizona, has been studied
again in adolescence
29
and early adulthood.
30
The key findings are that three pheno-
types of wheeze are identifiable in early childhood, namely, transient early wheeze
(TEW), persistent wheeze (PW), and late-onset wheeze (LOW). As discussed above,
infants with TEW have abnormal lung function before the onset of their wheeze. How-
ever, a more recent assessment of this cohort at age 22 years
30
found the TEW group
(with reduced airway function at birth) continued to have reduced airflow, and there-
fore may be at increased risk of subsequent chronic obstructive pulmonary disease.
Those with PW (ie, wheezed both in the first 3 years and beyond) appear to have def-
inite atopic asthma. Those with LOW have no wheeze in the first 3 years, but wheezed
Respiratory Noises 11
after the age of 3 years. Children with LOWhave been termed non-atopic wheezers (or
viral-induced wheeze), and appear to have a very mild form of asthma.
29
The distribu-
tion of these phenotypes in early childhood is as follows: approximately 50% of the
Tucson cohort had never wheezed; 20% had TEW; 15% had LOW; and 15% PW.
These figures indicate that most infants who wheeze in the first year of life do not
have asthma.
DO PARENTS AND CHILDREN AGREE ON SYMPTOMS OF WHEEZE?
In an attempt to validate parent-reported exercise wheeze in older children (age 6 to
18 years), 97 children were assessed in summer camps in California.
31
Both criterion
validity and construct validity were assessed by comparing reported symptoms on ex-
ercise with measured lung function following an exercise provocation test. Parents
completed a telephone survey of their childs symptoms with exercise. As expected,
parents generally report fewer exercise-related symptoms of wheeze than their chil-
dren. Although there was some correlation between the variables on lung function
testing with those reported by parents, these were generally weak. These results con-
firm other studies indicating that school-age children are more accurate reporters of
wheeze than their parents. These data have important implications for the clinical
care of asthma in school-age children.
ACOUSTIC ANALYSIS
Adult studies have highlighted problems with both accuracy (validity) and reliability (or
repeatability) of respiratory signs using a stethoscope.
3234
Given the increased diffi-
culty of examining young, uncooperative children, the assumption is that errors will be
substantially greater in pediatric practice. In an attempt to improve the utility of respi-
ratory noises, computerized acoustic analysis has been evaluated. Most studies have
been in adults and the published data in children are limited.
A small study (n 515) of infants suggested a potential role for acoustic analysis.
32
In
particular, the ability of acoustic analysis to clearly distinguish wheeze from rattle. El-
phick and colleagues
32
found the acoustic properties of wheeze and rattle were quite
distinct. Wheeze was characterized by a sinusoidal waveform, with several distinct
peaks in the power spectrum display (Fig. 3). Rattle (ruttle) was characterized by
an irregular nonsinusoidal waveform, with diffuse peaks in the power spectrumdisplay
(Fig. 4). The rattle also had a more intense sound at a frequency of less than 600 Hz.
Although the results in this study were encouraging, the 15 infants were carefully cho-
sen to ensure they had only one distinct sound (7 with wheeze, 8 with a rattle).
Unfortunately, in a more recent study of young children by the same authors,
33
acoustic analysis proved to be disappointing. This study assessed the validity and re-
liability of acoustic analysis of respiratory noises in infants younger than 18 months. A
total of 102 infants (mean age 5 months) who were in hospital with noisy breathing
were evaluated. Each child was tested independently with both a stethoscope (by
two experienced clinicians) and with acoustic analysis (also interpreted independently
by two observers). There was effective blinding of those performing each of these
measurements, and all measurements were taken either concurrently or immediately
sequentially. All measures were taken in the right upper zone during tidal breathing.
Most of these infants had acute viral bronchiolitis (58%) or an acute respiratory infec-
tion (eg, pneumonia, atelectasis, and cystic fibrosis). The investigators used prede-
fined definitions for wheeze, rattle, and crackle on stethoscope, and predefined
patterns for these three sounds on acoustic analysis.
Mellis 12
Both acoustic and stethoscope data were available for 100 infants. Agreement be-
tween stethoscope examination and acoustic analysis, using the Kappa (k) statistic
(agreement over and above chance agreement)
35
was poor for both wheeze (k 5
0.07) and rattles (k 5 0.11), and fair only (k 5 0.36) for crackles. Further, the ability
to distinguish between the two audible noises (wheeze and rattles) using both stetho-
scope and acoustic analysis was poor. These validity results are similar, or worse, than
those previously reported in adults. This is understandable, given the majority of the
infants had acute bronchiolitis, which characteristically causes multiple noises on aus-
cultation. Measures of reliability were also poor. There was poor agreement between
the two experienced observers using a stethoscope for wheeze (k 5 0.18), although
for rattles and crackles, agreement was moderate (k 5 0.53 and k 5 0.46, respec-
tively). Two observers also assessed the acoustic analysis results. Between-observer
agreement using acoustic analysis was poor for both wheeze and rattles (k 50.24 and
0.22, respectively), but moderate for crackles (k 5 0.44).
In summary, in a study using vigorous methodology for evaluating a diagnostic test,
the results for both validity and reliability of both the stethoscope and acoustic anal-
ysis were poor. Although it is possible that future development of acoustic analysis
techniques could result in improved validity and reliability, at present it appears acous-
tic analysis has little to offer over the stethoscope in real life clinical situations in infants
Fig. 3. Wheeze with characteristic sinusoidal pattern. (From Elphick HE, Ritson S, Rodgers H,
et al. When a wheeze is not a wheeze: acoustic analysis of breath sounds in infants. Eur
Respir J 2000;16:594; with permission.)
Fig. 4. Ruttles with nonsinusoidal irregular waveform pattern. (From Elphick HE, Ritson S,
Rodgers H, et al. When a wheeze is not a wheeze: acoustic analysis of breath sounds in in-
fants. Eur Respir J 2000;16:594; with permission.)
Respiratory Noises 13
with noisy breathing. Moreover, there is poor agreement among clinicians when listen-
ing to infants and young children with common respiratory noises.
UTILITYOF TRACHEAL SOUND RECORDINGS
Several groups have used tracheal sound recordings in children, particularly to ex-
plore this method as a more sensitive indicator of wheeze in bronchial provocation
testing of very young children. Godfrey and colleagues
36,37
used nebulized AMP chal-
lenge in 80 preschool children and found detection of wheeze acoustically to be
a more sensitive way of detecting airway obstruction than the stethoscope (PC
wheeze), thus enabling the challenge to be ceased earlier (and safer). Pediatric studies
have also analyzed lung sounds and breathing patterns in infants with acute viral bron-
chiolitis to assess response to bronchodilators.
38
This group noted complex wave-
forms that differed from the sinusoidal waveforms described as typical of wheeze,
indicating that multiple noises are characteristic of this clinical situation.
38
Several studies have found tracheal sounds to be more sensitive than the stetho-
scope for detecting wheeze
3941
in children with exercise-induced asthma. These
findings support those of Godfrey and colleagues,
36
namely, that amplification of
wheeze enables the clinician to detect this earlier than with a stethoscope. Further,
continuous tracheal sound recording appears to be of more substantial value in objec-
tively measuring cough, especially night cough.
40
USE OF VIDEO QUESTIONNAIRES TO IDENTIFYSTRIDOR
Video questionnaire has been used to identify upper airway abnormalities.
42
A group
of 43 preschoolers (range 3 to 58 months, median 17 months) with noisy breathing
were studied via fiberoptic bronchoscopy. Thirty (70%) had wheeze as their main
symptom, 19 were clinician confirmed, whereas the other 11 had only parent-reported
wheeze. Parents were shown previously validated video clips of wheeze, stridor, and
other airway noises. Ten of the 30 parents who initially reported wheeze identified the
noise as upper airway noise or stridor on the video. Of these 10 children, 7 had abnor-
mal upper or central airway pathology on bronchoscopy. Conversely, none of the chil-
dren whose parents correctly identified wheeze (on the video questionnaire) had an
abnormality on bronchoscopy.
Thus, a validated video questionnaire can improve the ability of parents to identify
upper airway abnormalities in children with parent-reported wheeze.
Unfortunately, clinicians do have problems distinguishing stridor from wheeze. The
entity exercise-induced inspiratory stridor (or vocal cord dysfunction [VCD]) is an ex-
cellent illustration of the difficulty clinicians have distinguishing wheeze from stridor.
Despite the noise being predominantly inspiratory in most patients, this condition is
almost invariably incorrectly diagnosed as exercise-induced asthma (EIA). This is de-
spite the noise being predominately inspiratory, coming on during, rather than after,
exercise, rapid recovery, and lack of effect of short-acting beta-agonists. In a large
case series (n 5 95) of predominantly young women with VCD, almost half also had
genuine asthma. However in those with VCD and no asthma, asthma had been mis-
diagnosed for an average of 5 years.
SUMMARY
A number of conclusions can be drawn from the research evidence on noisy breathing
(Box 1). It is clear that there are major problems with both the accurate (valid) and
Mellis 14
reliable (reproducible) identification of respiratory noises. This is particularly so
when the noise is parent reported, and not confirmed by a clinician.
Clearly, clinicians must exercise great care when diagnosing specific types of noisy
breathing to ensure it is not incorrectly labeled. An error in recognition will result in the
clinician assuming a specific anatomic level of airway obstruction, a misleading differ-
ential diagnosis, inappropriate investigation, and treatment. Clinicians need to con-
sider the whole constellation of symptoms and signs, and not totally focus on the
specific type of noise. In particular, any associated symptoms or signs, such as
breathlessness, cough, voice changes, and signs of a viral respiratory infection.
This is especially so with misclassification of a rattle as a wheeze, resulting in unnec-
essary and useless asthma treatment. This is of real concern with inhaled corticoste-
roids, because the lack of response can result in an escalation of the dose, resulting in
side effects. A more sinister error is misclassifying stridor as wheeze, and running the
risk of missing potentially severe, life-threatening upper airway obstruction.
Given the high error rate with parent-reported wheeze there is a need to reex-
amine the extensive literature on the epidemiology of wheeze in infants and young chil-
dren, since this is derived from parent-reported wheeze (ie, unconfirmed by
a clinician). Clearly a large percentage of these children have a rattle rather than
a wheeze, and it is inappropriate to call parent-reported wheeze an asthma
symptom.
20
This inflation of the rate of childhood asthma symptoms is particularly
prominent in infants and preschool young children. Finally, it is obvious we need
more high-quality research evidence to derive better evidence on the clinical utility
of these noises, and their natural history (see Box 1).
REFERENCES
1. Brown M, Wayne J. Clinical assessment and diagnostic approach to common
problems. In: Taussig L, Landau LI, editors. Pediatric respiratory medicine. Mis-
souri: Mosby; 1999. p. 13652.
2. McGee S. Understanding the evidence: diagnostic accuracy of physical findings.
Evidence-based physical diagnosis. Philadelphia: W.B Saunders Company;
2001. p. 323.
Box1
Summary points
Noisy breathing is a common symptom in infants.
Parent-reported wheeze does not mean the infant or child has a wheeze.
Many infants and children with parent-reported wheeze have a rattle rather than wheeze.
A rattle should not be considered an asthma symptom.
Clinicians do not always agree on the terminology of these common noises.
A major potential error is misclassifying stridor as a wheeze, and missing significant upper
airway obstruction.
Published epidemiology rates of asthma in young children are based on parent-reported
wheeze, and are clearly erroneous.
The use of videos of typical noises can improve the accuracy of parents descriptions of noises.
Current technology (such as acoustic analysis) to improve the utility of these noises is
disappointing.
More high-quality research is needed to establish the clinical utility of these noises.
Respiratory Noises 15
3. GRADE Working Party. Grading quality of evidence and strength of recommenda-
tions. BMJ 2004;328:18.
4. Fakhoury K, Seilheimer D, Hoppin A. Approach to wheezing in children. 2008.
Available at: http://www.uptodate.com. Accessed April 17, 2008.
5. Martinez F, Wright A, Taussig L, et al. Asthma and wheezing in the first six years of
life. The Group Health Medical Associated. N Engl J Med 1995;332(3):1338.
6. Turner S, Palmer L, Rye P, et al. The relationship between infant airway function,
childhood airway responsiveness, and asthma. Am J Respir Crit Care Med 2004;
169(8):9217.
7. Elphick H, Sherlock P, Foxall G, et al. Survey of respiratory sounds in infants. Arch
Dis Child 2001;84:359.
8. Elphick H, Ritson S, Ml E. Differential response of wheezes and ruttles to anticho-
linergics. Arch Dis Child 2002;86:2801.
9. Olney D, Greinwald JJ, Smith R, et al. Laryngomalacia and its treatment.
Laryngoscope 1999;109(11):17705.
10. Quintero D, Fakhoury K. Assessment of stridor in children. 2008. Available at:
http://www.uptodate.com. Accessed April 17, 2008.
11. Gozal D, Burnside M. Increased upper airway collapsibility in children with ob-
structive sleep apnea during wakefulness. Am J Respir Crit Care Med 2004;
169:1637.
12. Sterni L. Evaluation of snoring or suspected obstructive sleep-hypopnea in chil-
dren. 2008. Available at: http://www.uptodate.com. Accessed April 17, 2008.
13. Thornton A, Morley C, Hewson P, et al. Symptoms in 298 infants under 6 months
old, seen at home. Arch Dis Child 1990;65:2805.
14. Lewis S, Richards D, Bynner J, et al. Prospective study of risk factors for
early and persistent wheezing in childhood. Eur Respir J 1995;8(3):
34956.
15. Butland B, Strachan D. Asthma onset and relapse in adult life: the British 1958
birth cohort study. Ann Allergy Asthma Immunol 2007;98(4):33743.
16. Kull I, Bergstrom A, Lilja G, et al. Fish consumption during the first year of life and
development of allergic diseases during childhood. Allergy 2006;61(8):100915.
17. Clarisse B, Demattei C, Nikasinovic L, et al. Bronchial obstructive phenotypes in
the first year of life among Paris birth cohort infants. Pediatr Allergy Immunol
2008; [epub ahead of print].
18. Menezes A, Hallal P, Muino A, et al. Risk factors for wheezing in early adoles-
cence: a prospective birth cohort study in Brazil. Ann Allergy Asthma Immunol
2007;98(5):42731.
19. Samet J, Cushing A, Lambert W, et al. Comparability of parent reports of respira-
tory illness with clinical diagnosis in infants. Am Rev Respir Dis 1993;148:4416.
20. Asher M, Montefort S, Bjorksten B, et al. Worldwide time trends in the prevalence
of symptoms of asthma, allergic rhinoconjuctivits, and eczema in childhood:
ISAAC phases one and three repeat multicountry cross-sectional surveys. Lancet
2006;368:73343.
21. Cane R, Ranganathan S, McKenzie S. What do parents of wheezy children under-
stand by wheeze? Arch Dis Child 2000;82:32732.
22. Chong Neto H, Rosario N, Dela Bianca AC, et al. Validation of a questionnaire for
epidemiologic studies of wheezing in infants. Pediatr Allergy Immunol 2007;18:867.
23. Lowe L, Murray C, Martin L, et al. Reported versus confirmed wheeze and lung
function in early life. Arch Dis Child 2004;89:5403.
24. Cane R, McKenzie S. Parents interpretations of childrens respiratory symptoms
on video. Arch Dis Child 2001;84:314.
Mellis 16
25. Crane J, Mallol J, Beasley R, et al. Agreement between written and video ques-
tions for comparing asthma symptoms in ISAAC. Eur Respir J 2003;21(3):45561.
26. Riedler J, Reade T, Dalton M, et al. Hypertonic saline challenge in an epidemiological
survey of asthma in children. Am J Respir Crit Care Med 1994;150(6 Pt 1):16329.
27. Buechele G, Rzekhak P, Weinmayr G, et al. Assessing bronchial responsiveness
to hypertonic saline using the Stepwise Protocol of Phase Two of the International
Study of Asthma and Allergies in Childhood (ISAAC II). Pediatr Pulmonol 2007;
42:13140.
28. Turner S, Leone C, Harbour P, et al. Early rattles, purrs and whistles as predictors
of later wheeze. 2008. Available at: http://adc.bmjjournals.com. Accessed April
17, 2008.
29. Morgan W, Stern D, Sherrill D, et al. Outcome of asthma and wheezing in the first
6 years of life. Am J Respir Crit Care Med 2005;172(10):12538.
30. Stern D, Morgan W, Wright A, et al. Poor airway function in early infancy and lung
function by age 22 years: a non-selective longitudinal cohort study. Lancet 2007;
370(9589):7179.
31. Lara M, Duan N, Sherbourne C, et al. Differences between child and parents of
symptoms among Latino children with asthma. 1998;106(2). Available at: http://
www.pediatrics.org. Accessed April 17, 2008.
32. Elphick H, Ritson S, Rodgers H, et al. When a wheeze is not a wheeze: acoustic
analysis of breath sounds in infants. Eur Respir J 2000;16:5937.
33. Elphick H, Lancaster G, Solis A, et al. Validity and reliability of acoustic analysis of
respiratory sounds in infants. Arch Dis Child 2004;89:105963.
34. Dalmay F, Antonini M, Marquest R, et al. Acoustic properties of the normal chest.
Eur Respir J 1995;8:17619.
35. Altman D. Some common problems in medical researchinter-rater agreement.
Practical statistics for medical research. London: Chapman &Hall; 1991. p. 4048.
36. Godfrey S, UwyyedK, Springer C, et al. Is clinical wheezingreliable as the endpoint
for bronchial challenges inpreschool children? Pediatr Pulmonol 2004;37:193200.
37. Godfrey S, Shlomo C, Avital A, et al. Timing and nature of wheezing at the endpoint
of a bronichial challenge in preschool children. Pediatr Pulmonol 2005;39:2627.
38. Tal A, Sanchez I, Pasterkamp H. Respirosonography in infants with acute bron-
chiolitis. Am J Dis Child 1991;145(12):140510.
39. Rietveld S, Dooijes E. Characteristics and diagnostic significance of wheezes
during exercise-induced airway obstruction in children with asthma. Chest
1996;110(3):62431.
40. Rietveld S, Lous H, Rijssenbeek-Nouwens L. Diagnostics of spontaneous cough
in childhood asthma. Results of continuous tracheal sound recording in the
homes of children. Chest 1998;113(1):504.
41. Rietveld S, Oud M, Rijssenbeek-Nouwens L, et al. Characteristics and diagnostic
significance of spontaneous wheezing in children. J Asthma 1999;36(4):3518.
42. Saglani S, McKenzie S, Bush A, et al. A video questionnaire identifies upper
airway abnormalities in preschool children with reported wheeze. Arch Dis Child
2005;90:9614.
Respiratory Noises 17
Cough
Anne B. Chang, MBBS, MPHTM, FRACP, PhD
The prevalence of chronic cough (5%10%)
1,2
is likely dependent on the setting, age
of the cohort studied, instrument used, and definition of chronic cough.
3
Cough as
a symptomis almost ubiquitous for the entire respiratory system, ranging fromuncom-
plicated minor respiratory tract infections (RTI) to major illnesses, such as cystic fibro-
sis. Rarely, it may be a symptom of extrapulmonary disease, such as cardiac
abnormalities. Most acute cough in children is related to RTIs. Not surprisingly, cough
is often trivialized. Cough, however, especially when chronic, significantly impacts on
parents quality-of-life scores.
4,5
THE BURDEN AND BRIEF PATHOPHYSIOLOGYOF COUGH
The burden of cough is also reflected in the billions of dollars spent annually on over-
the-counter (OTC) cough medications,
6
and the number of consultations sought for
cough. In an Australian study, the number of medical consultations for coughing illness
in the last 12 months was high: more than 80% of children had greater than or equal to
five doctor visits, and 53% had greater than 10.
5
Parents of children with chronic
cough did not have symptoms of anxiety or depression but were stressed.
5
This is
in contrast to adults with chronic cough, which is associated with the presence of de-
pression and anxiety.
7,8
Clinicians need to be cognizant of the stress parents have
when dealing with children with chronic cough. The reasons for parental fears and
concerns included cause of the cough, fear of choking, and long-term respiratory
damage.
1,5,9
Physiologically, cough has three phases: (1) inspiratory, (2) compressive, and (3) ex-
piratory.
10
The inspiratory phase consists of inhaling a variable amount of air, which
serves to lengthen the expiratory muscles, optimizing the length-tension relationship.
The compressive phase consists of a very brief (200 millisecond) closure of the glottis
to maintain lung volume as intrathoracic pressure builds (up to 300 mm Hg in adults)
because of isometric contraction of the expiratory muscles against a closed glottis.
The expiratory phase starts with opening of the glottis, releasing a brief (3050
A.B. Chang is funded by the Royal Childrens Hospital Foundation and the National Health and
Medical Research Council, Australia.
Menzies School of Health Research, Charles Darwin University, Queensland Childrens Respira-
tory Centre, Royal Childrens Hospital, Herston Road, Brisbane, Queensland 4029, Australia
E-mail address: annechang@ausdoctors.net
KEYWORDS
Cough
Evidence-based medicine
Children
Systematic review
Clinical evaluation
Protocol
Pediatr Clin N Am 56 (2009) 1931
doi:10.1016/j.pcl.2008.10.002 pediatric.theclinics.com
0031-3955/08/$ see front matter 2009 Elsevier Inc. All rights reserved.
millisecond) supramaximal expiratory flow
11
(up to 12 L/s in adults, also termed the
cough spike) followed by lower (34 L/s) expiratory flows lasting a further 200 to
500 millisecond.
10
Dynamic compression of the airways occurs during the expiratory
phase and the high-velocity expulsion of gas (air) sweeps airway debris along. Airway
debris and secretions are also swept proximally by ciliary activity. Cough also
enhances mucociliary clearance in both healthy individuals and those with lung
disease.
12
Cough can be voluntarily initiated or suppressed, except when it is part of the laryn-
geal expiratory reflex when the larynx is mechanically stimulated by foreign materials.
Physiologists describe two basic types of cough: laryngeal cough (a true reflex, also
known as expiratory reflex) and tracheobronchial cough. Laryngeal cough protects
the airways from airway aspiration. Tracheobronchial cough is initiated distal to the
larynx and can be volitional. It is primarily stimulated by chemoreceptors in the lower
airways and can also be mechanically stimulated.
3
The primary function of tracheo-
bronchial cough is airway clearance and maintenance of the mucociliary apparatus.
It has been argued that differentiating the types of cough and what constitutes as
a cough is important.
13
Clinicians remain certain, however, what cough is in the clinical
setting.
The knowledge of cough neurophysiology has significantly advanced in recent
years, although much of the work is based on animal models and may have limited ap-
plicability to humans because significant interspecies differences exist.
14
Readers are
referred to recent reviews
1417
for in-depth aspects of cough-related neurophysiology.
As a gross oversimplification, the cough pathway can be compartmentalized to the af-
ferent arms (from cough stimulus to the respiratory center) and efferent arms (from re-
spiratory center to respiratory muscles, larynx, and pelvic muscles) of the cough
pathway; they are likely to be influenced by a bidirectional feedback loop, but this
has not yet been clearly established. Receptors involved in cough are terminations
of vagal afferents in airway mucosa and submucosa.
14,18,19
These afferent receptors
have different sensitivity to different stimuli and are unequally distributed in the air-
ways; generally, the larynx and proximal large airways are more mechanosensitive
and less chemosensitive than peripheral large airways. The existence of distinct cough
receptors, widely assumed to be present and first proposed by Widdicombe,
20
was
only recently proved.
15,18
Generation of action potentials (depolarization of the termi-
nal membrane) from these receptors is subclassified into ionotropic receptors (they
cause generator potentials by acting on ligand-gated ion channels) and metabotropic
receptors (they act indirectly on ligand-gated ion channels by G-protein coupled
receptors).
17,21
These cough and airway receptors mediated through the vagus nerve, jugular, and
nodose ganglions extend to the nucleus tractus solitaris, which is the first central ner-
vous system synaptic contact of these afferent fibers.
22
Second-order neurons from
the nucleus tractus solitaris have polysynaptic connections with the central cough
generator, which is also the respiratory pattern generator.
16,22
Nucleus tractus solitaris
is postulated to be the site of greatest modulatory influence and plasticity. The mech-
anisms underpinning chronic cough have been likened to that of chronic pain,
3
and
increased neurogenic markers have been described in children with increased cough
receptor sensitivity.
23
The intrathoracic pressure and effects of it generated by cough
may also perpetuate the chronic cough cycle as suggested by a recent animal study
that showed pressure effects enhance cough sensitivity.
24
An effective cough is dependent on generation of high linear velocities and interac-
tion between flowing gas and mucus in the airways.
10
This is dependent on the integ-
rity of the mechanisms described previously. Other physical characteristics also
Chang 20
influence cough efficiency: adequate airway caliber (efficiency decreased in presence
of flow-limitation
25
[eg, severe tracheomalacia]); mucous physical properties (sputum
tenacity, adhesiveness, water content, and so forth);
10
and respiratory muscle
strength.
10
The importance of the integrity of the cough reflex is reflected when it is
impaired. Aspiration lung disease occurs in those with a dysfunctional laryngeal reflex
(eg, central neurologic problems and multiple organ dysfunction).
26
When the muscu-
lar apparatus for an effective cough is impaired (eg, muscular dystrophy), recurrent
mucus retention and atelectasis occurs.
MANAGEMENT OF THE SYMPTOM OF COUGH
The overall management of cough entails an evaluation for the following: (1) etiology,
which includes assessing if further tests or treatment are required; (2) defining exac-
erbation factors (eg, exposure to environmental tobacco smoke); and (3) defining
the effect on the child and parents.
Defining the Etiology of the Cough
The most likely etiology depends on the setting, selection criteria of children studied,
follow-up rate, depth of clinical history, examination, and investigations performed. In
defining the etiology, it is helpful to define cough types in accordance to different con-
structs. Pediatric cough can be classified in several constructs based on (1) timeframe
(acute, chronic); (2) likelihood of an identifiable underlying primary etiology (specific
and nonspecific cough); and (3) characteristic (moist versus dry). For clinical practical-
ity timeframe is commonly used, divided into acute (<2 weeks), subacute (24 weeks),
and chronic (>4 weeks) cough. There are no studies that have clearly defined when
cough should be defined as chronic (variably defined from >48 weeks).
2729
Cough
related to an upper RTI resolves within 10 days in 50% of children and by 25 days
in 90%;
30
arguably, childhood chronic cough should be defined as persistent daily
cough of greater than 4 weeks. Chronic cough is further subdivided into specific
cough (cough associated with other symptoms and signs that are suggestive of an as-
sociated or underlying problem) and nonspecific cough (dry cough in the absence of
any identifiable respiratory disease or known etiology). These classifications, however,
are not mutually exclusive.
Acute cough and expected cough
Although acute RTIs are the most common cause of acute cough in children, all chil-
dren should be assessed for symptoms and signs of more serious cause, such as
inhaled foreign body. In 8% to 12% of children with upper RTIs complications
develop.
30
These conditions are discussed elsewhere in this issue.
Expected cough is the presence of cough in situations where cough is the norm,
such as during an acute respiratory infection. In most children, acute cough is self-lim-
iting and treatment, if any, should be directed at the cause rather than the symptom of
cough. OTC medications for cough confer no benefit in the symptomatic control of
cough or on the sleep pattern of children or parents and may cause harm. Steam
inhalation, vitamin C, zinc, and Echinacea for upper RTI have little benefit, if any, for
symptomatic relief of cough. Systematic reviews have also shown that oral or inhaled
b
2
-agonists also confer no benefit in children with acute cough and no evidence of air-
flow obstruction. Antimicrobials are nonbeneficial in acute cough associated with
colds. In contrast, honey (0.52 teaspoons depending on age) has been shown to
be useful in reducing nocturnal cough and improving sleep quality of parents and chil-
dren with an acute upper RTI-associated cough (Table 1).
31
Cough 21
Table1
Recommendations for possible interventions for nonspecific cough in children
Therapy Recommendation Grade
a
Type and Strength of Evidence Time to Response
b
Antihistamines
Nonsedating Not generally recommended unless
symptoms of rhinitis coexist
Moderate SR with RCTs
57,58
1 wk
Sedating Sedating antihistamines should
not be used, strong
Not relevant
Antimicrobials For wet cough only, strong High SR with RCTs
40
12 wk
Asthma-type therapy
Cromones Not recommended, weak Very low SR with single open trial
59
2 wk
Anticholinergics Not recommended, weak Very low SR, no studies in children RCTs
60
No data
Inhaled CS Not generally recommended
unless symptoms of asthma
present, strong
Moderate SR with RCTs
50,51
24 wk
Oral CS Not recommended, weak Low No data
b
2
-agonist (oral or inhaled) Not generally recommended
unless symptoms of asthma
present, weak
Moderate SR with RCTs
61
RCT
50
Not relevant
Theophylline Not recommended, weak Very low SR, no studies
62
12 wk
Leukotriene receptor antagonist Not recommended unless
symptoms of asthma
present, weak
Very low SR, observational study
63
23 wk
C
h
a
n
g
2
2
GERD therapy
Motility agents Not recommended as empiric
therapy, weak
Very low SR with single trial
64
Not relevant
Acid suppression Not recommended as empiric
therapy, weak
Very low SR with no RCTs in children
64
Food-thickening or
antireflux formula
Consider if other symptoms of reflux
present (infants only), weak
Moderate SR with RCTs
64
1 wk
Fundoplication Systematic review
64
Herbal antitussive therapy Not recommended, weak Very low No data
Nasal therapy
Nasal steroids Not generally recommended unless
symptoms of rhinitis coexist, weak
Low RCT
65
Beneficial when combined
with antibiotics for sinusitis
66
12 wk
Other nasal sprays Not recommended, strong Very low No data
Over-the-counter cough medications Not recommended, strong High SR with RCTs
57,6769
Not relevant
Other therapies
Steam, vapor, rubs Consider rubs but not vapor or steam,
weak
Low No data
Honey Recommended if no contraindications
for using of honey, strong
Moderate Single RCT on acute cough
31
1 d
Physiotherapy Not recommended unless cough related
to suppurative lung disease, weak
Very low No data in cough that is unrelated
to suppurative-like lung diseases
Abbreviations: CS, corticosteroids; GERD, gastro-esophageal reflux disease; RCT, randomized controlled trials; SR, systematic review.
a
Grading of evidence and recommendations.
70
b
Length in time for cough to resolve or substantially improve as reported by trialists.
C
o
u
g
h
2
3
Subacute and chronic cough
Chronic cough differs from acute cough in its management and etiologic factors. The
timeframe chosen for chronic cough is similar in the Australian
27
and American
28
guidelines, but differs from the British guidelines.
29
The difference likely reflects the
lack of evidence. It is unknown whether the primary stimulus for chronic cough in
many children is identical to that for acute cough. Further, it is unknown why the cough
associated with common acute viral upper RTIs resolves in most, yet persists in some.
Presumably, however, both the specific microbe (eg, cough is more likely to be pro-
longed after a potent respiratory infection, such as pertussis) or host factors (eg, ge-
netic predisposition to bronchitis) play a role. Unfortunately, there are no studies that
have clearly defined when cough should be defined as chronic. Studies have shown
that cough related to upper RTIs resolves within 1 to 3 weeks in greater than 90%
of children.
30,32
It is logical to define chronic cough as daily cough lasting greater
than 4 weeks; published definitions of chronic cough in children have varied from 3
to 12 weeks.
33
In contrast, the current definition of chronic cough in adults is 8 weeks.
The pediatric definition is based on the natural history of acute upper RTIs in chil-
dren
30,32
and the knowledge that pediatric respiratory illness has important differ-
ences than that in adults.
33
For example, such conditions as a missed foreign body,
which is more common in children (especially in those aged %5 years), can lead to
permanent lung damage.
34
Classically recognizable cough
Certain cough characteristics, such as croupy or brassy cough, are classically
taught to point to specific etiologies in children. Data on the sensitivity and specificity
of each classic recognizable cough type are limited; the data for brassy cough (for tra-
cheomalacia diagnosed at bronchoscopy) were 0.57 and 0.81, respectively.
35
Kappa
value for interobserver agreement for brassy cough was good at 0.79 (95% confi-
dence interval [CI], 0.730.86).
35
Although a pertussis-like cough in children is gener-
ally caused by Bordetella pertussis infection, it may also be caused by adenovirus,
parainfluenza viruses, respiratory syncytial virus, and mycoplasma.
36
By contrast,
the quality of cough has been shown to be of little use in adults.
37
Chronic productive
purulent cough is always pathologic. In obtaining a history in a child with chronic
cough, questions specific for classically recognizable cough, such as an exposure
to illness history (eg, pertussis and tuberculosis), should be obtained.
Wet-moist-productive cough versus dry cough
Even when airway secretions are present, young children rarely expectorate sputum;
hence, wet-moist cough is the preferable term rather than productive cough.
38,39
The distinction of dry and wet-moist cough has been shown to be both valid and
reliable. In a study of 106 children, cough quality (wet or dry) assessed by clinicians
had good agreement with parents assessment (K 5 0.75; 95% CI, 0.580.93), and
had good sensitivity (0.75) and specificity (0.79), when compared with bronchoscopy
findings.
35
The use of wet versus dry cough for predicting etiology of cough or re-
sponse to treatment has not been shown in children, except in protracted bronchitis.
40
Specific and nonspecific chronic cough
Clinical signs and symptoms that are suggestive of an underlying pulmonary or sys-
temic disorder are termed specific cough pointers (Box 1).
27
When any of these
pointers are present, the cough is referred to as specific cough. If specific cough
pointers are present, further investigations and management of the primary pulmonary
pathology is usually warranted. If not, a counsel, watch, wait, and review approach is
suggested. This approach is suggested for nonspecific cough (dry cough in the
Chang 24
absence of specific cough pointers). Such cough is more likely to undergo natural res-
olution.
41
A dry cough may be the early phase of a wet cough,
42
however, and children
should be reviewed and attention to exacerbation factors and parental concerns (see
later) are warranted.
In selected children with nonspecific cough, diagnoses with simple treatment op-
tions, (eg, asthma and complications of upper RTIs, such as sinusitis and bronchitis)
may be considered. The evidence for the association between asthma
3,43
and upper
airway disorders and cough is not as straightforward in children, however, as it is in
adults.
33,44
The use of isolated cough as a marker of asthma is controversial with
more recent evidence (clinical and community epidemiologic studies) showing that
in most children, isolated cough does not represent asthma.
3,45
Investigations
As a minimum, all children with chronic cough should have a spirometry (if age appro-
priate) and chest radiograph performed.
27,28
The validity of this has been shown.
41
When a chest radiograph taken for chronic cough is abnormal, the odds ratio of an
specific etiology was 3.16 (95% CI, 1.327.62).
41
Other tests to identify the etiology
of nonspecific cough have limited applicability in pediatrics. Identification of airway
hyperresponsiveness, diagnostic for asthma in adults, is of limited use in children
because of interpretation difficulties, and reliable tests can only be performed in older
children in whom cough is less common. The three most common causes of chronic
cough in adults (gastroesophageal reflux disease, asthma, and upper airways syn-
drome)
46
are not as common in children.
47
Increased cough sensitivity is found in
most conditions causing chronic cough but its use is limited to research.
28
Except when classical asthma is the etiology, children with specific cough usually
require additional tests (chest high-resolution CT scan, bronchoscopy, video fluoros-
copy, echocardiograph, sleep polysomnography, nuclear medicine scans,
Box1
Pointers for presence of specific cough
Auscultatory findings (wheeze, crepitations or crackles, differential breath sounds)
Cough characteristics (eg, cough with choking, cough quality, cough starting from birth)
Cardiac abnormalities (including murmurs)
Chest pain
Chest wall deformity
Daily moist or productive cough
Digital clubbing
Dyspnea (exertional or at rest)
Exposure to pertussis, tuberculosis, and so forth
Failure to thrive
Feeding difficulties or dysphagia (including choking or vomiting)
Hemoptysis
Immune deficiency
Medications or drugs (angiotensin-converting enzyme inhibitor)
Neurodevelopmental abnormality
Recurrent pneumonia
Cough 25
immunologic assessment, and so forth). The role of these tests for evaluation of lung
disease is beyond the scope of this article because it encompasses the entire spec-
trum of pediatric respiratory illness.
MEDICATIONS
Treatment for subacute and chronic cough should be etiologically based, and that for
specific cough is beyond the scope of this article. Cough is subjected to the period-
effect (ie, spontaneous resolution of cough); the benefit of placebo treatment for
cough has been reported to be as high as 85% and nonplacebo-controlled interven-
tion studies have to be interpreted with caution.
3
Evidence (or lack of) on treatment tri-
als for nonspecific cough are summarized in Table 1. Systematic reviews have
concluded that OTC cough remedies have little benefit in the symptomatic control
of childhood cough. Significant morbidity and mortality
48
from OTC cough remedies
can occur and OTC drugs are common unintentional ingestions in children aged
less than 5 years.
49
Cochrane reviews on symptomatic treatment of cough have
shown that diphenhyramine is not beneficial for pertussis-related cough; cromones
and anticholinergics have little, if any, role in nonspecific chronic childhood cough;
and 10 days of antimicrobials reduces persistent cough in children with chronic nasal
discharge but benefits are modest (number needed to treat was 8). Antimicrobials may
be indicated for subacute and chronic moist cough; two randomized controlled trials
(RCTs) showed predominance of Moraxella catarrhalis. Meta-analysis on antimicro-
bials for acute bronchitis in older children (aged >8 years) and adults showed a small
benefit of 0.58 days but with significantly more adverse events. Systematic review of
uncomplicated sinusitis in children showed that the clinical improvement rate was
88% with antimicrobial and 60% on no antimicrobial. There are only two published
RCTs on inhaled corticosteroids for nonspecific cough in children and both groups
cautioned against prolonged use.
50,51
In the North American guidelines for pediatric
gastroesophageal reflux, the conclusion on cough and gastroesophageal reflux
disease section was there is insufficient evidence and experience in children for a uni-
form approach to diagnosis and treatment.
52
If medications are trialed for nonspecific cough, the child should be reviewed and
time to response considered. For example, in asthma-related cough, earlier non-
RCT studies in adults and children that used medications for asthma for the era (ie,
nonsteroidal anti-inflammatory drugs, theophylline, terbutaline, major tranquillizers)
reported that cough completely resolved by 2 to 7 days.
3
Time to response is defined
as the expected length of time cough resolution occurred in studies where the cough
treated was related to the etiology defined.
Defining Exacerbation Factors
When reviewing any child with cough irrespective of the etiology, exacerbation factors
should be explored, although no RCTs have examined the effect of cessation of
environmental pollutants on cough. There is little doubt that children with environmen-
tal tobacco smoke exposure have increased risk of having chronic
53,54
and recurrent
cough.
55
The American Academy of Pediatrics policy on tobacco includes recommen-
dations for tobacco cessation.
56
Other exacerbation factors include exposure to
pollutants and secondary gains from having a cough.
Defining Effect on Child and Parent
Parents presenting to doctors for their childrens cough have significant concerns that
causes parental stress.
5
The most significant concerns and worries expressed by
Chang 26
parents are feelings of frustration, upset, sleepless nights, awakened at night, help-
lessness, stress, and feeling sorry for the child. Items that bothered the parents
most were the cause of cough, cough relating to a serious illness, child not sleeping
well, and cough causing damage.
5
Previous studies have described parental fears
Box 2
When a child with chronic cough presents
1. A complete medical examination with particular attention to the cardiorespiratory systems
and a focus on
a. The clinical pattern
Characteristic cough (eg, pertussis, tracheomalacic cough, see Box1)
Wet or dry cough? Protracted bronchitis?
Presence of specific cough pointers to differentiate specific from nonspecific cough,
(Table 2) (GRADE, moderate; Level of evidence, cohort studies)
41,47
b. Presence of exacerbation factors (eg, environmental tobacco smoke, curtailment of
physical activity)
c. Effect of the cough on the child and parents, and explore their concerns (see previously)
(GRADE, moderate; Level of evidence, cohort studies)
2. All should undergo
Chest radiograph
Spirometry (if aged >3 years) (GRADE, moderate; Level of evidence, cohort studies)
3. They should be further investigated and likely require referral if
Specific cough pointers are present (other than asthma) (seeTable 2)
Cough has not resolved with treatment trials (GRADE, moderate; Level of evidence, cohort
studies)
4. A wait, reassess, and review approach is recommended for children with nonspecific
cough because medications are generally not efficacious for nonspecific cough (seeTable1).
If medications are trialed, a reassessment is recommended in 2 to 3 weeks, which is the time
to response for most medications.
27,28
(GRADE, moderate; Level of evidence, cohort studies
and RCTs)
Table 2
Characteristic or classical types of cough
Cough Type Suggested Underlying Process
Barking or brassy cough Croup, tracheomalacia, habit cough
Honking Psychogenic
Paroxysmal ( inspiratory whoop) Pertussis and parapertussis
Staccato Chlamydia in infants
Cough productive of casts Plastic bronchitis or asthma
Chronic wet cough in mornings only Suppurative lung disease
Data from Chang AB, Glomb WB. Guidelines for evaluating chronic cough in pediatrics: ACCP
evidence-based clinical practice guidelines. Chest 2006;129:260S83S; and Chang AB. Causes,
assessment and measurement in children. In: Chung KF, Widdicombe JG, Boushey HA, editors.
Cough: causes, mechanisms and therapy. London: Blackwell Science; 2003. p. 5773.
Cough 27
of their child dying from choking, asthma attack, or cot death, and permanent chest
damage, disturbed sleep, and relief of discomfort.
1,9
These concerns are often not ap-
preciated by health professionals and exploration of parental expectations and fears is
valuable when managing a child with a chronic cough.
Providing parents with information on the expected time length of resolution of RTIs
may reduce anxiety in parents and the need for medication use. Parental and profes-
sional expectations and doctors perception of patients expectations influences con-
sulting rates and prescription of medications in RTIs. Educational input is best done
with consultation about the childs specific condition because written information
without consultation has only modest benefit in changing perceptions and behavior.
It is also known that information available from the Internet provides incorrect advice
on the home management of cough in children.
SUMMARY
Box 2 lists the steps to take when a child with chronic cough presents to the clinician.
REFERENCES
1. Faniran AO, Peat JK, Woolcock AJ. Persistent cough: is it asthma? Arch Dis Child
1998;79:4114.
2. Faniran AO, Peat JK, Woolcock AJ. Measuring persistent cough in children in
epidemiological studies: development of a questionnaire and assessment of
prevalence in two countries. Chest 1999;115:4349.
3. Chang AB. State of the art: cough, cough receptors, and asthma in children.
Pediatr Pulmonol 1999;28:5970.
4. Newcombe PA, Sheffield JK, Juniper EF, et al. Development of a parent-proxy
cough-specific QOL questionnaire: clinical impact vs psychometric evaluations.
Chest 2008;133:38695.
5. Marchant JM, Newcombe PA, Juniper EF, et al. What is the burden of chronic
cough for families? Chest 2008;134:3039.
6. Irwin RS. Introduction to the diagnosis and management of cough: ACCP evi-
dence-based clinical practice guidelines. Chest 2006;129:25S7S.
7. Dicpinigaitis PV, Tso R, Banauch G. Prevalence of depressive symptoms among
patients with chronic cough. Chest 2006;130:183943.
8. Ludviksdottir D, Bjornsson E, Janson C, et al. Habitual coughing and its associ-
ations with asthma, anxiety, and gastroesophageal reflux. Chest 1996;109:
12628.
9. Cornford CS, Morgan M, Ridsdale L. Why do mothers consult when their children
cough? Fam Pract 1993;10:1936.
10. McCool FD. Global physiology and pathophysiology of cough. Chest, in press.
11. Bennett WD, Zeman KL. Effect of enhanced supramaximal flows on cough
clearance. J Appl Phys 1994;77:157783.
12. Oldenburg FA, Dolovich MB, Montgomery JM, et al. Effects of postural drainage,
exercise and cough on mucus clearance in chronic bronchitis. Am Rev Respir Dis
1979;120:73945.
13. Widdicombe J, Fontana G. Cough: whats in a name? Eur Respir J 2006;28:105.
14. Canning BJ. Anatomy and neurophysiology of the cough reflex. Chest 2006;
129(Suppl 1):33S47S.
15. Canning BJ, Mazzone SB, Meeker SN, et al. Identification of the tracheal and
laryngeal afferent neurones mediating cough in anaesthetized guinea-pigs.
J Physiol 2004;557:54358.
Chang 28
16. Shannon R, Baekey DM, Morris KF, et al. Production of reflex cough by brainstem
respiratory networks. Pulm Pharmacol Ther 2004;17:36976.
17. Canning BJ. Anatomy and neurophysiology of the cough reflex: ACCP evidence-
based clinical practice guidelines. Chest 2006;129:33S47S.
18. Mazzone SB. Sensory regulation of the cough reflex. Pulm Pharmacol Ther 2004;
17:3618.
19. Undem BJ, Carr MJ, Kollarik M. Physiology and plasticity of putative cough fibres
in the Guinea pig. Pulm Pharmacol Ther 2002;15:1938.
20. Widdicombe J. The race to explore the pathway to cough: who won the silver
medal? Am J Respir Crit Care Med 2001;164:72930.
21. Lee MG, Kollarik M, Chuaychoo B, et al. Ionotropic and metabotropic receptor
mediated airway sensory nerve activation. Pulm Pharmacol Ther 2004;17:
35560.
22. Bonham AC, Sekizawa S, Joad JP. Plasticity of central mechanisms for cough.
Pulm Pharmacol Ther 2004;17:4537.
23. Chang AB, Gibson PG, Ardill J, et al. Calcitonin gene-related peptide relates to
cough sensitivity in children with chronic cough. Eur Respir J 2007;30:6672.
24. Hara J, Fujimura M, Ueda A, et al. Effect of pressure stress applied to the airway
on cough reflex sensitivity in guinea pigs. Am J Respir Crit Care Med 2008;177:
58592.
25. Smaldone GC, Messina MS. Flow limitation, cough, and patterns of aerosol depo-
sition in humans. J Appl Physiol 1985;59:51520.
26. Weir K, McMahon S, Barry L, et al. Oropharyngeal aspiration and pneumonia in
children. Pediatr Pulmonol 2007;42:102431.
27. Chang AB, Landau LI, van Asperen PP, et al. The Thoracic Society of Australia
and New Zealand. Position statement. Cough in children: definitions and clinical
evaluation. Med J Aust 2006;184:398403.
28. Chang AB, Glomb WB. Guidelines for evaluating chronic cough in pediatrics:
ACCP evidence-based clinical practice guidelines. Chest 2006;129:260S83S.
29. Shields MD, Bush A, Everard ML, et al. British thoracic society guidelines recom-
mendations for the assessment and management of cough in children. Thorax
2008;63:iii1iii15.
30. Hay AD, Wilson A, Fahey T, et al. The duration of acute cough in pre-school chil-
dren presenting to primary care: a prospective cohort study. Fam Pract 2003;20:
696705.
31. Paul IM, Beiler J, McMonagle A, et al. Effect of honey, dextromethorphan, and no
treatment on nocturnal cough and sleep quality for coughing children and their
parents. Arch Pediatr Adolesc Med 2007;161:11406.
32. Hay AD, Wilson AD. The natural history of acute cough in children aged 0 to
4 years in primary care: a systematic review. Br J Gen Pract 2002;52:4019.
33. Chang AB. Cough: are children really different to adults? Cough 2005;1:7.
34. Karakoc F, Karadag B, Akbenlioglu C, et al. Foreign body aspiration: what is the
outcome? Pediatr Pulmonol 2002;34:306.
35. Chang AB, Eastburn MM, Gaffney J, et al. Cough quality in children: a comparison
of subjective vs. bronchoscopic findings. Respir Res 2005;6:3.
36. Wirsing von Konig CH, Rott H, Bogaerts H, et al. A serologic study of organisms
possibly associated with pertussis-like coughing. Pediatr Infect Dis J 1998;17:
6459.
37. Mello CJ, Irwin RS, Curley FJ. Predictive values of the character, timing, and com-
plications of chronic cough in diagnosing its cause. Arch Intern Med 1996;156:
9971003.
Cough 29
38. Chang AB, Masel JP, Boyce NC, et al. Non-CF bronchiectasis-clinical and HRCT
evaluation. Pediatr Pulmonol 2003;35:47783.
39. De Jongste JC, Shields MD. Chronic cough in children. Thorax 2003;58:
9981003.
40. Marchant JM, Morris P, Gaffney J, et al. Antibiotics for prolonged moist cough in
children. Cochrane Database Syst Rev 2005:4.
41. Marchant JM, Masters IB, Taylor SM, et al. Utility of signs and symptoms of
chronic cough in predicting specific cause in children. Thorax 2006;61:6948.
42. Chang AB, Faoagali J, Cox NC, et al. A bronchoscopic scoring system for airway
secretions-airway cellularity and microbiological validation. Pediatr Pulmonol
2006;41:88792.
43. Chang AB, Redding GJ, Everard ML. Chronic wet cough: protracted bronchitis,
chronic suppurative lung disease and bronchiectasis. Pediatr Pulmonol 2008;43:
51931.
44. Kemp AS. Does post-nasal drip cause cough in childhood? Paediatr Respir Rev
2006;7:315.
45. McKenzie S. Cough: but is it asthma? Arch Dis Child 1994;70:12.
46. Irwin RS, Baumann MH, Bolser DC, et al. Diagnosis and management of cough
executive summary: ACCP evidence-based clinical practice guidelines. Chest
2006;129:1S23S.
47. Marchant JM, Masters IB, Taylor SM, et al. Evaluation and outcome of young chil-
dren with chronic cough. Chest 2006;129:113241.
48. Gunn VL, Taha SH, Liebelt EL, et al. Toxicity of over-the-counter cough and cold
medications. Pediatrics 2001;108:E52.
49. Chien C, Marriott JL, Ashby K, et al. Unintentional ingestion of over the counter
medications in children less than 5 years old. J Paediatr Child Health 2003;39:
2649.
50. Chang AB, Phelan PD, Carlin J, et al. Randomised controlled trial of inhaled sal-
butamol and beclomethasone for recurrent cough. Arch Dis Child 1998;79:611.
51. Davies MJ, Fuller P, Picciotto A, et al. Persistent nocturnal cough: randomised
controlled trial of high dose inhaled corticosteroid. Arch Dis Child 1999;81:3844.
52. Rudolph CD, Mazur LJ, Liptak GS, et al. Guidelines for evaluation and treatment
of gastroesophageal reflux in infants and children: recommendations of the North
American Society for Pediatric Gastroenterology and Nutrition. J Pediatr Gastro-
enterol Nutr 2001;2(Suppl 32):S131.
53. Holscher B, Heinrich J, Jacob B, et al. Gas cooking, respiratory health and white
blood cell counts in children. Int J Hyg Environ Health 2000;203:2937.
54. Jaakkola JJ, Jaakkola MS. Effects of environmental tobacco smoke on the respi-
ratory health of children. Scand J Work Environ Health 2002;2(Suppl 28):7183.
55. Hermann C, Westergaard T, Pedersen BV, et al. A comparison of risk factors for
wheeze and recurrent cough in preschool children. Am J Epidemiol 2005;162:
34550.
56. American Academy of Pediatrics. Tobaccos toll: implications for the pediatrician.
Pediatrics 2001;107:7948.
57. Schroeder K, Fahey T. Should we advise parents to administer over the counter
cough medicines for acute cough? Systematic review of randomised controlled
trials. Arch Dis Child 2002;86:1705.
58. Chang AB, Peake J, McElrea M. Anti-histamines for prolonged non-specific
cough in children. Cochrane Database Syst Rev 2008:2.
59. Chang AB, Marchant JM, Morris P. Cromones for prolonged non-specific cough
in children. Cochrane Database Syst Rev 2004:1.
Chang 30
60. Chang AB, McKean M, Morris P. Inhaled anti-cholinergics for prolonged non-
specific cough in children. Cochrane Database Syst Rev 2003:4.
61. Smucny JJ, Flynn CA, Becker LA, et al. Are beta2-agonists effective treatment for
acute bronchitis or acute cough in patients without underlying pulmonary dis-
ease? A systematic review. J Fam Pract 2001;50:94551.
62. Chang AB, Halstead RA, Petsky HL. Methylxanthines for prolonged non-specific
cough in children. Cochrane Database Syst Rev 2005:3.
63. Chang AB, Winter D, Acworth JA. Leukotriene receptor antagonist for prolonged
non-specific cough in children. Cochrane Database Syst Rev 2006:2.
64. Chang AB, Lasserson T, Gaffney J, et al. Gastro-oesophageal reflux treatment for
prolonged non-specific cough in children and adults. Cochrane Database Syst
Rev 2005:2.
65. Gawchik S, Goldstein S, Prenner B, et al. Relief of cough and nasal symptoms
associated with allergic rhinitis by mometasone furoate nasal spray. Ann Allergy
Asthma Immunol 2003;90:41621.
66. Barlan IB, Erkan E, Bakir M, et al. Intranasal budesonide spray as an adjunct to
oral antibiotic therapy for acute sinusitis in children. Ann Allergy Asthma Immunol
1997;78:598601.
67. Schroeder K, Fahey T. Over-the-counter medications for acute cough in children
and adults in ambulatory settings. Cochrane Database Syst Rev 2004:2.
68. Paul IM, Yoder KE, Crowell KR, et al. Effect of dextromethorphan, diphenhydra-
mine, and placebo on nocturnal cough and sleep quality for coughing children
and their parents. Pediatrics 2004;114:e8590.
69. Chang AB. Causes, assessment and measurement in children. In: Chung KF,
Widdicombe JG, Boushey HA, editors. Cough: causes, mechanisms and therapy.
London: Blackwell Science; 2003. p. 5773.
70. GRADE Working Group. Grading quality of evidence and strength of recommen-
dations. BMJ 2004;328:14907.
Cough 31
Percepti ons and
Pathophysi ol ogy of
Dyspnea and Exerci se
I ntol erance
Miles Weinberger, MD*, MutasimAbu-Hasan, MD
WHAT IS DYSPNEA?
Dsypnea is derived from the Latin dyspnoea, from Greek dyspnoia from dyspnoos,
and is often described by patients as shortness of breath. It involves the perception
of difficulty or painful breathing. It is a common symptom of numerous medical
disorders, but psychologic factors can also contribute to the sensation of dyspnea.
Dyspnea on exertion, or exertional dyspnea, indicates dyspnea that occurs or worsens
during physical activity. This article discusses the physiology, etiologies, evaluative
procedures, and treatment of dyspnea.
PATHOPHYSIOLOGYOF DYSPNEA
Dyspnea is a complex psycho-physiologic sensation that occurs in a variety of cardio-
pulmonary diseases (Fig. 1). Increased work of breathing occurs when there is an
increase in mechanical loading of the respiratory system, both resistive and elastic.
1,2
The sensation of dyspnea requires intact afferent and efferent pathways for the full
perception of the neuromechanical dissociation between the respiratory effort
attempted and the work actually accomplished.
3
The sensation is triggered or accen-
tuated by a variety of receptors located in the chest wall, respiratory muscles, lung
parenchyma, carotid body, and brain stem.
4
The sensation of dyspnea is stronger in
patients with higher scores for anxiety and has been reported in patients with anxiety
disorders with no cardiopulmonary disease.
59
These observations demonstrate the
importance of cerebral cognition in this complex symptom.
Pediatric Allergy and Pulmonary Division, Pediatrics Department, University of Iowa Childrens
Hospital, University of Iowa College of Medicine, 200 Hawkins Drive, Iowa City IA 52242, USA
* Corresponding author.
E-mail address: miles-weinberger@uiowa.edu (M. Weinberger).
KEYWORDS
Dyspnea
Exercise
Exercise testing
Respiratory distress
Ventilation
Pediatr Clin N Am 56 (2009) 3348
doi:10.1016/j.pcl.2008.10.015 pediatric.theclinics.com
0031-3955/08/$ see front matter 2009 Elsevier Inc. All rights reserved.
CLINICAL MANIFESTATIONS OF DYSPNEA
People describe dyspnea in different ways. They certainly dont use the word dysp-
nea. Instead, people will say things such as, I get tired easily, I have trouble catch-
ing my breath, I cant take a deep breath, my throat gets tight, my chest gets
tight, I cant keep up with the other kids, or simply I get short of breath. Some
of the differences appear to be cultural.
10
Complaints of dyspnea may occur sponta-
neously and unpredictably, in certain environments or during certain activities. They
can be episodic or continuous.
Other differences relate to perception.
11
Differences in perception influence the
recognition of asthma. Children with asthma symptoms that have not been recognized
by their parents have been shown to perceive dyspnea less readily than those whose
asthma has been recognized by their parents.
12
Patients with chronic severe obstruc-
tive lung disease, such as asthma and chronic obstructive pulmonary disease,
experience adaptation to the sensation of dyspnea. Such patients typically rate their
feeling of breathlessness low for severe degrees of obstruction when compared
with the acutely ill and with patients with mild chronic disease.
13
Of particular
Fig.1. Cardiopulmonary sites that can cause dyspnea. (From Collins RD. Differential diagnosis
in primary care. 4th edition. Philadelphia: Lippincott Williams & Wilkins; 2008. p. 141; with
permission.)
Weinberger & Abu-Hasan 34
importance is the demonstration that individuals who have experienced near-fatal ep-
isodes from asthma have a diminished perception of dyspnea.
14
When taking a history, it is important to have the patient describe their perception of
dyspnea in as much detail as possible. The level of function or dysfunction associated
with the dyspnea is also important in assessing the clinical manifestations of dyspnea.
In addition to the patients perception, observations should be obtained from parents,
teachers, coaches, or others who have the opportunity to observe the patient for signs
of increased work of breathing.
Interestingly, there is a dissociation between dyspnea and actual respiratory effort.
3
Examples include observations in adults with pulmonary embolism or pulmonary
hypertension who may report breathlessness out of proportion to respiratory effort,
including changes in minute ventilation or pulmonary mechanics. Additionally, induced
hypercapnia has been associated with dyspnea accompanied by actual reduction in
respiratory effort.
3
Thus, the sensation of dyspnea can reflect either actual increased
work of breathing, as in airway obstruction, or the perception of breathlessness, as
occurs with acute hypoxemia or hypercapnia.
The feeling of dyspnea or breathlessness can also occur from panic and hyperven-
tilation attacks, where the perception of difficulty breathing is not accompanied by any
respiratory pathophysiologic abnormality other than the effects of the hyperventilation
itself. Because dyspnea, fromwhatever cause, depends on perception, attempts have
been made to standardize perception. The Borg and the Visual Analog Scales have
been the most commonly used measures of dyspnea.
1517
PHYSICAL FINDINGS ASSOCIATED WITH DYSPNEA
Physical findings of dyspnea can range from none at all to obvious increased work of
breathing manifested by retractions, tachypnea, nasal flaring, use of accessory mus-
cles, and cyanosis. If the dyspnea occurs only during exercise, then reproduction of
the exercise-induced dyspnea may require a formal exercise test to reproduce the
symptom. This provides the opportunity to observe the patient during the dyspnea
and measure cardiopulmonary physiology associated with the dyspnea.
Respiratory sounds may include inspiratory stridor, expiratory wheezing, crackles,
or just normal air movement. Identifying respiratory sounds associated with the
dyspnea can be helpful in identifying the physiologic abnormality. Inspiratory sounds
indicate extrathoracic obstruction, while expiratory sounds indicate intrathoracic
obstruction. The pitch of the sounds can also provide clues. Low-pitched inspiratory
sounds are typically from supraglottic obstruction, while high-pitched inspiratory
sounds are more likely to be fromlaryngeal or subglottic narrowing. Expiratory wheez-
ing can be monophonic, representing obstruction of one intrathoracic airway, while
polyphonic expiratory wheezing indicates more diffuse airway involvement. The extent
of the obstruction influences the increased work of breathing to overcome the
narrowing of the specific component of the airway.
PHYSIOLOGIC ABNORMALITIES ASSOCIATED WITH DYSPNEA
Both cardiac and pulmonary disease can be associated with dyspnea. Pulmonary
edema affects lung compliance and gas exchange. Myocarditis affects cardiac output
and limits oxygen delivery to tissues. Pulmonary function testing can differentiate
betweenobstructiveandrestrictivecauses of dyspnea. Obstructivecauses arecharac-
terized by decreases in flow, while restrictive causes are characterized by decreased
lung volumes. Gas exchange abnormalities can be assessed by measurement of oxy-
genation and pCO
2
, while measurement of diffusing capacity can be used to determine
Perceptions and Pathophysiology of Dyspnea 35
if there is a loss of the pulmonary capillary bed, as occurs in interstitial lung disease and
pulmonary fibrosis. Exercise testing with cardiopulmonary monitoring can measure ox-
ygen use, CO
2
production, cardiac function, and ventilatory abnormalities.
EXERCISE-INDUCED DYSPNEA
Exercise-induced dyspnea can be present when cardiac or pulmonary function is
compromised at an earlier stage in the underlying disease than when dyspnea from
those problems occurs at rest. Dyspnea during exercise in patients who otherwise
have no known lung or heart disease is therefore a symptom that warrants investiga-
tion. It might represent a mild abnormality that is manifested only during exercise, in
which increased ventilation and cardiac output are required, or it could be caused
by a distinct pathophysiologic abnormality that is induced only by exercise.
18
Of the
latter, exercise-induced bronchospasm as a manifestation of asthma is the most
widely studied. Its prevalence is very high, but because of poor correlation between
the degree of airway obstruction and the sensation of dyspnea, exercise-induced
bronchospasm is subject to being unrecognized.
1921
However, exercise-induced
asthma is also subject to being over-reported.
22,23
Following are selected cases representing common and uncommon examples of
dyspnea, which demonstrate the diversity of clinical entities that can present with
this symptom.
CASE STUDIES OF DYSPNEA
Case 1
A 10-year-old boy with known asthma comes home from school complaining of
difficulty breathing. His mother observes that he has suprasternal retractions. He is
taken to the local emergency room, where diffuse polyphonic wheezing is heard
and oximetry indicates an O
2
saturation of 93%. Albuterol aerosol is given, his retrac-
tions decrease, his O
2
is now 92%, but he states that he feels better and that it is now
easier to breath. So what was the mechanism for his dyspnea? Central receptors for
hypoxemia? Was he also hypercapneic? Or was it the increased airway resistence
from bronchospasm?
It is unlikely that the modest degree of hypoxemia would have been sufficient to
make him complain of difficulty breathing. The rapid response to albuterol is consis-
tent with decreasing the resistence to air flow, with consequent lessor effort resulting
in chest wall receptors no longer sending signals of increased respiratory effort.
Hypoxemia can be from ventilation-perfusion mismatching and commonly occurs
early in acute asthma. Because albuterol relaxes pulmonary arteriol smooth muscle
in addition to bronchial smooth muscle, ventilation-perfusion mismatching may actu-
ally worsen from use of a bronchodilator, even though symptomatic relief results from
the decrease in airway resistance from the bronchodilatation. Alternatively, a severe
increase in airway resistance greater than can be maintained by the patient results
in hypoventilation, with a consequent increase in pCO
2
. The rapid relief of dyspnea,
despite the continued mild degree of hypoxemia, makes that scenario unlikely in
this patient. His dyspnea was therefore a manifestation of the increased work of
breathing perceived through receptors in the chest wall.
The presence of continued mild hypoxemia is from the ventilation-perfusion
mismatching, resulting from the shunting of pulmonary arterial blood from poorly
ventilated areas of the lung to better-ventilated areas. If the same degree of hypox-
emia was accompanied by continued increased work of breathing manifested by
continued retractions and discomfort, then obtaining a pCO
2
would be critical to
identify the potential for early signs of respiratory failure.
Weinberger & Abu-Hasan 36
Treatment requires a short course of oral corticosteroid to reverse the obstruction
from inflammation that results in differential ventilation and the consequent ventila-
tion-perfusion mismatching. Inhaled corticosteroids may then be indicated as long-
term maintenance medication if this episode is more than a manifestation of
intermittent viral respiratory-induced asthma.
24
Case 2
A 15-year-old girl takes a typical teenage summer-time job in Iowa, called detasseling.
(Detasseling is done to cross-breed, or hybridize, two different varieties of corn. Fields
of corn that will be detasseled are planted with two varieties of corn. By removing the
tassels from all plants of one variety, all the grain growing on those plants will be
fertilized by the other varietys tassels.) She developed severe dyspnea with respira-
tory sounds that were described as wheezing, and was taken to the local emergency
room, where an injection of epinephrine relieved her symptoms. The next day, she
again attempted detasseling, with the same result. She then abandoned her goal of
detasseling but continued for the next 3 weeks to have similar episodes of dyspnea,
described by the patient, emergency room care givers, and her primary care pediatri-
cian as wheezing. These episodes would occur both spontaneously and with exer-
tion, and would not respond to epinephrine as they did on the first 2 days. Trials by her
primary care pediatrician of antiasthmatic medications, including inhaled albuterol,
oral corticosteroids, and inhaled corticosteroids, failed to either prevent or relieve
acute symptoms when they occurred. Symptoms would last up to several hours,
considerably limiting activity of this normally very active adolescent.
After 3 weeks of these daily symptoms, she was referred to the authors pediatric
allergy and pulmonary clinic. She was initially asymptomatic. However, a treadmill
exercise reproduced her dyspnea and the respiratory sound previously described
as wheezing. The sound precipitated during exercise testing was high-pitched and
limited to inspiration. Spirometry before and after the onset of dyspnea demonstrated
inspiratory airway obstruction (Fig. 2).
25
Flexible laryngoscopy during the episode
demonstrated paradoxical vocal cord movement (video with audio can be seen and
heard as Video 3 at the following site: http://pediatrics.aappublications.org/cgi/
content/full/120/4/855).
This demonstrated that her dyspnea was from the vocal cord dysfunction
syndrome. While the evaluation included a large positive skin prick test to corn pollen,
which explained the initial episodes as being consistent with laryngeal edema from
intense exposure to the corn pollen during the detasseling procedure, the subsequent
episodes were from the functional disorder of vocal cord dysfunction with paradoxical
motion, whereby the vocal cords paradoxically closed on inspiration with relaxation
and consequent opening on expiration.
26
Instructions by a speech pathologist provided this girl with the ability to stop the
paradoxical movement when it would start, but it continued to occur during vigorous
activity, interfering with her activities as a cheerleader. Suspecting a vagal mechanism
for this, a trial of pre-exercise treatment with an anti-cholinergic inhaler, ipratropium,
reliably prevented the exercise-induced vocal cord dysfunction.
27
This regimen
allowed her to resume her usual athletic activities, including cheerleading.
Case 3
The 15-year-old girl in Case 3 had a 1.5-year history of recurrent, extremely severe
dyspnea. Episodes were sufficiently impressive to observers that paramedics were re-
peatedly called for urgent transportation to a local hospital emergency room. Symp-
toms would last for variable periods of time and occurred with sporadic frequency,
Perceptions and Pathophysiology of Dyspnea 37
without apparent inciting factors. She had been treated with various antiasthmatic
medications, including inhaled and oral corticosteroids, with no benefit. She had
been hospitalized several times, where she received intravenous corticosteroids
and vigorous use of inhaled bronchodilators, also without benefit.
The first time this girl was seen at the authors pediatric allergy and pulmonary clinic,
she was free of any symptoms of dyspnea and her physical examination was normal.
Initial spirometry was completely normal. To further assess the cause of the dyspnea,
a bronchoprovocation with histamine was planned. While preparing the vials of the
various concentrations of histamine needed for the progressive inhalational provoca-
tion, and before any had been administered, she began having severe respiratory
distress, with both inspiratory and expiratory wheezing-like sounds. Her spirometry
changed from showing normal inspiratory and expiratory flow to severe obstruction
in both phases of respiration (Fig. 3). Flexible laryngoscopy during the episode dem-
onstrated virtually complete closure of the vocal cords, leaving only a small aperture
for air movement with no abduction, except briefly during speech (video with audio
can be seen and heard as Video 4 at the following site: http://pediatrics.aappublica
tions.org/cgi/content/full/120/4/855).
25
Treatment focused on speech pathology, to teach the patient control over her vocal
cords when symptoms occurred. Response to treatment was only partially effective.
She was able to control some episodes but not others. Lack of continuity for her care
hampered progress. She and her single mother subsequently moved to Texas, and
she was lost to follow-up.
Case 4
A 9-year-old girl was transferred from a local hospital to the authors pediatric inten-
sive care unit (PICU) because of progressive dyspnea and hypoxemia. She had a prior
history of intermittent asthma, with appropriate responses to conventional measures,
Fig. 2. Spirometry before and after exercise in the girl described in Case 2, showing the
marked decrease in the inspiratory portion of the flow-volume loop in association with
dyspnea, and an inspiratory wheeze-like sound (technically a high-pitched stridor). (From
Weinberger M, Abu-Hasan M. Pseudo-asthma: when cough, wheezing, and dyspnea are
not asthma. Pediatrics 2007;120(4):860; with permission.)
Weinberger & Abu-Hasan 38
although the authors did not have the medical records for those ambulatory care
episodes. On this occasion, progressively greater need for oxygen had been needed
to keep O
2
saturations above 90%, despite frequent b
2
agonist (albuterol) aerosol and
intravenous corticosteroids. Transfer was arranged when that level of O
2
saturation
could not be maintained, even with 100% O
2
by mask. When seen in the PICU, she
was severely dyspneic, with rapid respirations and mild intercostal retractions.
Despite continuous albuterol aerosol and an intravenous b
2
agonist, her O
2
saturations
fell below 70%. She was intubated and ventilated with 100% O
2
, but her saturation
stayed at 70%. She required only 15-cmH
2
Opressure to provide adequate ventilation
at an appropriate volume setting for her size. A blood gas demonstrated a pCO
2
of
28 mm Hg at that ventilator setting.
Because there was no evidence of airway obstruction based on the modest pres-
sure requirements for ventilation, it appeared likely that the vigorous use of b
2
agonists
was increasing ventilation-perfusion mismatching in a lung disease other than asthma.
Stopping all bronchodilator use resulted in oxygen requirements to maintain satura-
tions greater than 90%, rapidly decreasing from 100% to an FiO
2
of 70%. After
permitting her to rest overnight on the ventilator with progressively decreasing O
2
requirement, she was extubated the following morning with only 40% O
2
required.
The need for oxygen gradually decreased over the ensuing days.
Pulmonary function testing the following day showed no evidence for airway
obstruction, but decreased lung volumes and diffusing capacity were observed.
This subsequently normalized over several weeks. Recurrences of this restrictive
lung disease were observed over subsequent years, but with gradually decreasing fre-
quency. Decreased lung volumes and diffusion capacity for carbon monoxide (DLCO)
without airway obstruction was observed with each of these, all of which were self-lim-
ited without treatment after a trial of corticosteroids was not found to alter the course.
Bronchodilators were avoided and hospitalization was rarely required, and then only
with no need for assisted ventilation or intensive care. By the time she started college,
these episodes stopped reoccurring.
While the etiology of this apparently interstitial lung disease was never identified,
this patients clinical course shows the potential danger of assuming asthma in all
cases of acute respiratory distress in children. Use of b
2
agonists for dyspnea with
hypoxemia in the absence of airway obstruction risks substantial worsening of
Fig. 3. Spirometry before and after the onset of dyspnea in the girl described in Case 3,
showing the marked decrease in the inspiratory and expiratory portion of the flow-volume
loop in association with an inspiratory wheeze-like sound (technically a high-pitched stridor
on inspiration and a monophonic wheeze on expiration). (From Weinberger M, Abu-Hasan
M. Pseudo-asthma: when cough, wheezing, and dyspnea are not asthma. Pediatrics
2007;120(4):860; with permission.)
Perceptions and Pathophysiology of Dyspnea 39
hypoxemia by pulmonary arteriolar dilatation, thereby overcoming the normal protec-
tive reflexive pulmonary arteriolar constriction that shunts blood frompoorly ventilated
to better ventilated areas of the lung. The improvement in ventilation that occurs from
the bronchodilatation of a b
2
agonist in asthma generally results in greater overall
benefit, whereas the absence a bronchospastic component to the clinical situation
results in only worsening of hypoxemia, as occurred in this patient.
Case 5
This 3-year-old boy was admitted to the University of Iowa Childrens Hospital
because of progressive dyspnea on exertion and recent onset of cyanosis. His mother
described him as becoming very short of breath when going up stairs. One month
earlier, he had similar symptoms, was hospitalized locally, given antibiotics, and
recovered completely within a few days. When seen by the authors, he had rapid res-
pirations with only minimal intercostal retractions. He appeared definitely cyanotic but
other than the tachypnea, he did not appear distressed at rest. He was afebrile. An
arterial blood gas showed a pO
2
of 50 with a pCO
2
of 32 mmHg. A chest X-ray showed
perihilar and right lower lobe infiltrates (Fig. 4).
In investigating the potential etiology, a history of raising doves in the front room of
the house was obtained (Fig. 5). Examination of the boys serum identified precipitins
to pigeon serum and pigeon droppings (Fig. 6). The common precipitin to pigeon
droppings and serum in this boy confirm that the lung disease is a manifestation of
pigeon breeders lung disease, an allergic alveolitis.
28
It was the impressive degree
of hypoxemia without a major degree of increased work of breathing that suggested
an interstitial or alveolar process and not an airway cause for his dyspnea.
Within a few days in the hospital, spontaneous recovery was apparent, with normal-
ization of his blood gases. He was kept in the hospital until his parents could remove
Fig. 4. Chest film of 3-year-old boy described in Case 5, with dyspnea on exertion, tachypnea,
cyanosis; he was afebrile, had minimal intercostal retractions, and did not appear to be dis-
tressed while at rest. (From Wolf SJ, Stillerman A, Weinberger M, et al. Chronic interstitial
pneumonitis in a 3-year-old from hypersensitivity to dove antigens. Pediatrics 1987;79(6):
1027; with permission.)
Weinberger & Abu-Hasan 40
the pigeons and clean the front room of the house. He subsequently remained well. In
contrast to his complete recovery, repeated exposure over prolonged periods can be
associated with irreversible pulmonary fibrosis in someone with allergic alveolitis, also
called hypersensitivity pneumonitis.
Case 6
A 16-year-old high school basketball player judged competitive for college scholar-
ships was seen in the Pediatric Allergy & Pulmonary Clinic for exercise-induced dysp-
nea. Although an excellent and aggressive player, he could not last a quarter without
complaining of shortness of breath. The coach would pull him out, and after a few
minutes rest he was able to re-enter the game. A previous diagnosis of asthma led
to the use of albuterol, without any response.
Physical examination revealed an extremely fit-looking tall adolescent. Baseline
pulmonary function was normal. Treadmill running with cardiopulmonary monitoring
Fig. 6. Ouchterlony double-gel diffusion with the serum of the patient described in Case 5;
his serum is in the center well and the indicated antigens are in six surrounding wells on an
agar plate. The common precipitin to pigeon droppings and serum in this boy confirm that
the lung disease is a manifestation of allergic alveolitis from pigeon breeders lung disease.
(From Wolf SJ, Stillerman A, Weinberger M, et al. Chronic interstitial pneumonitis in a 3-
year-old from hypersensitivity to dove antigens. Pediatrics 1987;79(6):10279; with
permission.)
Fig. 5. One of the doves (a pink pigeon) raised in the front room of the home of the child
described in Case 5.
Perceptions and Pathophysiology of Dyspnea 41
was performed with increasing ramp until his typical symptom of dyspnea was repro-
duced (Fig. 7).
Although the initial monitoring of cardiac and pulmonary gas exchange was consis-
tent with that of a well-conditioned athlete, the onset of his reproduced dyspnea was
associated with a sudden increase in the heart rate to 220 beats per minute. Upon
cessation of exercise, the heart rate stayed at 220 for up to 10 minutes, when it
abruptly dropped to 90. A consult from a cardiac electrophysiologist interpreted the
ECG as demonstrating supra-ventricular tachycardia. Electophysiologic studies
subsequently identified an alternate conductive pathway to the atrioventricular
bundle. A radio-frequency ablation procedure was then performed, after which he
was then able to complete quarters in basketball without the previously experienced
dyspnea.
The relevance of presenting this patient is the presence of the symptoms, shortness
of breath, in the absence of any pulmonary abnormality. At no time did this boy
complain of palpitations. In the absence of reproducing his symptoms during appro-
priate physiologic monitoring, his treatable problem would not have been identified.
Case 7
A 16-year-old girl was referred to the Pediatric Allergy & Pulmonary Clinic because of
exercise-induced dyspnea. She was captain of her basketball team, but continued to
Fig. 7. Treadmill testing with cardiopulmonary monitoring. Oxygen use and carbon dioxide
production with breath-by-breath analysis combined with ECG cardiac monitoring permit
assessment of physiologic function and physical conditioning. A pressure transducer permits
measurement of flow-volume loops during exercise to assess upper or lower airway obstruc-
tion during exercise. (From Weinberger M, Abu-Hasan M. Pseudo-asthma: when cough,
wheezing, and dyspnea are not asthma. Pediatrics 2007;120(4):862; with permission.)
Weinberger & Abu-Hasan 42
experience exercise-induced symptoms that limited her activity and required her to
frequently sit out of the game for a period of time because of dyspnea. These symp-
toms had been present for at least the two previous years. She had been diagnosed at
age 14 with exercise-induced asthma and placed on an inhaled corticosteroid. The
dose had been progressively increased because of continued exercise-induced dysp-
nea. She also used albuterol before exercise. Despite consistent adherence to the
prescribed regimen, no benefit was apparent from any of this.
Treadmill exercise testing with cardiopulmonary monitoring was performed while
running during a progressively increasing ramp. Based on the heart rate and oxygen
use, she demonstrated a high level of cardiovascular function consistent with being
a well-conditioned athlete. Her exercise-induced dyspnea was not reproduced until
well beyond her anaerobic threshold. Her capillary pH at the end of exercise was
7.18, and a pCO
2
of 42 mm Hg with no apparent cardiac or pulmonary
pathophysiology.
The diagnosis of her exercise-induced dyspnea was thus because of reaching
normal physiologic limitation. As exercise progressively increases, maximum oxygen
use is eventually reached and anaerobic metabolism becomes the eventual source of
energy. That produces lactic acid, and the resultant metabolic acidosis is translated
by receptors into a demand for greater minute ventilation to create compensatory
respiratory alkalosis by decreasing pCO
2
. However, increased carbon dioxide is being
simultaneously produced and the neurologic demand for increased ventilation
encounters the physical limits of ventilation. The continued respiratory drive beyond
the capability of the body to meet the demand results in dyspnea, which is interpreted
by some as abnormal shortness of breath.
In a study of children and adolescents referred to the authors for exercise-induced
dyspnea, most had been previously diagnosed and treated for asthma. The most
common cause of exercise-induced dyspnea in these patients, occurring in over
half of those tested, was physiologic limitation. It was the perception of these individ-
uals that the dyspnea they were experiencing represented an abnormal physical prob-
lem. These patients included the full range of cardiovascular conditioning from highly
conditioned competitive athletes to those attempting vigorous exercise with little prior
conditioning and consequent below-average cardiovascular conditioning. In the
absence of cardiopulmonary monitoring during exercise that reproduced their symp-
toms, the etiology of the exercise-induced dyspnea would have continued to be
inappropriately treated in many of these patients (Fig. 8).
22
Case 8
A 26-year-old pediatric cardiology fellow with a long history of severe chronic asthma
entered the authors care program. She had a documented history of at least one
episode of respiratory failure requiring intubation and ventilatory assistance. With
appropriate maintenance medication, her asthma had become well controlled until
she developed symptoms of a viral respiratory infection associated with disturbing
cough. As the cough increased, she became increasingly dyspneic, and came to
the University of Iowa Emergency Treatment Center. Because of impressive dyspnea
and tachypnea, she was admitted immediately to the medical intensive care unit.
A blood gas there showed a pO
2
of 220 on oxygen, a pH of 7.54, and a pCO
2
of
18 mm Hg. The presence of excellent oxygenation with respiratory alkalosis was con-
sistent with hyperventilation, a diagnosis that was as apparent to this medically
sophisticated patient as it was to the physicians caring for her.
While the cough was probably a manifestation of her asthma, her experience in the
recent past of requiring intubation and assisted ventilation from respiratory failure was
Perceptions and Pathophysiology of Dyspnea 43
the likely explanation for the anxiety-induced hyperventilation in this case. The authors
present this young adult because this medically sophisticated pediatric cardiology
fellowwas asked if she could tell the difference between the dyspnea she experienced
in this case and dyspnea when she experienced asthma leading to respiratory failure.
Her response was that both felt the same. This emphasizes that dyspnea is perceived
as dyspnea, whatever the etiology.
The authors have had several children and adolescents with similar histories of life-
threatening episodes from acute asthma who subsequently experienced similar
symptoms of dyspnea associated with hyperventilation. Unless emergency treatment
center physicians are alert to this possibility, inappropriate treatment for asthma will
be given that will not relieve the dyspnea and will continue to result in repeated
such care requirements. Such patients should be suspected if initial pulse oximetry
in a dyspneic asthmatic is in the high 90s while breathing room air. When a blood
gas, capillary, or venous is adequate, it can then be determined if the pH is high
and the pCO
2
is low, consistent with respiratory alkalosis from hyperventilation. Pro-
vision for a means of assessing lung function at home permits the patient to distinguish
dyspnea from the airway obstruction of acute asthma from that of anxiety and hyper-
ventilation, thereby preventing unnecessary episodes of urgent medical care.
Case 9
A 16-year-old girl with cystic fibrosis had been admitted to the hospital with an exac-
erbation of her lung disease. Despite increased cough and decreased spirometric
values indicating worsening airway obstruction, she was not initially dyspneic. She
was treated with intravenous tobramycin and piperacillin. Three days into treatment,
she began to experience increasingly severe dyspnea associated with neither hypox-
emia nor hypocapnia. She was transferred to the PICU. Her hemoglobin was found to
Fig. 8. Diagnoses determined by treadmill exercise testing with physiologic monitoring.
Abbreviations: EIB, exercise-induced bronchospasm; EIH, exercise-induced hyperventilation;
EIL, exercise-induced laryngomalacia; EIVTach, exercise-induced supraventricular tachycar-
dia; Physiologic, normal physiologic limitation without other abnormality; Restrictive,
apparent restriction of chest wall movement; VCD, vocal cord dysfunction. (From Weinberger
M, Abu-Hasan M. Pseudo-asthma: when cough, wheezing, and dyspnea are not asthma. Pe-
diatrics 2007;120(4):862; with permission.)
Weinberger & Abu-Hasan 44
have dropped to less than 4 mg/dL, in association with severe hemolysis mediated by
antibodies to the pipericillin.
This patient illustrates that increased airway obstruction in chronic lung disease,
such as cystic fibrosis, is often not associated with dyspnea, despite levels of airway
obstruction that would cause dyspnea when occurring acutely in someone with
asthma. This patient also demonstrates the potential for dyspnea from the decreased
oxygen-carrying capacity of severe anemia, even while blood gases themselves
remain normal.
Case 10
A 14-year-old boy with a diagnosis of systemic lupus erythematosis (SLE) made
3 years earlier, with no prior history of respiratory complaints, was admitted to the
PICU with a history of progressive fatigue, dyspnea, and chest pain. He had no fever
or cough. He was tachypneic and had an O
2
saturation by pulse oximetry of 91%,
which increased readily to 99% with supplemental O
2
. He appeared to be experienc-
ing increased respiratory effort, but there was minimal inspiratory movement with each
breath. He was started on 250 mg of intravenous methylprednisolone every 8 hours.
By the second day of admission, his O
2
saturation normalized although he was still
dyspneic. Pulmonary function at that time demonstrated no airway obstruction, but his
vital capacity was only 20% of predicted, and his total lung capacity was 34% of pre-
dicted. By day five he was no longer dyspneic; his vital capacity and total lung capacity
had increased to 31% and 44% of predicted, respectively. His single breath DLCO
normalized for alveolar volume (DLCO/Va) was only mildly reduced at 78% of pre-
dicted. Continued treatment by the pediatric rheumatologist further improved his vital
capacity and total lung capacity to 45% and 57% of predicted, respectively, by
23 days after admission; his DLCO/Va had increased somewhat to 87% of predicted
by that time.
While the physiologic mechanism of this uncommon complication of SLE, known as
shrinking lung syndrome, is only speculative, it appears to be associated with
restricted diaphragmatic movement, which was in fact demonstrated fluoroscopically
in this patient.
29
This case illustrates that restrictive changes are well tolerated until
a critically low level of ventilation is reached. This patient also demonstrates the value
of lung volumes and DLCO in addition to just spirometry in identifying the physiologic
abnormality associated with dyspnea. While there is the potential for interstitial lung
disease to be associated with collagen-vascular diseases, the modest decrease in
the DLCO for this patient did not provide support for that type of physiologic
abnormality.
SUMMARY
Dyspnea is a complex psycho-physiologic sensation that has many causes that can
be anatomic, physiologic, or psychologic. The entities causing dyspnea include
commonly occurring problems, such as asthma, and uncommon but clinically
important problems to identify, such as allergic alveolitis and the shrinking lung
syndrome of systemic lupus erythematosis. Functional disorders, such as the varia-
tions of vocal cord dysfunction and hyperventilation, require identification so those
patients can be treated behaviorally and not subjected to inappropriate medication.
Exercise-induced dyspnea, while a characteristic of asthma, should not be assumed
to be asthma in the absence of other symptoms of asthma and a convincing response
to prevention by pretreatment with an albuterol aerosol. Treadmill exercise testing that
reproduces symptoms with cardiopulmonary monitoring can identify the physiologic
Perceptions and Pathophysiology of Dyspnea 45
Table1
Intervention for dyspnea
Intervention Recommendation
Grading of Recommendation
(Based on Evidence of Benefit)
Quality of Supporting
Evidence
Albuterol (salbutamol) aerosol Only for asthma Strong Strong
Corticosteroids, inhaled Only for chronic asthma Strong Strong
Corticosteroids, oral, short course of high
dose
For exacerbations of asthma Strong Strong
Corticosteroids, oral, short course of high
dose
For assessment of response to
support the diagnosis of asthma
as the cause of dyspnea
Moderate Moderate
Long acting b
2
agonists As additive agent to inhaled
corticosteroids for chronic asthma
Moderate Strong
Montelukast For chronic asthma Low Moderate
Epinephrine (adrenalin) injection For acute laryngeal edema of
systemic anaphylactic reaction
High High
Speech therapy For recurring spontaneous
episodes of vocal cord dysfunction
Moderate Low
Ipratropium aerosol For prevention of exercise-induced
vocal cord dysfunction
Moderate Low
Ipratropium aerosol For severe acute asthma not
responding to albuterol
Moderate Moderate
Environmental adjustment For allergic asthma Moderate Low
Environmental adjustment For allergic alveolitis High Moderate
W
e
i
n
b
e
r
g
e
r
&
A
b
u
-
H
a
s
a
n
4
6
abnormality, whether exercise-induced bronchospasm, vocal cord abnormalities, or
the various other physiologic causes demonstrated to be associated with exercise-
induced dyspnea. The following outline (see also Table 1) lists the steps health care
professionals should follow when a patient presents with dyspnea:
I. A complete medical examination with particular attention to cardiorespiratory
systems and a focus on:
A. Determining its clinical pattern
1. Present all of the time
2. Present only during exercise
3. Present only with specific environmental exposures
B. Level of respiratory dysfunction (ie, degree of disability)
C. Observation of level of dysfunction from others
D. Presence of airway noises
II. Evaluation should include:
A. Chest X-ray
B. Baseline oximetry
C. Blood pH and pCO2 when oximetry below normal or if dyspnea presents with
normal oximetry
D. Spirometry with considerations for lung volumes and diffusing capacity if patient
is able to perform
E. Cardiorespiratory exercise test to reproduce exercise-induced symptoms if pa-
tient is able to do this
III. Referral for further evaluation and management if:
A. Dyspneic at rest and diagnosis not apparent
B. Hypoxemic and diagnosis not apparent
REFERENCES
1. Meek PM, Schwartzstein RM, and the ad hoc Committee of the Nursing Assembly
of the American Thoracic Society. Dyspneamechanisms, assessment, and
management: a consensus statement. American Thoracic Society. Am J Respir
Crit Care Med 1999;159(1):32140.
2. ODonnell DE, Hong HH, Webb KA. Respiratory sensation during chest wall
restriction and dead space loading in exercising men. J Appl Phys 2000;88(5):
185969.
3. Demediuk BH, Manning H, Lilly J, et al. Dissociation between dyspnea and respi-
ratory effort. Am Rev Respir Dis 1992;146(5 pt 1):12225.
4. The enigma of breathlessness [editorial]. Lancet 1986;1(8486):8912.
5. Zealley AK, Aitken RC. Breathlessness and anxiety. Br Med J 1970;2(5705):363.
6. Rietveld S, Everaerd W, van Beest I. Excessive breathlessness through emotional
imagery in asthma. Behav Res Ther 2000;38(10):100514.
7. Rietveld S, Prins PJ. The relationship between negative emotions and acute
subjective and objective symptoms of childhood asthma. Psychol Med 1998;
28(2):40715.
8. Janson C, Bjornsson E, Hetta J, et al. Anxiety and depression in relation to respi-
ratory symptoms and asthma. Am J Respir Crit Care Med 1994;149(4 Pt 1):9304.
9. Tiller J, Pain M, Biddle N. Anxiety disorder and perception of inspiratory resistive
loads. Chest 1987;91(4):54751.
10. Trochtenberg DS, BeLue R. Descriptors and perception of dyspnea in African-
American asthmatics. J Asthma 2007;48(10):8115.
Perceptions and Pathophysiology of Dyspnea 47
11. Fosi E, Stendardi L, Binazzi B, et al. Perception of airway obstruction and airway
inflammation in asthma: a review. Lung 2006;184(5):2518.
12. Van Gent R, van Essen-Zandvliet LEM, Rovers MM, et al. Poor perception of
dyspnea in 28 children with undiagnosed asthma. Eur Respir J 2007;30(5):
88791.
13. Veen JC, Smits HH, Ravensberg AJ, et al. Impaired perception of dyspnea in pa-
tients with severe asthma. Relation to sputum eosinophils. Am J Respir Crit Care
Med 1998;158(4):113441.
14. Restrepo RD, Peters J. Near-fatal asthma: recognition and management. Curr
Opin Pulm Med 2008;14(1):1323.
15. Borg G. Psychophysical bases of perceived exertion. Med Sci Sports Exerc
1982;14(5):37781.
16. Gift AG. Validation of a vertical visual analogue scale as a measure of clinical
dyspnea. Rehabil Nurs 1989;14(6):3235.
17. Wilson RC, Jones PW. Differentiation between the intensity of breathlessness and
the distress it evokes in normal subjects during exercise. Clin Sci 1991;80(1):
6570.
18. Pratter MR, Curley FJ, Dubois J, et al. Cause and evaluation of chronic dyspnea
in a pulmonary disease clinic. Arch Intern Med 1989;149(10):227782.
19. Hammerman SI, Becker JM, Rogers J, et al. Asthma screening of high school
athletes: identifying the undiagnosed and poorly controlled. Ann Allergy Asthma
Immunol 2002;88(47):3804.
20. Panditi S, Silverman M. Perception of exercise induced asthma by children and
their parents. Arch Dis Child 2003;88(9):80711.
21. Melani AS, Ciarleglio G, Pirelli M, et al. Perception of dyspnea during exercise-
induced bronchoconstriction. Respir Med 2003;97(3):2217.
22. Abu-Hasan M, Tannous B, Weinberger M. Exercise-induced dyspnea in children
and adolescents: if not asthma then what? Ann Allergy Asthma Immunol 2005;
94(3):36671.
23. Seear M, Wensley D, West N. How accurate is the diagnosis of exercise induced
asthma among Vancouver schoolchildren? Arch Dis Child 2005;90(9):898902.
24. Abu-Hasan M, Weinberger M. Management of asthma in children: translating
patient-oriented evidence into practice. Hosp Physician 2007;43(8):3649.
25. Weinberger M, Abu-Hasan M. Pseudo-asthma: when cough, wheezing, and
dyspnea are not asthma. Pediatrics 2007;120(4):85564.
26. Christopher KL, Wood RP 2nd, Eckert RC, et al. Vocal-cord dysfunction present-
ing as asthma. N Engl J Med 1983;308(26):156670.
27. Doshi D, Weinberger M. Long-term outcome of vocal cord dysfunction. Ann
Allergy Asthma Immunol 2006;96(6):7949.
28. Wolf SJ, Stillerman A, Weinberger M, et al. Chronic interstitial pneumonitis in
a 3-year-old from hypersensitivity to dove antigens. Pediatrics 1987;79(6):
10279.
29. Ferguson PJ, Weinberger M. Shrinking lung syndrome in a 14 year old boy with
systemic lupus erythematosus. Pediatr Pulmonol 2006;41(2):1947.
Weinberger & Abu-Hasan 48
Chest Pai n and Chest
Wal l Deformi ty
Janaki Gokhale, MD
a,b
, Steven M. Selbst, MD
a,b,
*
Chest pain is a relatively common complaint among pediatric patients and presents
a diagnostic challenge that is associated with significant emotional as well as mone-
tary costs. Patients as well as their families are often concerned about life-threatening
causes for the chest pain, although these are rarely identified. There are numerous eti-
ologies for pediatric chest pain and Box 1 lists the differential diagnosis of chest pain
in children.
The clinicians primary goal in evaluating the pain, whether it is in a primary care
office, cardiology clinic, or the emergency department (ED) setting, is to identify the
serious causes and rule out other organic pathology. Similarly, chest wall deformity
can also be of great concern to patients and their families. The goal in evaluation
and treatment of patients with chest wall deformity should be to maximize lung growth
and function as a child grows and to minimize related psychologic problems.
Table 1 describes the levels of evidence for studies discussed in this paper.
CHEST PAIN
The frequency of pediatric chest pain among different EDs has been shown to be
anywhere between 0.3% (Level of evidence [LOE] 2, Table 1)
1
and 0.6% of all visits
(LOE 2).
2,3
In an earlier study (LOE 2),
4
the occurrence rate of chest pain in the ED, car-
diac clinic, and primary care physicians office in one hospital was found to be
0.288%. One of these studies (LOE 2),
1
while finding very few serious causes of
chest pain, noted that almost 90%of patients considered the pain to be at least mod-
erate or severe in intensity; at least half of the patients interviewed by a psychiatrist in
another study were worried about the pain being related to their heart (LOE 2).
4
Given the perceived severity of pain and the surrounding anxiety about heart
problems and presumably other life-threatening problems, it would be useful to
have an evidence-based guide for chest pain that allowed efficient identification of
a
Jefferson Medical College, Philadelphia, PA 19107, USA
b
A.I. duPont Hospital for Children, 1600 Rockland Road, Wilmington, DE 19803, USA
* Corresponding author. Department of Pediatrics, A.I. duPont Hospital for Children, 1600
Rockland Road, Wilmington, DE 19803.
E-mail address: sselbst@nemours.org (S.M. Selbst).
KEYWORDS
Chest pain
Cardiac
Musculoskeletal
Pulmonology
Pectus deformity
Ischemia
Pediatr Clin N Am 56 (2009) 4965
doi:10.1016/j.pcl.2008.10.001 pediatric.theclinics.com
0031-3955/08/$ see front matter 2009 Elsevier Inc. All rights reserved.
Box1
Differential diagnosis of pediatric chest pain
Cardiac
Coronary artery disease-ischemia/infarction
Anomalous coronary arteries
Kawasaki disease (coronary arteritis)
Diabetes mellitus (long standing)
Arrhythmia
Supraventricular tachycardia
Ventricular tachycardia
Structural abnormalities of the heart
Hypertrophic cardiomyopathy
Severe pulmonic stenosis
Aortic valve stenosis
Infection
Pericarditis
Myocarditis
Gastrointestinal disorders
Reflux esophagitis
Pill induced esophagitis
Esophageal foreign body
Psychological disorders
Stress-related pain
Musculoskeletal disorders
Chest wall strain
Direct trauma/contusion
Rib fracture
Costochondritis
Idiopathic
Pulmonary/Respiratory disorders
Severe cough
Asthma
Pneumonia
Pneumothorax/pneumomediastinum
Pulmonary embolism
Miscellaneous disorders
Sickle cell crisis
Abdominal aortic aneurysm (Marfan syndrome)
Pleural effusion (collagen vascular disease)
Shingles
Pleurodynia (coxsackievirus)
Breast tenderness (pregnancy, physiologic)
Chest mass
50
life-threatening conditions and correct diagnosis of other etiologies. However, as has
been shown by several studies (all LOE 2),
14
life-threatening causes of chest pain are
rare in the pediatric population. It follows that it would be quite difficult for any random-
ized, prospective study to have sufficient power to provide evidence necessary to
direct diagnostic testing. However, based on the data available, we suggest a com-
monsense approach that should allow for reasonable use of resources without
compromising diagnostic sensitivity (Table 2). On review of the few studies that
have been devoted to the complaint of pediatric chest pain, one reassuring theme
is found: a thorough history and physical examination provide the best clues to deter-
mine etiology, and further diagnostic workup is not required in most cases.
Cardiac
As has already been stated, most patients/parents who present with chest pain are
concerned about their heart (LOE 2).
4
In fact, chest pain is the second most common
cause for referral to a pediatric cardiologist (LOE 5).
5
Although a cardiac problem is
generally not found with chest pain (all LOE 2),
14
arrhythmias, mitral valve prolapse,
and myocarditis/pericarditis are worth discussing. Rarely, one may see aortic dissec-
tion or ischemiathe latter with obstructive lesions, cocaine use, coronary artery
anomalies, coronary artery occlusion, or myocardial bridging. With more serious,
life-threatening causes, there may be a history of Marfan syndrome (see section on
Marfan syndrome later in this article) or congenital hyperlipidemia. Chest pain could
be the first sign of hypertrophic cardiomyopathy.
Previous studies have shown that a thorough history and physical examination are
often enough to identify cardiac causes of chest pain. In one study (LOE 2),
1
of 168 pa-
tients who presented to the ED with chest pain, 9 patients were found to have a car-
diac-related cause. Symptoms of fever (2/9), dyspnea (3/9), palpitations (5/9), pallor
(2/9) and most importantly pathologic heart auscultation (9/9) were found to be statis-
tically significantly related to a cardiac etiology. Interestingly, palpitations were also
Table1
Levels of evidence
Level Description
No. Papers CitedChest
Pain
No. papers CitedChest
Wall Deformity
1 Randomized controlled
trials or meta-analysis
0 1
2 Prospective or cohort
studies
8 2
3 Case control 2 3
4 Retrospective studies 6 2
5 Case series/case reports,
expert opinion/review
3 9
This system of classification was created specifically for the evidence found regarding chest pain
and chest wall deformity and has not been previously validated. A common validated method
of classification
27
cannot be used accurately in this case because we aim to provide guidance on
characterization and diagnosis, as well as management of chest pain. The classification of levels
of evidence for each of these goals is different based on this validated method. Therefore, we
have provided only a simple guide for the reader to understand the types of studies that are in-
cluded in this discussion. It is important to note that although a study may be listed as a LOE 2
it may not necessarily supercede a better-designed case control or evidence stated in a review
(LOE 5). Some studies have significant limitations and are discussed in the text where they appear.
Chest Pain and Chest Wall Deformity 51
found to be statistically significantly related to a psychogenic cause (5/15 patients), so
this may not be a reliable marker for cardiac pain. Pain with exercise has long been
considered worrisome for cardiac disease. In this study, chest pain associated with
exercise was found in only 6 of 108 patients with chest wallrelated pain, but it was
not significantly related to cardiac pain either. In the same study, 5 of 69 patients
who presented to a pediatric cardiology clinic for chest pain were found to have sup-
raventricular tachycardia. Again, palpitations were significantly correlated (5/5) pa-
tients for this category (LOE 2).
1
An earlier prospective study (LOE 2)
2
of children in
the ED with chest pain conducted electrocardiograms (EKGs) in 191 of 235 patients
with ill-defined or cardiac-related chest pain. Of these, 31 of 235 were found to
be abnormal, but only 4 of 235 showed new or not minor changes. Three revealed
arrhythmias that were noted on physical examination and one showed evidence of
pericarditis in a child who had fever and known systemic lupus erythematosis. In
this study, these same 235 patients had echocardiograms done, and of these there
were four that showed previously unknown mitral valve prolapse. However, these
may have been incidental findings not necessarily related to the chest pain. One study
(LOE 2)
6
of 106 patients with a chief complaint of murmur and chest pain (21/106)
found EKG and chest radiograph (CXR) to be helpful in evaluation even when no car-
diac disease was suspected on history and physical examination. However, a limita-
tion of this study, as noted in the paper, is that the two groups of patients were lumped
together and there is not sufficient power to make this conclusion for patients with
chest pain alone. Finally, a 1-year prospective study of 336 patients with chest pain
from a pediatric ED in Canada (LOE 2)
3
identified only 5 patients with cardiac disease.
It seems these were identified purely by clinical suspicion by history and physical ex-
amination, or by appropriately directed EKG or (presumably) echocardiogram. Using
this approach, the authors point out that misdiagnosis of serious organic etiology is
unlikely.
Table 2
Worrisome signs and symptoms to prompt further workup in pediatric patients (partial list)
Workup History/Symptom Sign
Chest x-ray Fever Fever
Cough Tachypnea, rales, distress
Shortness of breath Ill-appearing/sick
History of trauma Significant trauma
Pain wakes from sleep Extreme tachycardia
History of drug use (eg, cocaine) Pathologic auscultation of heart
Associated with exercise Absent/decreased breath sounds
Acute onset of pain Palpation of subcutaneous air
Serious medical problems (Marfan,
Kawasaki, lupus)
Tall, thin
Foreign body ingestion (coin,
button battery)
Drooling, gagging
Electrocardiogram Associated with exercise Pathologic auscultation of heart
Associated with syncope Tachycardia (>180 beats per
minute)
History of drug use (eg, cocaine) Ill-appearing/sick
Consider with fever Consider with fever
Gokhale & Selbst 52
These prospective studies suggest that a careful history and physical examination
are generally sufficient to diagnose cardiac-related chest pain. If not, they should at
least be sufficient to guide the use of CXRs, EKGs, and echocardiograms. While other
diagnoses such as pericarditis and ischemia are not adequately represented in these
studies to draw a conclusion, retrospective studies support the prospective studies
and commonsense approach outlined in Table 2. In a retrospective study of 20 pedi-
atric patients with acute pericarditis, 13 were found to have muffled heart sounds and
7 were found to have a friction rub (LOE 4).
7
The clinical examination generally
showed a sick child with chest pain, fever, and tachypnea, and all were found to
have cardiomegaly on CXR. Regarding ischemia and myocardial infarction, we found
two small retrospective studies with nine patients each with myocardial infarction after
presenting with chest pain to an ED. In one, the authors describe acute chest pain with
a mean duration of 40 hours (LOE 4),
8
and in the second the authors state that each
patient had typical severe retrosternal chest pain radiating to the left arm or jaw
(LOE 4).
9
Previous case reports and case series have also reported myocardial ischemia in
children with a prior history of Kawasaki disease, history of cocaine or amphetamine
drug use, familial hypercholesterolemia, hypercoagulability, myocardial tumors, and
family history of early coronary heart disease. Based on this evidence (and lack of ev-
idence), we recommend a commonsense approach for suspected ischemia. A history
of classic crushing substernal chest pain (not sharp), syncope with chest pain, chest
pain associated with exercise, family history for sudden death at a young age, use of
drugs like cocaine, or underlying cardiac disease, may imply a need to investigate car-
diac etiology for pain. Likewise, findings on physical examination such as decrease in
oxygen saturation, or significant changes in heart rate and blood pressure, with acute
presentation, abnormal cardiac examination should guide the workup and prompt
evaluation with an EKG and CXR. Although chest pain with fever is highly correlated
with pneumonia, uncommon cardiac infections such as myocarditis or pericarditis
should also be considered in a febrile child with chest pain.
Gastrointestinal
Prospective studies have shown that gastrointestinal (GI) pain can account for to 4%
of pediatric chest pain to an ED (LOE 2).
1,2
The exacerbation of pain when eating can
be significantly correlated (P 5.0003) to gastritis, esophagitis, or constipation accord-
ing to one prospective study of ED patients (LOE 2).
1
One clinical trial showed that
many patients who were initially diagnosed with idiopathic chest pain actually had
a GI cause for their pain. In that study, 21 of 27 had either esophagitis, gastritis, or
esophageal spasm confirmed by esophagogastroduodenoscopy (EGD), esophageal
manometry, and Bernstein acid perfusion test (LOE 2).
10
Interestingly, none of the pa-
tients had symptoms of heartburn, regurgitation, pain with swallowing, dysphagia,
hemorrhage, or water brash, and instead the pain was described as being over
the left side, either central or retrosternal, and lasting less than a minute to several
hours. A more recent study showed that patients who presented to a cardiology clinic
with chest pain who also had epigastric pain (44 of 132 patients) had positive findings
of gastritis on endoscopy (41/44 of these patients). Of these patients, 39 were treated
and 38 of these had resolution of symptoms (LOE 2).
11
Based on these findings, we
recommend that the suspicion of gastritis or esophagitis must remain on the differen-
tial diagnosis of chest pain even without overt symptoms. In the absence of other con-
cerning findings on history and physical examination, it may be reasonable to refer
these patients (midsternal burning type pain, worse with eating or lying down) to
Chest Pain and Chest Wall Deformity 53
a gastroenterologist or start a trial of H-2 blockers or proton pump inhibitors depend-
ing on the clinical setting to see if symptoms of chest pain improve.
Some young children will complain of acute significant chest pain following inges-
tion of a coin or other foreign body that lodges in the esophagus. Although many
such patients are nonverbal, these children may present with obvious discomfort
and they may have associated drooling or dysphagia if the coin is trapped in the upper
esophagus. Some patients or parents can give a clear history of an ingested foreign
body, but in some cases the diagnosis is less obvious. Although there are no studies
to provide evidence-based guidance, it seems reasonable to obtain a CXR to look for
an esophageal foreign body in a young child with acute onset of midsternal pain, es-
pecially if the child is drooling.
Psychiatric
Chest pain related to a psychogenic cause has an incidence of anywhere between 5%
(LOE 2)
5
and 9% (LOE 2)
1,2
in children who present to the ED. The pain is generally
thought to be precipitated by hyperventilation, stressful life event, depression, or anx-
iety with no other organic etiology. One study used a specific questionnaire to identify
signs of stress and depression, but these questions were not statistically significantly
associated with a psychogenic diagnosis (LOE 2),
3
although recurrence of pain was
(LOE 2).
3
Another study found psychogenic chest pain to be 2.5 times more likely in
adolescents (P 5 .02) and three times more likely with a family history of chest pain
(P 5 .001) (LOE 2).
2
The association of psychogenic chest pain with children of older
age was confirmed by a second study (P 5 .01) (LOE 2).
1
Finally, one study found that
compared with slightly older children referred to a cardiology clinic for benign heart
murmur, children with noncardiac chest pain were significantly more likely to have
anxiety symptoms (LOE 3).
12
Currently, although significant demographic associations do seem to exist in previ-
ous studies, there are no specific questions that can be used in a practical setting to
reliably identify patients with this type of pain. However, the clinician should inquire
about possible stressors and significant life events that may correlate with the onset
of chest pain. If a stressful life event or history of anxiety is obvious, in patients with
no other significant findings on history and physical examination, it may be reasonable
to conclude the chest pain is related to stress. In others, where a stressful event is not
immediately obvious, it is reasonable to probe further into causes for emotional stress
before labeling chest pain as idiopathic.
Musculoskeletal
Musculoskeletal chest pain appears to be a relatively common cause for pediatric
chest pain in both the ED and cardiology clinic settings. Studies from the ED put
the incidence of costochondritis between 9.0%and 22.5%of patients, trauma-related
chest pain to be about 5%, and other musculoskeletal pain such as muscle strain in
5%to 15%of patients (all LOE 2).
2,4,13
Musculoskeletal chest pain is generally consid-
ered when pain is reproducible to palpation or suggested by a history of muscle strain
or minor trauma. Reproducibility of chest wall pain is generally a good marker for cost-
ochondritis or chest wall pain. However, the absence of this finding does not always
exclude a musculoskeletal cause. The duration of musculoskeletal chest pain can
be relatively long. In differentiating between costochondritis and idiopathic chest
pain, an early study found that the former had a mean duration of pain of 96.8 days,
but that idiopathic chest pain was still significantly longer in duration (797.8 days)
(LOE 2).
4
The studies indicate that a musculoskeletal etiology should always be con-
sidered when evaluating a patient with chest pain simply based on the frequency of
Gokhale & Selbst 54
this diagnosis. One might assume that palpitations associated with chest pain would
point to a cardiac etiology for pain. However, one study showed that in patients who
presented to the cardiology clinic with chest pain, palpitations were actually signifi-
cantly associated with both chest wall pain (83% of all etiologies) and cardiac-related
diagnoses (LOE 2).
1
Diagnostic studies usually do not help identify musculoskeletal
chest pain.
Idiopathic
Idiopathic chest pain is perhaps the most common diagnosis for children who present
with chest pain. Despite a careful history and physical examination, in 21% to 45% of
cases of pediatric chest pain, evaluated in two studies in a prospective manner, no di-
agnosis could be determined with certainty (LOE 2).
2,4
The childs pain was then la-
beled as idiopathic in these cases. Nonorganic disease including idiopathic chest
pain was more likely if pain persisted more than 6 months (P 5.0009)
2
(LOE 2). Driscoll
and colleagues
4
(LOE 2) also found children with idiopathic pain had symptoms longer
than other diagnostic groups (mean 798 days). The more chronic the complaint of
pain, the less likely it is that a specific etiology will be found.
Precordial catch syndrome is sometimes diagnosed in children with chest pain. This
condition, also called Texidors twinge, was first described by Miller and Texidor
14
in
1955 in a case series of adult patients (LOE 5). They noted patients had sudden, sharp,
stabbing well-localized precordial pain. It is often worse with a deep breath, and ex-
amination findings are normal (LOE 5).
15
One study of 168 children with chest pain
in the ED included precordial catch syndrome in the musculoskeletal category and
found the incidence to be 64%(LOE 2).
1
They defined the category of musculoskeletal
chest pain as classically stabbing and exaggerated with respiration, [lasting] seconds
to minutes.not associated with activity (or occurs after participation in sports activ-
ity) and sometimes, may be reproduced by palpation. Based on this definition and
forward selection analysis these authors found that a lack of cough, previous trauma,
stressful event, dyspnea, meal-related pain, fever, pathologic cardiac auscultation,
palpitations, and anxiety predicted the adherence of 97% of [chest wall] patients to
that category (LOE 2).
1
However, Selbst and colleagues
2
included patients with pre-
cordial catch syndrome in their idiopathic category, because the etiology is un-
known (LOE 2).
Studies have shown that if the history and examination are unrevealing, diagnostic
studies such as CXR and EKG are also unlikely to pinpoint a diagnosis. Abnormal lab-
oratory studies usually reveal previously known or clinically suspected problems from
the history and physical examination (LOE 2).
2,4
It is thus recommended that labora-
tory studies should not be obtained empirically, but rather be based on history and
physical examination findings.
Pulmonary
Although most parents are concerned about a cardiac etiology for chest pain, clini-
cians should not overlook pulmonary causes of chest pain, as these are often readily
treatable. Pulmonary causes of chest pain include common disease processes such
as pneumonia and asthma, as well as less frequent diagnosespneumothorax, pneu-
momediastinum, pleural effusion, pleurodynia, foreign body aspiration, and pulmonary
embolism. Pulmonary causes of chest pain have been estimated between 13% and
19% based on two prospective studies from the ED setting (LOE 2).
1,3
When the pul-
monary etiology was further delineated, 10% of patients had chest pain because of
persistent cough, 7% because of asthma, and 4% because of pneumonia (LOE 2).
2
Chest Pain and Chest Wall Deformity 55
These prospective studies were naturally not designed to assess the frequency of
more rare and serious diagnoses such as pneumothorax or pulmonary embolism.
However, chest pain is thought to be a prominent feature in almost all patients with
pneumothorax. One 12-year retrospective study of 17 pediatric patients with pneumo-
thorax found that 100% of children had chest pain on initial presentation (LOE 4).
16
Chest pain may be less common in children with pneumomediastinum. According
to a 10-year retrospective study of 29 patients in Ohio, neck pain and sore throat
were the most common (38%) presenting symptoms in patients with this condition
(LOE 4).
17
Chest pain was not discussed as a specific symptom in this study, and
the most common presenting finding was subcutaneous emphysema. Pneumothorax
and pneumomediastinum are generally found in children with asthma or lower respi-
ratory tract disease such as bronchiolitis, cystic fibrosis, and Marfan syndrome (see
section on Marfan syndrome later in this article). However, previously healthy children
may rupture an unrecognized subpleural bleb with minimal precipitating factors and
present with respiratory distress and chest pain as a result of a spontaneous pneumo-
thorax. Decreased breath sounds on the affected side are likely if the pneumothorax is
significant. Case reports indicate that patients who snort cocaine are also at risk for
barotraumas and may present with sudden severe chest pain, anxiety, respiratory dis-
tress, and tachycardia (LOE 5).
18
There are few studies describing chest pain and pulmonary embolism (PE) in chil-
dren. A recent retrospective case series of 14 patients with PE noted that all children
were symptomatic (LOE 5).
19
All patients either had chest pain (71%) or dyspnea on
exertion (79%). Screening with D-dimer was normal in 40% and this inconsistency
may have delayed diagnosis in some cases (LOE 5).
19
This condition is rare in the pe-
diatric population and multicenter trials are needed to better evaluate clinical charac-
teristics and risk factors for PE. However, this diagnosis should be considered in any
pediatric patient with venous thromboembolism or with increased likelihood of clot-
ting. The latter can be seen in nephrotic syndrome, systemic lupus erythematosis, ma-
lignancy, inflammatory bowel disease, postoperative state, hypercoagulable states,
recent abortion, or leg injury (LOE 4).
20
Patients with pulmonary embolism are likely
to have acute onset of pleuritic chest pain as well as dyspnea or cough.
History of fever and signs of tachypnea, shortness of breath, or pathologic auscul-
tation of the lungs should prompt further evaluation for a pulmonary cause of chest
pain. In addition, in a patient with a known history of asthma, one should always con-
sider chest pain could be secondary to this underlying diagnosis. While this may seem
self-evident, asthma exacerbation as a cause of chest pain may be underdiagnosed.
Massin and colleagues
1
(LOE 2) in their study of chest pain in the ED setting observed
that five patients who were categorized as having chest wall pain did, in fact, have
a history of asthma without signs of wheezing. They postulated that the lung examina-
tion might be normal in small airways hyperreactivity. Another study of 88 children with
chest pain who underwent exercise-stress testing found significant improvement in
symptoms as well objective measures of pulmonary function after bronchodilator
treatment (LOE 4).
21
The frequency of asthma in patients who present with chest
pain was found in 15% in one study (LOE 2).
3
Given this relatively high incidence, it
is reasonable in clinically stable patients with a prior history of asthma to try broncho-
dilator therapy in the office or ED setting to try to relieve symptoms regardless of the
presence of wheezing on examination.
Fever associated with chest pain should also raise suspicion of pulmonary disease
such as pneumonia or other organic disease (rare cardiac infections as noted above).
Selbst and colleagues
2
(LOE 2) found that fever with chest pain was significantly asso-
ciated (P<.001) with a diagnosis of pneumonia, documented on CXR, in their
Gokhale & Selbst 56
prospective study of 407 pediatric patients. Similarly, Massin and colleagues
1
found
that fever was significantly correlated (P<.05) with respiratory or cardiac disease
(LOE 2). Cough was also significantly correlated with respiratory conditions (P<.05).
Cough and fever predicted 99% of patients with a respiratory cause of chest pain
(LOE 2).
1
In addition, one retrospective study of 368 patients showed that chest pain
was significantly associated with complicated pneumococcal pneumonia compared
with uncomplicated pneumonia (LOE 3).
22
An obvious limitation of this study is that
all patients may not have been asked about chest pain specifically because it was a ret-
rospective study. It is important to note that chest pain alone is generally not enough to
diagnose pneumonia. In one study designed to look at clinical decision making regard-
ing diagnosis and treatment of pneumonia, the prevalence of pleuritic pain was found
to be only 8%(LOE 5).
23
However, given the evidence, we would recommend obtaining
a chest radiograph if chest pain is present with either fever or cough.
CHEST WALL DEFORMITIES
Chest wall deformities in children are sometimes correlated with chest pain. They can
also lead to restricted lung function, and many are related to psychologic problems in
children because of the associated cosmetic defects.
Pectus Excavatum
Pectus excavatum (chest depression) is the most common congenital deformity of the
anterior chest wall. The condition is generally present at birth or shortly after, but is usu-
ally asymptomatic initially. It may become more marked during childhood and teenage
growth (LOE 3).
24
Problems such as chest pain and adverse physiologic effects like de-
creased exercise tolerance may be noted over time (LOE 3, LOE 5, LOE 4).
2527
Signif-
icant psychologic stress related to the cosmetic defect is common (LOE 5).
26
It is
believed that cardiac filling is reduced in pectus excavatum as a result of compression
of the sternum on the right heart chambers, thereby lowering exercise cardiac output.
In a study of 13 patients with pectus excavatum, Zhao and colleagues
25
(LOE 3)
showed reduced oxygen uptake and stroke volume when subjects were exercising
in the sitting position, but this was equal to controls during supine exercises. The su-
pine advantage in patients with pectus excavatum suggests that upright exercise ca-
pacity is affected by reduced filling of the heart in the nonsupine position.
Children with pectus excavatum may become short of breath during strenuous ex-
ercise and complain that they are easily fatigued (LOE 3).
24
However, it is not clear if
this is clinically significant as the complaints are subjective. Pulmonary function tests
may be normal or may show a restrictive defect in children with this deformity. Haller
and Loughlin
24
studied 36 teenage patients with pectus excavatum who underwent
surgical correction (LOE 3). Before surgery, pectus subjects had significantly lower
forced vital capacity (FVC) than controls (81% 14% versus 98% 9% predicted,
P<.001). Mean values fell within normal range. Postoperative exercise pulmonary
stress tests showed a significant increase in duration of exercise in patients with the
pectus deformity but not in controls. The absolute FVC was increased after surgery in
patients with pectus excavatum, but when expressed as a percent predicted, it did
not change significantly. There were no differences in preoperative respiratory function
during exercise between controls and patients with the pectus deformity. After surgery,
patients withpectusexcavatumexercisedfor longer andhadimprovedcardiacfunction
during exercise, as shown by an elevated oxygen and a decrease in heart rate for the
same workload. Many also had subjective improvement. In summary, a few patients
with pectus excavatum have mild restrictive pulmonary function tests at rest. This
Chest Pain and Chest Wall Deformity 57
restrictive disease is not improved significantly by surgery. There is a statistically signif-
icant improvement inexercisedurationandcardiacfunctionfollowingsurgery (LOE3).
24
Patients with pectus excavatum often have EKG abnormalities. An EKG usually
shows right axis deviation and depressed ST segments (LOE 5).
26
Cardiac arrhythmias
such as supraventricular tachycardia (SVT) and atrial fibrillation have been reported,
presumably as a result of impingement of the sternum on the heart. Wolff-Parkinson-
White (WPW) syndrome is found in 4% of patients with this deformity,
28
whereas the
incidence is about 0.5% in the general population. One study found that patients with
severe pectus deformity are less likely to have WPW and SVT, suggesting cardiac im-
pingement is not the mechanism (LOE 4).
28
The diagnosis of pectus excavatum is clinical, although a chest radiograph may
demonstrate the depression. Standard anterior/posterior (AP) and lateral chest radio-
graphs show sternal depression and cardiac displacement. Pectus excavatum is con-
sidered severe if the defect is greater than 2.5 cm (ie, the childs sternum is 2.5 cm or
more below the chest wall) (LOE 3)
24
Park recommends an EKG to evaluate children
with a pectus deformity, as it is inexpensive and noninvasive (LOE 4).
28
An EKG may
show right axis deviation or mitral valve prolapse (MVP). Echocardiograms may also
demonstrate MVP, but the clinical significance of this is unclear (LOE 4).
29
A CT
scan of the chest is no longer recommended for children with pectus excavatum.
The CT scan demonstrates the depression and can quantitate the extent of the defor-
mity. However, a study of 12 adolescents showed that the Haller index, used to mea-
sure the severity of the deformity, could be measured just as accurately using a chest
radiograph as with a CT scan (LOE 4).
27
The CT scan offered no additional information
for operative planning. In children with pain or other symptoms, a CT may be consid-
ered (LOE 4).
27
There is not clear evidence to support a best management practice for children with
pectus excavatum. Surgery may be done for cosmetic reasons. Haller and Loughlin
24
recommends surgery for those withshortness of breath, fatigue duringexercise, abnor-
mal breathing dynamics in which the sternumretracts paradoxically instead of expand-
ing during inspiration, or for a CT scan that shows a pectus index greater than 3 and
arangeof 3.2to6.0(LOE3). Whether surgical correctionhalts progressionof cardiovas-
cular compromiseandimproves exercisetoleranceis debated. Ameta-analysis of eight
studies (169 patients with pectus excavatum) found that surgical repair of the chest wall
defect significantly improved cardiovascular function (LOE 1).
30
However, a more
recent study criticized that meta-analysis. In their review of 1600 reports from 1965
to 2007, the authors found five papers with primary data on cardiac function before
and after surgery. There was no convincing evidence of improvement in pulmonary or
cardiac function after thoracic surgery for pectus excavatum (LOE 5).
31
Pectus Carinatum
Pectus carinatum (pigeon chest) is the second most common congenital defect of the
anterior chest wall, but it is much less common than pectus excavatum (LOE 5).
32
It is
usually not noticed until early school years and progression at puberty is common.
Symptoms (chest pain, dyspnea with exertion) are less likely than with pectus excava-
tum, and some report no physical limitations related to this condition (LOE 5).
33
A pec-
tus carinatum deformity often leads to psychologic issues for a child because of the
unsightly protuberant chest. In some instances, chest pain is noted. It is theorized
that this is because of compression of intercostal nerves between adjacent costo-
chondral cartilages. The pain is said to be sharp and brief in quality, and radiates to
the epigastrium (LOE 5).
33
The diagnosis of pectus carinatum is clinical, but chest
radiographs and CT scans add details (LOE 5).
32
Gokhale & Selbst 58
Surgical correction of this deformity has been the mainstay of treatment. However,
there is no evidence of changes between preoperative and postoperative pulmonary
or cardiac function tests for these patients (LOE 5).
33
A retrospective review of 100 pa-
tients with pectus carinatum showed a custom fitted, unobtrusive chest compression
brace (worn for 14 to 16 hours/day for 2 years) was just as effective as surgery. In this
study, 29 patients were fitted for a brace and 22 of those were followed more than
6 months. Another 17 patients underwent surgery. Outcomes were successful for all
andtherewere nosignificant complications ineither group. This study was not well con-
trolled and 57 patients had no specific treatment. Those children with no therapy were
monitored during the 7-year study period, but their outcome is not reported (LOE 4).
34
Marfan Syndrome
Chest wall deformities are common in Marfan syndrome and these patients are at
risk for serious complications, which could lead to chest pain and death. Marfan
syndrome is an autosomal dominant disorder of connective tissue with an incidence
of 1 in 10,000 in the general population (LOE 5).
35
In approximately 15% of cases,
there is no family history for Marfan syndrome, indicating a new mutation. Patients
with Marfan syndrome have clinical findings involving three major organ systems:
skeletal, cardiac, and ocular. Some of the skeletal abnormalities associated with
this syndrome include increased height and arm span, scoliosis, thoracic lordosis,
and disorders of the anterior chest, including pectus deformities (LOE 5).
26
Approx-
imately 66% of patients with Marfan syndrome have pectus excavatum or pectus
carinatum (LOE 5).
36
Severe pectus excavatum may impact on subsequent cardio-
thoracic procedures that many patients with Marfan syndrome require. Also, a se-
vere pectus deformity, in association with scoliosis or lordosis may compromise the
patients respiratory status by reducing lung capacity in children with Marfan syn-
drome. Because of these potential problems, Arn and colleagues
37
recommends
surgical repair of pectus excavatum in patients with Marfan syndrome after the pa-
tient becomes skeletally mature (LOE 3).
Patients with Marfan syndrome may present with chest pain because the connec-
tive tissue defect puts them at risk for spontaneous pneumothorax. These patients
are also at risk for dissection of the aorta. Progressive aortic root dilatation occurs
in 80% to 100% of cases. Because both such conditions may be life threatening,
the complaint of chest pain in a patient with suspected Marfan syndrome must be
taken seriously. Echocardiography facilitates detection of patients with cardiac com-
plications and is recommended for all patients with this condition (LOE 2).
38
Summary
When a child presents with chest pain:
1. Take a careful history and focus on:
Onset of painacute pain is more likely to have an organic etiology
Pain wakes child from sleepmore likely to have an organic etiology
Pain associated with exertion, syncopemore likely to be cardiac in nature, or
exercise-induced asthma
Report of fevermore likely to be pneumonia; consider myocarditis, pericarditis
Description of midsternal burning pain, worsens when recumbentconsider
gastroesophageal reflux
History of heart diseasepain is sometimes related to underlying condition
(often just anxiety about the underlying condition)
Chest Pain and Chest Wall Deformity 59
Serious associated conditions (long-standing diabetes mellitus, Kawasaki dis-
ease, asthma, Marfan syndrome, lupus)these children are at risk for serious
complications like ischemia, pneumothorax, pleural effusion
Stressful life events that correlate with onset of painconsider psychogenic pain
(anxiety)
Grade: Moderate
Level of evidence: Mostly prospective or cohort studies, some retrospective studies
2. Perform a complete physical examination and focus on:
Respiratory distress, abnormal vital signsconsider transfer to ED
Decreased breath sounds, palpable subcutaneous airconsider pneumonia,
pneumothorax
Wheezingconsider asthma and pain related to complications like pneumome-
diastinum, pneumothorax
Abnormal auscultation of the heart (pathologic murmur, rub, arrhythmia)con-
sider pericarditis, myocarditis, SVT, structural heart disease
Feverconsider pneumonia, myocarditis, pericarditis
Evidence of traumaconsider pneumothorax, chest wall injury
Reproducible painconsider musculoskeletal pain, costrochondritis
Drooling in a young childconsider foreign body (coin) ingestion
Tall, thin patientconsider pneumothorax
Grade: Moderate
Level of Evidence: Prospective studies, retrospective studies, case series, case
reports
3. Consider a chest radiograph if (see Table 2):
Unexplained pain of acute onset
Respiratory distress, abnormal chest examination
Abnormal cardiac examination
Significant cough
Fever
Drooling, gagging, young child
Underlying heart disease or serious medical problems
Grade: Moderate
Level of Evidence: Prospective studies, retrospective studies, case series, case
reports
4. Consider an electrocardiogram if (see Table 2):
Pain associated with exercise, syncope
Abnormal cardiac examination
Fever
Underlying serious medical problems (Kawasaki disease, long-standing diabetes
mellitus, congenital heart disease)
Grade: Moderate
Level of Evidence: Retrospective studies, case series, case reports
5. Consider further testing:
D-dimer, chest CT scanif patient has increased risk for pulmonary embolism
(coagulation disorder, recent abortion, trauma, takes oral contraceptives)
Gokhale & Selbst 60
Drug screen for cocaineif anxious adolescent, hypertension, tachycardia
present
Echocardiogramif cardiac disease suspected
Holter monitorif arrhythmia suspected
Exercise stress test, pulmonary function testsif pain is related to exercise
Grade: Low
Level of Evidence: Retrospective studies, case series, case reports
6. Begin treatment directed at underlying etiology:
Bronchodilators for asthma-related pain
Antibiotics for suspected pneumonia
H-2 blocker or proton pump inhibitor for midsternal burning pain
Analgesics for musculoskeletal pain
Grade: Low
Level of Evidence: Prospective studies, retrospective studies, case series, case
reports
7. Treat idiopathic or undiagnosed pain:
Analgesics for all (acetaminophen or ibuprofen)
Consider H-2 blocker or proton pump inhibitor as a therapeutic trial
Arrange follow-up care
Grade: Low
Level of Evidence: Prospective studies, retrospective studies, expert opinion
8. Refer patients if:
Significant distress, traumadirect referral to ED
Pleural effusion, pneumothoraxdirect referral to ED
Significant anxiety, depressionconsider referral to a psychologist, psychiatrist
Associated syncope, dizziness, exercise inducedconsider referral to
a cardiologist
Abnormal cardiac examinationconsider referral to cardiologist
History of heart diseaseconsider referral to cardiologist
Underlying illness that puts the patient at risk for cardiac diseaseconsider
referral to cardiologist
Esophageal foreign bodyrefer to a specialist for prompt removal
Abdominal pain, burning midsternal painconsider referral to a general pediatri-
cian or gastroenterologist
Persistent wheezingconsider referral to a general pediatrician or pulmonologist
Grade: Moderate
Level of Evidence: Prospective studies, retrospective studies, expert opinion
SUMMARY
Chest pain and chest wall deformities are common in children. Chest pain is often a re-
current, chronic symptom. Although most children with chest pain have a benign diag-
nosis, some have a serious etiology for pain, so the complaint must be addressed
carefully. Unfortunately, there are few prospective studies to evaluate this complaint
in children. Table 3 summarizes the prospective studies on pediatric chest pain.
Most available studies involve small numbers and are not well controlled. Serious
causes for chest pain are rare, making it difficult to develop clear guidelines for
Chest Pain and Chest Wall Deformity 61
Table 3
Summary of prospective studies on chest pain
Name Setting Patients Included Etiology of Chest Pain Follow-Up Limitations
Driscoll DJ, et al.
(1976)
Outpatient, ED, or
Cardiac Clinic at
Milwaukee Childrens
Hospital
43 (40 agreed to
participate) patients in
9 weeks with a primary
complaint of chest pain
Idiopathic 18/40 (45%)
Costochondritis 9/40
(23%)
Bronchitis/cough 5/40
(13%)
Muscle strain 2/40 (5%)
Direct trauma 2/40 (5%)
Miscellaneous (10%):
Sickle cell disease 1/40
(3%)
Lobar pneumonia 1/40
(3%)
Viral syndrome 1/40 (3%)
Disc space narrowing 1/40
(3%)
Telephone follow-up at
4 to 8 weeks, contacted
31/40 patients
(1) 3 patients not
included.
(2) Small number from
various settings (none
fully represented).
(3) Were categories
established in ad-
vance or for
convenience based
on results?
Massin MM, et al.
(2004)
ED and Cardiac Clinic in
Liege, Belgium
168 ED patients with
primary complaint of
chest pain and 69
patients referred to
cardiac clinic for
primary complaint of
chest pain
ED
Chest wall pain 108/168
(64%)
Pulmonary 21/168 (13%)
Psychologic 15/168 (9%)
Cardiac 9/168 (5%)
Traumatic 8/168 (5%)
Gastrointestinal 6/158
(3%)
Herpes zoster 1/168 (1%)
Cardiac Clinic
Chest Wall pain 61/69
(81%)
Cardiac / SVT 5/69 (7%)
Respiratory 3/69 (4%)
Passive follow-up
through medical
records available,
unclear for what time
period
(1) ED patients only ex
amined by a resident
physician?
(2) Idiopathic pain
lumped with chest
wall pain so cannot
distinguish the two
with statistical
markers.
(3) 23% of patients from
outside the EU, so
may have included
many travelers?
G
o
k
h
a
l
e
&
S
e
l
b
s
t
6
2
Rowe BH, et al.
(1990)
ED at Childrens Hospital
of Eastern Ontario,
Ottawa, Canada
336 patients with
complaint of
chest pain over
1 year
Chest wall pain 90/325
(28%)
Pulmonary 60/325 (19%)
Traumatic 49/325 (15%)
Idiopathic 39/325 (12%)
Psychogenic 17/325 (5%)
Miscellaneous (21%)
Upper respiratory tract
30/325 (99%)
Abdominal pain referred
27/325 (89%)
Cardiac 5/325 (29%)
No formal follow-up,
but authors felt that
adverse outcomes
would be made
known to them
because of the nature
of the common health
system and their role
as a referral center for
serious pediatric
conditions.
(1) Physical examination
in 325/336 (others
only had surveys).
(2) Authors assumed that
they would know
about adverse
outcomes because
children always come
to their hospital from
the specific referral
area.
Selbst SM, et al.
(1988)
ED at Childrens Hospital
of Philadelphia
407 children with
complaint of
chest pain over
1 year
Idiopathic 21%
Musculoskeletal 15%
Cough 10%
Costochondritis 9%
Psychogenic origin 9%
Asthma 7%
Trauma 5%
Pneumonia 4%
Gastrointestinal
disorders 4%
Cardiac disease 4%
Sickle cell crisis 2%
Miscellaneous 9%
(Including precordial
catch, pneumothorax,
pregnancy, thyroid
disease, drugs, etc.)
Follow-up with EKG/Echo
for ill-defined or
cardiac chest pain. Also
had follow-up of 147
patients for 6 months
and 51 patients for 21
years in separately
published results.
(1) 23% of patients only
seen by a resident
physician.
(2) Only patients in an
ED, so more acute
patients likely.
(3) Diagnostic studies
were not standard-
izedEKG and CXR
were left to the dis-
cretion of the
clinicians.
(4) No patients had
sudden death related
to chest pain.
Abbreviations: CXR, chest radiograph; ED, emergency department; EKG, electrocardiogram; EU, European Union.
C
h
e
s
t
P
a
i
n
a
n
d
C
h
e
s
t
W
a
l
l
D
e
f
o
r
m
i
t
y
6
3
evaluation andmanagement. Basedon evidence available the following seems reason-
able. A detailed history and physical examination are essential. Although diagnostic
tools such as CXR and EKG are relatively inexpensive, it is not practical or necessary
to obtain these for all children with chest pain. Laboratory tests should be reserved
for those with concerning findings on the history or physical examination. The child
with acute onset of pain, pain that is precipitated by exercise, associated with syncope,
palpitations, or shortness of breath should be evaluated with diagnostic tests such as
CXR and EKG. Also, pain related to a possible coin ingestion, trauma, previous heart
disease, asthma, or Marfan syndrome deserves further study. In addition, any child
with chest pain that also has abnormalities on physical examination (fever, respiratory
distress, abnormal breath sounds, abnormal cardiac examination, obvious trauma, or
concerning vital signs) should have a more thorough investigation. The child who ap-
pears well, has a normal physical examination, and lacks worrisome history noted
above, deserves reassurance and careful follow-up rather than extensive studies.
The level of evidence backing many recommendations in this report is not of supe-
rior quality. Multicenter, controlled trials are needed to provide better evidence for
diagnosis and management of chest pain and chest wall deformities.
REFERENCES
1. Massin MM, Bourguignont A, Coremans C, et al. Chest pain in pediatric patents
presenting to an emergency department or to a cardiac clinic. Clin Pediatr 2004;
43(3):2318.
2. Selbst SM, Ruddy RM, Clark BJ, et al. Pediatric chest pain: a prospective study.
Pediatrics 1988;82:31923.
3. Rowe BH, Dulberg CS, Peterson RQ, et al. Characteristics of children presenting
with chest pain to a pediatric emergency department. CMAJ 1990;143(5):38894.
4. Driscoll DJ, Glicklich LB, Gallen WJ. Chest pain in children: a prospective study.
Pediatrics 1976;57:64851.
5. Brenner JI, Ringel RE, Berman MA. Cardiologic perspectives of chest pain in
childhood: a referral problem? To whom? Pediatr Clin North Am 1984;31:124158.
6. Swenson JM, Fischer DR, Miller SA. Are chest radiographs and electrocardio-
grams still valuable in evaluating pediatric patients with heart murmurs or chest
pain? Pediatrics 1997;99(1):13.
7. Roodpeyma S, Sadeghian N. Acute pericarditis in childhood: a 10-year experi-
ence. Pediatr Cardiol 2000;21(4):3637.
8. Desai A, Patel S, Book W, et al. Myocardial infarction in adolescents: do we have
the correct diagnosis? Pediatr Cardiol 2005;26:62731.
9. Lane JR, Ben-Shachar G. Myocardial infarction in healthy adolescents. Pediatrics
2007;120:e93843.
10. Berezin S, Medow MS, Glassman MS, et al. Chest pain of gastrointestinal origin.
Arch Dis Child 1988;63:145760.
11. Sabri MR, Ghavanini AA, Haghighat M, et al. Chest pain in children and adoles-
cents: epigastric tenderness as a guide to reduce unnecessary work-up. Pediatr
Cardiol 2003;24:35.
12. Lipsitz JD, Masia-Warner C, Apfel H, et al. Anxiety and depressive symptoms and
anxiety sensitivity in youngsters with noncardiac chest pain and benign heart
murmurs. J Pediatr Psychol 2004;29(8):60712.
13. Selbst SM, Ruddy R, Clark BJ. Chest pain in children: follow-up of patients
previously reported. Clin Pediatr 1990;29:3747.
Gokhale & Selbst 64
14. Miller A, Texidor TA. Precordial catch: a neglected syndrome of precordial pain.
J Am Med Assoc 1955;159:13645.
15. Reynolds JL. Precordial catch syndrome in children. South Med J 1989;82:
122830.
16. Wilcox DT, Glick PL, Karamanoukian HL, et al. Spontaneous pneumothorax:
a single-institution, 12-year experience in patients under 16 years of age.
J Pediatr Surg 1995;30(10):14524.
17. Damore DT, Dayan PS. Medical causes of pneumomediastinum in children. Clin
Pediatr 2001;40:8791.
18. Uva JL. Spontaneous pneumothoraces, pneumomediastinum and pneumoperito-
neum: consequencesof smokingcrackcocaine. Pediatr EmergCare1997;13:245.
19. Rajpurkar M, Warrier I, Chitiur M, et al. Pulmonary embolismexperience at a sin-
gle childrens hospital. Thromb Res 2007;119(6):699703.
20. Sirachainan N, Chuanswmrit A, Angchaisuksiri P, et al. Venous thromboembolism
in Thai children. Pediatr Hematol Oncol 2007;24(4):24556.
21. Weins L, Sabath R, Ewing L. Chest pain in otherwise healthy children and adoles-
cents is frequently causedby exercise-inducedasthma. Pediatrics 1992;90:3503.
22. Tan TQ, Mason EO, Wald ER, et al. Clinical characteristics of children with compli-
catedpneumonia causedby Streptococcus pneumoniae. Pediatrics 2002;110:16.
23. Grossman LK, Caplan SE. Clinical laboratory, and radiological information in the
diagnosis of pneumonia in children. Ann Emerg Med 1988;17(1):436.
24. Haller JA, Loughlin GM. Cardiorespiratory function is significantly improved fol-
lowing corrective surgery for sever pectus excavatum. J Cardiovasc Surg
2000;41:12530.
25. Zhao L, Feinberg MS, Gaides M, et al. Why is exercise capacity reduced in
subjects with pectus excavatum? J Pediatr 2000;136:1637.
26. Ellis DG. Chest wall deformities in children. Pediatr Ann 1989;18(3):1615.
27. Mueller C, Saint-Vil D, Bouchard S. Chest x-ray as a primary modality for preop-
erative imaging of pectus excavatum. J Pediatr Surg 2008;43:713.
28. Park JM, Farmer AR. Wolff-Parkinson-White syndrome in children with pectus
excavatum. J Pediatr 1988;112(6):9268.
29. Shamberger RC, Welch KJ, Sanders SP. Mitral valve prolapse associated with
pectus excavatum. J Pediatr 1987;111(3):4046.
30. Malek MH, Berger DE, Housh TJ, et al. Cardiovascular function flowing surgical
repair of pectus excavatuma meta-analysis. Chest 2006;130:50016.
31. Guntheroth WG, Spiers PS. Cardiac function before and after surgery for pectus
excavatum. Am J Cardiol 2007;99:17624.
32. McGuigan RM, Azarow KS. Congenital chest wall defects. Surg Clin North Am
2006;86:35370.
33. Golladay ES, Golladay GJ. Chest wall deformities. Indian J Pediatr 1997;64:
33950.
34. Frey AS, Garcia VF, Brown RL, et al. Non-operative management of pectus cari-
natum. J Pediatr Surg 2006;41:405.
35. Giampietro PF, Raggio C, Davis JG. Marfan syndrome: orthopedic and genetic
review. Curr Opin Pediatr 2002;14:3541.
36. Pyeritz RE, McKusick VA. The Marfan syndrome: diagnosis and management.
N Engl J Med 1979;300:7727.
37. Arn PH, Scherer LR, Haller JA. Outcome of pectus excavatum in patients with
Marfan syndrome and in the general population. J Pediatr 1989;115:9548.
38. Van Karnebeek CDM, Naeff MSJ, Mulder BJM, et al. Natural history of cardiovas-
cular manifestations in Marfan syndrome. Arch Dis Child 2001;84:12937.
Chest Pain and Chest Wall Deformity 65
Recurrent Respi ratory
I nfecti ons
AndrewBush, MBBS (Hons), MA, MD, FRCP, FRCPCH
a,b,
*
This article begins with a symptom-based approach to the diagnosis of the child who
has recurrent infections of the upper or lower respiratory tract, or of both. Because
the differential diagnosis is huge, it is summarized in tables, but no attempt is made
todescribeindetail every conceivableconditionthat canpresent (eg, multifocal consol-
idation). The second section discusses the presentation of a few specific respiratory
conditions that may present as recurrent upper and/or lower respiratory tract infection
(eg, cystic fibrosis [CF]). For reasons of space, this article does not discuss the details of
specific therapies for these conditions. The problem in trying to provide an evidence-
based reviewof this topic is that there is very little, if any, evidence to review. The meth-
odology required would be to recruit prospectively a large cohort of children presenting
with a particular condition (eg, multifocal consolidation), to investigate themin detail, to
generate predictive indices for particular conditions or indices that would exclude the
need for certain tests, and to validate these indices in at least one other population.
Although a systematic approach has been described for cough,
1
it has not been vali-
dated in a second population, and in most cases there is not even a discovery
population.
Most children experience one or more acute respiratory infections. The challenge is
first to decide when the time has come to move fromsymptomatic therapy to perform-
ing diagnostic testing, then to determine which tests need to be done and when test-
ing should be discontinued, and finally to institute specific therapies for the childs
underlying condition.
The key decision, whether or not to investigate, is always made on the basis of clin-
ical judgment and experience. Factors to be considered vary with the different specific
conditions and are discussed later. General pointers are listed in Boxes 13.
a
Imperial School of Medicine at National Heart and Lung Institute, London, UK
b
Department of Paediatric Respiratory Medicine, Royal Brompton Hospital, Sydney Street,
London SW3 6NP, UK
* Department of Paediatric Respiratory Medicine, Royal Brompton Hospital, Sydney Street,
London SW3 6NP, UK.
E-mail address: a.bush@rbh.nthames.nhs.uk
KEYWORDS
Pneumonia
Croup
Otitis media
Immunodeficiency
Cystic fibrosis
Primary ciliary dyskinesia
Human immunodeficiency virus
Gastro-esophageal reflux
Pediatr Clin N Am 56 (2009) 67100
doi:10.1016/j.pcl.2008.10.004 pediatric.theclinics.com
0031-3955/08/$ see front matter 2009 Elsevier Inc. All rights reserved.
Unless otherwise stated in this article, the level of evidence should be assumed to
be low, based on informal consensus and case reports or series.
CLINICAL SCENARIOS: UPPER AIRWAY
Most children presenting with recurrent upper airway infection are normal. Immunode-
ficiency, however, can present with upper airway problems.
2,3
Particular triggers for
further investigation include:
4
Eight or more new ear infections within a year
Two or more serious sinus infections (eg, requiring intravenous antibiotic treatment)
within a year
Persistent oral or cutaneous candidiasis
Two or more months of continuous antibiotics with no effect
The need for intravenous antibiotics to clear infections
Associated systemic features including recurrent deep-seated or skin abscesses
or infections, recurrent pneumonia, failure to thrive, positive family history of
immunodeficiency
Recurrent Viral Colds
A large, community-based study documented that in childhood the median number of
viral colds is five per year, but more than 10% of children have 10 or more colds per
Box1
Pointers that suggest early investigation of a child with recurrent infection may be indicated
The acronymSPUR (Severe, Persistent, Unusual, Recurrent) may be a useful mnemonic.
Respiratory infection plus extrapulmonary infections or other disease (eg, arthropathy)
Positive family history: unexplained death, infections or multisystem disease
Severe infection
Persistent infection and failure of expected recovery
Unusual organisms (eg, Pneumocystis jiroveci)
Recurrent infection
Box 2
Pointers in the history of a child presenting with respiratory symptoms that should lead
to further investigation
Is the child/family in fact describing true wheeze?
Marked chronic upper airway symptoms: snoring, rhinitis, sinusitis
Symptoms from the first day of life
Very sudden onset of symptoms
Chronic moist cough/sputum production (differentiate from recurrent acute symptoms)
More severe symptoms (or irritability) after feeds and when the child is lying down (vomiting
and choking on feeds suggests gastroesophageal reflux or aspiration syndrome)
Any feature of a systemic immunodeficiency
Continuous, unremitting, or worsening symptoms
Bush 68
year.
5,6
A viral cold usually is a trivial illness. The mean duration of symptoms is around
8 days, but the normal range extends beyond 2 weeks.
6
Symptoms are nasal conges-
tion, rhinorrhea, cough, sore throat, and fever. Thus a normal child may have symp-
toms of the common cold for nearly 6 months in the year. The misinterpretation of
common symptoms as wheeze
710
may lead to an incorrect diagnosis of asthma.
Not unexpectedly, attendance in child day care facilities early in life increases the
risk of viral colds.
11
The frequency and duration of colds may come as a surprise, par-
ticularly to first-time parents, and misconceptions about the need for treatment are
common.
12
The issue of virally induced wheezing is discussed under in the section
devoted to the lower airway.
Recommendations
Intheabsenceof anyother worryingfeaturesonhistoryandexamination(Boxes2and3),
isolated recurrent viral colds do not require further investigation unless the frequency is
morethan15per year, andthedurationhabituallyismorethan15daysper episode. Level
of evidence: low.
Rhinitis
Intermittent acute rhinitis must be distinguished fromchronic rhinitis, which has a wider
differential diagnosis. The definitions of acute and persistent rhinitis are variably de-
fined; one group defined persistent rhinitis as occurring at least 4 days a week for
at least 4 weeks;
13
another group holds that acute rhinitis may last as long as
12 weeks.
14
The evidence base on the timing and nature of appropriate investigations
in persistent rhinitis is scanty; however, recent combined adult and pediatric guide-
lines have listed potential investigations that may be useful.
14
The two common
causes are infective and allergic rhinitis, and skin prick testing may be indicated.
Unilateral rhinitis should lead to consideration of anatomic abnormalities such as
unilateral choanal stenosis or the presence of a foreign body. The combination of per-
sistent rhinitis and lower respiratory tract symptoms should prompt diagnostic consid-
eration of allergic rhinitis and asthma (the most common cause); primary ciliary
dyskinesia (PCD), especially with neonatal onset of rhinitis; CF (especially if there
are nasal polyps); and Wegeners granulomatosis (seen in 21 of 25 patients in one
series).
15
Recommendations
Persistent rhinitis usually does not require detailed investigations. Evidence of allergic
sensitization may be sought, and empiric therapeutic trials are reasonable, unless
Box 3
Pointers in the physical examination of a child presenting with respiratory symptoms that should
lead to further investigation
Digital clubbing, signs of weight loss, failure to thrive
Upper airway disease: enlarged tonsils and adenoids, prominent rhinitis, nasal polyps
Unusually severe chest deformity (Harrisons sulcus, barrel chest)
Fixed monophonic wheeze
Stridor (monophasic or biphasic)
Asymmetric wheeze
Signs of cardiac or systemic disease
Recurrent Respiratory Infections 69
there is evidence that rhinitis is part of a more generalized disease. Level of evidence:
low.
Recurrent Tonsillitis and Pharyngitis
In childhood, significant tonsillar disease manifests commonly as either obstructive
sleep apnea (not discussed here) or recurrent acute tonsillitis. Children are considered
to have an episode of significant tonsillitis if they satisfy at least one of the following
criteria: (1) an oral temperature of at least 38.3
C; (2) cervical lymphadenopathy (en-
larged by > 2 cm or tender cervical nodes); (3) tonsillar or pharyngeal exudate; and
(4) a positive culture for group A b-hemolytic streptococcus. Conventionally, tonsillec-
tomy is indicated if there have been seven or more documented episodes in the pre-
ceding year, five or more in each of the 2 preceding years, or three or more in each of
the preceding 3 years.
16
The other indication for tonsillectomy is obstructive sleep ap-
nea. One study has suggested tonsillectomy is a cost-effective strategy for treating
obstructive sleep apnea,
17
but in a randomized, controlled trial the risks of surgery
were thought to outweigh any benefits.
18
Furthermore, about two thirds of operations
are performed for less stringent and thus even less evidence-based criteria.
19
Usually
no other investigations are performed for isolated recurrent tonsillitis in the absence of
features listed in Boxes 2 and 3, but there is no good-quality evidence to inform the
decision making about the need for further investigation.
Recommendations
Isolated recurrent tonsillitis and pharyngitis do not require further investigation in the
absence of any other worrying features (see Boxes 2 and 3). Level of evidence: low.
Sinusitis
Acute sinusitis in children is common and usually a self-limiting disease that requires
no investigation. Further investigation, usually in collaboration with an ear, nose, and
throat surgeon, should be considered in children who have recurrent acute or severe
chronic sinusitis. The differential diagnosis includes respiratory allergy, CF (particularly
if nasal polyps or other features of this condition are present), PCD (nasal polyps are
said to be common in this condition, but this has not been the authors experience),
and systemic immunodeficiency.
14
Mechanical obstruction of the ostia should be
considered; the most common isolated cause is an antrachoanal polyp. Gastro-
esophageal reflux also enters the differential diagnosis or may be a significant comor-
bidity.
20
Of note: laryngopharyngeal reflux disease may differ from the more usual
patterns of reflux, being more common when the patient is upright, and extending
into the hypopharynx.
21
Many patients are unaware of the extent of this problem.
22
In a child who has recalcitrant sinusitis, allergy should be excluded with skin prick
tests or radioallergosorbent tests to aeroallergens; the exact panel should be deter-
mined by the childs environment. In very young children, genuine allergy may be pres-
ent, but the skin prick test may not have become positive. As discussed later, it may be
necessary to exclude CF, PCD, and immunodeficiency. Imaging of the sinuses with CT
or MRI may enable rare anatomic diagnoses to be made.
23
Endoscopy may need to be
considered for unilateral disease. Endoscopy also can indicate the presence of reflux
disease, which may be associated with one or more of the following observations;
24
Cobblestoning of the mucosa of the larynx and pharynx
Inflammation of the upper respiratory tract
Sinus involvement
Rhinorrhea
Bush 70
Subglottic stenosis
Velopharyngeal insufficiency
Pharyngotracheitis
Tracheomalacia
Diagnosis may be confirmed by a pH study, or a therapeutic trial of medication may
be given.
Recommendations
Most children who have sinusitis need no investigation. Unusually severe or chronic
sinusitis may be the presenting feature of a local or systemic immunodeficiency or
of gastroesophageal reflux. There is little evidence on which to make specific recom-
mendations about the nature and timing of the most appropriate investigations for
sinusitis. Level of evidence: low.
Recurrent Acute and Chronic Otitis Media with Effusion
Acute otitis media is common: one study reported 1.72 episodes per child per year be-
tween 6 months and 3 years of age.
6
Viral colds were complicated by acute otitis me-
dia (37%) and otitis media with effusion (24%).
24
Chronic otitis media with effusion
may be a sign of respiratory allergy (for investigation, see the previous discussion of
sinusitis) and immunodeficiency. Eight or more new ear infections per year should
be considered a sign of potential immunodeficiency.
4
Curiously, middle ear disease
is not increased greatly in CF but is an important feature of PCD. Particular features
pointing to a diagnosis of PCD include early-onset and severe hearing loss and pro-
longed offensive otorrhea after tympanostomy tube insertion. Typically, there is
chronic infection with Pseudomonas aeruginosa that can be eliminated only with qui-
nolone eardrops. The child has an obvious smelly discharge running down the side of
the face, and there is no improvement in hearing. Unfortunately, multiple procedures
often are performed before the diagnosis is made.
25
Recommendations
Most children who have otitis media with or without effusion need no investigation.
The possibility of underlying immune deficiency, and in particular PCD, should be
borne in mind. There is little evidence on which to make specific recommendations
about the nature and timing of the most appropriate investigations for middle ear dis-
ease. Level of evidence: low.
Croup and other Causes of Acute Upper Airway Obstruction
Viral croup typically presents with the sudden onset of barking cough, stridor, and re-
spiratory distress in the setting of a coryzal illness. The acute management and differ-
ential diagnosis are well described in two recent reviews.
26,27
Importantly, medical
management with oral dexamethasone or another oral steroid and nebulized adrena-
line should permit intubation to be avoided. Generally infants only have a single or very
few episodes, but occasionally patients experience multiple episodes that extend into
mid-childhood. In neither review is there any recommendation as to when and how to
investigate further. The differential diagnosis includes spasmodic croup, an unsus-
pected congenital structural abnormality such as a web, subglottic hemangioma,
and acquired laryngeal disorders such as a foreign body, subglottic stenosis second-
ary to previous intubation, or respiratory papillomatosis. Stridor caused by a subglottic
hemangioma may present as croup and apparently respond to steroids, because they
lead to shrinkage, only to recur subsequently as the hemangioma re-expands.
28
Recurrent Respiratory Infections 71
Recommendations
A single episode of uncomplicated croup with rapid and complete recovery does not
require further investigation. Croup should be investigated if
1. The episode is severe (prolonged intubation required).
2. There are atypical features in the history or on examination.
3. Symptoms or signs persist beyond an arbitrary time period (eg, 2 weeks). Croup
can be complicated by subglottic stenosis if intubation has been required, and sub-
glottic stenosis enters the differential diagnosis of persistent stridor in a previously
well child.
4. There are recurrent episodes, particularly if severe.
There is, however, insufficient evidence to identify the point at which investigation is
warranted. Level of evidence: low.
Further investigations in upper airway obstruction
Before any investigation is undertaken, a detailed history and examination should be
performed. If the child is old enough, a flowvolume curve should be performed; the
typical truncated shape of extrathoracic obstruction may be seen (Fig. 1). In younger
infants, a tidal flowvolume loop may be suggestive of large airway obstruction.
29
A
neck radiograph may reveal a radiopaque foreign body but generally is not helpful.
The most useful investigations are a fiberoptic bronchoscopy, under general anesthe-
sia using a pernasal approach via a facemask held by the anesthetist; and serum cal-
cium levels (hypocalcemia may present as recurrent stridor) and C
1
-esterase inhibitor
levels (deficiency presents as recurrent subglottic swelling leading to stridor).
The relationship between croup, croup with wheeze, and recurrent croup with
subsequent asthma is controversial. In one study
30
physician-diagnosed croup was
inversely associated with atopy at school age. The Oslo study showed that atopic chil-
dren who had a diagnosis of croup were less likely to have a subsequent diagnosis of
asthma, whereas non-atopic children were more likely to have a later diagnosis of
asthma.
31
Another study showed that the odds ratio for a diagnosis of asthma was
increased by a diagnosis of croup and increased still further if croup was recurrent.
32
Croup with wheeze may be more predictive of subsequent asthma.
33
Overall, although
croup may be a marker for future asthma in some children, for most children it is an
Fig. 1. Pulmonary function testing. Rigid tracheal obstruction is suggested by abrupt atten-
uation of flows in inspiration and expiration.
Bush 72
isolated illness with no long-term sequelae. Because the early institution of inhaled
corticosteroids has not been shown to prevent recurrent croup and certainly does
not prevent the progression of intermittent wheeze to multi-trigger wheeze,
3438
the
debate about the relationship between croup and asthma is not of practical clinical im-
portance at the moment.
Recently, the most important infectious cause of stridor is bacterial tracheitis.
39
Im-
munization has almost completely abolished acute epiglottitis and laryngeal diphthe-
ria, although these diseases should be considered in the nonimmunized child.
Retropharyngeal abscess, which may be associated with a penetrating foreign
body, is another rare cause of presentation with a crouplike illness, although the child
usually is more toxic.
Recommendations for further investigations
There is no evidence on which to base guidelines for further investigation of children
who have upper airway infections causing stridor not caused by viral laryngotracheitis.
Most pediatricians would not investigate a single episode in an otherwise well child.
Possibly, a single documented episode of type B Haemophilus Influenzae epiglottitis
in a fully immunized child might merit further investigation. Level of evidence: low.
CLINICAL SCENARIOS: LOWER AIRWAY
This section is divided into three parts: chronic productive cough, recurrent wheezing
lower respiratory tract infection, and recurrent radiologic shadowing. This approach
has been found to be useful in personal practice, although some investigations that
cut across clinical scenarios may be described inadequately or, conversely, there
may be repetition. Specific conditions that are referred to in the differential diagnosis
in these sections (eg, CF, PCD, and immunodeficiency) are discussed in the final sec-
tions of the article.
Many children are too young for pulmonary function testing, although increasingly
techniques such as airway resistance using the interrupter technique (R
INT
)
40
and the
lung clearance index
4143
are applicable in preschool-age children. The shape of the
tidal flowvolume loop may suggest an obstructive picture.
29
If there are facilities to
carry out spirometry, lung volumes, and carbon monoxide transfer, and the child is
able to performthese tests, much useful information can be obtained. Pulmonary func-
tion testing provides only part of the clinical information, however, and the only specific
diagnoses that can be made in the pulmonary function laboratory are exercise-induced
asthma and hyperventilation syndromes.
Airway disease is suggested by the combination of hyperinflation (raised residual
volume, functional residual capacity, and total lung capacity) with reduced 1-second
forced expiratory volume (FEV
1
) and FEV
1
to forced vital capacity (FVC) ratio. Elevated
carbon monoxide transfer (DL
CO
) is suggestive of asthma or bronchiectasis, whereas
reduced DL
CO
suggests parenchymal destruction as well as airflow obstruction (eg,
the sequelae of chronic lung disease of prematurity). Parenchymal disease is
suggested by reduced FEV
1
and FVC, with a normal or elevated FEV
1
:FVC ratio and
reduced residual volume, functional residual capacity, and total lung capacity. A
high DL
CO
per liter of accessible lung volume suggests chest wall restriction, such
as scoliosis. An isolated reduction in DL
CO
suggests pulmonary vascular disease,
such as recurrent pulmonary embolism or primary pulmonary hypertension. An iso-
lated elevation in DL
CO
suggests recent pulmonary hemorrhage.
The shape of the flowvolume loop may give additional clues. Rigid tracheal
obstruction is suggested by abrupt attenuation of flows in inspiration and expiration
(see Fig. 1). Attenuation in only the expiratory limb suggests variable obstruction
Recurrent Respiratory Infections 73
(eg, malacia) of the intrapulmonary trachea or large airways. Isolated attenuation of the
inspiratory limb may be caused by variable obstruction of the extrathoracic trachea,
inspiratory muscle (diaphragm) dysfunction, or stiff lungs. Marked variability, and in
particular a very variably impaired inspiratory flowvolume curve, is highly suggestive
of vocal cord dysfunction.
44
Another important issue is the state of the childs immune system. In the following
sections, it is assumed that the child does not have a known and diagnosed immune
deficiency but is thought at presentation to have a normal immune system. The special
problems of the immunodeficient child are discussed in a separate section or are re-
ferred to specifically where applicable. For example, recurrent infiltrates would be in-
vestigated very differently, and much more urgently, in a child who has pancytopenia
after chemotherapy than in an otherwise well child who has similar radiologic
appearances.
Chronic, Usually Productive Cough
It is important to distinguish recurrent, acute, productive-sounding cough, which usu-
ally is secondary to a series of viral colds, from a continuous productive cough, which
needs investigation if it persists beyond a certain time period. In a group of children
who had cough severe enough to be referred to a specialist pediatrician and who
then were submitted to a detailed diagnostic algorithm after 3 weeks of cough (nearly
90% of which was productive), more than 20% got better spontaneously, suggesting
this duration of cough is too short to merit referral.
1
The British Thoracic Society rec-
ommends 8 weeks as the definition of chronic cough,
45
but this recommendation is
not based on any firm evidence. Clearly context is crucial: if the child is clinically un-
well, investigation may need to begin at once, and it would be wrong to specify a du-
ration that warrants investigation. In a hospital context, it is clear that parental report of
a productive cough correlates well with the finding of secretions in the lower airway.
46
The largest study systematically investigating children who had chronic cough used
a protocol of successively performing laboratory tests (sweat chloride, common CF
mutations, serum Mycoplasma pneumoniae IgM, and Bordetella pertussis IgA serol-
ogy, immunoglobulins G, A, M, and E and IgG subclasses), bronchoscopy (occasion-
ally induced sputum), chest high-resolution CT (HRCT), and a pH probe. Finally, when
necessary, blind trials of therapy were performed. A number of important lessons
emerged. The first is that the adult causes of chronic cough (asthma, gastroesopha-
geal reflux disease, and upper airway disease) are uncommon causes of chronic
cough in children. Indeed, many lines of evidence support the viewthat isolated cough
in children is rarely caused by asthma and should not be treated as such.
47,48
The
most common cause identified was persistent bacterial bronchitis (PBB) in nearly
40%of children.
1
In this report the diagnostic criteria for confirmed PBB were a history
of chronic moist cough, a positive bronchoalveolar lavage fluid (BAL) culture, and re-
sponse to antibiotic treatment (amoxicillin/clavulanic acid suspension) with resolution
of the cough within 2 weeks. Probable PBB was defined as a history of chronic moist
cough and either positive BAL culture or immediate response to antibiotic therapy with
resolution of the cough within 2 weeks. In most cases of probable PBB, the BAL cul-
ture reached only 10
3
or 10
4
colony-forming units (cfu)/mL rather than an arbitrary
10
5
cfu/mL, or the patients required additional antibiotic therapy before the cough dis-
appeared. A subsequent article suggested that multiple courses of antibiotics were
needed to resolve the cough,
49
and that the rapid response to a short course reported
by Marchant and colleagues
1
might reflect the relatively short duration of symptoms in
their group. It also is not clear whether it would be more cost effective to prescribe an
empiric course of antibiotics before embarking on investigations.
Bush 74
PBB is undoubtedly a real and important entity, but most clinicians believe that the
diagnostic criteria should be tighter than those listed in the previous paragraph. PBB is
a diagnosis of exclusion; it should be suspected in the child who has chronic produc-
tive cough lasting longer than 8 weeks, and investigations should show a neutrophilic
BAL with positive cultures (with normal BAL cytology, a positive culture may represent
a contaminant) but also must eliminate bronchiectasis, gastroesophageal reflux dis-
ease, and local and systemic immunodeficiency as a cause for the symptoms. BAL
findings alone are insufficient for the diagnosis. The relationship between PBB and
subsequent idiopathic bronchiectasis is unclear. An attractive hypothesis is that un-
treated PBB can progress to idiopathic bronchiectasis, but at the moment there is
no evidence that PBB is pre-bronchiectatic.
50
There also is no knowledge of the etiol-
ogy; PBB may be the result of a congenital or acquired postinfective localized immune
deficiency, which subsequently may improve. The presence of PBB in children older
than age 10 years suggests that the abnormality is acquired.
Although asthma is not an infectious disease, the problem of cough-variant
asthma is considered here because it is misdiagnosed so frequently. There is no
doubt that cough-variant asthma does exist, but it is rare and is virtually unknown
in non-atopic children. The author is reluctant to diagnose any form of asthma in
the absence of significant breathlessness. Indeed, it is rare to find airway eosino-
philia suggestive of asthma even in atopic children who have cough as their sole
symptom.
48
In children old enough to perform pulmonary function tests, cough-
variant asthma should not be diagnosed unless clear-cut evidence of variable airflow
obstruction can be demonstrated. In the younger child, in whom pulmonary function
testing is not be practical in most circumstances, a three-stage therapeutic trial is
recommended:
1. Commence inhaled corticosteroids. There is some evidence that some children
who seem not to respond to inhaled salbutamol respond to inhaled corticoste-
roids.
51,52
Oral steroids are not recommended because of potential systemic
effects and also because of possible upper airway effects (eg, shrinking adenoidal
tissue), which may confuse the issue. There is no evidence on which to base the
dose and duration of inhaled corticosteroids; anecdotally, a moderately high-
dose (800 mg/d) beclomethasone equivalent for 8 weeks is suggested.
2. Stop therapy after a period of time. The duration of the trial should be sufficient to
ensure that any possible response is detected. If there is no response, the child
does not have cough-variant asthma. An apparent response, however, may in
fact be a spontaneous regression of cough, in which case treatment is not
indicated.
3. Restart therapy only if the symptoms recur on stopping treatment. This precaution
eliminates the possibility of labeling transient symptoms as cough-variant asthma.
Treatment then is titrated down to the lowest dose needed to control symptoms.
It is convenient to consider what role, if any, exhaled nitric oxide measurements
(FeNO) have in the diagnostic process. Nasal NO is discussed in the section devoted
to PCD. In general, there is too much overlap between the FeNO measurements for
CF, bronchiectasis, PCD, and asthma for this test to be of much use in diagnosing in-
dividuals.
53
A very high FeNO (twice the upper limit of normal) was reported only in
children who had asthma. Some individuals, however, seem to have a constitutively
high FeNO in the absence of symptoms,
54
and a high FeNO should not be equated
uncritically with a diagnosis of asthma. At the present time, FeNO cannot be recom-
mended as a diagnostic test in recurrent respiratory infections.
Recurrent Respiratory Infections 75
Recommendations
1. A child who has a true chronic cough (as opposed to recurrent acute cough) of sev-
eral weeks duration should be investigated systematically. The duration of symp-
toms before investigation is not clear but should not exceed 8 weeks and should be
shorter in a child who is unwell. Systematic, protocol-driven evaluation leads to
a high diagnostic yield. Level of evidence: moderate
2. Chronic isolated cough is rarely caused by asthma and should not be treated as
such. Cough-variant asthma usually is a diagnosis of exclusion. Level of evidence:
moderate
3. FeNOis not a useful test in the diagnosis of recurrent respiratory infections. Level of
evidence: moderate to high
Recurrent Wheezing Lower Respiratory Tract Infection
In young children, recurrent wheezing in the lower respiratory tract almost always is
caused by recurrent viral infection. It is important to note that patients families often
use the term wheeze imprecisely. Some European languages do not have such
a term; in England, many different airway sounds may be described as wheeze, in-
cluding upper airway rattling and even stridor.
710
The use of a video questionnaire
may help define the noise. In one study, physician assessment of wheeze correlated
with objective measurements, but parents and nurses were not so accurate.
55
Further-
more, the nomenclature of this condition is confused: wheeze can be defined either by
symptompatternor by epidemiologiccourse. Symptompatternis moreuseful prospec-
tively, and the history should categorize the pattern as either episodic (viral) or multi-
trigger wheeze. Epidemiologically, wheezeis either transient (disappearingafter thefirst
3 years of life) or persistent (present throughout the first 6 years of life). It sometimes is
assumed that the terms viral (episodic) and transient, and multi-trigger and per-
sistent can be used interchangeably, but there is no evidence that this is the case.
Thus, further investigation should be considered in three scenarios:
1. Recurrent acute or chronic nonspecific airway sounds (not true wheeze)
2. Episodic (viral) wheeze
3. Multi-trigger wheeze (usually a combination of episodic, viral-associated symp-
toms and interval, multi-trigger wheeze)
There also has been interest in the role of bacterial coinfection in viral wheeze. The
Copenhagen Prospective Study on Asthma in Childhood (COPSAC) study showed
that positive upper airway cultures for bacterial pathogens in babies are associated
with subsequent wheeze.
56
A smaller study showed that serologic investigation fre-
quently revealed evidence of bacterial coinfection with respiratory virusinduced
wheeze,
57
although features suggestive of a major infection, such as systemic toxicity
and elevation in C-reactive protein, were rare. The most likely hypothesis is that the
propensity for viral wheeze and low-grade mucosal bacterial infection are both man-
ifestations of a subtle and probably maturational mucosal immune deficiency,
58
which
may be related to antenatal events such as maternal smoking
5961
and possibly to epi-
genetic mechanisms.
62
Further discussion of this possibility is beyond the scope of
this article.
Airway sounds that are not true wheeze
Commonly the child has viral colds with relatively prolonged symptoms or nonspecific
upper airway noises that require no treatment other than reassurance of the family.
Symptoms may persist beyond the third birthday. Occasionally, stridor may be
Bush 76
misdiagnosed as wheeze and should be investigated along standard lines; most
would advocate an early bronchoscopy.
Episodic (viral) wheeze
Wheeze with viral colds is common, often is not severe (ie, is not life threatening), but
frequently is a cause of considerable morbidity and loss of time from work for the
childs care givers. In some children, however, the attacks really may be severe. In
an otherwise well child who has mild to moderate episodic wheeze, investigation is
not necessary. If the wheezing illness really is severe, investigation may be indicated,
as discussed later.
Multi-trigger wheeze
In older children, multi-trigger wheeze usually is associated with demonstrable vari-
able airflowobstruction and responds to standard asthma therapy. When no other fea-
ture of the history or examination suggests an alternative diagnosis, no further
investigation is required. One group used a detailed protocol to investigate severely
affected wheezy (episodic and multi-trigger) preschool children.
63
Measurements in-
cluded immunoglobulins and subclasses, a sweat test, nasal ciliary brushings, a pH
probe, HRCT, and bronchoscopy. There was a high yield of abnormal findings,
including gastroesophageal reflux, PBB, and airway eosinophilia, often despite oral
or inhaled steroid therapy. What this group could not demonstrate was whether this
aggressive approach leads to an improved outcome; a prospective clinical trial is
required for this issue to be resolved.
Recommendations
1. Most children who have true wheezing caused by lower respiratory tract infections
do not require further investigation. Level of evidence: moderate
2. Aggressive, protocol-driven investigation of severe wheeze will lead to new
diagnoses, but the clinical relevance of these diagnoses often is not clear. Level
of evidence: moderate.
Recurrent Radiologic Shadowing
The vague term radiologic shadowing is used because many of these conditions
can cause either consolidation or atelectasis. Although radiologic patterns may give
a clue to the diagnosis, the patterns often are nonspecific, and detailed further inves-
tigation usually is indicated.
Recurrent chest infection in lay parlance usually means recurrent episodes of
a productive cough, generally in association with viral colds, and is not the same as
recurrent shadowing on chest radiographs. Recurrent bouts of coughing may require
investigation, as discussed previously, but cough is normal,
64
and the frequency of
cough is notoriously poorly evaluated by parents and children.
6568
At least two epi-
sodes of documented radiologic shadowing are required to merit investigation for
possible recurrent lower respiratory tract infection. A single episode of uncomplicated
lobar pneumonia in an otherwise well and thriving child does not require investigation.
Indeed, if the child is seen by an experienced clinician and is thought to have made
a complete recovery, even a follow-up chest radiograph is not necessary.
69,70
Further
investigation is mandated, however, if the child has had a previous history of unusual
infections, there is a family history of an immune problem or an unexplained death
from infection, there are any features to suggest a systemic illness, or the pneumonia
is at all atypical in its course.
Recurrent Respiratory Infections 77
The child with recurrent shadowing on the chest radiograph should not be assumed
to be having repeated infections, particularly if there is not complete radiologic
clearing between episodes. The differential diagnoses and investigation of recurrent
shadowing in the same area and of multifocal recurrent shadowing are described
here in turn. The reader will need to consult standard texts for the further detailed
investigation of many of these conditions.
Recurrent radiologic shadowing in the same place
A child with two or more radiologically documented episodes of shadowing in the
same lobe or segment, particularly if there is incomplete clearing between episodes
or with a single episode that does not clear should be investigated further. The differ-
ential diagnosis is summarized in Box 4. The radiologic changes of acute pneumonia
may take 6 to 12 weeks or even longer to resolve, depending on the causative
Box 4
Differential diagnosis of recurrent or chronic localized radiographic changes
Right middle lobe syndrome
Localized airway obstruction
Within the lumen
Congenital webs
Endobronchial foreign body
Mucus plug
Carcinoid or other pedunculated tumor
Inflammatory pseudotumor secondary to previous intubation
Within the airway wall
Localized malacia
Localized bronchiectasis (underlying cause must be sought)
Complete cartilage rings
Intramural tumor
Extrinsic compression
Congenital thoracic malformation
Enlarged cardiac chamber caused by right to left shunting, cardiomyopathy
Vascular ring, pulmonary artery sling
Lymph nodes: tuberculosis, lymphoma, other
Mediastinal or lung tumor
Fibrosing mediastinitis
Pulmonary parenchymal disease
Congenital: cystic congenital thoracic malformation
Acquired: infection in residual cystic change after a cavitating pneumonia or tuberculosis
(tumor will be focal and progressive)
First manifestation of a cause of recurrent fluctuating multifocal consolidation (see Box 5)
Bush 78
organism.
71,72
Determining when to investigate thus becomes a matter of clinical judg-
ment, depending on the history, whether the child is improving clinically, and whether
there are any other features suggestive of another condition. There are no evidence-
based recommendations to guide the clinician.
Right middle lobe syndrome probably is the most common clinically encountered
focal consolidation for which there is some evidence to base recommendations. It is
the most common recurrent focal investigation encountered in clinical practice and
thus merits a separate section. Right middle lobe syndrome also may be related to
the conditions listed in Box 4. The definition of right middle lobe syndrome is clinical: at-
electasis of the right middle lobe or lingula persisting for more than 1 month or recurring
twice or more despite treatment.
73
The authors experience is that the lingula is affected
only rarely in comparison with the right middle lobe, although others report right middle
lung disease being as only twice as common as lingula disease.
74
The likely explanation
of the frequency of right middle lobe disease is the anatomy: every bronchoscopist is
familiar with the acute take-off andoften slitlike orifice of the right middle lobe bronchus,
which intuitively makes it likely to be vulnerable to occlusion. A pathologic study of 21
resectedspecimens (adults andchildren) showedbronchiectasis (n510), chronicbron-
chitis and bronchiolitis with lymphoid hyperplasia (n 57), patchy organizing pneumonia
(n 56), atelectasis (n 55), granulomatous inflammation (n 55), and abscess formation
(n 54).
75
These findings obviously represent the most severe cases but suggest that in-
fection is important, and thus early diagnosis and aggressive treatment of infection may
be beneficial. Studies in which BAL was performed documented infection in one third to
one half of cases; H. influenzae was the most common pathogen. Only 2 of 53 subjects
had an endobronchial obstruction seen at bronchoscopy. More than 25%had bronchi-
ectasis, and, unsurprisingly, their outcome after treatment was less good.
73
The relationship between right middle lobe syndrome and atopy and asthma is con-
troversial. One group made the diagnosis more commonly in atopic patients.
74
An-
other group showed an increase in bronchial responsiveness, but not atopy, in
children who had right middle lobe syndrome.
76
By contrast, De Boeck and col-
leagues
77
showed that one third of the children who had been diagnosed with right
middle lobe syndrome had subsequent chronic asthmalike symptoms. It seems likely
(but is unproven) that any hypersecretory respiratory syndrome such as asthma may
be complicated by right middle lobe syndrome, but the series are too small to pick up
such an effect (eg, in the largest recent series only 5 of 53 subjects had an eosinophilic
lavage).
73,76
It would be wise to follow these children carefully.
Recommendations
1. Children who have right middle lobe syndrome may have underlying chronic infec-
tion and bronchiectasis. If radiologic changes have not cleared within 1 month, or if
they recur after treatment, further investigation with bronchoscopy and perhaps
HRCT scanning is indicated. The diagnostic yield of these tests probably is high,
but there are no outcome data to show that aggressive investigation is beneficial.
Level of evidence: moderate
2. The families of children who have right middle lobe syndrome should be advised
that these children are at risk of chronic respiratory symptoms and asthma and
should be followed carefully or should return for re-evaluation at the first signs of
recurrent symptoms. Level of evidence: moderate.
Other recurrent focal abnormalities in a single site
Important steps in the investigation of focal abnormalities are a fiberoptic bronchos-
copy to rule out focal airway disease and HRCT scanning to exclude focal
Recurrent Respiratory Infections 79
parenchymal disease. Other imaging modalities that may help include endobronchial
ultrasound to demonstrate complete cartilage rings and CT reconstruction of the air-
way anatomy. It always is good practice to try to obtain previous imaging, to see if the
abnormality is new or might be congenital. Ideally HRCT should be performed when
the child is not acutely infected, because acute changes may complicate the interpre-
tation of the scans. It is worth considering giving intravascular contrast with the HRCT
to delineate vascular anatomy: if the abnormality has an arterial supply from the ab-
dominal aorta or drains into the systemic circulation, a congenital thoracic malforma-
tion is likely. If mediastinal disease is thought to be an issue, an MRI scan may be
indicated; the lack of radiation makes this modality attractive, but the current require-
ment for general anesthesia for small children in most centers militates against its use
unless essential. An echocardiogram is a simple investigation which is often forgotten
and which may show an enlarged cardiac chamber compressing the bronchus. The
differential diagnosis is wide and is summarized in Box 4. If HRCT and bronchoscopy
have not established the diagnosis, a more invasive approach, including surgical ex-
cision or lymph node biopsy, may be indicated. The possibility that a single-site
change may be the first presentation of a generalized illness should not be forgotten.
Recommendations
1. The differential diagnosis of recurrent or chronic shadowing in a single site is wide,
and investigation is indicated. There is no evidence base to inform the clinician of
the optimal timing of investigation or the optimal sequence of tests. Level of
evidence: low
2. If simple investigations have not yielded a diagnosis, aggressive investigation of
recurrent or chronic shadowing in a single site, including surgical excision or me-
diastinoscopy as appropriate, is justified. Level of evidence: low.
Recurrent multifocal radiologic shadowing
Again, the differential diagnosis for recurrent multifocal shadowing, as for recurrent ra-
diologic shadowing in a single site, is wide (Box 5), and details of specific conditions
are given elsewhere. Fixed or relentlessly progressing pulmonary shadowing (eg,
caused by malignancy or interstitial lung disease) is not discussed here. This section
suggests a few, perhaps less obvious, points that may be valuable in elucidating this
problem, without attempting to all possibilities in detail.
As always, a detailed history is essential. Because international travel is common,
a detailed history of where the child has been is vital. A medication history is important
and should not be limited to prescription drugs.
78
Nervous system disease may affect
the lung through many mechanisms. Neurologic incoordinate swallowing may be
overlooked easily. Specific questions about choking and swallowing must be asked,
and if there is any doubt, the child should be evaluated by an experienced speech
therapist. Another cause of swallowing problems is a laryngeal cleft, which may be
overlooked unless a rigid bronchoscope is used to examine the upper airway. Laryn-
geal cleft may coexist with esophageal atresia and enters the differential diagnosis of
recurrent aspiration after surgical repair of the atresia.
79
Cough is a fundamental de-
fense mechanism, requiring both inspiratory and especially expiratory muscle
strength. Disease such as spinal muscular atrophy may present first in the respiratory
muscles and typically affects the expiratory muscles preferentially, leading to recur-
rent infection and mucus plugging.
Gastroesophageal reflux and respiratory disease have a complex relationship.
There is no doubt that respiratory disease can worsen aspiration by multiple mecha-
nisms. Also, reflux can cause respiratory disease, both by direct aspiration and by an
Bush 80
esophagobronchial reflex,
80
or reflux can be an incidental finding of no consequence.
The diagnosis of reflux also is controversial. The reference standard for a diagnosis of
acid reflux is 24-hour pH-metry. This technique has been refined by the use of an up-
per and lower esophageal electrode, to try to determine the significance of any esoph-
ageal acid,
81
but, as pointed out previously, acid reflux confined to the lower
esophagus is not necessarily benign. The significance of non-acid reflux has been
debated. Although non-acid reflux now can be detected, its measurement between
24-hour periods is more variable than that of pH-metry,
82
and currently the evidence
that this measurement adds anything of clinical importance to the standard test is, at
best, controversial.
83
If reflux is difficult to identify, is it possible to diagnose direct aspiration of gastric
contents into the respiratory tract? This finding would be unequivocal evidence of
harm. The use of lipid-laden macrophages measured on BAL has long been popular,
but this test lacks specificity.
84
Perhaps the best evidence is negative: if there are no
lipid-laden macrophages in the BAL, significant aspiration is unlikely. Measurement of
BAL pepsin may be more specific,
85
but this test is not widely available. Finally, simul-
taneous measurement of intra-esophageal and intratracheal pH has been de-
scribed,
86
but this tool is unlikely to be practical in children.
Late-presenting congenital H-type fistula may be difficult to diagnose.
87
A tube
esophagram is the usual investigation, but in the authors experience a normal test
does not exclude a fistula, and direct visualization at bronchoscopy may be needed.
For suspected esophageal dysmotility defects, sophisticated manometry may be
needed.
Pulmonary hemorrhagic syndromes may result in a diagnostic challenge if the child
swallows rather than expectorates blood. Presentation then may be with iron defi-
ciency anemia, and an extensive gastroenterologic work-up must be performed.
88
Iron-laden macrophages on the BAL are pathognomonic of pulmonary hemorrhage
but cannot distinguish between the various causes of primary and secondary bleed-
ing. Generally, if there is no evidence of a systemic disease or secondary cause of
pulmonary hemorrhage, the condition is considered to be idiopathic pulmonary hemo-
siderosis, and a confirmatory lung biopsy is not performed. If the child bleeds repeat-
edly, however, open lung biopsy to exclude a neutrophilic capillaritis should be
considered,
89
because this diagnosis may prompt treatment with cyclophosphamide.
If a connective tissue disease is suspected, the help of a pediatric rheumatologist
should be sought. If immunodeficiency is suspected (discussed later), the author per-
forms simple screening investigations but refers the patient for more sophisticated
testing. A reasonable series of screening tests for the pediatric pulmonologist who
suspects a connective tissue disease consists of an erythrocyte sedimentation rate,
anti-neutrophil cytoplasmic antibody studies, double-stranded DNA, rheumatoid fac-
tor, complement studies, anti-glomerular basement membrane antibody (for children
who have pulmonary hemorrhage and renal disease), and circulating immune
complexes.
Recommendations
1. Children who have recurrent multifocal chest radiographic changes should be
investigated, but there is no evidence base to guide the clinician as to the most
appropriate timing or sequence of investigations. Level of evidence: low
2. The differential diagnosis of recurrent multifocal chest radiographic changes is so
wide, and the number of possible tests is so great, that a targeted approach, based
on clinical suspicion driven by history and physical examination, is recommended.
Level of evidence: low.
Recurrent Respiratory Infections 81
Box 5
Differential diagnosis of recurrent fluctuating multifocal radiographic changes
Recurrent respiratory infection
Local immunodeficiency
Cystic fibrosis
Primary ciliary dyskinesia
Other subtle abnormalities of mucosal defense also likely
Systemic immunodeficiency (most require investigation by immunologic specialist)
Congenital (see Box 7)
Acquired (see Box 7)
Structural abnormality
Postinfective or idiopathic bronchiectasis
Neurologic disease causing weakness of particularly expiratory muscles
Unusual non-granulomatous infections
Hydatid disease (usually but not inevitably nonfluctuating)
Recurrent aspiration syndromes
Bulbar and pseudobulbar palsy
Central neurologic disease, peripheral nerve or muscle disease
Laryngeal cleft
Isolated, late-presenting H-type fistula
Esophageal dysmotility syndromes
After tracheoesophageal fistula repair
Achalasia
Others
Severe gastroesophageal reflux
Primary or secondary to respiratory disease
Anatomic defects: hiatus hernia
Delayed gastric emptying
Lipid inhalation
Oily medication and nose drops
Recurrent pulmonary edema
Left to right shunting (eg, ventricular septal defect, patent arterial duct)
Heart failure (eg, cardiomyopathy}
Major airway obstruction (trachea, carina, large bronchi)
Vascular rings and slings (look for a right-sided aortic arch on the chest radiograph)
Generalized bronchomalacia (Williams Campbell syndrome, others)
Multiple complete cartilage rings
Airway compression by an enlarged heart or great vessels (eg, absent pulmonary valve
syndrome)
Bush 82
DIAGNOSINGSPECIFIC CONDITIONS PRESENTING AS CHRONIC OR RECURRENTACUTE
ON CHRONIC PRODUCTIVE COUGH
Cystic Fibrosis
Increasingly, most cases of CF are diagnosed by newborn screening. Even in areas
where screening is routine, however, mild atypical cases are missed. In areas where
the prevalence is thought to be a low, the diagnosis may be forgotten. The respiratory
phenotype suggestive of CF as against other causes of recurrent infection is chronic
Latrogenic
Direct pulmonary drug toxicity
Indirect effects of medications (eg, on the heart)
Hypersecretory syndromes
Hypersecretory asthma
Plastic bronchitis syndromes
Pulmonary hemorrhagic syndromes
Secondary pulmonary hemorrhage
Pulmonary venous hypertensive syndromes
Coagulopathy
Bronchial circulatory hypertrophy of any cause
Isolated pulmonary syndromes
Idiopathic pulmonary hemosiderosis
Isolated pulmonary vasculitic syndromes
Pulmonary arteriovenous malformation
Part of a systemic disease
Goodpastures syndrome
Other autoimmune diseases and vasculitis
Autoimmune disease unrelated to pulmonary hemorrhage
Systemic lupus erythematosus
Rheumatoid syndromes
Others
Allergic lung disease
Allergic bronchopulmonary aspergillosis (usually secondary to cystic fibrosis)
Extrinsic allergic alveolitis
Granulomatous disease
Sarcoidosis
Tuberculosis
Other chronic infections
Recurrent Respiratory Infections 83
productive cough with positive cultures for typical CF-related organisms, especially
when combined with suggestive extrapulmonary features. Typical CF organisms in-
clude Staphylococcus aureus, Pseudomonas aeruginosa (especially mucoid strains),
other gram-negative rods such as Burkholderia cepacia and Stenotrophomonas mal-
tophilia, and nontuberculous Mycobacteria. H. influenzae also is found in CF but is not
particularly specific to that disease. Extrapulmonary manifestations that must be
sought actively include pancreatic insufficiency, rectal prolapse, electrolyte disorders
(heat exhaustion, hyponatremia), liver disease (which occurs only if the child has pan-
creatic insufficiency), very severe sinus disease, and particularly nasal polyps, which in
childhood are almost pathognomonic of CF.
Once CF is suspected, diagnosis usually is straightforward. The sweat test is diag-
nostic in more than 98% of cases.
90
For practical purposes, a properly performed
sweat test with a chloride concentration of more than 60 mmol in duplicate can be
considered diagnostic. The most common cause of a false-positive finding is operator
inexperience, followed by eczema. Although a number of extremely rare conditions
are reported to elevate sweat chloride,
91
this writer has never encountered them in
practice. Although most cases are diagnosed easily, a small minority presents
a very vexatious problem. The diagnosis of CF has undergone a revolution in the
last 20 years: whereas the sweat test previously was considered the reference stan-
dard for the diagnosis of CF, it has become clear that patients who have CF may
have normal sweat electrolytes. These cases often, but not invariably, have a mild
or atypical phenotype. A study in adults suggested that in equivocal cases, giving flu-
drocortisone, 3 mg/m
2
, on two successive days, and repeating the sweat test on the
third day may be helpful; healthy persons who had an equivocal sweat sodium then
present in the normal range.
92
In the absence of pediatric data, however, this test
should be used with caution.
Genetic testing may be helpful; however, at least 1300 variants of the CF transmem-
brane conductance regulator (CFTR) gene have been described, and routine labora-
tory testing detects the only most common 90% to 95%. There are marked ethnic
differences in CFTR gene frequencies, and if the genetic laboratory is to be used
most efficiently, race-specific panels should be used. Even with this approach, in
many cases only a single gene or no gene is detected, leaving the diagnosis still in
doubt. Complete gene sequencing may be helpful but is not widely available.
There are a number of potential problems with genetic testing.
93
First, it is essential
to distinguish harmless polymorphisms from disease-producing mutations. At least in
theory, a second CFTR mutation can cancel out the effects of the first. Even with nor-
mal exon amino acid sequences, CF may be produced by intron modifications. Finally,
phenotypic CF has been described with completely normal CFTR gene sequences.
94
The explanation of these findings is unknown, but a likely possibility comes from con-
sideration of the biology of CFTR. CTFR is a multifunctional protein that interacts with
many other proteins at the cell surface and also requires interaction with many other
proteins to traverse to the cell surface.
95
It may be that CF with a normal CFTR gene
sequence is caused by a mutation in one of these interacting proteins. There is prece-
dent for such an idea: the histologic pattern of pulmonary alveolar proteinosis may be
produced by mutations in either the surfactant B or C genes but also occurs without
abnormality in these genes but with mutations in a surfactant protein-processing
gene, ABCA3.
96
A further direct test of CFTR function is the measurement of electrical potential dif-
ferences in the nose,
97
the lower airway,
98
or on rectal biopsy in an Ussing chamber.
99
All these tests require sophisticated apparatus and operator skill and experience and
are not widely available. The nasal test requires cooperation from the patient and is
Bush 84
difficult in unsedated young children. Protocols usually involve making baseline mea-
surements referenced to a peripheral electrode, then perfusing the nose with amiloride
to block sodium transport, and then stimulating CFTR by perfusion with isoproterenol
and low-chloride solution.
97
Compared with unaffected persons, the CF patient has
a more negative baseline PD, a bigger positive deflection with amiloside, and no neg-
ative deflection with low-chloride/isoproterenol, this last being the most discriminatory
test. Lower airway potentials measured during bronchoscopy are a research tech-
nique that probably will find a place as an end point in clinical trials of novel therapies.
Rectal biopsy and in vitro measurement of CFTR function is available in only a very few
centers.
Ancillary testing may be helpful in the diagnosis. Human fecal elastase 1 can be mea-
sured in a small sample of stool and is sensitive and specific for pancreatic insuffi-
ciency,
100
which supports a diagnosis of CF. In males, absence of the vas deferens
(which may be diagnosed on ultrasound) or azoospermia also is supportive. The com-
plete absence of upper airway disease on HRCT scanning would be very unusual in CF.
Where does this discussion leave the diagnosis of CF in the twenty-first century?
Most cases are obvious, but how should the clinician proceed in the gray areas?
The question has been reviewed,
93
and the conclusion was almost paradoxical: de-
spite the advent of ever-more-sophisticated testing, the diagnosis of CF must be
a clinical one. The two main difficult situations are (1) the child who has positive tests
but no symptoms, and (2) the child who has clinical indications of CF (eg, bronchiec-
tasis with chronic infection with S. aureus and mucoid P. aeruginosa) but negative
tests. For the well child in whom tests are positive, the term pre-CF has been pro-
posed but has not been uniformly accepted. The chances of progression to full-blown
clinical CF depend on the nature of the tests, progression being inevitable for the
asymptomatic child who is homozygous for DF
508
but less certain for an asymptom-
atic elevation in sweat chloride with no or mild genetic mutations discovered on test-
ing. These children, who are well, certainly cannot be said to have a disease, but they
should be monitored carefully to ensure that the earliest signs of disease are detected.
For the second group, the diagnostic tests should be reviewed in detail, and other pos-
sibilities should be considered. If a different diagnosis is not found, these children
should be followed and treated exactly as if they had CF, with treatment of any com-
plication such as P. aeruginosa infection along standard lines. The alternative, of reas-
suring the family that the tests are negative, the child does not have CF, and therefore
no follow-up is needed, can have catastrophic consequences. In a proportion of chil-
dren, the sweat test or other test may be positive when repeated, and the child then is
found to have CF after all; even if the child only has a CF-like illness, the consequences
may be as bad as for CF itself.
101
The management of CF, once diagnosed, is de-
scribed in standard texts and reviews and is beyond the scope of this article.
Recommendations
1. The diagnosis of CF should be suspected, particularly if the child has a chronic in-
fection with typical CF-associated organisms and associated with extrapulmonary
features of CF, but CF also enters the differential diagnosis in many less specific
scenarios. Level of evidence: high
2. In most cases the diagnosis of CF can be made by a properly performed sweat test,
but rare and atypical cases may need more sophisticated testing. Both false-pos-
itive and false-negative CF diagnoses have been described. Level of evidence: high
3. If the diagnosis of CF is in doubt, the patient still should be followed carefully,
because in a proportion of cases either the diagnosis will become clear, or, while
Recurrent Respiratory Infections 85
still undiagnosed, the child may develop significant complications. Level of evi-
dence: moderate.
Primary Ciliary Dyskinesia
The management of PCD in the lower airway is similar to that of bronchiectasis from
any other cause, but it is important to make the diagnosis because the disease in the
upper airway is managed in a different way,
25
and there are genetic implications. PCD
usually is inherited as an autosomal recessive, occasionally X-linked, condition. Cilia
are complex structures formed from more than 250 different proteins. The complexity
of the various genes discovered has been reviewed recently.
102
The prevalence is not
known but is estimated to be 1 in 15,000. Particular features that should alert the cli-
nician to the possibility of the diagnosis are given in Table 1. Typically, the child has
a combination of upper and lower airway symptoms; isolated dry cough is unlikely
to be caused by PCD. It is important to be alert to the diagnosis; it is missed frequently,
probably because many of the symptoms of PCD (rhinitis, cough, otitis media with ef-
fusion) are common in normal children,
103
and diagnosis is delayed.
104
Diagnostic
testing is a sequential process.
102
Unless the clinical features are highly suggestive
(for example, mirror image arrangement with neonatal onset of respiratory distress
and chronic rhinorrhea), in which case direct diagnostic testing is indicated, other,
more common conditions such as CF are excluded first. In vivo mucociliary clearance
may be tested in the older, cooperative child by using the saccharine test or a variant
thereof.
105
A small saccharine tablet is placed on the inferior turbinate. The child is
asked to lean forward without coughing, sneezing, or sniffing and should be able to
taste saccharine within 60 minutes. If the child does not taste the saccharine, further
testing is required; PCDcannot be diagnosed using this test alone. There also is a dan-
ger that PCD may be excluded wrongly, if the child tastes the saccharine because he
has sniffed the microtablet into the pharynx. Nasal nitric oxide (nNO) measurements
may be a more useful screening test. A normal nNO virtually excludes PCD, and if
the history is not typical and nNO is normal, further testing may not be needed.
106
There is much less experience with nNO in infants than in older children,
107,108
and
measurements in uncooperative younger children should be interpreted with caution.
Table1
Features leading to the diagnosis of primary ciliary dyskensia
Presenting Feature Number of Cases (%) (n 555)
Significant neonatal respiratory distress 37 (67)
Abnormal situs 38 (69)
Cough most days 46 (84)
Sputum production 24 (44)
Rhinorrhea from the newborn period 42 (76)
Wheeze 16 (29)
Sinusitis 6 (11)
Serous otitis media 28 (51)
Hearing loss 14 (25)
Diagnosis made in a sibling 6 (11)
Most children had multiple symptoms, typically a combination of upper and lower airway disease.
Data from Coren ME, Meeks M, Buchdahl RM, et al. Primary ciliary dyskinesia (PCD) in children
age at diagnosis and symptom history. Acta Paediatr 2002;91:6679.
Bush 86
If nNO is low, further testing is mandated; low nNO is reported in CF
109
and also in dif-
fuse panbronchiolitis.
110
The test that usually is most specific is obtaining nasal brushings to study the func-
tion and morphology of cilia in vitro.
102
This test is an out-patient procedure. Strips of
ciliated epithelial cells are examined by light microscopy, and beat frequency and pat-
tern are reported. The findings also are recorded digitally, and the sample is examined
under an electron microscope. The most common finding is the absence of either or
both of the inner and outer dynein arms, but many others have been described.
Whether primary ciliary disorientation exists is controversial; disoriented cilia more
usually are secondary to chronic infection. Key to the diagnosis is to distinguish pri-
mary (congenital) abnormalities from secondary ciliary dysfunction caused by a viral
or other infection. Secondary postviral abnormalities may take many weeks to reverse,
and if there is any doubt, the brushing should be repeated. It may be difficult to obtain
an adequately ciliated sample if the child has chronic infective rhinitis, even after
energetic medical treatment. In such cases, culture of the ciliary biopsy is useful.
Secondary ciliary abnormalities disappear in culture, whereas primary ones persist.
Genetic testing may be useful in some cases, although this service is far from being
routinely available. Sophisticated immunofluorescence staining also may be helpful
111
but is not widely available.
Recommendations
1. Adiagnosis of PCDshouldbe suspected if there is a combination of upper and lower
airway symptoms, particularly with onset in the neonatal period. Although mirror im-
age arrangement and heterotaxy are seen in nearly 50% of patients who have
PCD,
112
their absence does not exclude the condition. Level of evidence: moderate
2. Although simple screening tests such as the saccharine test and nNO may be use-
ful to exclude the need for further testing for PCD, the diagnosis always should be
confirmed by detailed examination of ciliary function and structure in an experi-
enced center. If clinical suspicion is high, screening tests may be omitted, and
the child should proceed directly to definitive testing. Level of evidence: high
3. PCD may be confused with secondary ciliary dysfunction caused by a viral
infection; if there is any doubt, the tests must be repeated after a few months.
Alternatively, cilia can be examined from another site or cultured in vitro. Level of
evidence: high
Idiopathic Bronchiectasis
Bronchiectasis has been described as an orphan disease. It is much more common
and more severe in the developing world,
113
but one group has estimated its
prevalence to be at least 1 in 15,000 in a developed-world setting.
114
The key
symptom that should prompt consideration of the diagnosis is chronic productive
cough lasting without remission for at least 8 weeks. Other diagnostic clues are sum-
marized in Box 6. Suspicion should be particularly high if there also is an unexplained
suggestive family history or if there are extrapulmonary features of a specific condition
such as CF, PCD, or immunodeficiency.
There is no evidence base to guide the clinician in the sequence and timing of the
investigation. When the diagnosis is suspected, the author first confirms that bronchi-
ectasis is present with a HRCT scan. Although the distribution of any bronchiectasis
offers some diagnostic clues (eg, CF initially is an upper lobe disease, and PCD pre-
dominantly affects the lower lobes), in general the distribution is not a reliable basis for
Recurrent Respiratory Infections 87
diagnosis. Even if the HRCT does not demonstrate frank bronchiectasis, the clinician
should not be lulled into a false sense of security but should continue to investigate the
child (as discussed previously in the section, Chronic, Usually Productive, Cough)
and should institute appropriate treatment to prevent airway damage. The next series
of investigations is to determine the underlying cause. A detailed protocol applied in
two tertiary referral centers in the United Kingdom determined the cause in about
two thirds of patients, and the diagnosis led to a management change in more than
half the patients.
114
A specific cause may have consequences for the airway manage-
ment (eg, recombinant human deoxyribonuclease is very effective in many children
who have CF
115
but not in children who have idiopathic bronchiectasis)
116
and for ex-
trapulmonary management (chronic secretory otitis media in PCDis managed very dif-
ferently from the same condition in otherwise healthy children).
25
There may be
specific treatments, such as immunoglobulin replacement therapy; and there may
be genetic implications for the extended family, as in CF, PCD, and immunodeficiency.
The diagnostic protocol should be very different in a developed-world setting, where
tuberculosis and other infections are a major cause. (The diagnosis of tuberculosis is
discussed in detail in a later section.)
There are numerous causes of bronchiectasis, and hence there are many possible
investigations. The authors practice is to exclude CF and PCD, to screen for immuno-
deficiency (as described later), and to exclude reflux and aspiration (as described pre-
viously) in all cases. The need for more sophisticated testing is determined by the
history, examination, and the initial test results. Finally, the consequences of bronchi-
ectasis should be assessed. If the disease is severe, nocturnal hypoxemia may lead to
pulmonary hypertension; if in doubt, it is wise to perform an overnight oximetry study
and a baseline echocardiogram.
Recommendations
Children suspected of having bronchiectasis should be investigated in detail to deter-
mine the cause. In more than 50% of cases, this investigation leads to a change in
management. Level of evidence: moderate.
Box 6
Diagnostic pointers to the presence of bronchiectasis in the child in whomthe diagnosis is suspected
for the first time
Chronic unremitting productive cough lasting more than 8 weeks
Atypical asthma that does not respond to therapy
A single positive sputum culture for an unusual organism (eg, S. aureus, P. aeruginosa,
B. cepacia)
Nonresolving pneumonia
Recurrent or persistent radiographic changes
Prior infection with known predisposing organisms (eg, B. pertussis, adenovirus serotype 7, 14,
and 21)
Palpable secretions on coughing, persistent over time
Persistent crackles on auscultation
Severe esophageal disease
Localized bronchial obstruction including right middle lobe syndrome
Bush 88
The Special Problems of Congenital and Acquired Immunodeficiency
The number of immunodeficiencies is large, and the diagnosis and management of
many of these conditions requires the expertise of a specialist pediatric immunologist
(Box 7). Many immunodeficiencies, however, are seen first by a pediatric pulmonolo-
gist. The clinical picture and simple tests may indicate the presence of an underlying
immunodeficiency. The acronym SPUR was introduced in the opening section of
this article. Additional pointers to immunodeficiency include hepatosplenomegaly,
arthropathy, failure to thrive, and a family history of immunodeficiency.
The initial investigations may contain clues that often are overlooked. Neutropenia is
always sought on a full blood cell count, but lymphopenia (<2.8) often is overlooked
and may be a clue to the diagnosis of severe combined immunodeficiency. In one se-
ries, 28 (88%) of 32 infants would have been diagnosed before 6 months of age if the
possibility of immunodeficiency had investigated after the first low lymphocyte
count.
117
In this report, the first symptoms occurred at a median of 5 weeks (range,
1 day to 8 months) and included respiratory infection (91%), vomiting and diarrhea
(81%), failure to thrive (88%), candidiasis (50%), and skin lesions (28%). The median
delay between the first abnormal lymphocyte count and diagnosis was 7 weeks (range
1 day to 13 months). This report and others highlight unusually severe mucocutaneous
candidiasis as a sign of possible immunodeficiency. The chest radiograph may yield
clues. Bronchial situs should be determined, because right isomerism (bilateral right
lung morphology, Ivemarks syndrome) and hence susceptibility to overwhelming
pneumococcal sepsis is associated with asplenia in around 80% of cases.
118
The type of infection may give a clue to the nature of the immunodeficiency. In one
series,
2
pneumonia was diagnosed in 92%, 81%, and 77% of patients who had anti-
body, combined, and cellular deficiencies, respectively. Other major illnesses such as
bronchiolitis, acute gastroenteritis, otitis media, and bacteremia did not differ in prev-
alence. Skin abscess, pneumonia, and lymphadenitis (in 55%, 45%, and 27% of
cases, respectively) were the most common infections in patients who had phagocyte
defects. Age at onset of infection was around 3 years in common variable
immunodeficiency but was as early as 4 months in the hypogammaglobulinemias.
Combined deficiencies presented at around 6 months of age. Sixty percent of all pa-
tients were hospitalized initially for infection. A specific microbiologic diagnosis could
be made in a little more than half the episodes. Patients who have antibody
deficiencies have a propensity for infection with capsulated organisms, Pneumocystis
jiroveci and enterovirus; intracellular pathogens are a feature of cellular deficiency.
Chronic granulomatous disease may present with B. cepacia or catalase-positive
infection, whereas disseminated nontuberculous Mycobacterial infection suggests
a defect of the interferon gamma/interleukin-12 axis.
119
A large study of common vari-
able immunodeficiency
3
reported that respiratory presentations, especially bronchitis,
sinusitis, pneumonia and bronchiectasis, are very common. Associated diarrhea was
a feature in more than one third of cases. Although there is evidence that diagnostic
delays are lessening over time, they still are unacceptably long in many children,
underscoring the need for the respiratory pediatrician to be alert to the possibility of
immunodeficiency.
The investigation of the immunocompromised child who has single or multiple infil-
trates is likely to be much more urgent than in the otherwise well child. The differential
diagnosis includes the full spectrum of infectious disease (bacterial, viral, fungal, par-
asitic, and mycobacterial, depending on the nature of the immunodeficiency, and, in
a transplanted child, on the time from transplantation), iatrogenic complications
such as pulmonary drug toxicity, pulmonary edema caused by iatrogenic
Recurrent Respiratory Infections 89
Box 7
Important congenital and acquired immunodeficiencies that may have a respiratory presentation
Congenital immunodeficiencies
Antibody deficiency
X-linked
Common variable immunodeficiency
IgA deficiency (not invariably significant)
Hyper IgM (CD40 deficiency)
IgG subclass deficiency (may be insignificant)
Complement disorders
C3 deficiency
Mannose-binding lectin deficiency
Neutrophil disorders
Autoimmune neutropenia of infancy
Cyclical neutropenia
Shwachman-Diamond syndrome
Kostman syndrome
Chronic granulomatous disease
Other syndromes
Di George syndrome (T-cell deficiency)
Down syndrome
Heterotaxic syndromes with asplenia (right isomerism, Ivemarks syndrome)
Ataxia telangiectasia
Wiskott-Aldrich syndrome
Hyper-IgE (STAT-3 mutations)
Interferon gamma receptor mutations (suspect if disseminated mycobacterial disease)
Interleukin-12 pathway mutations (suspect if disseminated mycobacterial disease)
Acquired
Infective
HIV
Iatrogenic
Steroids or immunosuppressant medication
Postradiotherapy
Post bone marrow and solid organ transplantation
Malignancy (often also associated with iatrogenic)
Leukemia and lymphoma
Solid organ
Miscellaneous
Acquired hyposplenism (trauma, sickle cell anemia)
Malnutrition of any cause
Chronic renal or liver failure
Diabetes
Burns
90
cardiomyopathy or as part of the spectrum of acute lung injury, and recurrence of leu-
kemia or lymphoma, if that was the primary cause of the immunodeficiency. HRCT
scanning may be suggestive of specific diagnoses (for example, the halo sign
suggests invasive aspergillosis) or may guide the site of BAL. In most children, early
bronchoscopy and BAL are performed. The authors practice is not to performa trans-
bronchial biopsy in this setting because of the risk of bleeding and pneumothorax. The
diagnostic yield varies with the underlying condition and with the duration and nature
of any anti-infection prophylaxis and blind therapy. There are no satisfactory evi-
dence-based guidelines to determine the optimal timing of bronchoscopy. If no diag-
nosis is made on the initial BAL, and the child is continuing to deteriorate, it is
preferable to proceed straight to an open-lung biopsy rather than perform further
BAL.
120
Tuberculosis
This section summarizes a huge topic very briefly, and the reader is referred to a recent
evidence-based guideline.
121
Readers in the developing world may need to modify the
Box 8
Potential diagnostic tests for tuberculosis
Obtaining an organism
Gastric aspirate
Spontaneously expectorated sputum (older child)
Induced sputum
String test
Bronchoscopy
Early-morning urine (disseminated tuberculosis)
Bone marrow biopsy (disseminated tuberculosis)
Lymph node aspiration or biopsy (lymph node tuberculosis)
Imaging (nondiagnostic)
Chest radiograph
CT scan (more sensitive for nodal involvement, but false positives likely)
Molecular test on infected material
PCR for Mycobacterium tuberculosis
PCR for genes encoding drug resistance
Skin tests
Heaf test
Mantoux test
Serologic tests
Specific T-cell interferon-g synthesizing cells
Other tests
Organ biopsy
Recurrent Respiratory Infections 91
Box 9
Summary of potential investigations in the child who has recurrent infections
Suspected CF
Sweat test
CF genotype
Electrical potentials (nasal, bronchial, rectal biopsy)
Supportive tests (eg, human fecal elastase-1)
Suspected PCD
Screening: saccharine test, nasal nitric oxide
Ciliary structure and function: high-speed videomicroscopy, electron microscopy
Culture of ciliary biopsy
Genetic studies
Immunostaining of specific dynein proteins
Screening for suspected immune deficiency (referral to a pediatric immunologist mandatory
for most specific immunodeficiencies)
Full blood cell count (neutropenia, lymphopenia)
T-cell subsets
Immunoglobulins
Immunoglobulin subclasses
Vaccine antibody responses
Complement studies
HIV test
Suspected gastroesophageal reflux
pH-metry
Impedance probe
Isotope milk scan
Barium swallow (exclude anatomic causes such as hiatus hernia)
Esophageal manometry
Suspected incoordinated swallowing
Videofluoroscopy
Rigid endoscopy to exclude laryngeal cleft
Suspected aspiration
HRCT scan: dependant bronchocentric consolidation (not specific)
Lipid-laden macrophages (absence probably excludes significant aspiration)
BAL pepsin (gastric contents)
Suspected structural esophageal disease
Tube esophagram
Bronchoscopy (H-type fistula)
Barium swallow
Bush 92
recommendations substantially in the light of resources available to them. In develop-
ing countries, tuberculosis should be considered in almost all clinical settings. In the
developed world, particularly in these days of easy international travel, the possibility
of tuberculosis should not be overlooked. Most work on the symptoms that should
lead to a suspicion of pulmonary tuberculosis has come from the developing world.
These symptoms may be very nonspecific, but highly suggestive in a high-prevalence
area is the combination of persistent, unremitting cough lasting longer than 2 weeks,
documented failure to thrive for 3 months, and fatigue.
122
This combination was less
reliable in children under 3 years of age and in HIV-positive children (a minority of
tuberculosis-infected children, even in regions where HIV is common). In other stud-
ies, weight loss, fatigue, and chest pain were fairly specific for tuberculosis but
were poorly sensitive.
123
In general, a high index of suspicion is needed, especially
in young children (in whom treatment legitimately may be started on clinical suspicion
alone, because of the horrific potential consequences of miliary and, in particular,
central nervous system and meningeal tuberculosis) and in those who are HIV
infected.
The particular diagnostic algorithms used depend on the setting and available
resources (Box 8).
Suspected structural airway disease
Bronchoscopy
Endobronchial ultrasound
CT reconstruction
Suspected bronchiectasis
HRCT scanning
Exclude CF, PCD, immunodeficiency, tuberculosis (see other sections)
Consider excluding esophageal disease, incoordinated swallowing, reflux, and aspiration
Echocardiogram, overnight saturation studies
Suspected tuberculosis
See Box 8
Suspected cardiovascular disease
Echocardiogram (enlarged cardiac chambers caused by left-to-right shunt, vascular ring)
Barium swallow (vascular ring)
CT or MRI with vascular reconstruction (vascular ring)
Suggested vasculitis or connective tissue disease (referral to pediatric rheumatologist probably
is advisable)
Erythrocyte sedimentation rate, C-reactive protein
Double-stranded DNA
Rheumatoid factor
Antineutrophil cytoplasmic antibody studies
Circulating immune complexes
Anti-glomerular basement membrane antibodies
Recurrent Respiratory Infections 93
Combinations of tests may be better than the individual tests alone; for example, the
diagnostic yield with both gastric aspirates and induced sputum tests is better than
that of either test alone. In the past, gastric aspirates were reported to be more
sensitive than bronchoscopy, but with the use of PCR technology the differences
are not great,
124
although with bronchoscopy direct visualization of endobronchial
tuberculosis may allowimmediate confirmation of the diagnosis. The chest radiograph
is used widely in children and has a sensitivity of 39% and a specificity of 74%,
125
but
interobserver agreement is not good, at least for the detection of lymphadenopa-
thy.
126
HRCT scan reveals more lymphadenopathy than a chest radiograph,
127
although whether these nodes are always tuberculous is conjectural, and in most parts
of the world, HRCT may not be readily available.
The use of serologic tests to diagnose tuberculosis is a current hot topic, and the
place of these tests has yet to be determined, particularly in young children and those
who are HIV infected. Two serologic tests currently are available.
121
One measures the
release of interferon-g from whole blood after stimulation with early secreted antigenic
target (ESAT)-6 and culture filtrate protein (CFP)-10, which are relatively specific for
Mycobacterium tuberculosis. In the other test, individual ESAT-6 and CFP-10 T cells
are delineated with enzyme-linked immunosorbent spot methodology. In the past,
robust guidelines have been produced on the basis of skin tests and chest radiogra-
phy; whether and how these newer tests can improve the diagnosis of tuberculosis
has yet to be worked out fully.
In summary, it can be seen that the diagnosis of tuberculosis can be challenging
even with newer investigations. The timeless principles remain: a high index of suspi-
cion is essential, and when in doubt, particularly in high-risk situations such as very
young children, blind treatment is safer than a prolonged period of diagnostic
havering.
SUMMARY
The child who has recurrent infections poses one of the most difficult diagnostic
challenges in pediatrics. The outcome may be anything from reassurance that the
child is normal to the diagnosis of a life-threatening condition. A huge range of tests
is available (Box 9).
The clinician faces a twofold challenge in determining:
1. Is this child normal? (This question may be the most difficult in all clinical practice.)
2. If this child seems to have a serious disease, howcan the diagnosis be confirmed or
excluded with the minimum number of the least-invasive tests?
It is hoped that, in the absence of good-quality evidence for most clinical scenarios,
the experience-based approach described in this article may prove a useful guide to
the clinician.
REFERENCES
1. Marchant JM, Masters IB, Taylor SM, et al. Evaluation and outcome of young chil-
dren with chronic cough. Chest 2006;129:113241.
2. Chang SH, Yang YH, Chiang BL. Infectious pathogens in pediatric patients with
primary immunodeficiencies. J Microbiol Immunol Infect 2006;39:50315.
3. Oksenhendler E, G
erard L, Fieschi C, et al. DEFI Study Group. Infections in 252
patients with common variable immunodeficiency. Clin Infect Dis 2008;46:
154754.
Bush 94
4. Primary Immodeficiency Resource Center home page. Available at: http://www.
info4pi.org. Accessed November 15, 2008.
5. Chonmaitree T, Revai K, Grady JJ, et al. Viral upper respiratory tract infection
and otitis media complication in young children. Clin Infect Dis 2008;46:81523.
6. Gru ber C, Riesberg A, Mansmann U, et al. The effect of hydrotherapy on the
incidence of common cold episodes in children: a randomised clinical trial.
Eur J Pediatr 2003;162:16876.
7. Cane RS, Ranganathan SC, McKenzie SA. What do parents of wheezy children
understand by wheeze? Arch Dis Child 2000;82:32732.
8. Elphick HE, Ritson S, Rodgers H, et al. When a wheeze is not a wheeze: acous-
tic analysis of breath sounds in infants. Eur Respir J 2000;16:5937.
9. Cane RS, McKenzie SA. Parents interpretations of childrens respiratory symp-
toms on video. Arch Dis Child 2001;84:314.
10. Saglani S, McKenzie SA, Bush A, et al. A video questionnaire identifies upper
airway abnormalities in preschool children with reported wheeze. Arch Dis Child
2005;90:9614.
11. Ball TM, Holberg CJ, Aldous MB, et al. Influence of attendance at day care on
the common cold from birth through 13 years of age. Arch Pediatr Adolesc
Med 2002;156:1216.
12. Lee GM, Friedman JF, Ross-Degnan D, et al. Misconceptions about colds and
predictors of health service utilization. Pediatrics 2003;111:2316.
13. Bousquet J, Van Cauwenberge P, Khaltaev N. Allergic rhinitis and its impact on
asthma. J Allergy Clin Immunol 2001;108:S147334.
14. Scadding GK, Durham SR, Mirakian R, et al. British Society for Allergy and
Clinical Immunology. BSACI guidelines for the management of allergic and
non-allergic rhinitis. Clin Exp Allergy 2008;38:1942.
15. Akikusa JD, Schneider R, Harvey EA, et al. Clinical features and outcome of
pediatric Wegeners granulomatosis. Arthritis Rheum 2007;57:83744.
16. Paradise JL, Bluestone CD, Bachman RZ, et al. Efficacy of tonsillectomy for
recurrent throat infection in severely affected children. Results of parallel
randomized and nonrandomized clinical trials. N Engl J Med 1984;310:67483.
17. Tarasiuk A, Simon T, Tal A, et al. Adenotonsillectomy in children with obstructive
sleep apnea syndrome reduces health care utilization. Pediatrics 2004;113:
3516.
18. Paradise JL, Bluestone CD, Colborn DK, et al. Tonsillectomy and adenotonsillec-
tomy for recurrent throat infection in moderately affected children. Pediatrics
2002;110:715.
19. van den Akker EH, Schilder AG, Kemps YJ, et al. Current indications for
(adeno)tonsillectomy in children: a survey in The Netherlands. Int J Pediatr Oto-
rhinolaryngol 2003;67:6037.
20. Jecker P, Orloff LA, Wohlfeil M, et al. Gastroesophageal reflux disease (GERD),
extraesophageal reflux (EER) and recurrent chronic rhinosinusitis. Eur Arch
Otorhinolaryngol 2006;263:6647.
21. Ford CN. Evaluation and management of laryngopharyngeal reflux. JAMA 2005;
294:153440.
22. Bercin S, Kutluhan A, Yurttas V, et al. Evaluation of laryngopharyngeal reflux in
patients with suspected laryngopharyngeal reflux, chronic otitis media and
laryngeal disorders. Eur Arch Otorhinolaryngol 2008;265:153943.
23. Scadding GK, Durham SR, Mirakian R, et al. British Society for Allergy and
Clinical Immunology. BSACI guidelines for the management of rhinosinusitis
and nasal polyposis. Clin Exp Allergy 2008;38:26075.
Recurrent Respiratory Infections 95
24. Barbero GJ. Gastro-esophageal reflux and upper airway disease. Otolaryngol
Clin North Am 1996;29:2738.
25. Hadfield PJ, Rowe-Jones JM, Bush A, et al. Treatment of otitis media with effu-
sion in children with primary ciliary dyskinesia. Clin Otolaryngol Allied Sci 1997;
22:3026.
26. Bjornson CL, Johnson DW. Croup. Lancet 2008;371:32939.
27. Cherry JD. Clinical practice. Croup. N Engl J Med 2008;358:38491.
28. Kiff KM, Mok Q, Dunne J, et al. Steroids for intubated croup masking airway hae-
mangioma. Arch Dis Child 1996;74:667.
29. Reiterer F, Eber E, Zach MS, et al. Management of severe congenital tracheo-
bronchomalacia by continuous positive airway pressure and tidal breathing
flow-volume loop analysis. Pediatr Pulmonol 1994;17:4013.
30. Ramsey CD, Gold DR, Litonjua AA, et al. Respiratory illnesses in early life and
asthma and atopy in childhood. J Allergy Clin Immunol 2007;119:1506.
31. NafstadP, Brunekreef B, Skrondal A, et al. Early respiratory infections, asthma, and
allergy: 10-year follow-up of the Oslo Birth Cohort. Pediatrics 2005;116:e25562.
32. Van Bever HP, Wieringa MH, Weyler JJ, et al. Croup and recurrent croup: their
association with asthma and allergy. An epidemiological study on 58-year-old
children. Eur J Pediatr 1999;158:2537.
33. Castro-Rodr
guez JA, Holberg CJ, Morgan WJ, et al. Relation of two different
subtypes of croup before age three to wheezing, atopy, and pulmonary function
during childhood: a prospective study. Pediatrics 2001;107:5128.
34. van Essen-Zandvliet EE, Hughes MD, Waalkens HJ, et al. Effects of 22 months of
treatment with inhaled corticosteroids and/or beta-2-agonists on lung function,
airway responsiveness, and symptoms in asthma. The Dutch Chronic Non-
specific Lung Disease Study Group. Am Rev Respir Dis 1992;146:54754.
35. Waalkens HJ, van Essen-Zandvliet EE, Hughes MD, et al. Cessation of long-term
treatment with inhaled corticosteroid (budesonide) in children with asthma
results in deterioration. The Dutch CNSLD Study Group. Am Rev Respir Dis
1993;148:12527.
36. Murray CS, Woodcock A, Langley SJ, et al. Secondary prevention of asthma by
the use of inhaled fluticasone dipropionate in wheezy Infants (IWWIN): double-
blind, randomised controlled study. Lancet 2006;368:75462.
37. Guilbert TW, Morgan WJ, Zeiger RS, et al. Long-term inhaled corticosteroids in
preschool children at high risk for asthma. N Engl J Med 2006;354:198597.
38. Bisgaard H, Hermansen MN, Loland L, et al. Intermittent inhaled corticosteroids
in infants with episodic wheezing. N Engl J Med 2006;354:19982005.
39. Hopkins A, Lahiri T, Salerno R, et al. Changing epidemiology of life-threatening
upper airway infections: the reemergence of bacterial tracheitis. Pediatrics
2006;118:141821.
40. Pao CS, Healy MJ, McKenzie SA. Airway resistance by the interrupter technique:
which algorithm for measuring pressure? Pediatr Pulmonol 2004;37:316.
41. Gustafsson PM, Aurora P, Lindblad A. Evaluation of ventilation maldistribution as
an early indicator of lung disease in children with cystic fibrosis. Eur Respir
J 2003;22:9729.
42. Aurora P, Bush A, Gustafsson P, et al. Multiple breath washout as a marker of
lung disease in preschool children with cystic fibrosis. Am J Respir Crit Care
Med 2005;171:24956.
43. LumS, Gustafsson P, Ljungberg H, et al. Early detection of cystic fibrosis lung dis-
ease: multiple-breath washout vs. raised volume tests. Thorax 2007;62:3417.
44. GoldmanJ, MuersM. Vocal corddysfunctionandwheezing. Thorax1991;46:4014.
Bush 96
45. Shields MD, Bush A, Everard ML, et al. British Thoracic Society guidelines.
Recommendations for the assessment and management of cough in children.
Thorax 2008;63(Suppl 3):iii115.
46. Chang AB, Gaffney JT, Eastburn MM, et al. Cough quality in children: a compar-
ison of subjective vs. bronchoscopic findings. Respir Res 2005;6:3.
47. Kelly YJ, Brabin BJ, Milligan PJ, et al. Clinical significance of cough and wheeze
in the diagnosis of asthma. Arch Dis Child 1996;75:48993.
48. Ferreira de A, Filho LV, Rodrigues JC, et al. Comparison of atopic and nonatopic
children with chronic cough: bronchoalveolar lavage cell profile. Pediatr Pulmo-
nol 2007;42:85763.
49. Donnelly D, Critchlow A, Everard ML. Outcomes in children treated for persistent
bacterial bronchitis. Thorax 2007;62:804.
50. Eastham KM, Fall AJ, Mitchell L, et al. The need to redefine non-cystic fibrosis
bronchiectasis in childhood. Thorax 2004;59:3247.
51. Chavasse RJ, Bastian-Lee Y, Richter H, et al. Persistent wheezing in infants with
an atopic tendency responds to inhaled fluticasone. Arch Dis Child 2001;85:
1438.
52. Chavasse RJ, Bastian-Lee Y, Richter H, et al. Inhaled salbutamol for wheezy
infants: a randomised controlled trial. Arch Dis Child 2000;82:3705.
53. Narang I, Ersu R, Wilson NM, et al. Nitric oxide in chronic airway inflammation in
children: diagnostic use and pathophysiological significance. Thorax 2002;57:
5869.
54. Pijnenburg MW, Bakker EM, Lever S, et al. High fractional concentration of nitric
oxide in exhaled air despite steroid treatment in asthmatic children. Clin Exp
Allergy 2005;35:9205.
55. Levy ML, Godfrey S, Irving CS, et al. Wheeze detection in infants and pre-school
children: recordings versus assessment of physician and parent. J Asthma
2004;41:84553.
56. Bisgaard H, Hermansen MN, Buchvald F, et al. Childhood asthma after bacterial
colonization of the airway in neonates. N Engl J Med 2007;357:148795.
57. Lehtinen P, Jartti T, Virkki R, et al. Bacterial coinfections in children with viral
wheezing. Eur J Clin Microbiol Infect Dis 2006;25:4639.
58. von Mutius E. Of attraction and rejectionasthma and the microbial world.
N Engl J Med 2007;357:15457.
59. Devereux G, Barker RN, Seaton A. Antenatal determinants of neonatal immune
response to allergens. Clin Exp Allergy 2002;32:4350.
60. Noakes PS, Holt PG, Prescott SL. Maternal smoking in pregnancy alters neona-
tal cytokine responses. Allergy 2003;58:10538.
61. Noakes PS, Hale J, Thomas R, et al. Maternal smoking is associated with
impaired neonatal toll-like-receptor-mediated immune responses. Eur Respir
J 2006;28:7219.
62. Miller RL, Ho SM. Environmental epigenetics and asthma: current concepts and
call for studies. Am J Respir Crit Care Med 2008;177:56773.
63. Saglani S, Nicholson A, Scallan M, et al. Investigation of young children with
severe recurrent wheeze. Any clinical benefit? Eur Respir J 2006;27:2935.
64. Munyard P, Bush A. How much coughing is normal? Arch Dis Child 1996;74:
5314.
65. Archer LNJ, Simpson H. Night cough counts and diary card scores in asthma.
Arch Dis Child 1985;60:4734.
66. Falconer A, Oldman C, Helms P. Poor agreement between reported and
recorded nocturnal cough in asthma. Pediatr Pulmonol 1993;15:20911.
Recurrent Respiratory Infections 97
67. Munyard P, Busst C, Logan-Sinclair R, et al. A new device for ambulatory cough
recording. Pediatr Pulmonol 1994;18:17886.
68. Hamutcu R, Francis J, Karakoc F, et al. Objective monitoring of cough in children
with cystic fibrosis. Pediatr Pulmonol 2002;34:3315.
69. Gibson NA, Hollman AS, Paton JY. Value of radiological follow up of childhood
pneumonia. Br Med J 1993;307:1117.
70. Sur
en P, Try K, Eriksson J, et al. Radiographic follow-up of community-acquired
pneumonia in children. Acta Paediatr 2008;97:4650.
71. Geppert EF. Chronic and recurrent pneumonia. Semin Respir Infect 1992;7:
2828.
72. Stein RT, Marostica PJC. Community-acquired bacterial pneumonia. In: Cher-
nick V, Boat TF, Wilmott RW, et al, editors. Kendigs disorders of the respiratory
tract in children. 7th edition. Philadelphia: Saunders; 2006.
73. Priftis KN, Mermiri D, Papadopoulou A, et al. The role of timely intervention in
middle lobe syndrome in children. Chest 2005;128:250410.
74. Sekerel BE, Nakipoglu F. Middle lobe syndrome in children with asthma: review
of 56 cases. J Asthma 2004;41:4117.
75. Kwon KY, Myers JL, Swensen SJ, et al. Middle lobe syndrome: a clinicopatholog-
ical study of 21 patients. Hum Pathol 1995;26:3027.
76. Priftis KN, Anthracopoulos MB, Mermiri D, et al. Bronchial hyperresponsiveness,
atopy, and bronchoalveolar lavage eosinophils in persistent middle lobe syn-
drome. Pediatr Pulmonol 2006;41:80511.
77. De Boeck K, Willems T, Van Gysel D, et al. Outcome after right middle lobe syn-
drome. Chest 1995;108:1502.
78. Gattuso JM, Kamm MA. Adverse effects of drugs used in the management of
constipation and diarrhoea. Drug Saf 1994;10:4765.
79. Ratan SK, Ratan J. Laryngotracheo-esophageal cleft in a neonate with esopha-
geal atresia and tracheo-esophageal fistula: report of a case. Surg Today 2001;
31:5961.
80. Wilson NM, Chudry N, Silverman M. Role of the oesophagus in asthma induced
by the ingestion of ice and acid. Thorax 1987;42:50610.
81. Mitchell DJ, McClure BG, Tubman TR. Simultaneous monitoring of gastric and
oesophageal pH reveals limitations of conventional oesophageal pH monitoring
in milk fed infants. Arch Dis Child 2001;84:2736.
82. Dalby K, Nielsen RG, Markoew S, et al. Reproducibility of 24-hour combined
multiple intraluminal impedance (MII) and pH measurements in infants and chil-
dren. Evaluation of a diagnostic procedure for gastroesophageal reflux disease.
Dig Dis Sci 2007;52:215965.
83. Vandenplas Y, Salvatore S, Devreker T, et al. Gastro-oesophageal reflux disease:
oesophageal impedance versus pH monitoring. Acta Paediatr 2007;96:95662.
84. Rosen R, Fritz J, Nurko A, et al. Lipid-laden macrophage index is not an indicator
of gastroesophageal reflux-related respiratory disease in children. Pediatrics
2008;121:e87984.
85. Farrell S, McMaster C, Gibson D, et al. Pepsin in bronchoalveolar lavage fluid:
a specific and sensitive method of diagnosing gastro-oesophageal reflux-
related pulmonary aspiration. J Pediatr Surg 2006;41:28993.
86. Jack CI, Calverley PM, Donnelly RJ, et al. Simultaneous tracheal and oesopha-
geal pH measurements in asthmatic patients with gastro-oesophageal reflux.
Thorax 1995;50:2014.
87. Ng J, Bartram J, Antao B, et al. H-type tracheoesophageal fistula masquerading
as achalasia cardia in a 13-year-old child. J Paediatr Child Health 2006;42:2156.
Bush 98
88. Yao TC, Hung IJ, Jaing TH, et al. Pitfalls in the diagnosis of idiopathic pulmonary
haemosiderosis. Arch Dis Child 2002;86:4368.
89. Jennings CA, King TE Jr, Tuder R, et al. Diffuse alveolar hemorrhage with under-
lying isolated, pauciimmune pulmonary capillaritis. Am J Respir Crit Care Med
1997;155:11019.
90. Cystic Fibrosis Foundation. Patient registry 1996 annual data report. Bethesda
(MD): National Institutes of Health; 1997.
91. Wallis C. Diagnosis of cystic fibrosis. In: Hodson M, Geddes DM, Bush A, edi-
tors. Cystic fibrosis. 3rd edition. London: Publ Edward Arnold; 2007. p. 99108.
92. Hodson ME, Beldon I, Power R, et al. Sweat tests to diagnose cystic fibrosis in
adults. Br Med J (Clin Res Ed) 1983;286:13813.
93. Bush A, Wallis C. Time to think again: cystic fibrosis is not an all or none dis-
ease. Pediatr Pulmonol 2000;30:13944.
94. Groman JD, Meyer ME, Wilmott RW, et al. Variant cystic fibrosis phenotypes in
the absence of CFTR mutations. N Engl J Med 2002;347:4017.
95. Wang X, Venable J, LaPointe P, et al. Hsp90 cochaperone Aha1 downregulation
rescues misfolding of CFTR in cystic fibrosis. Cell 2006;127:80315.
96. Doan ML, Guillerman RP, Dishop MK, et al. Clinical, radiological and patholog-
ical features of ABCA3 mutations in children. Thorax 2008;63:36673.
97. Middleton PG, Geddes DM, Alton EW. Protocols for in vivo measurement of the
ion transport defects in cystic fibrosis nasal epithelium. Eur Respir J 1994;7:
20506.
98. Davies JC, Davies M, McShane D, et al. Potential difference measurements in
the lower airway of children with and without cystic fibrosis. Am J Respir Crit
Care Med 2005;171:10159.
99. Veeze HJ, Sinaasappel M, Bijman J, et al. Ion transport abnormalities in rectal
suction biopsies from children with cystic fibrosis. Gastroenterology 1991;101:
398403.
100. Cohen JR, Schall JI, Ittenbach RF, et al. Fecal elastase: pancreatic status
verification and influence on nutritional status in children with cystic fibrosis.
J Pediatr Gastroenterol Nutr 2005;40:43844.
101. Lebecque P, Leal T, De Boeck C, et al. Mutations of the cystic fibrosis gene and
intermediate sweat chloride levels in children. Am J Respir Crit Care Med 2002;
165:75761.
102. Bush A, Chodhari R, Collins N, et al. Primary ciliary dyskinesia. Arch Dis Child
2007;92:113640.
103. Bush A, OCallaghan C. Primary ciliary dyskinesia. Arch Dis Child 2002;87:
3635.
104. Coren ME, Meeks M, Buchdahl RM, et al. Primary ciliary dyskinesia (PCD) in
childrenage at diagnosis and symptom history. Acta Paediatr 2002;91:6679.
105. Deitmer T. A modification of the saccharine test for nasal mucociliary clearance.
Rhinology 1986;24:23740.
106. Karadag B, James AJ, Gultekin E, et al. Nasal and lower airway level of nitric
oxide in children with primary ciliary dyskinesia. Eur Respir J 1999;13:14026.
107. Franklin PJ, Turner SW, Mutch RC, et al. Measuring exhaled nitric oxide in infants
during tidal breathing: methodological issues. Pediatr Pulmonol 2004;37:2430.
108. Gabriele C, van der Wiel EC, Nieuwhof EM, et al. Methodological aspects of
exhaled nitric oxide measurements in infants. Pediatr Allergy Immunol 2007;
18:3641.
109. Balfour-Lynn IM, Laverty A, Dinwiddie R. Reduced upper airway nitric oxide in
cystic fibrosis. Arch Dis Child 1996;75:31922.
Recurrent Respiratory Infections 99
110. Nakano H, Ide H, Imada M, et al. Reduced nasal nitric oxide in diffuse panbron-
chiolitis. Am J Respir Crit Care Med 2000;162:221820.
111. Fliegauf M, Olbrich H, Horvath J, et al. Mislocalization of DNAH5 and DNAH9 in
respiratory cells from patients with primary ciliary dyskinesia. Am J Respir Crit
Care Med 2005;171:13439.
112. Kennedy MP, Omran H, Leigh MW, et al. Congenital heart disease and other
heterotaxic defects in a large cohort of patients with primary ciliary dyskinesia.
Circulation 2007;115:281421.
113. Twiss J, Stewart AW, Byrnes CA. Longitudinal pulmonary function of childhood
bronchiectasis and comparison with cystic fibrosis. Thorax 2006;61:4148.
114. Li AM, Sonnappa S, Lex C, et al. Non-CF bronchiectasis: does knowing the
aetiology lead to changes in management? Eur Respir J 2005;26:814.
115. Fuchs HJ, Borowitz DS, Christiansen DH, et al. Effect of aerosolized
recombinant human DNase on exacerbations of respiratory symptoms and on
pulmonary function in patients with cystic fibrosis. The Pulmozyme Study Group.
N Engl J Med 1994;331:63742.
116. Wills PJ, Wodehouse T, Corkery K, et al. Short-term recombinant human DNase
in bronchiectasis. Effect on clinical state and in vitro sputum transportability. Am
J Respir Crit Care Med 1996;154:4137.
117. Hague RA, Rassam S, Morgan G, et al. Early diagnosis of severe combined
immunodeficiency syndrome. Arch Dis Child 1994;70:2603.
118. Cesko I, Hajd u J, T
oth T, et al. Ivemark syndrome with asplenia in siblings.
J Pediatr 1997;130:8224.
119. Glosli H, Stray-Pedersen A, Brun AC, et al. Infections due to various atypical
mycobacteria in a Norwegian multiplex family with dominant interferon-gamma
receptor deficiency. Clin Infect Dis 2008;46:e237.
120. Stefanutti D, Morais L, Fournet JC, et al. Value of open lung biopsy in
immunocompromised children. J Pediatr 2000;137:16571.
121. National Institute for Health and Clinical Excellence. Tuberculosis guidelines.
Availableat: http://www.nice.org.uk/guidance/index.jsp?action5byID&o510979.
Accessed November 15, 2008.
122. Marais BJ, Gie RP, Hesseling AC, et al. A refined symptom-based approach to
diagnose pulmonary tuberculosis in children. Pediatrics 2006;118:e13509.
123. Marais BJ, Obihara CC, Gie RP, et al. The prevalence of symptoms associated
with pulmonary tuberculosis in randomly selected children from a high burden
community. Arch Dis Child 2005;90:116670.
124. Chierakul N, Anantasetagoon T, Chaiprasert A, et al. Diagnostic value of gastric
aspirate smear and polymerase chain reaction in smear-negative pulmonary
tuberculosis. Respirology 2003;8:4926.
125. De Villiers RV, Andronikou S, Van de Westhuizen S. Specificity and sensitivity of
chest radiographs in the diagnosis of paediatric pulmonary tuberculosis and the
value of additional high-kilovolt radiographs. Australas Radiol 2004;48:14853.
126. Du Toit G, Swingler G, Iloni K. Observer variation in detecting lymphadenopathy
on chest radiography. Int J Tuberc Lung Dis 2002;6:8147.
127. Swingler GH, du Toit G, Andronikou S, et al. Diagnostic accuracy of chest
radiography in detecting mediastinal lymphadenopathy in suspected
pulmonary tuberculosis. Arch Dis Child 2005;90:11536.
Bush 100
Upper Respi ratory Tract
I nfecti ons ( I ncl udi ng
Oti ti s Medi a)
Peter S. Morris, MBBS, PhD, FRACP
a,b,c,
*
Upper respiratory tract infections (including otitis media) are the most common
illnesses affecting children.
1
On average, children experience around six to eight
upper respiratory tract infections (URTIs) each year.
2
Although these infections usually
are mild and self limiting, they occasionally lead to complications that can be life
threatening. Most URTIs can be placed within three main categories of infection:
rhinosinusitis, pharyngitis, and otitis media. Within each category of illness there is
a range of related conditions that may have similar or overlapping clinical presenta-
tions.
3
Some judgment is required in determining which part of the respiratory mucosa
is most affected. In this article, the term rhinosinusitis is used to describe illnesses
with predominantly nasal symptoms (including the common cold, nasopharyngitis,
and sinusitis). The term pharyngitis is used to describe illnesses when sore throat
is most prominent (including tonsillitis). The term otitis media is used to describe
illnesses with predominantly middle ear symptoms (including acute otitis media
[AOM], otitis media with effusion [OME], and chronic suppurative otitis media
[CSOM]). Children who have cough as the predominant symptom are considered to
have bronchitis (a lower respiratory tract infection). To make matters more compli-
cated, all areas of the respiratory mucosa may be affected, simultaneously or at
different times, during one illness.
The cause of these respiratory mucosal infections most commonly is viral but can
be bacterial (Table 1),
4
and many infections involve both viruses and bacteria.
5
In de-
veloped countries, both viral and bacterial infections are likely to be self limited.
Persistent disease is most likely to indicate a bacterial infection.
a
Child Health Division, Menzies School of Health Research, P.O. Box 41096, Casuarina, NT 0811,
Darwin, Australia
b
Institute of Advanced Studies, Charles Darwin University, Darwin, Australia
c
Northern Territory Clinical School, Flinders University, Darwin, Australia
* Menzies School of Health Research, Child Health Division, P.O. Box 41096, Darwin, Casuarina,
NT 0811, Australia.
E-mail address: peterm@menzies.edu.au
KEYWORDS
Evidence based
Rhinosinusitis
Pharyngitis
Otitis media
Management
Pediatr Clin N Am 56 (2009) 101117
doi:10.1016/j.pcl.2008.10.009 pediatric.theclinics.com
0031-3955/08/$ see front matter 2009 Published by Elsevier Inc.
The frequency of infection and association with fever and constitutional symptoms
creates significant distress for the child and the family. By understanding the evidence
available from high-quality studies, the clinician can advise the families on appropriate
action.
6
The goal of this article is to support clinicians in answering the following
questions:
1. What happened to children with these conditions when no additional treatment was
provided?
2. Which interventions have been assessed in well-designed studies?
3. Which interventions have been shown to improve outcomes?
4. How large is the overall benefit?
THE APPROACH TOEVIDENCE USED IN THIS ARTICLE
URTIs are extremely common in children, and there is a long list of potential interven-
tions. Because URTIs are common illnesses, there is no reason why high-quality
randomized, controlled trials (RTCs) should not be conducted.
7
In addition, all families
experience these conditions and may have strong personal preferences about treat-
ment. The challenge for the clinician is to make an accurate diagnosis and then to
match the effective treatment options with the preferences of the family.
Table1
Spectrumof disease, accepted terminology, and etiology of the common upper respiratory tract
infections in children
Condition Related Diagnoses Etiology
Rhinosinusitis Common cold, nasopharyngitis,
infective rhinitis, acute
rhinosinusitis, acute sinusitis,
chronic sinusitis
Viral: rhinovirus, coronavirus,
enterovirus, parainfluenza,
influenza, respiratory syncytial
virus, adenovirus,
metapneumovirus
Bacterial: Streptococcus
pneumoniae, Haemophilus
influenzae, Moraxella
catarrhalis, Staphylococcus
aureus, Streptococcus pyogenes
Pharyngitis Pharyngitis, tonsillitis, recurrent
tonsillitis
Viral: adenovirus, respiratory
syncytial virus, Epstein-Barr
virus, cytomegalovirus,
parainfluenza, influenza
Bacterial: Streptococcus pyogenes,
Group C and G Streptococci,
Mycoplasma pneumoniae
Otitis media Acute otitis media without
perforation, acute otitis media
with perforation, otitis media
with effusion, chronic
suppurative otitis media.
Viral: respiratory syncytial virus,
influenza, adenovirus,
rhinovirus, coronavirus,
enterovirus, parainfluenza,
metapneumovirus
Bacterial: Streptococcus
pneumoniae, Haemophilus
influenzae, Moraxella
catarrhalis, Streptococcus
pyogenes
Morris 102
This article initially considers the effects of an intervention compared with no inter-
vention. Because each condition covers a spectrumof disease, the acute presentation
of the initial URTI is discussed first and then, when appropriate, interventions for per-
sistent disease or complications of the initial complaint are addressed. Because of the
focus on trial evidence, not all the information relevant to an individual decision may be
discussed. Furthermore, because the clinical course of participants enrolled in RCTs
may be different from the clinical course observed in ones own practice, the overall
effects of an intervention may need to be adjusted. Despite these limitations, clinicians
using this article should be confident that they understand which interventions have
been rigorously assessed and the overall findings of these assessments.
The GRADE Working Group has described the steps required to review evidence.
8,9
Ideally, explicit criteria should be used. Although this process has many advantages in
terms of transparency, it does not guarantee that recommendations will be consistent
across different sets of evidence-based guidelines (although this consistency is the
long-term aim).
10
The GRADE Working Group proposes that a recommendation
should indicate the decision that the majority of well-informed individuals would
make.
8
It is difficult to be dogmatic about interventions for self-limited conditions
with a low risk of complications. Therefore, the author has tried to provide a summary
of evidence to assist discussions with families (Tables 24). The authors approach
(informed by the best available evidence) is described in Box 1.
IMPORTANT HEALTH OUTCOMES AND TREATMENT EFFECTS
The self-limiting nature of these conditions is of the utmost importance in determining
which treatments are indicated. The outcomes the author considers important are (1)
persistent disease (short term, %14 days; medium term, >2 weeks to 6 months; and
long term >6 months), (2) time to cure, and (3) complications arising from progressive
disease. The author considered interventions to have very large effects if they were as-
sociated with a reduction in the outcome of interest of more than 80%; large effects
were associated with a reduction in outcome of interest of at least 50%.
11
Reductions
in outcome of interest between 20% and 50% were considered modest, and reduc-
tions of less than 20% were considered slight (or small). Because only a proportion
of children who have URTIs experience bad outcomes, even large relative effects
may not translate to clinically significant absolute benefits.
SEARCHSTRATEGY
The authors search targeted evidence-based guidelines, evidence-based summa-
ries, systematic reviews, and RCTs of interventions for rhinosinusitis, pharyngitis,
and otitis media (Box 2). Even this simple strategy identified more than 6500 sources
using PubMed alone. Inclusion as an evidence-based guideline, summary, or system-
atic review required an explicit search strategy and criteria for study inclusion. Inclu-
sion as a clinical trial required randomization. The author used three primary sources
to identify relevant information: Clinical Evidence;
11
the Cochrane library
12
and Med-
line (last accessed via PubMed on June 16, 2008). The evidence-based summaries
in Clinical Evidence have links to major guidelines and use the GRADE Working Group
approach to assess quality of evidence and strength of recommendations.
11
RESULTS OF SEARCH
The search identified more than 50 evidence-based guidelines, evidence summaries,
and systematic reviews (and many more additional RCTs) published since 2000. This
Upper Respiratory Tract Infections 103
article does not include interventions that have been assessed in nonrandomized
studies, interventions that have been assessed in studies with fewer than 200 partic-
ipants (sparse data),
11
or studies of interventions that are available only
experimentally.
RHINOSINUSITIS
Rhinosinusitis is an URTI that predominantly affects the nasal part of the respiratory
mucosa.
1315
Common cold infections are caused mainly by viruses (typically rhinovi-
rus, but also coronavirus, respiratory syncytial virus, metapneumovirus, and others).
2
For many colds, no infecting organism can be identified. Common colds usually have
a short duration. Symptoms peak within 1 to 3 days and generally clear by 7 to 10
days, although an associated cough (bronchitis) often persists.
2
Most people who
have acute rhinosinusitis are assessed and treated in a primary-care setting.
Table 2
Treatment effects of interventions for rhinosinusitis in children that have been assessed
in randomized, controlled trials
Intervention Evidence Effect
Prevention
Vitamin C 30 studies (11,350
participants)
No significant reduction in proportion of
participants experiencing the common
cold (48%)
Echinacea Three studies (498
participants)
No significant reduction in proportion of
participants experiencing the common
cold (45%)
Treatment of initial rhinosinusitis
Antihistamines Five studies (3492
participants)
No significant reduction in proportion of
participants with persistent symptoms at 1
to 2 days (55%)
Vitamin C Seven studies (3294
participants)
No significant reduction in median duration
of symptoms
Antibiotics Six studies (1147
participants)
No significant reduction in persistent
symptoms at 7 days (35% versus 31%);
significant reduction in persistence of
purulent rhinitis from 42% to 24%
Decongestants Six studies (643
participants)
Subjective assessment of congestion reduced
by 6% after one dose. Effect persisted with
repeated doses over 3 days
Zinc lozenges 13 studies (516
participants)
No consistent effects on symptoms
Echinacea Two studies (200
participants)
Proportion experiencing full cold reduced
by 12% to 23% but no effect in other
studies of different outcomes
Treatment of persistent rhinosinusitis/clinical sinusitis
Intranasal
corticosteroids
Three studies (1792
participants)
Persistent disease reduced from 27% to 19%.
Antibiotics 14 studies (1309
participants)
Persistent disease at around 2 weeks reduced
from 60% to 46% in adults and from 46%
to 35% in children
Morris 104
A preceding viral URTI often is the trigger for acute sinusitis; about 0.5% to 5% of
common colds become complicated by the development of acute sinusitis.
16
Acute
sinusitis is defined pathologically by transient inflammation of the mucosal lining of
the paranasal sinuses lasting less than 30 days.
17,18
Clinically, acute sinusitis is char-
acterized by nasal congestion, nasal discharge, and facial pain.
19
The diagnosis of
acute sinusitis in infants and children usually is made in children who have purulent
nasal drainage persisting beyond 10 days.
17
In straightforward cases, no investiga-
tions are required.
17
In more complicated (or frequent) presentations, possible under-
lying factors include nasal airway obstruction, immunodeficiencies, ciliary
dysfunction, cystic fibrosis, and allergic rhinitis. The usual pathogens in acute bacterial
sinusitis are Streptococcus pneumoniae and Haemophilus influenzae, with occasional
infection with Moraxella catarrhalis and Staphylococcus aureus. Rarely, bacterial
sinusitis in children leads to rare, life-threatening complications, such as meningitis,
cavernous venous thrombosis, and orbital cellulitis.
4
Options for Interventions
Most children who have rhinosinusitis improve spontaneously within 14 days, and
complications from this illness are uncommon. There is evidence about the preventive
effects of vitamin C and Echinacea on the onset of the illness.
20,21
Neither of these
interventions has been proven to be effective. There is evidence about the treatment
effects of antihistamines, vitamin C, antibiotics, decongestants, zinc lozenges, and
Echinacea (see Table 2).
2028
Of these interventions, only decongestants have been
proven to be effective, but their beneficial effect is small.
26
Decongestants have not
Table 3
Treatment effects of interventions for pharyngitis inchildrenthat have beenassessedinrandomized,
controlled trials
Intervention Evidence Effect
Treatment of initial pharyngitis
Antibiotics 15 studies (3621
participants)
Pain at 3 days reduced from 66% to 48%
13 studies (2974
participants)
Pain at 7 days reduced from 18% to 12%
15 studies (3621
participants)
Median time to cure reduced from 4 days
to 3 days
Eight studies (2443
participants)
Peritonsillar abscess within 2 months
reduced from 2.3% to 0.1%
16 studies (10,101
participants)
Rheumatic fever within 2 months reduced
from 1.8% to 0.7%
11 studies (3760
participants)
Otitis media within 14 days reduced from
2% to 0.5%
Analgesics 17 studies (1742
participants)
Pain scores reduced by 25% to 80%
within 4 hours; benefits persisted with
regular treatment over 2 o 5 days
Corticosteroids Five studies (421
participants)
Pain reduced by 12 to 24 hours but effects
inconsistent
Treatment of recurrent pharyngitis
(Adeno)Tonsillectomy Six studies (1618
participants)
Sore throat episodes over 3 years reduced
from 2.4 to 1.2 episodes per year
Upper Respiratory Tract Infections 105
Table 4
Treatment effects of interventions for otitis mediainchildrenthat havebeenassessedinrandomized,
controlled trials
Intervention Evidence Effect
Prevention
Conjugate
pneumococcal
vaccine
Three studies
(39,749
participants)
Acute otitis media episodes reduced by
6% (eg, from 1.0 to 0.94 episodes per
year); insertion of tympanostomy tubes
reduced from 3.8% to 2.9%
Influenza vaccine 11 studies
(11,349
participants)
Inconsistent results; modest protection
against otitis media during influenza
season in some studies
Treatment of initial acute otitis media
Antihistamines and
decongestants
12 studies (2300
participants)
No significant difference in persistent
acute otitis media at 2 weeks
Antibiotics Eight studies (2287
participants)
Persistent pain on day 2 through 7
reduced from 22% to 16%
Six studies (1643
participants)
Persistent reduced from 55% to 30% in
children younger than 2 years old who
had with bilateral acute otitis media
and from 53% to 19% in children who
had acute otitis media with perforation
Myringotomy Three studies (812
participants)
Early treatment failure increased from
5% to 20%
Analgesics One study (219
participants)
Persistent pain reduced from 25% to 9%
on day 2
Treatment of recurrent acute otitis media
Antibiotics 16 studies (1483
participants)
Episodes of acute otitis media reduced
from 3.0 to 1.5 episodes per year
Adenoidectomy Six studies (1,060
participants)
No significant reduction in rates of acute
otitis media
Tympanostomy tubes Five studies (424
participants)
Episodes of acute otitis media reduced
from 2.0 to 1.0 episodes per year
Treatment of persistent otitis media with effusion
Antibiotics Nine studies (1534
participants)
Persistent otitis media with effusion at
around4weeks reducedfrom81%to68%
Tympanostomy tubes 11 studies (w1300
participants)
Modest improvement in hearing (9 dB at
6 months and 6 dB at 12 months); no
improvement in language or cognitive
assessment
Antihistamines and
decongestants
Seven studies (1177
participants)
No difference in persistent otitis media
with effusion at 4 weeks (75%)
Autoinflation Six studies (602
participants)
Inconsistent results; modest improvement in
tympanometry at 4 weeks in some studies
Antibiotics plus
steroids
Five studies (418
participants)
Persistent otitis media with effusion at 2
weeks reduced from 75% to 52%
Treatment of chronic suppurative otitis media
Topical antibiotics Seven studies (1074
participants)
Persistent chronic suppurative otitis
media at 2 to 16 weeks reduced from
around 75% to 20% to 50%
Ear cleaning Two studies (658
participants)
Inconsistent results; noreductioninpersistent
chronic suppurativeotitis mediaat 12to16
weeks (78%) in a large African study
Morris 106
Box1
Suggested approach for assessing and managing a child who has an upper respiratory infection
1. Take a history of the presenting complaint to elicit the primary symptom: nasal discharge
(rhinosinusitis), sore throat (pharyngitis) ear pain, ear discharge, or hearing loss (otitis
media). Ask about the frequency and severity of previous URTIs. Clarify the duration of
illness and the presence of any associated features, including cough (bronchitis), fever,
respiratory distress, cyanosis, poor feeding, or lethargy. Determine the concerns,
expectations, and preferences of the child and the caregivers. (Grade: very low; level of
evidence: cohort studies and other evidence)
2. Examine the child to confirm whether investigation and management should be directed at
rhinosinusitis, pharyngitis, or AOM. Assess temperature, pulse and respiratory rate, presence
and color of nasal discharge, nasal obstruction, facial tenderness, tonsillar enlargement,
tonsillar exudate, cervical lymphadenopathy, presence of cough, presence of middle ear
effusion (using pneumatic otoscopy or tympanometry), position and integrity of tympanic
membrane, and proptosis. Ensure normal hydration, perfusion, conscious state, and no
meningism, periorbital swelling, limitation of eye movements, upper airway obstruction,
respiratory distress, or mastoid tenderness. (Grade: very low; level of evidence: cohort
studies and other evidence)
3. Investigations
Rhinosinusitis: none required unless patient is febrile and less than 3 months of age or
danger signs (respiratory distress, cyanosis, poor feeding, or lethargy) are present.
(Grade: low; level of evidence: cohort studies)
Pharyngitis: none required unless patient is febrile and less than 3 months of age or
danger signs (respiratory distress, cyanosis, poor feeding, or lethargy) are present.
(Grade: low; level of evidence: cohort studies)
AOM: none required unless patient is febrile and less than 3 months of age or danger
signs (respiratory distress, cyanosis, poor feeding, or lethargy) are present.
(Grade: low; level of evidence: cohort studies)
4. Management
Rhinosinusitis: Provide symptomatic pain relief if indicated during watchful waiting with
advice to parents on likely course and possible complications. Antibiotics can be
considered if there is persistent nasal discharge for more than 10 days or purulent nasal
discharge. Decongestants may be used in an older child who has significant nasal
obstruction. (Grade: moderate; level of evidence: RCTs)
Pharyngitis: Provide symptomatic pain relief if indicated during watchful waiting with
advice to parents on likely course and possible complications. Antibiotics can be used if
pain is severe and does not respond to analgesics, if there is tonsillar exudate plus cervical
lymphadenopathy and no nasal discharge or cough, or if the patient is at high risk of
complications (especially rheumatic fever or peritonsillar abscess). (Grade: moderate;
level of evidence: RCTs)
AOM: Provide symptomatic pain relief if indicated during watchful waiting with advice to
parents on likely course and possible complications. Antibiotics can be used if the patient
has AOM with perforation or is younger than 2 years old and has bilateral AOM, if there
has been no improvement after 48 hours of watchful waiting, or if the patient is at high
risk of suppurative complications (especially perforation of the tympanic membrane).
(Grade: high; level of evidence: RCTs)
Upper Respiratory Tract Infections 107
been tested in young children. Antibiotics seem to be effective in individuals who have
purulent rhinosinusitis, but the beneficial effect is modest.
24
Given the available evidence from RCTs, most well-informed individuals choose
a course of watchful waiting. Symptomatic relief using analgesic agents has not
been assessed in RCTs but would be a reasonable in children who have pain or dis-
comfort. Antibiotics are an option for children who have purulent nasal discharge but
provide only a modest benefit. Decongestants are an option for older children who
have nasal obstruction. It probably is worth persisting with decongestants only
when there is symptomatic relief with the first dose.
A small proportion of children go on to develop persistent rhinosinusitis or classic
sinusitis. There is evidence about the treatment effects of intranasal corticosteroids
(from adult studies) and antibiotics.
17,18,2933
Both of these interventions seem to be
beneficial, but the beneficial effects are modest. If antibiotics are to be used, there
no consistent evidence that a longer course of treatment (R7 days) is more effective
than a shorter course.
32
There is no evidence to support the belief that any one of the
commonly used antibiotics is more effective than the others (although the cephalospo-
rin class of antibiotics does seem to be inferior to amoxicillin-clavulanate).
32
Given the
available evidence from RCTs, most well-informed individuals choose either watchful
waiting or a trial of antibiotics. Intranasal corticosteroids are a reasonable option in
older children, particularly those who have any features of atopy.
PHARYNGITIS
Pharyngitis is an acute URTI that affects the respiratory mucosa of the throat, resulting
in a predominant symptom of pain that may be associated with headache, fever, and
general malaise.
3,34,35
In the United States, acute pharyngitis accounts for about 1%
of primary care consultations and ranks in the top 20 diagnoses.
34
Infections leading
to pharyngitis can be viral or bacterial (Table 5). It is difficult to distinguish bacterial
infections from viral infections clinically. Studies have found that tonsillar or pharyn-
geal exudate, tender cervical lymphadenopathy, and recent exposure to streptococ-
cal throat infection are most useful in predicting bacterial infection.
36
A useful clinical
prediction rule found that streptococcal infection was present in 50% of children if
three of the following features were positive: fever higher than 38
C; tonsillar swelling
or exudate; tender cervical lymphadenopathy; and absence of cough. Even without
treatment, sore throat resolves in 40% of cases by 3 days and in 85% of cases by
1 week.
3
A small proportion of children experience progression of the illness. Suppu-
rative complications include peritonsillar abscess (quinsy), AOM, and acute sinusitis.
Nonsuppurative complications include acute rheumatic fever and acute
glomerulonephritis.
Options for Interventions
Most children who have pharyngitis improve spontaneously within 14 days, and
complications from this illness are uncommon. There is evidence about the
Box 2
A simple PubMed search strategy to identify evidence-based guidelines, evidence-based summaries,
systematic reviews, and randmoized controlled trials on common upper respiratory tract infections
rhinitis[MeSH Terms] OR nasopharyngitis[MeSH Terms] OR common cold
[MeSH Terms] OR sinusitis[MeSH Terms] OR pharyngitis[MeSH Terms] OR tonsillitis[MeSH
Terms] OR otitis[MeSH Terms] AND (practice guideline[pt] OR systematic[sb] OR clinical
evidence[jour] OR clinical trial[pt]).
Morris 108
treatment effects of antibiotics, analgesics, and corticosteroids on the onset of illness
(see Table 3).
3,35,3741
The beneficial effect of analgesics is large and persists over
several days of treatment.
3,40
Antibiotics also have been proven to be effective,
3,37,38
with large to very large beneficial effects for preventing complications (peritonsillar ab-
scess, rheumatic fever, and otitis media). These complications generally affect less
than 2% of children, however. Antibiotics have a modest, short-term beneficial effect
in improving the sore throat itself. If oral penicillin is used for treatment, there is evi-
dence that a full 10-day course is more effective than shorter courses.
39
There is
some evidence that systemic corticosteroids reduce pain within 12 to 24 hours.
3,41
Given the available evidence from RCTs, most well-informed individuals choose
symptomatic relief with analgesics and either watchful waiting or antibiotics. Antibi-
otics would be most appropriate in children at increased risk of complications, those
who have features more consistent with a bacterial infection (fever higher than 38
C,
tonsillar exudate, enlarged tender cervical nodes, and absence of nasal discharge and
cough), and those who have severe pain that does not respond to analgesics.
Corticosteroids are an option for children who have severe pain not responding to
analgesics or who have very large tonsils that may lead to obstruction.
A small proportion of children go on to develop recurrent tonsillitis. There is
evidence on the treatment effects of tonsillectomy.
35,42,43
Tonsillectomy has a large
beneficial effect, but the rates of tonsillitis also reduce spontaneously without treat-
ment, so absolute benefits are modest. In addition, the operation itself is associated
with postoperative pain and some risk of complications. High-quality trials of
prophylactic antibiotic treatment have not been done, but this treatment would be
a reasonable option for families who want treatment but decide against surgery. Sur-
gery is likely to be most beneficial in children who have very frequent severe infections.
If surgery is the chosen treatment option, cold steel tonsillectomy is associated with
less postoperative pain and bleeding than operation by diathermy.
35,44
Table 5
Typical clinical features of the common upper respiratory infections in children that have been
assessed in randomized, controlled trials
Condition Typical Clinical Features
Rhinosinusitis Febrile illness associated with nasal discharge
Persistent rhinosinusitis Persistent nasal discharge plus abnormalities on sinus
radiographs
Pharyngitis Febrile illness associated with sore throat plus localizing
signs on examination
Recurrent tonsillitis Recurrent febrile illnesses (more than three per year)
associated with sore throat plus localizing signs
on examination
Acute otitis media Clinical diagnosis of acute otitis media with red
tympanic membrane and ear pain
Recurrent acute otitis media Recurrent clinical diagnosis of acute otitis media (three
or more episodes in 6 months) with red tympanic
membrane and ear pain
Otitis media with effusion Asymptomatic persistent middle ear effusion confirmed
by tympanometry
Chronic suppurative otitis media Discharge through a perforated tympanic membrane
for 2 to 6 weeks
Upper Respiratory Tract Infections 109
OTITIS MEDIA
Otitis media is an acute URTI that affects the respiratory mucosa of the middle ear cleft.
It isacommonillnessinyoungchildrenandoccursmuchlessfrequentlyinchildrenmore
than6yearsold.
45,46
Indevelopedcountries, otitismediais themost commonindication
for antibiotic prescribing and surgery in young children. In the United States, annual
costs associated with otitis media were estimated to be $3 to $5 billion in the 1990s.
45
Otitis media is best regarded as a spectrum of disease. The most important condi-
tions are OME, AOM without perforation (AOMwoP), acute otitis media with perfora-
tion (AOMwiP), and CSOM. Unfortunately, there currently is a lack of consistency in
definitions of different forms of otitis media (especially AOM).
47
Generally, AOM is de-
fined as the presence of a middle ear effusion plus the presence of the symptoms
(especially pain) or signs (especially bulging of the tympanic membrane or fresh
discharge). The diagnostic criteria used in studies of AOM vary. Some use symptom-
atic criteria, some use otoscopic criteria, and some require that both symptomatic and
otoscopic criteria be met. OME usually is defined as the presence of a middle ear
effusion without symptoms or signs of an acute infection. CSOM usually is defined
as discharge through a perforated tympanic membrane for longer than 2 to 6 weeks.
Children who have immunodeficiency or craniofacial abnormalities (eg, cleft palate,
Downs syndrome) are at increased risk of otitis media. Other risk factors that have
been identified in epidemiologic studies include recent respiratory infection, family
history, siblings, child care attendance, lack of breast feeding, passive smoke expo-
sure, and use of a pacifier.
48
Most children experience at least one episode of AOM.
45
The peak incidence of in-
fection occurs between 6 and 12 months. Although the pathogenesis of AOM is mul-
tifactorial, both viruses and bacteria are implicated.
45
Bacteria infection with the
common respiratory pathogens (S. pneumoniae, H. influenzae, and M. catarrhalis) of-
ten is preceded by a viral infection. Viruses (especially respiratory syntactical virus and
influenza) can cause AOM without coinfection with bacteria.
45
The pain associated
with AOMresolves within 24 hours in around 60%of cases and within 3 days in around
80%.
46
AOM is less likely to resolve spontaneously in children younger than 2 years.
49
Complications of AOM include CSOM, mastoiditis, labyrinthitis, facial palsy, meningi-
tis, intracranial abscess, and lateral sinus thrombosis.
50
Mastoiditis was the most
common life-threatening complication in the pre-antibiotic era. It occurred in 18%
of children admitted to hospital with AOM in one study.
51
Mastoiditis and all other
complications now are rare in developed countries.
CSOM is the most severe form of otitis media.
52
Although there is a lack of well-de-
signed longitudinal studies, CSOM is the type of otitis media most likely to persist
without treatment. In developing countries, CSOM occurs as a complication of
AOM with perforation and can be a major health issue. The range of bacterial patho-
gens associated with CSOM is considerably broader than those seen in AOM.
Pseudomonas, Staphylococcus, Proteus, and Klebsiella species are the most com-
monly isolated pathogens, and mixed infections are common.
52
Multidrug antibiotic
resistance is seen often in Pseudomonas infections. The associated hearing loss usu-
ally is greater than seen in OME, and CSOM is the most important cause of moderate
conductive hearing loss (>40 dB) in many developing countries.
53
In developed countries, CSOM now is very uncommon. A recent risk factor study in
Holland found that most cases of CSOM now occur as a complication of tympanos-
tomy tube insertion.
54
Children who have immunodeficiency and some indigenous
populations also are at greatly increased risk. In rural and remote communities in
northern Australia, more than 20% of young children are affected.
55
Morris 110
OME is the most common form of otitis media. The point prevalence in screening
studies is around 20% in young children.
45
OME can occur spontaneously, as a com-
ponent of rhinosinusitis, or following an episode of AOM. The same respiratory bacte-
rial pathogens associated with AOM have been implicated in the pathogenesis of
OME. Most children who have OME improve spontaneously within 3 months, and
complications from this illness are uncommon.
45
The average hearing loss associated
with OME is around 25 dB.
45
Despite large numbers of studies, a causal relationship
between OME and speech and language delay has not been proven.
50,56
Children who have otitis media usually present with features related to (1) pain and
fever (AOM); (2) hearing loss (OME); or (3) ear discharge (AOMwiP or CSOM). In some
children, otitis media is detected as part of a routine examination. Making an accurate
diagnosis is not easy. Generally a good viewof the whole tympanic membrane and the
use of either pneumatic otoscopy or tympanometry are required to confirm the pres-
ence of a middle ear effusion.
47,57
Studies of diagnostic accuracy in AOM have found
ear pain to be the most useful symptom, but it is not very reliable on its own. Bulging,
opacity, and immobility of the tympanic membrane are highly predictive of AOM.
Normal color (pearly gray) of the tympanic membrane makes AOM unlikely.
58
Options for Interventions
Most children who have AOM improve spontaneously within 14 days, and complica-
tions from this illness are uncommon. There is evidence concerning the preventive ef-
fects of conjugate pneumococcal vaccine and influenza vaccine on the onset of illness
(see Table 4).
46,5961
Both these vaccines have been shown to be effective, but the
beneficial effects in terms of overall rates of infection are slight. The beneficial effects
of the conjugate pneumococcal vaccine in reducing the rate of insertion of tympanos-
tomy tubes are modest.
62
Most children do not fall into this risk group. There also is
evidence about the treatment effects of antihistamines and decongestants, antibi-
otics, myringotomy, and analgesics (see Table 4).
46,50,51,63
Regular analgesics (para-
cetamol or ibuprofen) provide a benefit (assessment on day 2), and the beneficial
effects are large.
46
Antibiotics also are effective,
49,51
but in most children the short-
term beneficial effects are slight. The beneficial effects are modest in children younger
than 2 years old who have bilateral AOM and are large in those who have AOMwiP.
Studies of initial treatment with antibiotics have not documented a long-term effect.
If antibiotics are to be used, there is evidence that a longer course of treatment
(R 7 days) is more effective, but the beneficial effects are modest (persistent AOM
reduced from 22% to 15%).
64
There is no evidence that any one of the commonly
used antibiotics is more effective than the others. The use of antihistamines and
decongestants has not been shown to be beneficial, and myringotomy seems to be
harmful compared with no treatment or antibiotics (see Table 4).
46,50,63
Given the available evidence from RCTs on AOM, most well-informed individuals
choose symptomatic relief with analgesics and either watchful waiting or antibiotics.
Antibiotics are most appropriate in children younger than 2 years who have bilateral
AOM, children who have AOMwiP, children at high risk of complications, and children
who already have had 48 hours of watchful waiting. If the child is not in a high-risk,
group, but the family prefers antibiotic treatment, the clinician should discuss wait
and see prescribing. Provision of a script for an antibiotic along with advice to use
it only if the pain persists for 48 hours can reduce antibiotic use by two thirds (with
no negative effect on family satisfaction).
6567
A small proportion of children who have AOM experience recurrent AOM (three ep-
isodes within 6 months or four episodes within 12 months).
45
There is evidence about
the treatment effects of prophylactic antibiotics, adenoidectomy, and tympanostomy
Upper Respiratory Tract Infections 111
tube insertion.
46,50,6870
Antibiotics have been proven to be effective, but the beneficial
effects are modest. The rates of AOM also reduce spontaneously without treatment,
so the absolute benefits are less impressive than anticipated. Insertion of tympanos-
tomy tubes also seems to reduce rates of AOM, and the level of effect is similar to that
of antibiotics. Either of these options could be considered in children who have very
frequent severe infections, especially infections occurring before the peak of respira-
tory illness in winter. Children who have tympanostomy tubes may develop a discharg-
ing ear, however, so tympanostomy tubes are not a good option in children who are at
increased risk of suppurative infections (including those who have immunodeficiency
or persistent bacterial rhinosinusitis). In these children, prophylactic antibiotics or
prompt antibiotic treatment of infections probably is a more appropriate choice.
Adenoidectomy does not seem to be an effective treatment.
50,69,70
A small proportion of children who have AOMwiP go on to develop CSOM. In devel-
oped countries, CSOM occurs most commonly as a complication of tympanostomy
tube placement. There is evidence about the treatment effects of topical antibiotics,
topical antiseptics, systemic antibiotics, and ear cleaning.
52,53,7173
The interpretation
of a large number of small studies is challenging, but topical antibiotics have been
proven to be effective, although the beneficial effects vary from large to modest. Most
studies have not documented a long-term effect. Topical antibiotics also seem to be
more effective than antiseptics andsystemic antibiotics.
53
The role of topical antibiotics
plus systematic antibiotics is unclear.
74
Cleaningthe middle ear discharge has not been
provento be effective in RCTs but generally is regardedas necessary before insertion of
topical antibiotics (at least in childrenwhohaveprofuse discharge). Althoughnot seenin
RCTs, there also is a very small risk of ototoxicity associated with most topical antibi-
otics (except topical quinolones) and topical antiseptics.
50
For children who do not re-
spond to prolonged courses of topical antibiotics, two small studies (85 participants)
have documented high cure rates and large beneficial effects associated with 2 to 3
weeks of intravenous antipseudomonal antibiotics (such as ceftazidime).
75,76
Given the available evidence from RCTs on CSOM, most well-informed individuals
choose topical antibiotic treatment. Even though this treatment is effective, prolonged
or repeated courses of treatment often are required. If prolonged or repeated courses
of topical antibiotic are needed, topical quinolones provide a slight benefit in terms of
risk of ototoxicity.
OME affects all children but usually is asymptomatic.
45
A small proportion of chil-
dren have persistent OME with associated hearing loss. There is evidence that screen-
ing to identify young children who have OME or hearing loss associated with OME is
not effective in developed countries.
77
There also is evidence on the treatment effects
of antibiotics, insertion of tympanostomy tubes, autoinflation devices, antihistamines
and decongestants, and antibiotics plus steroids (see Table 4).
49,51,7885
Early inser-
tion of tympanostomy tubes (compared with watchful waiting with the option of later
insertion) improves hearing at 6 and 12 months, but the beneficial effect is
modest.
78,79,81
This improvement in hearing has not been associated with improve-
ment in language development or cognitive assessment scores.
81
Tympanostomy
tubes usually last 6 to 12 months, and there is no evidence of any ongoing benefit after
they have been extruded. Antibiotics also have been shown to be an effective treat-
ment, but the beneficial effects are slight and do not seem to persist long
term.
50,78,79
Combining antibiotics with steroids seems to provide short-term benefits,
but again the beneficial effect is modest.
78,85
There is some evidence that autoinflation
devices are effective.
78,83
but the benefits are modest and have been documented to
be only short term. Antihistamines and decongestants provide no benefit (see
Table 4).
78,79,84
Morris 112
Given the available evidence from RCTs on OME, most well-informed individuals
initially choose a course of watchful waiting. For children who have persistent OME
in both ears associated with hearing loss despite watching waiting for 6 to 12 months,
a trial of antibiotics is reasonable. Insertion of tympanostomy tubes is most appropri-
ate in children when the primary concern is conductive hearing loss and communica-
tion difficulties. Children who have the most severe conductive hearing loss are most
likely to benefit. Children who experience frequent suppurative infections (including
those who have immunodeficiency or persistent bacterial rhinosinusitis) are at great-
est risk of developing CSOM as a complication of tympanostomy tubes. Families
should be informed that a small proportion of children suffer recurrent persistent
OME when the tympanostomy tubes are extruded and may need a second operation.
In these children, tympanostomy tubes plus adenoidectomy is a reasonable
option.
79,80
SUMMARY
URTIs are the most common illnesses affecting children. Most illnesses are mild and
resolve completely without specific treatment. Multiple interventions have been
assessed in the treatment of rhinosinusitis, pharyngitis, and otitis media. None of
the interventions had substantial absolute benefits for the populations studied. There-
fore, for most children, symptomatic relief and watchful waiting (including education of
the parents about important danger signs) is the most appropriate treatment option.
Antibiotics have a role in children who have persistent bacterial infection and those
at risk of complications.
REFERENCES
1. Monto AS. Epidemiology of viral respiratory infections. Am J Med 2002;
112(Suppl 6A):4S12S.
2. Heikkinen T, Jarvinen A. The common cold. Lancet 2003;361(9351):519.
3. Kenealy T. Sore throat. BMJ Clinical Evidence 2008. Available at: http://clinical
evidence.bmj.com. Accessed June 27, 2008.
4. Behrman RE. Textbook of pediatrics. 15th edition. Philadelphia: W.B. Saunders
Company; 1996.
5. Revai K, Dobbs LA, Nair S, et al. Incidence of acute otitis media and sinusitis
complicating upper respiratory tract infection: the effect of age. Pediatrics
2007;119(6):e140812.
6. Irwig L, Irwig J, Sweet M, et al. Smart health choices: making sense of health
advice. Sydney (Australia): Hammersmith Press; 2007.
7. Altman DG, Bland JM. Statistics notes. Treatment allocation in controlled trials:
why randomise? BMJ 1999;318(7192):1209.
8. Atkins D, Best D, Briss PA, et al. Grading quality of evidence and strength of
recommendations. BMJ 2004;328(7454):14907.
9. Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an emerging consensus on rating
quality of evidence and strength of recommendations. BMJ 2008;336(7650):9246.
10. Atkins D, Briss PA, Eccles M, et al. Systems for grading the quality of evidence
and the strength of recommendations II: pilot study of a new system. BMC Health
Serv Res 2005;5(1):2536.
11. Clinical evidence. Available at: http://clinicalevidence.bmj.com. Accessed June
27, 2008.
12. The Cochrane Library. Available at: http://www3.interscience.wiley.com/cgi-bin/
mrwhome/106568753/HOME. Accessed June 16, 2008.
Upper Respiratory Tract Infections 113
13. Gwaltney- JMJ, Phillips CD, Miller RD, et al. Computed tomographic study of the
common cold [see comments]. N Engl J Med 1994;330(1):2530.
14. Puhakka T, Makela MJ, Alanen A, et al. Sinusitis in the common cold. J Allergy
Clin Immunol 1998;102(3):4038.
15. Pratter MR. Cough and the common cold: ACCP evidence-based clinical prac-
tice guidelines. Chest 2006;129(1 Suppl):72S4S.
16. Ramadan HH. Pediatric sinusitis: update. J Otolaryngol 2005;34(Suppl 1):S147.
17. American Academy of Pediatrics, Subcommittee on Management of Sinusitis and
Committee on Quality Improvement. Clinical practice guideline: management of
sinusitis. Pediatrics 2001;108(3):798808.
18. Ioannidis JP, Lau J. Technical report: evidence for the diagnosis and treatment of
acute uncomplicated sinusitis in children: a systematic overview. Pediatrics 2001;
108(3):E5764.
19. Williams JW Jr, Simel DL. Does this patient have sinusitis? Diagnosing acute
sinusitis by history and physical examination. JAMA 1993;270(10):12426.
20. Douglas RM, Hemila H, Chalker E, et al. Vitamin C for preventing and treating the
common cold. Cochrane Database Syst Rev 2007;(3):CD000980.
21. Linde K, Barrett B, Wolkart K, et al. Echinacea for preventing and treating the
common cold. Cochrane Database Syst Rev 2006;(1):CD000530.
22. Arroll B. Common cold. BMJ Clinical Evidence 2008. Available at: http://clinical
evidence.bmj.com. Accessed June 27, 2008.
23. Sutter AI, Lemiengre M, Campbell H, et al. Antihistamines for the common cold.
Cochrane Database Syst Rev 2003;(3):CD001267.
24. Arroll B, Kenealy T. Antibiotics for the common cold and acute purulent rhinitis.
Cochrane Database Syst Rev 2005;(3):CD000247.
25. Arroll B, Kenealy T. Are antibiotics effective for acute purulent rhinitis? Systematic
review and meta-analysis of placebo controlled randomised trials. BMJ 2006;
333(7562):27982.
26. Taverner D, Latte J. Nasal decongestants for the common cold. Cochrane
Database Syst Rev 2007;(1):CD001953.
27. Kollar C, Schneider H, Waksman J, et al. Meta-analysis of the efficacy of a single
dose of phenylephrine 10 mg compared with placebo in adults with acute nasal
congestion due to the common cold. Clin Ther 2007;29(6):105770.
28. Marshall I. Zinc for the common cold. Cochrane Database Syst Rev
1999;(2):CD001364.
29. Ah-See K. Sinusitis (acute). BMJ Clinical Evidence 2008. Available at: http://clini
calevidence.bmj.com. Accessed June 27, 2008.
30. Zalmanovici A, Yaphe J. Steroids for acute sinusitis. Cochrane Database Syst
Rev 2007;(2):CD005149.
31. Young J, De Sutter A, Merenstein D, et al. Antibiotics for adults with clinically
diagnosed acute rhinosinusitis: a meta-analysis of individual patient data. Lancet
2008;371(9616):90814.
32. Ip S, Fu L, Balk E, et al. Update on acute bacterial rhinosinusitis. Evid Rep Tech-
nol Assess 2005;124:13.
33. Morris P, Leach A. Antibiotics for persistent nasal discharge (rhinosinusitis) in
children. Cochrane Database Syst Rev 2002;(4):CD001094.
34. Vincent MT, Celestin N, Hussain AN. Pharyngitis. Am Fam Physician 2004;69(6):
146570.
35. Georgalas CC, Tolley NS, Narula A. Recurrent throat infections (tonsillitis). BMJ
Clinical Evidence 2008. Available at: http://clinicalevidence.bmj.com. Accessed
June 27, 2008.
Morris 114
36. Ebell MH, Smith MA, Barry HC, et al. The rational clinical examination. Does this
patient have strep throat? JAMA 2000;284(22):29128.
37. Del Mar CB, Glasziou PP, Spinks AB. Antibiotics for sore throat. Cochrane Data-
base Syst Rev 2006;(4):CD000023.
38. Robertson KA, Volmink JA, Mayosi BM. Antibiotics for the primary prevention of
acute rheumatic fever: a meta-analysis. BMC Cardiovasc Disord 2005;5(1):119.
39. Casey JR, Pichichero ME. Metaanalysis of short course antibiotic treatment for
group a streptococcal tonsillopharyngitis. Pediatr Infect Dis J 2005;24(10):
90917.
40. Thomas M, Del Mar C, Glasziou P. How effective are treatments other than anti-
biotics for acute sore throat? Br J Gen Pract 2000;50(459):81720.
41. Olympia RP, Khine H, Avner JR. Effectiveness of oral dexamethasone in the treat-
ment of moderate to severe pharyngitis in children. Arch Pediatr Adolesc Med
2005;159(3):27882.
42. Burton MJ, Towler B, Glasziou P. Tonsillectomy versus non-surgical treatment for
chronic/recurrent acute tonsillitis. Cochrane Database Syst Rev 2000;(2):
CD001802.
43. van Staaij BK, van den Akker EH, van der Heijden GJ, et al. Adenotonsillectomy for
upper respiratory infections: evidence based? Arch Dis Child 2005;90(1):1925.
44. Leinbach RF, Markwell SJ, Colliver JA, et al. Hot versus cold tonsillectomy: a sys-
tematic review of the literature. Otolaryngol Head Neck Surg 2003;129(4):3604.
45. Rovers MM, Schilder AG, Zielhuis GA, et al. Otitis media. Lancet 2004;363(9407):
46573.
46. Bradley-Stevenson C, ONeill P, Roberts T. Otitis media in children (acute). BMJ
Clinical Evidence 2008. Available at: http://clinicalevidence.bmj.com. Accessed
June 27, 2008.
47. American Academy of Pediatrics Subcommittee on Management of Acute Otitis
Media. Diagnosis and management of acute otitis media. Pediatrics 2004;113(5):
145165.
48. Uhari M, Mantysaari K, Niemela M. A meta-analytic review of the risk factors for
acute otitis media [see comments]. Clin Infect Dis 1996;22(6):107983.
49. Rovers MM, Glasziou P, Appelman CL, et al. Antibiotics for acute otitis media:
a meta-analysis with individual patient data. Lancet 2006;368(9545):142935.
50. Rosenfeld RM, Bluestone CD. Evidence-based otitis media. Hamilton (UK): B.C.
Decker Inc; 2003.
51. Glasziou PP, Del Mar CB, Sanders SL, et al. Antibiotics for acute otitis media in
children. Cochrane Database Syst Rev 2004;(1):CD000219.
52. Verhoeff M, van der Veen EL, Rovers MM, et al. Chronic suppurative otitis media:
a review. Int J Pediatr Otorhinolaryngol 2006;70(1):112.
53. Acuin J. Chronic suppurative otitis media. BMJ Clinical Evidence 2008. Available
at: http://clinicalevidence.bmj.com. Accessed June 27, 2008.
54. van der Veen EL, Schilder AG, van Heerbeek N, et al. Predictors of chronic
suppurative otitis media in children. Arch Otolaryngol Head Neck Surg 2006;
132(10):11158.
55. Leach AJ, Morris PS. The burden and outcome of respiratory tract infection in
Australian and aboriginal children. Pediatr Infect Dis J 2007;26(10 Suppl):S47.
56. Roberts JE, Rosenfeld RM, Zeisel SA. Otitis media and speech and language:
a meta-analysis of prospective studies. Pediatrics 2004;113(3 Pt 1):e23848.
57. Takata GS, Chan LS, Morphew T, et al. Evidence assessment of the accuracy of
methods of diagnosing middle ear effusion in children with otitis media with
effusion. Pediatrics 2003;112(6 Pt 1):137987.
Upper Respiratory Tract Infections 115
58. Rothman R, Owens T, Simel DL. Does this child have acute otitis media? JAMA
2003;290(12):163340.
59. Straetemans M, Sanders EA, Veenhoven RH, et al. Pneumococcal vaccines for
preventing otitis media. Cochrane Database Syst Rev 2004;(1):CD001480.
60. Jefferson T, Rivetti A, Harnden A, et al. Vaccines for preventing influenza in
healthy children. Cochrane Database Syst Rev 2008;(2):CD004879.
61. Manzoli L, Schioppa F, Boccia A, et al. The efficacy of influenza vaccine for
healthy children: a meta-analysis evaluating potential sources of variation in effi-
cacy estimates including study quality. Pediatr Infect Dis J 2007;26(2):97106.
62. Fireman B, Black SB, Shinefield HR, et al. Impact of the pneumococcal conjugate
vaccine on otitis media. Pediatr Infect Dis J 2003;22(1):106.
63. Flynn CA, Griffin GH, Schultz JK. Decongestants and antihistamines for acute
otitis media in children. Cochrane Database Syst Rev 2004;(3):CD001727.
64. Kozyrskyj AL, Hildes-Ripstein GE, Longstaffe SE, et al. Short course antibiotics
for acute otitis media. Cochrane Database Syst Rev 2000;(2):CD001095.
65. Spurling GK, Del Mar CB, Dooley L, et al. Delayed antibiotics for respiratory in-
fections. Cochrane Database Syst Rev 2007;(3):CD004417.
66. Spiro DM, Tay KY, Arnold DH, et al. Wait-and-see prescription for the treatment of
acute otitis media: a randomized controlled trial. JAMA 2006;296(10):123541.
67. Little P, Gould C, Williamson I, et al. Pragmatic randomised controlled trial of two
prescribing strategies for childhood acute otitis media. BMJ 2001;322(7282):
33642.
68. Leach AJ, Morris PS. Antibiotics for the prevention of acute and chronic suppu-
rative otitis media in children. Cochrane Database Syst Rev 2006;(4):CD004401.
69. Mattila PS, Joki-Erkkila VP, Kilpi T, et al. Prevention of otitis media by adenoidec-
tomy in children younger than 2 years. Arch Otolaryngol Head Neck Surg 2003;
129(2):1638.
70. Hammaren-Malmi S, Saxen H, Tarkkanen J, et al. Adenoidectomy does not signif-
icantly reduce the incidence of otitis media in conjunction with the insertion of
tympanostomy tubes in children who are younger than 4 years: a randomized
trial. Pediatrics 2005;116(1):1859.
71. Macfadyen CA, Acuin JM, Gamble C. Topical antibiotics without steroids for
chronically discharging ears with underlying eardrum perforations. Cochrane
Database Syst Rev 2005;(4):CD004618.
72. Macfadyen CA, Acuin JM, Gamble C. Systemic antibiotics versus topical treat-
ments for chronically discharging ears with underlying eardrum perforations.
Cochrane Database Syst Rev 2006;(1):CD005608.
73. Acuin J, Smith A, Mackenzie I. Interventions for chronic suppurative otitis media.
Cochrane Database Syst Rev 2000;(2):CD000473.
74. van der Veen EL, Rovers MM, Albers FW, et al. Effectiveness of trimethoprim/
sulfamethoxazole for children with chronic active otitis media: a randomized,
placebo-controlled trial. Pediatrics 2007;119(5):897904.
75. Leiberman A, Fliss DM, Dagan R. Medical treatment of chronic suppurative otitis
media without cholesteatoma in childrena two-year follow-up. Int J Pediatr
Otorhinolaryngol 1992;24(1):2533.
76. Dagan R, Fliss DM, Einhorn M, et al. Outpatient management of chronic suppu-
rative otitis media without cholesteatoma in children. Pediatr Infect Dis J 1992;
11(7):5426.
77. Simpson SA, Thomas CL, van der Linden MK, et al. Identification of children in
the first four years of life for early treatment for otitis media with effusion.
Cochrane Database Syst Rev 2007;(1):CD004163.
Morris 116
78. Williamson I. Otitis media with effusion. BMJ Clinical Evidence 2008. Available at:
http://clinicalevidence.bmj.com. Accessed June 27, 2008.
79. American Academy of Family Physicians, American Academy of Otolaryngology-
Head and Neck Surgery, American Academy of Pediatrics Subcommittee on Oti-
tis Media With Effusion. Otitis media with effusion. Pediatrics 2004;113(5):
141229.
80. Rosenfeld RM. Surgical prevention of otitis media. Vaccine 2000;19(Suppl 1):
S1349.
81. Lous J, Burton MJ, Felding JU, et al. Grommets (ventilation tubes) for hearing loss
associated with otitis media with effusion in children. Cochrane Database Syst
Rev 2005;(1):CD001801.
82. Rovers MM, Black N, Browning GG, et al. Grommets in otitis media with effusion:
an individual patient data meta-analysis. Arch Dis Child 2005;90(5):4805.
83. Perera R, Haynes J, Glasziou P, et al. Autoinflation for hearing loss associated
with otitis media with effusion. Cochrane Database Syst Rev 2006;(4):CD006285.
84. Griffin GH, Flynn C, Bailey RE, et al. Antihistamines and/or decongestants for
otitis media with effusion (OME) in children. Cochrane Database Syst Rev
2006;(4):CD003423.
85. Thomas CL, Simpson S, Butler CC, et al. Oral or topical nasal steroids for hearing
loss associated with otitis media with effusion in children. Cochrane Database
Syst Rev 2006;3:CD001935.
Upper Respiratory Tract Infections 117
Acute Bronchi ol i ti s
and Croup
Mark L. Everard, MB, ChB, FRCP, DM
Respiratory viruses are responsible for an extremely high proportion of all disease in
young children presenting to medical services. Preschool children infected by one
of these pathogens usually exhibit clinical illness with one or more upper airways
manifestations such as coryza, pharyngitis, or otitis media. Extension of infection
into the lower airways below the larynx most commonly causes bronchitis, adding
cough to the symptoms associated with the previously mentioned conditions. If the
virus induces airways obstruction (most commonly through the induction of increased
airways secretions and mucosal edema and/or bronchospasm), this obstruction may
be manifest by increased work of breathing resulting in tachypnea and subcostal re-
cession, gas trapping as manifested by hyperinflation, and noisy breathing caused by
turbulent airflow.
The clinical phenotype of disease induced by a viral lower respiratory tract infection
is determined by a number of factors, including the site of maximal inflammation,
which in turn depends in part on the virus, the age of the infant or young child, and
the existence of comorbidities such as atopic asthma. Although certain viruses clas-
sically are associated with certain disease phenotypes, such as parainfluenza with
croup, respiratory syncytial virus (RSV) with acute bronchiolitis, and rhinovirus with ex-
acerbation of asthma, any of the viruses can induce any of the clinical phenotypes.
15
The acute bronchiolitis associated with rhinovirus is clinically indistinguishable from
that caused by RSV; RSV also is an important cause of croup and is responsible for
a significant proportion of exacerbations of asthma in young children. The number
of viruses known to target the respiratory tract continues to grow; viruses such as hu-
man metpneumovirus and human bocavirus have been added to the list of proven and
likely respiratory pathogens.
5
As Fig. 1 indicates for RSV (see Fig. 1A) and rhinovirus
(see Fig. 1B), any of the conditions can be caused by any of the viruses, but the relative
likelihood if a particular virus causing a particular condition varies with the virus.
One of the great challenges for those dealing with lower respiratory tract disease in
children is that the lungs have a very limited repertoire of responses to acute or chronic
insults. Increased airways secretions and cough are common to many conditions,
such as acute or persistent bacterial infections, acute viral infections, untreated
Department of Respiratory Medicine, Sheffield Childrens Hospital, Western Bank, Sheffield S10
2TH, UK
E-mail address: m.l.everard@sheffield.ac.uk
KEYWORDS
Acute bronchiolitis
Croup
Wheeze
Wheezy bronchitis
Pediatr Clin N Am 56 (2009) 119133
doi:10.1016/j.pcl.2008.10.007 pediatric.theclinics.com
0031-3955/08/$ see front matter 2009 Elsevier Inc. All rights reserved.
asthma, and recurrent aspiration. In some individuals bronchoconstriction also can
contribute to airways obstruction. Disease within the lower airways frequently leads
to the generation of adventitial sounds. Secretions within the large airways can induce
audible rattles and coarse airways noises
6,7
but also may contribute to the wheeze in
patients experiencing an exacerbation of asthma or wheezy bronchitis. The lack of
precision in using the term wheeze adds to the difficulties in this area. It is clear
that parents and doctors use the term wheeze for a variety of respiratory, and
indeed nonrespiratory, noises.
79
Because wheeze is a key symptom driving both di-
agnostic and therapeutic decisions, this imprecision is a major problem. Obstruction
of distal airways with secretions may lead to the generation of inspiratory crackles
(crepitations) heard on auscultation as units of alveoli pop open.
The lack of a simple test to distinguish conditions such asthma, wheezy bronchitis,
and bronchiolitis means that care must be taken to describe accurately the phenotype
of disease being experienced by an individual patient. This identification is a key step
in ensuring that the patient receives optimal management. It must also be recognized
that, even when the key clinical features have been considered carefully, it frequently
Fig. 1. Phenotypes of respiratory illness caused by respiratory syncytial virus and rhinovirus.
Everard 120
is impossible to provide an accurate diagnostic label. Apreschool-age child with a clin-
ically apparent viral upper respiratory tract infection, cough, and initial episode of
wheeze may have a viral bronchitis with associated wheezing (wheezy bronchitis) or
an exacerbation of asthma (see Fig. 1). There is no test to distinguish between the
two conditions. Adding to the confusion, many clinicians label such an episode acute
bronchiolitis. The use of the term virally associated wheeze to describe wheezing
associated with a viral infection in a nonasthmatic patient adds further unnecessary
confusion, because the term includes both patients experiencing an exacerbation of
asthma and patients who have wheezy bronchitis. Similarly, the termreactive airways
disease does not help the clinician arrive at a more accurate diagnostic label. Al-
though phenotypically the 13-month-old patient who has asthma may be indistin-
guishable form the 13-month-old patent who has wheezy bronchitis, there may be
very important differences in some of the inflammatory components and the degree
of bronchoconstriction. Thus a child who has wheezy bronchitis may look phenotyp-
ically like a child who has the first exacerbation of asthma; the airways inflammation
dominated by neutrophils is likely to be very similar to that in a young child who has
acute bronchiolitis characterized by widespread crackles. Thus two children with an
obvious viral infection and prominent wheeze may look very similar but may respond
quite differently to therapeutic interventions.
The lack of a definitive test and the resulting reliance on a clinical diagnosis adds
a level of complexity to the consideration of the literature addressing lower airways
conditions such as bronchiolitis. This complexity is compounded by lack of agreement
between countries and indeed among clinicians within countries as to the definition of
acute bronchiolitis.
The clinical entity referred to as acute viral croup (acute laryngotracheobronchi-
tis)
10
is less fraught with ambiguity, and this clarity probably accounts for the relative
lackof controversy concerningthiscondition. Acuteviral croupisidentifiedmorereadily
because, althoughtheinflammationtends toinvolvethelarynx, trachea, andlargebron-
chi, the site of maximal airways obstruction generally is just belowthe larynx and thus is
effectively extrathoracic. This extrathoracic positioning leads to airways obstruction
that is maximal during inspiration: the negative pressure generated during inspiration
leads to narrowing of the upper airway and the extrathoracic portion of the trachea.
As a result, a RSV infection causing significant edema in the upper trachea produces
the clinical picture of croup. When the inflammation is predominantly distal, it may
cause acute bronchiolitis or an exacerbation of asthma with airways obstruction being
maximal during the expiratory phase of the respiratory cycle. The differential diagnosis
of a child who has an apparent viral infection, barking cough, and inspiratory stridor is
quitedifferent fromthat of themany conditions causingobstructioninthedistal airways,
and it is a condition that is much easier to characterize on clinical grounds.
ACUTE BRONCHIOLITIS
Evidence-Based Guidelines
At least two comprehensive evidence-based guidelines covering the diagnosis, man-
agement, and prevention of acute bronchiolitis have been published in the past 18
months. Both the American Academy of Pediatrics (AAP)
11
and the Scottish Intercol-
legiate Guideline Network (SIGN) guidelines
12
from Scotland used rigorous evidence-
based methodology, including a comprehensive review of the literature, the use of
relevant systematic reviews, consultation, and peer review. Reassuringly, in most re-
spects, they have reached the same conclusions and reflect the authors practice
based on a reviewof the literature (Table 1). They state that diagnosis should be based
Acute Bronchiolitis and Croup 121
Table1
Diagnosis and management of acute bronchiolitis and croup
Practice
Recommended/Not
Recommended
Strength of
Recommendation
a
Quality of
Supporting
Evidence
Acute bronchiolitis
Diagnosis and assessment
Diagnosis on basis of history and
examination
Recommended
(see text)
Moderate Low
Transcutaneous oxygen
saturation
Recommended Strong Moderate
Admission based on severity and
risk factors
Recommended Strong Moderate
Virologic testing (for infection
control)
Recommended Weak Low
Hematology/biochemistry Not recommended Strong Moderate
Chest radiograph Not recommended Strong Moderate
Interventions
Oxygen prescription for
transcutaneous oxygen < 92%
Recommended Weak Low
Prevent dehydration and
moderate fluid restriction
Recommended Strong Moderate
Beta-agonists Not recommended Strong Moderate
Adrenaline Not recommended Strong Moderate
Routine antibiotics Not recommended Strong High
Inhaled corticosteroids Not recommended Strong Moderate
Oral corticosteroids Not recommended Strong Moderate
Physiotherapy Not recommended Strong Low
Antiviral therapy (ribavirin) Not recommended Strong Moderate
Antileukotriene therapy Not recommended Strong Moderate
Infection control
Hand decontamination Recommended Strong Strong
Gloves and gowns Recommended Strong Moderate
Croup
Diagnosis and assessment
Clinical diagnosis Recommended Strong Moderate
Admission based on clinical
assessment of severity and risk
factors
Recommended Strong Moderate
Transcutaneous oxygen
measurements
Not recommended Weak Low
Virology Not recommended Strong Moderate
Hematology/biochemistry Not recommended Strong Moderate
Radiology Not recommended Strong Moderate
Interventions
Systemic (or nebulized)
corticosteroids for moderate
and severe croup
Recommended Strong High
(continued on next page)
Everard 122
on clinical assessment and that no test is helpful in making the diagnosis. Assessment
of the severity and need for admission to hospital or intensive care also should be
based on clinical grounds, including assessment of age and risk factors such as pre-
maturity, chronic lung disease, or significant cardiac disease. Pulse oximetry is helpful
in identifying hypoxia, but the two guidelines agree that there is little evidence to sup-
port the use of any one or group of features as a means of predicting progression of
the illness. Investigations such chest radiographs and blood tests are not indicated
unless the illness is atypical or particularly severe. Management consists of good sup-
portive care, which may include intensive supportive care. Management has not
changed essentially since Reynolds and Cook
13
stated in 1963 that oxygen is vitally
important and there is little evidence that any other therapy is consistently or even oc-
casionally useful. Supportive care includes administration of fluids sufficient to pre-
vent dehydration but restricted to prevent problems with hyponatremia caused by
inappropriate antidiuretic hormone secretion. Both guidelines are clear that there is
no proven pharmacologic treatment other than oxygen and that pharmacologic
agents such as a- or b-agonists, inhaled or systemic corticosteroids, ribavirin, and an-
tibiotics should not be used routinely. The use of good infection control measures is
key to preventing nosocomial spread within pediatric units. Hand decontamination,
preferably with an alcohol-based rub, is the most important measure. Gloves and
gowns probably provide further benefit, and education of staff, relatives, and visitors
has been shown to have value. Both guidelines state that monoclonal prophylaxis may
be given to infants at risk, but pharmacoeconomic issues lead to differences in the
strength of the recommendation. Neither set of guidelines mentions a role for interven-
tions to prevent future morbidity, but at present there is no evidence that any treat-
ment, including inhaled or systemic steroids
14
and antileukotriene antagonists
administered during or immediately after the illness, has any impact on future
morbidity.
The guidelines grade the strength of many of these recommendations as high be-
cause they are based on a number of systematic reviews, many of which were under-
taken as part of the Cochrane Collaboration.
1519
There are, however, some subtle,
potentially important differences within this broad consensus that infants and young
children should be managed conservatively, avoiding the unnecessary tests and ther-
apies that do not have any effect. These differences include a trial of a- and b-ago-
nists, the indications for using supplemental oxygen, the use of monoclonal
antibodies in the prevention of RSV disease, the value of viral testing in helping prevent
Table1
(continued)
Practice
Recommended/Not
Recommended
Strength of
Recommendation
a
Quality of
Supporting
Evidence
Nebulized adrenaline for moderate to
severe croup
Recommended Strong Moderate
Heliox Not recommended Weak Low
Humidification/steam Not recommended Strong Moderate
Quality of supporting evidence regarding treatment depends entirely on whether there are
important subgroups within the spectrum of disease covered by the term acute bronchiolitis.
a
Grading is based on the GRADE approach in Guyatt GH, Oxman AD, Vist GE, et al. GRADE: an
emerging consensus on rating quality of evidence and strength of recommendations. BMJ
2008;336:9246.
Acute Bronchiolitis and Croup 123
nosocomial spread, and, perhaps most important of all, the diagnosis of the condition.
Indeed both sets of guidelines seem to have some internal contradictions relating to
some of these issues.
It also is of interest that these guidelines do not reflect practice in many coun-
tries, and there is good evidence that the introduction of similar guidelines in
a variety of countries has had little effect on practice, particularly recommendations
relating to pharmacologic agents, which still are widely prescribed.
2023
In part this
lack of effect may result from the well-known difficulty of changing clinical practice,
in part because clinicians feel that they should provide treatment even though there
is little evidence to support the practice. Principally, however, this lack of effect
probably results from the difficulties involved in agreeing about what acute bron-
chiolitis is. The following section considers possible reasons for the ongoing con-
troversies that exist in this area.
Bronchodilators Should Not Be Used Routinely But Remain an Option
Although the AAP guideline states under recommendation 2a that bronchodilators
should not be used routinely in the management of bronchiolitis (recommendation:
evidence level B; randomized, controlled trials (RCTs) with limitations; preponderance
of harm of use over benefit). It then almost immediately makes recommendation 2b:
that a carefully monitored trial of a-adrenergic or b-adrenergic medication is an option.
Inhaled bronchodilators should be continued only if there is a documented positive
clinical response to the trial using an objective means of evaluation.
Although all national guidelines state that there is no evidence that any pharmaco-
logic agent is useful in the treatment of acute bronchiolitis, the position advocated un-
der recommendation 2b reflects the practice of many clinicians around the world, and
many publications have noted that compliance with the recommendation not to use
pharmacologic agents is poor.
2023
This apparent discrepancy within a guideline
(and the lack of compliance with guidelines) probably reflects the lack of consistency
and specificity in the use of terms such as acute bronchiolitis, asthma, and
wheezy bronchitis by clinicians, be they primary care physicians or tertiary special-
ists. As with all systematic reviews, the conclusions that can be drawn are only as
good as the quality of data available for assessment. Reynolds and Cook13 noted
more than 45 years ago that
Much of the confusion about the management of bronchiolitis results fromthe fact
that are probably two groups of patients: (1) those with obstructive disease result-
ing entirely from infection, thickening of the bronchiolar walls and intrabronchial
secretions and (2) those with a pre-disposition to asthma who develop obstruction
as a result of both inflammation and bronchospasm. The two groups cannot be
readily distinguished on clinical grounds, it would appear that most patients fall
in the first group.
If data are derived from different studies that have different population of patients or
from studies that contain mixed populations, the results at best may be mixed and at
worst are misleading.
Implications of the Lack of Precision in the Definition of Acute Bronchiolitis
When assessing the literature referring to infants who have acute bronchiolitis, it is im-
portant to understand that the publication may refer to one of at least two quite distinct
phenotypes. In the United States and a number of European countries, the term is
used to describe a young child or infant who has an apparent viral respiratory tract in-
fection and a first episode of wheeze, but in the United Kingdom, Australia, and some
Everard 124
parts of Europe, the term refers to an infant who has an apparent viral respiratory tract
infection with lower airways obstruction accompanied by widespread crackles (crep-
itations). The later definition recognizes that such infants may wheeze occasionally or
intermittently during the disease, but widespread crackles are the key diagnostic fea-
ture. The presence of crackles indicates that maximal obstruction is at the level of the
distal airways (bronchiolitis) with terminal unit opening suddenly during inspiration and
resulting in the discontinuous adventitial sounds. Interestingly, countries using this
second definition have much better compliance with the guidelines suggesting that
pharmacologic agents are of little value.
24
Previous studies have indicated that the inflammatory process in patients who
have RSV-induced UK bronchiolitis is dominated by an intense neutrophilic influx
into the airways.
25
This influx seems to be driven by very high levels of cytokines
such as interleukin-8
26
and inhibition of polymorphonuclear neutrophil (PMN) apo-
ptosis.
27
A PMN response seems to be characteristic of the response to this and
other respiratory viruses.
28
PMN products such as human neutrophil elastase
and myeloperoxidase are potent inflammatory mediators driving mucus secretion,
airways edema, and cough. At present it is not known whether the PMNs contribute
significantly to elimination of the virus, and it is possible that the virus utilizes this
response to assist in dissemination to other subjects. In such a context, standard
interventions used to treat older patients who have asthma might well prove to
be ineffective. Corticosteroids are believed to have little effect on neutrophilic
airways inflammation, whereas b-agonists are unlikely to have much effect if bron-
choconstriction is not a prominent feature.
As noted previously and as illustrated in Fig. 1, it is possible that a child who has
an apparent viral infection with a first episode of wheezing (American bronchioli-
tis) may be experiencing a first exacerbation of asthma or may have wheezy
bronchitis. Epidemiologic data suggest that, in patients who have wheezy bron-
chitis, pre-existing factors, which may include relative airways size,
29
predispose
these children to suffering one or more episodes of airways obstruction induced by
a viral lower respiratory tract infection that is accompanied by wheeze. This ten-
dency to wheeze with a viral lower respiratory tract infection declines in the pre-
school years. It is probable, but not proven, that these children have a pattern of
inflammation similar to that seen in those who have UK bronchiolitis but that
the manifestations are different because of lung growth and factors such as the de-
velopment of pores of Kohn. Hence, phenotypically these patients may be indistin-
guishable from a child of similar age who has an exacerbation of asthma, but in
terms of inflammation they are much closer to patients who have UK acute bron-
chiolitis. Hence two children who look very similar may react very differently to
pharmacologic agents.
Because the type of patient included in any cohort or therapeutic study influ-
ences the results obtained, this semantic issue may be key to understanding why
there is such controversy in this field. A group selected on the presence of wheeze
without crepitations is likely to include a sizable group of asthmatics, but epidemi-
ologic data indicate that asthmatics still will represent a minority of the patients.
Consequently any treatment effect that might be present if pure asthmatics
were included might be lost if there is little or no benefit in the wheezy bronchitis
groups. Similarly, if a substantial proportion of the recruited subjects are asth-
matics, this population might be sufficient for a study to show a statistically signif-
icant benefit, even if there is no clinical benefit in the nonasthmatic subjects. The
danger is that such a conclusion might be generalized to the whole population of
young, acutely wheezy children.
Acute Bronchiolitis and Croup 125
The AAP guidelines notes that
Overall, results of the meta-analysis indicated that, at most, 1 in 4 children treated
with bronchodilators might have a transient improvement in clinical score of un-
clear clinical significance. This needs to be weighed against the potential adverse
effects and cost of these agents and the fact that most children treated with bron-
chodilators will not benefit from their use. Studies assessing the impact of bron-
chodilators on long-term outcomes have found no impact on the overall course of
the illness.
Such results would be consistent with the proposal that a significant minority of
those in whom wheeze, in the absence of crackles, is the prominent symptom is likely
to have a virally induced exacerbation of asthma. An alternative explanation, however,
is that, as in any study, some patients will improve while others may remain static or
indeed deteriorate before improving, and that post hoc subgroup analysis provides
spurious evidence for a subgroup of responders.
Clinicians would not withhold b-agonists from an older child experiencing a virally
induced exacerbation of asthma, even though the bronchodilation achieved is limited
(in contrast to an asthmatic with poor control, in whom large changes in lung function
may be observed)
30
and even though bronchodilator per se does not have a significant
impact on the course of the illness or duration of hospitalization. The bronchodilator
provides modest, temporary relief while waiting for the corticosteroids to take effect.
Acute BronchiolitisDiagnostic Recommendations from Guidelines
In their review Reynold and Cook
13
noted that pediatricians recognized that bronchio-
litis is the most common acute lower respiratory tract infection necessitating hospital-
ization in infants less than 1 year of age, but the lack of a clear definition of the illness
has been associated with a marked confusion concerning its management. This prob-
lem is reflected 45 years later in the AAP guidelines that define bronchiolitis as
a disorder most commonly caused in infants by viral lower respiratory tract
infection. It is the most common lower respiratory infection in this age group. It
is characterized by acute inflammation, edema, and necrosis of epithelial cells
lining small airways, increased mucus production, and bronchospasm.
Although most of these features have been confirmed by histology in the most
severely affected patients who die from the condition, the inclusion of bronchospasm
is difficult to justify, particularly because a key recommendation is that bronchodila-
tors should not be used routinely in the management of bronchiolitis.
The guidelines recommend that the diagnosis and assessment should be based on
history and physical examination. They note:
Most clinicians recognize bronchiolitis as a constellation of clinical symptoms and
signs including a viral upper respiratory prodrome followed by increased respira-
tory effort and wheezing in children less than 2 years of age. Clinical signs and
symptoms of bronchiolitis consist of rhinorrhea, cough, wheezing, tachypnea,
and increased respiratory effort manifested as grunting, nasal flaring, and inter-
costal and/or subcostal retractions.
There is no mention of crackles in this section on diagnosis and assessment, al-
though the introduction contains a similar paragraph that includes the sentence,
Signs and symptoms are typically rhinitis, tachypnea, wheezing, cough, crackles,
use of accessory muscles, and/or nasal flaring.
Everard 126
Similarly, the SIGN guidelines are not entirely internally consistent with their defini-
tion of the condition stating that bronchiolitis is a condition characterized by fever,
nasal discharge, a dry wheezy cough and on examination there are widespread fine
crackles and/or high pitched expiratory wheeze. The guidelines then comment that
In the UK, crackles on auscultation are considered to be the hall mark of the
condition. Infants with no crackles and only transient early wheezing are usually
categorised as having viral-induced wheezing and not bronchiolitis. American
definitions place much greater emphasis on the inclusion of wheeze in the defini-
tion. This makes it difficult to extrapolate from American research. Or vice versa!
Does the Definition of Acute Bronchiolitis Matter?
A study of patients admitted to hospital with an RSV infection demonstrated that the
host response is an important determinant of both the phenotype of the acute illness
and subsequent respiratory morbidity.
31
At presentation the patients were ascribed
the phenotypes RSV acute bronchiolitis (bilateral crepitation) or RSV wheeze
(wheeze but no crepitations), and the children were followed to 3 years of age. The
group with wheeze was older at the time of the acute illness and had significantly
higher rates of personal atopy than either the controls or the patients who had RSV
bronchiolitis. (The patients who had RSV bronchiolitis, in turn, had slightly lower levels
of atopy than controls). At 3 years of age the wheezing group had much higher levels of
respiratory morbidity and use of inhaled corticosteroids. This finding suggests that the
wheezing cohort was made up of two different groups, despite their sharing the same
phenotype. Although there was some increase in respiratory morbidity, mainly with vi-
ral infections, in the patients who had RSV bronchiolitis, they did not have higher levels
of inhaled corticosteroid use. These data suggest that it is not the virus per se but host
factors (including immunologic, inflammatory, and physiologic factors) that determine
the phenotype of the acute illness and the pattern of subsequent respiratory morbidity.
Other studies have tried to distinguish RSV bronchiolitis (crackles) from RSV wheeze
prospectively and have found differences in the inflammatory process.
32
These factors
also influence the therapeutic effect, if any, of pharmacologic agents.
Until there is a simple test to diagnose asthma other than its being a condition that
improves significantly with asthma treatment (as manifested by objective bronchodi-
lation in response to b-agonists or a significant change in morbidity in response to
inhaled corticosteroids) and reoccurs if the treatment is withdrawna position
advocated by both the British SIGN/British Thoracic Society
33
and GINA guide-
lines
34
the AAP recommendation 2b is likely to remain reasonable, if wheeze is con-
sidered the key feature of bronchiolitis.
Potential Importance of Choosing the Appropriate End Points
As noted earlier, the inclusion of a mixed population in a study of a pharmacologic
agent may result in missing valuable treatment effects in a minority. Under re-
commendation 2b, the reviews noted that a minority of patients seemed to have
a transient improvement in clinical score of unclear clinical significance. In this
setting the clinical benefit may be missed because of the patients inability to commu-
nicate. The use of b-agonists would not be recommended in older children if their use
did not lead to more rapid discharge compared with systemic corticosteroids alone.
The transient and often small improvement in lung function observed when treating
a patient who has a significant exacerbation of asthma is still appreciated by the
patient while waiting for the corticosteroids to take effect.
Acute Bronchiolitis and Croup 127
Another example of a potential problem in developing evidence-based guidelines is
illustrated in a letter criticizing the AAP guidelines for its recommendation that supple-
mental oxygen be administered if the patients transcutaneous oxygen readings fall
consistently below 90%. In the SIGN guidelines, a threshold value of 92% is
suggested. Neither level seems to be associated with adverse outcomes in the short
term. Extrapolating from the treatment of other conditions, it has been suggested
that accepting levels as low as 90% may be associated with subtle but possibly
important long-term neurodevelopment problems.
35
Because no study has ever
addressed this issue, there is no means of addressing this potential problem without
undertaking a long-term study. Clearly long-term outcomes are very important, as
illustrated by the concerns regarding the possible link between the use of postnatal
corticosteroids to treat chronic lung disease and neurodevelopmental outcomes.
Summary
Two rigorous evidence-based guidelines have come to very similar conclusions, but
there are important, if subtle, differences that seem to relate to the precision with
which terms such as acute bronchiolitis are used. The strength of the recommenda-
tions depends entirely on the robustness of the entry criteria in the studies subject to
systematic reviews. Although the guidelines grade the evidence behind most recom-
mendations as good, being based on RTCs, this grading presupposes that the
subjects included are a homogeneous, clean population, an assumption that may
not be valid.
Presumably because the AAP committee working on the guideline recognized that
this is a definitive, evidence-based guideline with potential limitations beyond their
control, they inserted the prudent statement,
This clinical practice guideline is not intended as a sole source of guidance in the
management of children with bronchiolitis. Rather, it is intended to assist clini-
cians in decision-making. It is not intended to replace clinical judgment or estab-
lish a protocol for the care of all children with this condition. These
recommendations may not provide the only appropriate approach to the manage-
ment of children with bronchiolitis.
CROUP
Viral croup is a common clinical illness most commonly seen in preschool children,
generally between 6 months and 5 years of age. The incidence peaks in the second
year of life, and around 15% of children experience at least one episode. Although
the infection involves the larynx and large central airways, the airways obstruction,
when present, occurs during inspiration with the maximal narrowing occurring in the
upper, extrathoracic, trachea.
10
As with all viral infections, the severity ranges widely,
from an irritating barking cough to severe, life-threatening airways obstruction. The
management of croup has been transformed during the past 20 years, in large part
because of a systematic review that reviewed earlier small studies assessing the
potential role of steroids in the management of croup.
36
Many pediatric pulmonolo-
gists previously had conclude that steroids had no place in the management of this
conditions. This conclusion was based on small, underpowered studies; some of
these studies had found a trend toward benefit, but none had demonstrated any clear,
statistically significant benefit. The meta-analysis undertaken by Kairys and
colleagues,
36
however, showed clearly that this opinion should be reconsidered. A
series of studies, first in the ICU
37
and then in the emergency room, followed,
Everard 128
indicating that corticosteroids, administered orally, parentally, or inhaled, led to a rapid
improvement in the clinical status of patients who had croup.
38
Many centers have
reported that admissions to hospital and intensive care have fallen dramatically with
this approach,
39
although the use of corticosteroids does not inevitably prevent pro-
gression and even death.
40
More recent studies have considered the use of cortico-
steroids even for milder disease managed in the community. Interestingly, despite
the systematic review and evidence from the ICU, one of the first large emergency
room studies was rejected by a major journal largely because one reviewer believed
that such a study was unethical as everyone knew steroids did not work in croup
(G. Geelhoed, personal communication, 1998).
Assessment
Diagnosis
The diagnosis of acute viral croup is based on clinical assessment. The differential di-
agnosis in patients who have moderate to severe airways obstruction with stridor in-
cludes any condition that might cause acute narrowing at the larynx or upper
trachea.
10,40,41
Traditionally the most important differential diagnosis has been acute
epiglottitis, although the incidence of this condition has fallen dramatically with the
widespread use of vaccination against type b Haemophilus influenzae. It still is impor-
tant, however, to consider the possibility that it a child may have epiglottitis, which can
occur because of vaccine failure or infection with other organisms. Laryngeal foreign
bodies, bacterial tracheitis, retropharyngeal abscess, and angioedema are other
important conditions to consider. Particularly severe symptoms or presentation at
a very young age should raise the possibility of an underlying problem such as
subglottic stenosis. It is important to ensure that the diagnosis is correct, because sev-
eral of these conditions require urgent and distinct forms of treatment.
Severity
Children who have stridor should be kept as calm as possible, and medical staff
should avoid upsetting the child. Crying generates large negative intrathoracic pres-
sures that exacerbate the collapse of the narrowed tracheal lumen and can provoke
a vicious circle of increased distress caused by the increased difficulty breathing
that leads to further crying and continued excessive airways narrowing. A number
of croup scores have been devised, principally for the research setting. The most
widely used is the one reported by Westley,
42
which has been used in a number of
therapeutic trials. Although a number of emergency departments use these scores,
evidence is lacking that the use of a scoring system improves treatment decisions
or outcomes. It is argued consistently that clinical assessment of airways obstruction,
which includes the patients general appearance as well as the presence of stridor and
recession, is critical, as is regular, repeated reassessment until the patient is clearly
improving.
10,41,43
This approach can be viewed as a consensus position based on
expertise rather than on objective studies. Pulse oximetry is widely used but is of
limited significance, because values are normal or minimally affected in almost all
infants. Low oxygen saturations caused by narrowing of the extrathoracic trachea,
as seen in croup, is evidence of very severe narrowing. In distal airways obstruction,
as seen in bronchiolitis, the huge number of airways within each generation means
that hypoxia can be treated with supplemental oxygen without placing the patient at
risk of catastrophic obstruction. In upper tracheal obstruction, however, the lumen
narrows markedly before the child becomes hypoxic, and the patient then is at risk
of catastrophic cardiorespiratory arrest. Therefore hypoxia caused by croup is an
indication that the child should be transferred safely to an ICU or high-dependency
Acute Bronchiolitis and Croup 129
unit. Conversely, patients who have mild disease may have evidence of mild hypoxia
caused by concurrent involvement of the lower airways tract.
There is no evidence that any other investigation is helpful, and indeed investiga-
tions such as blood tests or radiographs, which may cause distress, can exacerbate
the situation significantly, both in croup and in conditions that can mimic croup, such
as epiglottitis.
Treatment
As noted earlier, the key change in the management of croup has been the widespread
administration of corticosteroids, by a variety of routes, to patients who have moder-
ate or severe croup (see Table 1). There is increasing evidence that a single dose of
a corticosteroid may have benefits even in patients who have relatively mild symp-
toms, such as mild stridor and recession only when upset. It is widely believed that
a single dose has no significant long-term effects, so the riskbenefit ratio favors
the use of such agents. The Cochrane review addressing this issue
38
was updated
most recently in 2004 and found significant benefits in a range of outcomes, including
improvements in severity scores at 6 hours, reduced re-presentation and readmis-
sions, shorter length of stay in those admitted to hospital, and a reduction in the
use of epinephrine. The review was unable to show an effect on the need for intuba-
tion. When assessing the relative effectiveness of oral and inhaled therapy, the
reviewers were unable to identify a clear benefit of one method of administration
over the other, although there was a strong trend for inhaled fluticasone delivered
via spacer to be less effective than dexamethasone or nebulized budesonide. The
reviewers concluded, In the absence of further evidence, a single oral dose of dexa-
methasone, probably 0.6 mg/kg, should be preferred because of its safety, efficacy,
and cost-effectiveness. In a child who is vomiting, nebulized budesonide or intramus-
cular dexamethasone might be preferable. Studies to define optimal doses are on
going, with a number of studies suggesting that lower doses are as effective as higher
ones.
44,45
The other pharmacologic agent shown to have a benefit is epinephrine. There is no
meta-analysis, but a number of RTCs consistently have indicated that there are clinical
benefits.
4652
Although early studies reported using racemic adrenaline, this drug has
not been shown to be superior to L-epinephrine.
46
Unlike corticosteroids, this form of
therapy does not alter the natural history of the illness but does reduce the severity of
symptoms transiently, probably through vasoconstriction leading to reduced hyper-
emia and edema. The onset is rapid (< 30 minutes), but the duration of efficacy is short
(< 2 hours). The standard dose seems to be 0.5 mL/kg body weight nebulized up to
a maximum of 5 mL (10 kgs or greater). Although there is good evidence that epineph-
rine can reduce symptom scores temporarily, there is no clear guidance as to when it
should be used. It is used frequently to provide symptomatic relief in patients who
have moderate to severe symptoms while waiting for corticosteroids to take effect.
Tachycardia and pallor are relatively common; more serious side effects seem to be
rare,
53
although a case of myocardial infarction has been reported following frequent
administration in a young child who had severe obstruction.
54
Potentially, the most
significant problem is that frequent use of epinephrine could mask a significant
deterioration in the underlying obstruction.
Heliox (70/30 helium/oxygen mixture) also has been advocated as a therapeutic
intervention in patients who have severe croup, on the basis that its lower density,
as compared with air, improves gas flow. A small, double-blind, randomized trial
comparing heliox with nebulized epinephrine in patients already receiving systemic
steroids did not identify any benefit of heliox over epinephrine.
55
Unless further data
Everard 130
support this form of therapy, it is unlikely that heliox can be recommended, given the
increased complexity of its use.
A recent Cochrane review found no evidence to support the use of humidified air to
treat children who have croup,
56
even though this practice has been widely advocated
for many decades. The review identified only three small studies based in the emer-
gency department and none in primary care. A subsequent study again found no
benefit from humidification, and this practice cannot be recommended.
57
Summary
Although there is little current controversy regarding the management of croup, as-
sessment remains largely clinical. The natural history seems to be modified by a single
dose of steroids. Although there is a benefit from oral, nebulized, or intramuscular
treatment, oral dexamethasone seems to be the most acceptable method for most
patients. Temporary benefit can be derived from the use of nebulized epinephrine,
and studies indicate that patients can be discharged within 3 to 4 hours after the
last dose, providing there is no deterioration after the effects of epinephrine have
worn off and that the patient is continuing to improve.
REFERENCES
1. Elliott SP, Ray CG. Viral infections of the lower respiratory tract. In: Taussig L,
Landau L, editors. Pediatric respiratory medicine. 2nd Edition. Philadelphia: Mos-
by Elsevier; 2008. p. 48190.
2. Chonmaitree T, Revai K, Grady JJ, et al. Viral upper respiratory tract infection and
otitis media complication in young children. Clin Infect Dis 2008;46:81523.
3. Rihkanen H, Ro nkko E, Nieminen T, et al. Respiratory viruses in laryngeal croup of
young children. J Pediatr 2008;152:6615.
4. Brownlee JW, Turner RB. New developments in the epidemiology and clinical
spectrum of rhinovirus infections. Curr Opin Pediatr 2008;20:6771.
5. Sloots TP, Whiley DM, Lambert SB, et al. Emerging respiratory agents: new
viruses for old diseases? J Clin Virol 2008;42(3):23343.
6. Elphick HE, Ritson S, Rogers H, et al. When a wheeze is not a wheezeanalysis
of breath sounds in infancy. Eur Respir J 2000;16:5937.
7. Elphick H, Everard ML. Noisy breathing in children. In: David T, editor. Recent
advances in paediatrics. The Royal Society of Medicine. London; 2002.
8. Elphick H, Shirlock P, Foxall G, et al. Respiratory noises in early childhood
misuse of the term wheeze by parents and doctor. Arch Dis Child. 2001;84:359.
9. Cane RS, Ranganathan SC, McKenzie SA. What do parents of wheezy children
understand by wheeze? Arch Dis Child 2000;82:32732.
10. Asher MI, Grant CC. Infections of the upper respiratory tract. In: Taussig L,
Landau L, editors. Pediatric respiratory medicine. 2nd Edition. Philadelphia:
Mosby Elsevier; 2008. p. 45380.
11. American Academy of Pediatrics Subcommittee on Diagnosis and Management
of Bronchiolitis. Diagnosis and management of bronchiolitis. Pediatrics 2006;118:
177493.
12. SIGN. Bronchiolitis in children. Available at: http://www.sign.ac.uk. Accessed
November 17, 2008.
13. Reynolds EOR, Cook CD. The treatment of bronchiolitis. J Pediatr 1963;63:
12057.
Acute Bronchiolitis and Croup 131
14. Blom D, Ermers M, Bont L, et al. Inhaled corticosteroids during acute bronchiolitis
in the prevention of post-bronchiolitic wheezing. Cochrane Database Syst Rev
2007;(1):CD004881.
15. Gadomski AM, Bhasale AL. Bronchodilators for bronchiolitis. Cochrane Database
Syst Rev 2006;(3):CD001266.
16. Spurling GK, Fonseka K, Doust J, et al. Antibiotics for bronchiolitis in children.
Cochrane Database Syst Rev 2007;(1):CD005189.
17. Perrotta C, Ortiz Z, Roque M. Chest physiotherapy for acute bronchiolitis in
paediatric patients between 0 and 24 months old. Cochrane Database Syst
Rev 2005;(2):CD004873.
18. Patel H, Platt R, Lozano JM, et al. Glucocorticoids for acute viral bronchiolitis in
infants and young children. Cochrane Database Syst Rev 2004;(3):CD004878.
19. Ventre K, Randolph A. Ribavirin for respiratory syncytial virus infection of the
lower respiratory tract in infants and young children. Cochrane Database Syst
Rev 2004;(4):CD000181.
20. Behrendt CE, Decker MD, Burch DM, et al. International variation in the manage-
ment of infants hospitalized with respiratory syncytial virus. International RSV
Study Group. Eur J Pediatr 1998;157:21520.
21. Barben J, Hammer J. Current management of acute bronchiolitis in Switzerland.
Swiss Med Wkly 2003;133:915.
22. Brand PL, Vaessen-Verberne AA. Differences in management of bronchiolitis
between hospitals in The Netherlands. Dutch Paediatric Respiratory Society.
Eur J Pediatr 2000;159:3437.
23. Touzet S, R
efabert L, Letrilliart L, et al. Impact of consensus development confer-
ence guidelines on primary care of bronchiolitis: are national guidelines being
followed? J Eval Clin Pract 2007;13:6516.
24. Barben JU, Robertson CF, Robinson PJ. Implementation of evidence-based man-
agement of acute bronchiolitis. J Paediatr Child Health 2000;36:4917.
25. Everard ML, Swarbrick A, Wrightham M, et al. Analysis of cells obtained by
bronchial lavage of infants with respiratory syncytial virus infection. Arch Dis Child
1994;71:42832.
26. Turner RB. The role of neutrophiles in the pathogenesis of rhinovirus infections.
Pediatr Infect Dis J 1990;9:8325.
27. Abu-HarbM, Bell F, Rao WH, et al. IL-8 andneutrophil inflammatory mediators in the
upper respiratory tract of infants withRSVbronchiolitis. Eur Respir J 1999;14:1504.
28. Evans GS, Jones A, Qui JM, et al. Neutrophil survival is prolonged in the airways
of healthy infants and infants with RSV bronchiolitis. Eur Respir J 2002;20:6517.
29. Martinez FD. Development of wheezing disorders and asthma in preschool chil-
dren. Pediatrics 2002;109(2 Suppl):3627.
30. Reddel H, Ware S, Marks G, et al. Differences between asthma exacerbations
and poor asthma control. Lancet 1999;353:3649.
31. Elphick H, Ritson S, Rigby AS, et al. Phenotype of acute respiratory syncytial virus
lower respiratory tract illness in infancy and subsequent morbidity. Acta Paediatr
2007;96:13.
32. Pitrez PM, Brennan S, Sly PD. Inflammatory profile in nasal secretions of infants
hospitalized with acute lower airway tract infections. Respirology 2005;10:
36570.
33. BTS/SIGN. British guidelines on the management of asthma. Thorax 2003;58
(Suppl 1):196.
34. Bateman ED, Hurd SS, Barnes PJ, et al. Global strategy for asthma management
and prevention: GINA executive summary. Eur Respir J 2008;31(1):4378.
Everard 132
35. Bass JL, Gozal D. Oxygen therapy for bronchiolitis. Pediatr 2007;119:611.
36. Kairys SW, Olmstead EM, OConnor GT. Steroid treatment of laryngotracheitis:
a meta-analysis of the evidence from randomized trials. Pediatrics 1989;83:68393.
37. Tibballs J, Shann FA, Landau LI. Placebo-controlled trial of prednisolone in
children intubated for croup. Lancet 1992;340:7458.
38. Russell K, Wiebe N, Saenz A, et al. Glucocorticoids for croup. Cochrane Data-
base Syst Rev 2008;(Issue 2). John Wiley & Sons, Ltd.
39. Geelhoed G. Sixteen years of croup in a western Australian teaching hospital:
effects of routine steroid treatment. Ann Emerg Med 1996;28:6216.
40. Fisher JD. Out-of-hospital cardiopulmonary arrest in children with croup. Pediatr
Emerg Care 2004;20:356.
41. Fitzgerald DA, Kilham HA. Croup: assessment and evidence-based manage-
ment. Med J Aust 2003;179:3727.
42. Westley CR, Cotton EK, Brooks JG. Nebulized racemic epinephrine by IPPB for
the treatment of croup: a double-blind study. Am J Dis Child. 1978;132:4847.
43. Bjornson CL, Johnson DW. Croup. Lancet 2008;371:32939.
44. Geelhoed GC, Macdonald WB. Oral dexamethasone in the treatment of croup:
0.15 mg/kg versus 0.3 mg/kg versus 0.6 mg/kg. Pediatr Pulmonol 1995;20:3628.
45. Chub-Uppakarn S, Sangsupawanich P. A randomized comparison of dexameth-
asone 0.15 mg/kg versus 0.6 mg/kg for the treatment of moderate to severe
croup. Int J Pediatr Otorhinolaryngol 2007;71:4737.
46. Waisman Y, Klein BL, Boenning DA, et al. Prospective randomized double-blind
study comparing L-epinephrine and racemic epinephrine aerosols in the treat-
ment of laryngotracheitis (croup). Pediatrics 1992;89:3026.
47. Gardner H, Powell K, Roden V, et al. The evaluation of racemic epinephrine in the
treatment of infectious croup. Pediatrics 1973;52:6871.
48. Fogel J, Berg I, Gerber M, et al. Racemic epinephrine in the treatment of croup:
nebulization alone versus nebulization with intermittent positive pressure breath-
ing. J Pediatr 1982;101:102831.
49. Rizos J, DiGravio B, Sehl M, et al. The disposition of children with croup treated
with racemic epinephrine and dexamethasone in the emergency department.
J Emerg Med 1998;16:5359.
50. Ledwith C, Shea L, Mauro RD. Safety and efficacy of nebulized racemic epineph-
rine in conjunction with oral dexamethasone and mist in the outpatient treatment
of croup. Ann Emerg Med 1995;25:3317.
51. Kunkel N, Baker M. Use of racemic epinephrine, dexamethasone, and mist in the
outpatient management of croup. Pediatr Emerg Care 1996;12:1569.
52. Prendergast M, Jones J, Hartman D. Racemic epinephrine in the treatment of lar-
yngotracheitis: can we identify children for outpatient therapy? Am J Emerg Med
1994;12:6136.
53. Zhang L, Sanguebsche L. The safety of nebulization with 3 to 5 ml of adrenaline
(1:1000) in children: an evidence based review. J Pediatr (Rio J) 2005;81:1937.
54. Butte M, Nguyen B, Hutchison T, et al. Pediatric myocardial infarction after race-
mic epinephrine administration. Pediatr 1999;104:e9.
55. Weber JE, Chudnofsky CR, Younger JG, et al. A randomized comparison of
helium-oxygen mixture (Heliox) and racemic epinephrine for the treatment of
moderate to severe croup. Pediatrics 2001;107:e96.
56. Moore M, Little P. Humidified air inhalation for treating croup. Cochrane Database
Syst Rev 2006;(3):CD002870.
57. Scolnik D, Coates A, Stephens D, et al. Controlled delivery of high vs lowhumidity vs
mist therapy for croup in emergency departments. JAMA 2006;295:127480.
Acute Bronchiolitis and Croup 133
Pneumoni a and Other
Respi ratory I nfecti ons
Sarath C. Ranganathan, MBChB, PhD
a,b,c,
*,
Samatha Sonnappa, MBBS, MD
d,e
EPIDEMIOLOGY
Pneumonia is a leading killer of children, causing an estimated 1.9 million deaths
worldwide in children under the age of 5 years (Fig. 1).
1,2
The true mortality caused
by pneumonia probably is underestimated, because most deaths in developing na-
tions occur at home without a true medical diagnosis. Ninety percent of the deaths
are thought to occur in the developing world, with 50% of these occurring in Africa.
3
The incidence of pneumonia in North America and Europe is approximately 36 per
1000 per year.
4,5
Thus, although mortality is low, pneumonia causes significant mor-
bidity even in developed countries.
DEFINITION
Pneumonia can be defined solely by clinical features
6
or with the addition of radiologic
findings. In part because of the considerable overlap between the diagnosis of bron-
chiolitis and pneumonia in young children,
4
lower respiratory illness is a frequently
used alternative term. Lower respiratory illness has been defined as fever, acute respi-
ratory symptoms, and radiologic evidence of parenchymal infiltrates; the World Health
Organization (WHO) guidelines use tachypnea as an important indicator of pneumonia
when radiology facilities are unavailable.
6
Tachypnea is defined as a respiratory rate
a
Department of Respiratory Medicine, Royal Childrens Hospital Melbourne, Flemington Road,
Parkville, Melbourne, VIC 3052, Australia
b
Infection, Immunity & Environment Theme, Murdoch Childrens Research Institute,
Flemington Road, Parkville, Melbourne, VIC 3052, Australia
c
Department of Paediatrics, University of Melbourne, Flemington Road, Parkville, Melbourne,
VIC 3052, Australia
d
Department of Respiratory Medicine, Great Ormond Street Hospital, Great Ormond Street,
London WC1N 3JH, UK
e
Portex Anaesthesia, Intensive Therapy and Respiratory Medicine Unit, Institute of Child
Health, 30 Guilford Street, London WC1N 1EH, UK
* Corresponding author. Department of Respiratory Medicine, Royal Childrens Hospital
Melbourne, Flemington Road, Parkville, Melbourne, VIC 3052, Australia.
E-mail address: sarath.ranganathan@rch.org.au (S.C. Ranganathan).
KEYWORDS
Pneumonia
Tuberculosis
Respiratory infections
Treatment of pneumonia
Complications of community-acquired pneumonia
Pediatr Clin N Am 56 (2009) 135156
doi:10.1016/j.pcl.2008.10.005 pediatric.theclinics.com
0031-3955/08/$ see front matter 2009 Elsevier Inc. All rights reserved.
greater than 60 breaths per minute in infants younger than 2 months, greater than
50breaths per minuteinchildren2to12months, andgreater than40breaths per minute
in children over 1 year of age. In children who have been symptomatic for more than
3 days, tachypnea has a sensitivity of 74% and a specificity of 67% for radiologically
diagnosed pneumonia.
7
In this study, sensitivity decreased when other clinical signs
were included with tachypnea, but the addition of these other clinical signs increased
specificity in relation to the reference standard of radiologically diagnosed pneumonia.
ETIOLOGY
Pneumonia usually begins as a colonization of the mucosa of the nasopharynx
followed by spread into the lower respiratory tract. The infection can be community
acquired or nosocomial. Bacteria, viruses, atypical organisms, and fungi are all known
to cause pneumonia. In prospective research studies, a causative organism can be
identified in nearly three quarters of cases of pneumonia. Respiratory viruses seem
to be responsible for approximately 40% of cases of community-acquired pneumonia
in children who are hospitalized, particularly in those under 2 years of age, whereas
Streptococcus pneumoniae is responsible for 27% to 44% of the cases of commu-
nity-acquired pneumonia.
8,9,10,11
Although infection with Mycoplasma pneumoniae
and Chlamydia pneumoniae usually are considered to cause pneumonia in children
of school age and in older patients, one study, in which preschool-aged children had
as many episodes of atypical bacterial pneumonia episodes as older children, chal-
lenges this view.
9
In this study a bacterial cause was identified in 60% of cases of
pneumonia, with S. pneumoniae causing 73% of the cases in which a bacterial cause
was identified. Other bacterial causes such as Staphylococcus aureus, Moraxhella
catarrhalis, group A Streptococci, Streptococcus milleri, and Haemophilus species
(nontype b) were identified infrequently. Mycoplasma pneumoniae and Chlamydia
pneumoniae were responsible for 14% and 9% of cases of pneumonia, respectively.
The most severe disease occurred in patients who had infection with a typical bacte-
rial organism or in the 23% in whom mixed bacterial (usually S. pneumoniae) and viral
coinfection were identified.
9
Fig. 1. Global distribution of cause-specific mortality among children under age 5 years in
2004. Pneumonia was the leading killer of children worldwide. (From UNICEF/WHO. Pneu-
monia: the forgotten killer of children. New York and Geneva: The United Nations Childrens
Fund (UNICEF)/World Health Organization (WHO); 2006; with permission.)
Ranganathan & Sonnappa 136
CLINICAL FEATURES
Bacterial pneumonia is unlikely when wheeze is identified in young children (level
of evidence: moderate).
Bacterial pneumonia should be considered in children if fever is higher than 38.5
C
and is accompanied by tachypnea and recession.
12,13
Although auscultatory findings
are not considered as reliable as other clinical signs in the diagnosis of pneumonia,
crackles increase its likelihood. Wheeze in young children (preschool age and below)
suggests a viral cause and in older subjects increases the possibility of infection by
M pneumoniae. Fever, headache, and myalgia in older children are associated with
M pneumoniae, whereas sticky eyes in a neonate are associated with Chlamydia
trachomatis infection.
12,13
MANAGEMENT OF ACHILDWHO HAS COMMUNITY-ACQUIRED PNEUMONIA
AT PRESENTATION
Assess for Contributing Etiology
History is important in the evaluation of community-acquired pneumonia, and the
physician should inquire about contacts, travel, immunization history, the possibility
of foreign body aspiration or primary aspiration, stools consistent with malabsorption,
sinusitis, asthma, and environmental exposure. The examination should evaluate
general features such as growth, upper airway anatomy, dysmorphism suggesting
syndrome, neuromuscular weakness, and swallowing and gag reflexes. The pulmo-
nary examination should assess oxygen saturation, respiratory rate, accessory muscle
use, wheezes, and other auscultatory findings such as crackles. Cardiovascular
examination also is important to rule out signs of cardiac failure.
Assess for Severity of Pneumonia
In terms of severity, the WHO recommends that children who have chest indrawing be
admitted to hospital.
13
The British Thoracic Society guidelines
12,14
regarding admis-
sion to hospital in the developed world are shown in Box 1.
Box1
British Thoracic Society guidelines: factors indicating need for admission of a child
who has pneumonia
Oxygen saturations % 92%
Respiratory rate > 70 breaths per minute in infants or > 50 breaths per minute in older
children
Intermittent apnea, grunting
Difficulty in breathing
Infant not feeding or signs of dehydration in older children
Family unable to provide appropriate observation or supervision
Data from British Thoracic Society. British Thoracic Society guidelines for the management of
community acquired pneumonia in childhood. Thorax 2002;57(Suppl I):i124; and Kumar P,
McKean MC. Evidence based paediatrics: review of BTS guidelines for the management of
community acquired pneumonia in children. J Infect 2004;48(2):1348.
Pneumonia and Other Respiratory Infections 137
AMBULATORYCARE OF ACHILD WHOHAS COMMUNITY-ACQUIRED PNEUMONIA
Investigations are not indicated routinely in mild childhood pneumonia.
The optimal duration of treatment is unknown, but most advocate treatment for 5
to 7 days (level of evidence: low).
Numerous adjunctive therapies in addition to antibiotics are prescribed
frequently for the treatment of pneumonia (Table 1).
INVESTIGATIONS OF ACHILDADMITTED WITH PNEUMONIA
There are widespread variations in practice regarding the investigation of pneumonia
in children who are admitted with this condition.
Chest Radiographs
Chest radiographs should not be performed routinely in children suspected of
having pneumonia (level of evidence: high).
Radiologic findings are accepted as the reference standard for defining pneumonia,
but it is not clear to what extent chest radiographs alter the outcome of childhood
pneumonia even though they frequently are used to confirm the presence, site, and
extent of pulmonary infiltrates. In one study in children between 2 months and 5 years
of age, recovery occurred at a median of 7 days, whether or not a chest radiograph
Table1
Adjunct therapies used in the treatment of childhood community-acquired pneumonia
Medication/
Intervention Recommendation
Grading of
Recommendation
(Based on
Evidence
of Benefit)
Quality of
Supporting Evidence
Antipyretics Pain, fever, and irritability;
no benefit on duration
or severity of pneumonia
Low No randomized,
controlled trials
Cough
suppressants
Not recommended
as adjunct to treat cough
in pneumonia
Moderate Systematic review
concluded
insufficient
evidence
15
Mucolytics Not recommended
in acute community-
acquired pneumonia
Low Systematic review
concluded
insufficient
vidence
15
Chest physical
therapy
Not indicated in
acute community-
acquired
pneumonia
High Randomized,
controlled
trial
16
Zinc
supplementation
Zinc deficiency in
high-mortality
settings decreases
prevalence and
mortality of
pneumonia
High Meta-analysis of 17
randomized,
controlled trials
in children < 5
years
17
Ranganathan & Sonnappa 138
had been performed, and there was no difference in subsequent health care use.
Having a chest radiograph significantly increased the likelihood of being prescribed
antibiotics, however. Routine use of chest radiography was not beneficial in ambula-
tory children over the age of 2 months who had acute lower respiratory tract infec-
tion.
18
The British Thoracic Society suggests that a chest radiograph be considered
in a child younger than 5 years who has with a fever higher than 39
C of unknown or-
igin and without features typical of bronchiolitis.
12
Although lobar infiltrates, effusions,
abscesses, and cavities on a chest radiograph are likely to be a consequence of bac-
terial rather than viral pneumonia,
19
there are no other chest radiograph changes that
are specific in differentiating bacterial from viral pneumonia and therefore indicating
a need for treatment with antibiotics.
Blood Cultures
Blood cultures are positive in only 10% to 30% of children who have pneumonia and
only in pneumonias where bacteremia occurs.
20
In a study in The Gambia, clinical
signs that predicted a positive blood culture were high fever (>38
C), dehydration,
nasal flaring, grunting, bronchial breath sounds, and diminished air entry.
21
Recent
antibiotic use further reduces the chance of a positive blood culture, so in a developed
country, where antibiotics are prescribed earlier in the course of lower respiratory
illness, the clinical features that predict a positive blood culture are likely to be differ-
ent. The British Thoracic Society guidelines recommend performing a blood culture in
all children who are hospitalized and when bacterial pneumonia is suspected.
12
Further Microbiology
Lung aspirates should be considered when peripheral consolidation is proven by
chest radiograph (level of evidence: moderate).
Pleural aspiration is indicated when significant pleural effusion is identified (level
of evidence: moderate).
Microbiologic investigations generally are not recommended for patients being
managed in the community.
12
Within the hospital setting, older children may be able
to provide a sputum sample, but younger children usually cannot. When pulmonary
tuberculosis (TB) is suspected, consecutive early morning, preprandial, preambulatory
gastric washings are indicated and are more sensitive than bronchoalveolar lavage.
Induction of sputum using hypertonic saline may also be useful when TB is suspected,
but this technique increases the chances of a typically noninfectious patient being
rendered temporarily infectious during the procedure.
22
In hospitalized infants under
18 months of age a nasopharyngeal aspirate should be sent for viral antigen detection
(such as immunofluorescence) with or without viral culture.
12
When significant pleural
fluid is present, it should be aspirated and sent for microscopic aspiration and culture
as early as possible during the course of disease, and a specimen should be saved for
bacterial antigen detection.
12
If pleural fluid is associated with a complicated
parapneumonic effusion, a sample of pleural fluid is likely to be obtained during the
management of this complication, so in this circumstance an additional diagnostic
pleural tap may not be in the best interest of the child. Lung aspirates are rarely
performed, but the technique is safer than widely perceived and can provide a bacte-
rial diagnosis in more than 50% of cases.
23
Lung aspirates therefore are more sensi-
tive than blood cultures, but the organisms identified by this technique frequently are
different from those identified by blood cultures taken in the same children.
24
The
limitations of lung aspirates is that they are painful and result in a small (but usually
clinically insignificant) pneumothorax, and the technique usually is limited to
Pneumonia and Other Respiratory Infections 139
pneumonias associated with dense peripheral consolidations close to the chest wall.
Lung aspiration in conjunction with use of nucleic amplification tests can potentially
increase the yield further,
25
and therefore lung aspiration should be considered if
the benefits of identifying the causative agent outweigh the modest risk of the proce-
dure and equipment for and expertise in the management of the potential complication
of a pneumothorax are available.
ORGANISMS CAUSING PNEUMONIA ACCORDING TOAGE
Neonates
Common organisms causing pneumonia in neonates are group B streptococci,
gram-negative enteric bacteria, cytomegalovirus, Ureaplasma urealyticum, Listeria
monocytogenes, and C trachomatis.
Less common organisms causing pneumonia in neonates are S pneumoniae, group
D streptococcus, and anaerobes.
Infants
Common organisms causing pneumonia in infants are respiratory syncytial virus, par-
ainfluenza viruses, influenza viruses, adenovirus, metapneumovirus, S pneumoniae,
H influenzae, M pneumoniae, and Mycobacterium tuberculosis.
Less common organisms causing pneumonia in infants are Bordetella pertussis and
Pneumocystis jiroveci.
Preschool Children
Common organisms causing pneumonia in preschool-age children are respiratory
syncytial virus, parainfluenza viruses, influenza viruses, adenovirus, metapneumovi-
rus, S pneumoniae, H influenzae, M pneumoniae, and M tuberculosis.
A less common organism causing pneumonia in preschool-age children is
C pneumoniae
School-Age Children
Common organisms causing pneumonia in school-age children are M pneumoniae,
C pneumoniae, S pneumonia, M tuberculosis, and respiratory viruses.
Organisms Rarely Causing Pneumonia
The following organisms rarely cause pneumonia:
Viruses: Coronavirus, Varicella-zoster, Epstein-Barr, Mumps
Atypical organisms: Chlamydia psittaci, Coxiella Burnetti
Bacteria: Klebsiella pneumoniae, Legionella, Streptococcus pyogenes, Brucella
abortus
Fungi: Coccidioides immitis, Histoplasma capsulatum, Blastomyces dermatitidis
TREATMENT OF CHILDREN ADMITTED WITH PNEUMONIA
General
Hypoxia (oxygen saturation %92%) should be treated with supplemental oxygen
(level of evidence: moderate).
Initial management always should commence with an assessment of the airway,
breathing, and circulation. Most children do not require admission to hospital. Children
whose oxygen saturation is 92% or less in air should receive supplemental
oxygen therapy.
12
In a Zambian study, the mortality from pneumonia was increased
Ranganathan & Sonnappa 140
when hypoxemia was present, a finding that highlights the importance of oxygen in
treatment.
26
Intravenous fluids rarely are indicated but may be required in the
presence of severe dehydration, ongoing vomiting, severe electrolyte disturbances,
or respiratory failure. In this context, inappropriate secretion of antidiuretic hormone
may occur,
27
and intravenous fluids may need to be administered at 80% of full
maintenance.
Antibiotics
Children who have mild symptoms do not require treatment with antibiotics (level
of evidence: moderate).
Amoxicillin or co-amoxyclavulanic acid is the antibiotic of choice in preschool
children (level of evidence: moderate).
Children over 5 years of age also can be treated with amoxicillin or co-
amoxyclavulanic acid or with a macrolide (or both) when atypical infection is
suspected (level of evidence: moderate).
Antibiotics administered orally are safe and effective for most children (level of
evidence: high).
The optimal duration of treatment for a child admitted with pneumonia is
unknown, but most recommend 5 to 7 days of antibiotics (level of evidence: low).
When a decision has been made to treat with antibiotics, the oral route is the most
appropriate for most children. Although co-trimoxazole is widely used as the first-
choice antibiotic throughout the world, it is inferior to treatment with amoxicillin in
severe pneumonia.
28,29
Amoxicillin is recommended as the first line of therapy for
children under 5 years because it is relatively inexpensive, is well tolerated, and is
effective against most of the pathogens in this age group. Co-amoxyclavulanic acid
seems to be significantly more effective than oral amoxicillin alone but is more expen-
sive.
29
In children older than 5 years, amoxicillin again is an appropriate first-line agent
unless mycoplasma or chlamydia pneumonia is suspected, in which case a macrolide
antibiotic, either alone or in addition, is appropriate. Erythromycin is equally as
effective as
29
and is significantly cheaper than second-generation macrolides such
as azithromycin, clarithromycin, or roxithromycin, but it has a shorter half-life and
requires more frequent dosing. It also may be associated with more frequent adverse
effects, especially involving the gastrointestinal tract.
There is no evidence that intravenous treatment is superior to oral treatment in
community-acquired pneumonia. Intravenous antibiotics therefore are reserved for
severe cases of pneumonia or for pneumonia in a child unable to tolerate oral antibi-
otics. Appropriate antibiotics to administer intravenously include benzyl penicillin, co-
amoxyclavulanic acid, a second- or third-generation cephalosporin, and the addition
of a macrolide if atypical infection is considered a possibility.
ANTIBIOTIC RESISTANCE
Antibiotic resistance is common and increasing, partly in response to inappropri-
ate antibiotic prescribing (level of evidence: moderate).
Principles of good antibiotic prescribing (eg, using the appropriate antibiotic with
the narrowest spectrum, aiming for high tissue or plasma concentrations, a short-
half life, and administered as a short, intensive course) are important and are less likely
to induce antibiotic resistance.
30
Resistance to antibiotics usually is acquired through
selective pressure on bacteria resulting from exposure to antibiotics and preferential
survival of resistant organisms. Pneumococcal resistance has been documented in
Pneumonia and Other Respiratory Infections 141
up to 40% of isolates,
31
and high rates have been reported in Spain, France, and the
United States.
31,32
Mutations in genes coding for penicillin-binding proteins lead to
decreased affinity for penicillin and consequently the failure of penicillin to inhibit
the enzymes responsible for cell wall synthesis. Pneumococcal resistance to penicillin
occurs when the mean inhibitory concentration is less than 2 mg/mL, but there is no
evidence that treatment with high-dose penicillin or cephalosporins for pneumonia
in which pneumococcal resistance is documented is associated with clinical fail-
ure.
33,34,35
Most, however, would consider using a third-generation cephalosporin
or vancomycin if clinical resistance is suspected or when resistance is identified in
a child who is immunosuppressed.
Up to 34% of isolates of H influenzae (including nontypeable strains) are resistant to
ampicillin because of the production of -lactamases by the organism that inhibit the
antibiotic.
36
Therefore, in areas of high endemic resistance, or when resistance is sus-
pected clinically or is identified in an immunosuppressed individual, treatment with
a third-generation cephalosporin is indicated.
Most strains of S aureus are penicillin resistant, because -lactamases are very
prevalent. Methicillin/flucloxacillin resistance also is widespread now, particularly in
hospital-acquired infection but also can be found in community-acquired infections.
37
Vancomycin or teicoplanin are the antibiotics of choice to treat such infections, at least
when vancomycin resistance is not suspected. The outcome may be better when ri-
fampicin is added to treatment with vancomycin,
38
but this benefit is not confirmed
in community-acquired pneumonia. Apart fromresistant S aureus, most other bacteria
that cause hospital-acquired pneumonia are gram-negative organisms such as Pseu-
domonas species, Serratia species, Escherichia coli, and Enterobacter species. Mul-
tidrug resistance has been documented in each of these bacteria, so local guidelines
are necessary for the appropriate selection of antibiotics.
PREVENTION
Vaccines
Vaccines against H influenzae and S pneumoniae are effective (level of evidence:
high).
Vaccines are not currently available in populations where pneumonia has the
highest mortality (level of evidence: high).
The recent development and introduction of conjugate vaccines for H. influenzae
type b (Hib) and S pneumoniae has led to a degree of control of pneumonia caused
by these two organisms in developed countries where they have been introduced
into the immunization schedule. Hib vaccine was introduced in 1990. The first report
froma bacterial pneumonia vaccine trial in the developing world was fromThe Gambia
in 1997,
39
where Hib vaccination reduced clinical pneumonia by 4% and radiologic
pneumonia by 20%. No lung aspirates were identified as culture positive for Hib in chil-
dren who received the vaccine in this study. A further study in Chile also confirmed the
clinical efficacy of Hib vaccine.
40
An Indonesian study, however, in which coverage
with chest radiographs was much greater than in the other two studies, found no ev-
idence for reduction of radiologic pneumonia as a result of the vaccine, even though
a reduction in clinically diagnosed lower respiratory illness was confirmed.
41
The first pneumococcal conjugate vaccine was introduced in 1990. Studies in the
United States,
42
South Africa,
43
and The Gambia
44
have demonstrated its efficacy
against development of clinically diagnosed pneumonia, severe pneumonia, radiolog-
ically defined pneumonia, and vaccine serotypespecific bacteremia or lung aspirate
culture.
45
Newer vaccines that incorporate more serotypes than the nine included in
Ranganathan & Sonnappa 142
the Gambian and South African studies are likely to offer improved efficacy when they
are introduced. Because there are at least 90 pneumococcal serotypes, however, the
risk is that serotype replacement eventually will result in diminished benefit from vac-
cination. The optimal schedule for administration of the seven-valent pneumococcal
vaccine has not yet been determined.
46
As antibiotics become less effective against common bacterial causes of childhood
pneumonia, the role of primary vaccination will become increasingly important. Vacci-
nation decreases the circulation of resistant organisms and, in the case of S pneumo-
niae, the current seven-valent vaccine is effective against the serotypes most
commonly associated with antibiotic resistance.
47
OTHER PREVENTION MEASURES
Environmental, nutritional, and socioeconomic factors affect mortality in child-
hood pneumonia and are preventable (level of evidence: high).
Over the next decade, it is crucial that vaccines become available to children in the
developing world, who are at greatest risk of dying from pneumonia. Failure to make
these vaccines available would indicate that the motives behind vaccine development
do not include a desire to affect significantly the global childhood mortality caused by
pneumonia. Environmental, nutritional, and socioeconomic factors that affect equity of
access are crucially important also.
48
A concerted effort to address these factors in
many developed nations at the beginning of the last century resulted in the large
reduction in mortality from pneumonia that occurred before the availability of antibi-
otics
49
and points out that mortality from pneumonia in childhood reflects socioeco-
nomic disadvantage above all other factors.
COMMON RESPIRATORY ISSUES IN DEVELOPING COUNTRIES
The WHO estimates that nearly one fifth of childhood deaths are caused by pneumo-
nia, which claims more than 2 million lives annually (see Fig. 1). Most of these deaths
occur in Africa and Southeast Asia
2,50
and are caused either by community-acquired
pneumonia or by infections secondary to measles, pertussis, or AIDS/HIV. Most of
these deaths are preventable with available interventions.
51
Although few of these ep-
isodes result in death, they produce significant morbidity and short-term sequelae,
which may have a detrimental effect on the childs nutritional status and also may
influence the risk of other childhood diseases. Effective strategies to combat this
problem include the WHO Integrated Management of Childhood Illness (IMCI)
program, nutritional interventions, and immunization. The use of case management
guidelines recommended by IMCI for childhood pneumonia has reduced overall and
pneumonia-specific mortality in children significantly.
52,53,54
INTEGRATED MANAGEMENT OF CHILDHOOD ILLNESS
The generic IMCI guidelines are meant to target the leading causes of mortality and
severe morbidity in children below 5 years of age, who are a particularly vulnerable
age group. The IMCI strategy incorporates assessment of feeding, updating immuni-
zation status, and provision of vitamin A prophylaxis. The three components of the
IMCI program are improving the skills of health workers, improving the health system,
and improving household and community practices. IMCI is considered to be among
the most cost-effective interventions in both low- and middle-income countries and to
be the program most likely to have the greatest impact on the global burden of
Pneumonia and Other Respiratory Infections 143
disease. As of December 2000, more than 81 countries around the world had adopted
IMCI guidelines.
MANAGEMENT OPTIONS FOR ACUTE RESPIRATORY INFECTION FOLLOWING THE INTEGRATED
MANAGEMENT OF CHILDHOOD ILLNESS APPROACH
Use oral co-trimoxazole rather than other oral/parenteral antibiotics in the treat-
ment of nonsevere pneumonia (level of evidence: high).
Use ambulatory short-course amoxicillin for treatment of severe pneumonia
(level of evidence: high).
Use parenteral chloramphenicol instead of ampicillin plus gentamicin for very
severe pneumonia (level of evidence: high).
Community-based interventions to identify and treat pneumonia have a consider-
able effect on child mortality. The WHO guidelines for the case management of acute
respiratory infections are based on simple signs such as fast breathing and indrawing
of the chest and are designed for countries with an infant mortality rate higher than 40
per 1000 live births.
55
The WHO defines cases of suspected pneumonia as children
reported to have an illness associated with a cough accompanied by fast and/or
difficult breathing. It is recommended that children who have cough without fast
breathing be treated as outpatients without antibiotics; those who have fast breathing
(nonsevere pneumonia) be treated at home with oral co-trimoxazole or amoxicillin for
5 days; and those who have lower chest indrawing (severe pneumonia) and general
danger signs (very severe disease) be referred to hospital and treated with parenteral
ampicillin/penicillin.
A recent meta-analysis assessing the effect of the pneumonia case-management
approach on mortality identified a 24% reduction in total mortality and a 36% reduc-
tion in pneumonia mortality in children under 5 years of age.
52
This analysis of nine
studies
53,54,5662
concluded that community-based interventions to identify and treat
pneumonia have reduced child mortality considerably, with consistent results, despite
the diversity of pneumonia interventions and developing-country settings in which
these trials took place. A potential limitation of this analysis is that all the studies
were undertaken more than a decade ago, and with the increasing prevalence of an-
timicrobial resistance their implications for public health programs are unclear.
In the last decade, and more recently, studies have looked at the efficacy of various
antibiotic regimens in developing country settings.
28,6368
All cases of suspected
pneumonia in these settings should be treated with oral or parenteral antibiotics, de-
pending on severity. The potential choice of antibiotics is wide but should be applica-
ble for large-scale use in low-resource settings. Co-trimoxazole is a cheap and
effective drug, and all the studies show that it compares favorably with other
antibiotics for nonsevere pneumonia. A study comparing the efficacy of co-trimoxa-
zole and that of amoxicillin for nonsevere pneumonia and examining the association
with in vitro co-trimoxazole susceptibility found no difference in efficacy between
co-trimoxazole and amoxicillin, despite high in vitro resistance to co-trimoxazole.
28
Another study comparing the clinical efficacy of twice-daily oral co-trimoxazole and
twice-daily oral amoxicillin found that both were equally effective for the treatment
of nonsevere pneumonia.
63
Three other studies comparing co-trimoxazole with chlor-
amphenicol;
64
with procaine penicillin on day 1 followed by 5 days of oral ampicillin;
65
and with intramuscular procaine penicillin G or benzathine penicillin G in combination
with procaine penicillin G
66
did not indicate any difference in efficacy with alternative
antibiotic regimens. Another double-blind, randomized, controlled trial comparing
a course of the standard dose (45 mg/kg/d) of oral amoxicillin for the treatment of
Ranganathan & Sonnappa 144
nonsevere pneumonia versus a course of a double dose (8090 mg/kg/d) found no dif-
ference between the two doses.
69
The only study assessing oral treatment for severe
pneumonia concluded that home treatment with high-dose oral amoxicillin is equiva-
lent to currently recommended hospitalization and parenteral ampicillin for treatment
of severe pneumonia without underlying complications,
67
but a recent Cochrane re-
view suggested that amoxicillin is better than co-trimoxazole for severe pneumonia.
29
Another study showed that the combination of parenteral ampicillin and gentamicin
was more efficacious than parenteral chloramphenicol alone.
68
Based on these find-
ings, the WHO has revised the guidelines for the management of severe pneumonia to
include home treatment with high-dose oral amoxicillin or a combination of parenteral
ampicillin and gentamicin for hospitalized patients.
TUBERCULOSIS IN CHILDREN ANDADOLESCENTS
The worsening TB pandemic remains a major threat to global health. TB kills nearly 2
million people every year (5000 per day).
70
Precise estimates for the burden of child-
hood TB are not readily available, primarily reflecting the difficulty in diagnosing TB
accurately in children. Children represent an increasing proportion of the total number
of cases in TB-endemic areas, however, with almost 500,000 children succumbing to
the disease each year. Although the overwhelming burden of disease is in developing
countries, several developed countries also have reported a recent increase in the
number of TB cases in children.
71,72
Although in most children the initial infection
occurs in the lungs, TB in children and adolescents should be considered, at least
potentially, to be a systemic disease. The primary complex comprising the site of
infection and the involved regional lymph nodes may heal, or complications may
develop from enlargement or rupture of the regional lymph nodes or from the spread
of tubercle bacilli into the bloodstream, giving rise to disseminated disease. The risk of
dissemination is greatest in the first 5 years of life and within the first 12 to 24 months
after infection and is seen more commonly in children than in adults.
Recently, the Tuberculosis Coalition for Technical Assistance and its partners have
published international standards of care for the management of TB.
73
The reader is
referred to this important document and its 17 standards relating to the diagnosis,
treatment, and public health responsibilities of TB.
Diagnosis
Tuberculosis infection
Diagnosis of TB infection is based on tuberculin skin testing (TST) in the absence of
signs or radiologic findings suggestive of TB disease. The interpretation of a positive
test may be modified by the risk of infection, which is influenced by the contact history,
duration of contact, medical history, and age of the individual and their Bacille Calm-
ette-Guerin (BCG) vaccination status. The TST is an imperfect test. Its interpretation
and subsequent clinical management depend on the prior probability of the test being
positive and on the clinical circumstances of the individual or family.
Tuberculosis disease
Diagnosis of TB disease is based on clinical symptoms and signs, chest radiographs
or other investigations, and smear and culture of infected body material. Although
there are conflicting reports as to whether lateral chest radiographs increase the yield
for detecting intrathoracic lymphadenopathy,
74,75
CT is considered an excellent tool
for detecting mediastinal nodes. CT, however, requires a volumetric scanning protocol
and should not be performed routinely because of the associated high radiation dose.
Pneumonia and Other Respiratory Infections 145
Even though the yieldfromcultures is lowin children, microbiologic confirmation of TB
should be sought. Treatment should be started as soon as samples have been obtained.
Microbiology
In patients unable to produce sputum, gastric aspirates are the investigation of
choice for pulmonary TB in children (level of evidence: moderate).
In younger children, when it is not possible to obtain sputum, gastric aspirates
should be collected on 3 consecutive days. About 50 mL of gastric contents should
be aspirated via a nasogastric tube early in the morning after the child has fasted
for 8 to 10 hours, preferably while the child is still recumbent. Both a smear and culture
should be performed on the aspirate.
If there is radiologic evidence of focal disease, such as lobar, segmental, or subseg-
mental collapse, or clinical evidence of bronchial obstruction, a flexible fiberoptic bron-
choscopy may be indicated to identify and biopsy endobronchial lesions, ideally, with
bronchoalveolar lavage performed in addition to gastric aspiration. Otherwise, bron-
choscopy with bronchoalveolar lavage offers no advantages over gastric aspiration.
76
Inhalation of nebulized sterile hypertonic saline (3% to 6%) via an ultrasonic nebu-
lizer can be used to induce sputum in patients unable to expectorate sputum. The
cough produced by this technique may be of sufficient force to aerosolize tubercle ba-
cilli and infect health care workers, however. Ideally, sputum should be induced in
areas with high-efficiency particulate air filters, and qualified personnel should wear
appropriate respiratory protection.
ROLE OF INTERFERON-GAMMA RELEASE ASSAYS IN CHILDREN
The sensitivity of the currently available interferon-gamma release assays for the diag-
nosis of culture-confirmed TB disease in children is not high enough for these assays
to be used alone to rule out TB.
77
In most studies interferon-gamma release assays
and TST yield equivalent results for the detection of latent TB infection in children,
once adjustment is made for interpretation of the TST based on differing cut-offs,
and some evidence suggests these assays may be less sensitive than TST in
children.
78
Limited data suggest that in situations in which the value of TST is greatly
reduced (eg, in patients infected with HIV), interferon-gamma release assays may
prove useful when used as an adjunct to TST to increase sensitivity. Other specific
situations in which the interferon-gamma release assays might be indicated are
To confirm infection in a child who has been vaccinated with BCG and the TST
result is borderline positive/negative
As a replacement for TST when repeat testing with TST is likely to result in
a booster phenomenon
If TST testing is considered likely to result in a blistering or a large painful
response (eg, in a patient who has had a strong reaction to TST in the past)
For achildwhois unableor unlikely toreturnat 48to72hours for readingof theTST
TREATMENT
Latent Tuberculosis Infection
Treatment of children who have latent TB infection and no evidence of TB disease is
indicated for two reasons: first, to reduce the risk of the patients developing disease in
the years immediately after acquiring the infection, particularly in children under the
age of 5 years, when extrapulmonary disease is more common, and second, to reduce
the lifelong risk of developing TB disease as a consequence of infection. These goals
Ranganathan & Sonnappa 146
can be achieved by the use of isoniazid therapy for a minimum of 6 months. Although
a dose of isoniazid, 5 to10 mg/kg once daily, is recommended, a dose of 10 mg/kg is
optimal: children eliminate isoniazid faster than adults, and therefore relatively larger
doses are required to achieve comparable serum concentrations.
79
Treatment of latent TB infection is particularly important in HlVpositive children,
children in whom corticosteroid or immunosuppressive therapy is contemplated,
and in those who have diabetes or other chronic diseases associated with malnutrition
(eg, celiac disease).
Treatment of latent TB infection in children and adolescents has few side effects.
The incidence of liver toxicity in children is extremely low, and routine monitoring of
liver function is not recommended.
TREATMENT OF PULMONARY TUBERCULOSIS DISEASE
A rifampicin-containing regime is the backbone of antituberculosis treatment for
drug-susceptible M tuberculosis (level of evidence: high).
At least 6 months treatment is recommended using three or four drugs for 2
months with a further continuation phase of 4 months with isoniazid and rifampi-
cin (level of evidence: high).
Children who have TB disease usually are treated with daily therapy with four drugs,
isoniazid, rifampicin, pyrazinamide, and ethambutol, for 2 months, and then generally
with two drugs, isoniazid and rifampicin, for a further 4 months. Normally these drugs
are given daily, but supervised therapy given 3 days a week sometimes is necessary
when adherence with daily therapy is considered to be poor.
Such short-course therapy (6 months) has been shown to be effective in children
who have primary TB and complicated primary TB limited to the respiratory tract.
Infectivity
Childhood TB is rarely contagious (level of evidence: high) because
Children who have TB disease usually have a small bacterial load.
Children are less able to generate the tussive forces needed to aerosolize bacilli.
Children very rarely have cavitating disease.
Young children swallow rather than expectorate sputum.
Occasionally adolescents are seen with cavities caused by TB and then may be
infectious.
Strategies to Improve Adherence
Adherence is a multidimensional phenomenon determined by the interplay of socio-
economic, health system, disease-related, patient-related, and therapy-related fac-
tors.
73
A few pragmatic strategies to enhance treatment adherence include
Emphasizing the importance of adherence at outset of treatment to child and
family
Assigning a key worker to each family with information on how to contact the
worker
Using professional interpreters to communicate if necessary, rather than family
members
Giving information about potential side effects to the child and the family
Providing pill organizers for multidrug regimes
Using combination antibiotic preparations when available and if tolerated
Providing written information in appropriate languages
Pneumonia and Other Respiratory Infections 147
Maintaining close liaison with the dispensing pharmacy regarding collection of
scripts
Having liquid preparations readily available for preschool children
Providing easy access to follow-up
RESPIRATORY INFECTIONS IN HIV-INFECTED CHILDREN
Parenteral benzyl penicillin or ampicillin should be used in combination with gen-
tamicin (level of evidence: high).
The clinical expression of HIV disease in children is highly variable. HIV-related
lower respiratory infections account for 30% to 40% of pediatric admissions and
have a case fatality rate of up to 35%, much higher than the 10% for children not in-
fected with HIV. In addition to S pneumoniae and S aureus, P jiroveci, gram-negative
bacteria, and cytomegalovirus are important opportunistic infections in this group of
children.
80
The WHOdeveloped revised guidelines for presumptive treatment of pneu-
monia in young children in regions where the prevalence of HIV is high. It is recommen-
ded that children admitted with severe pneumonia in HIV-endemic areas receive
benzyl penicillin or ampicillin in combination with gentamicin, irrespective of age,
and that all infants receive high-dose co-trimoxazole because of the high prevalence
of P jiroveci.
81
There are no reported studies assessing the efficacy of these treatment
guidelines since publication. A study conducted before the publication of the guide-
lines used the same recommendations and concluded that in children older than 1
year the WHO guidelines were effective, irrespective of HIV status. For those aged
younger than 1 year, however, the guidelines were found to be inadequate, because
nearly half of the infants did not respond to therapy. This failure was attributed to poly-
microbial disease.
82
COMMON TROPICAL RESPIRATORY INFECTIONS
Pulmonary Hydatid Cyst (Echinococcosis)
Surgical excision of the cyst in conjunction with benzimidazoles is recommended
(level of evidence: moderate).
Exclusive medical therapy is reserved for patients who are poor candidates for
surgery (level of evidence: moderate).
Echinococcosis or hydatid disease is caused by the cystic larval stage of the tape-
worm Echinococcus. The liver is the most common site of cyst formation, followed by
the lung in 10% to 30% of cases. Pulmonary disease seems to be more common in
children and younger individuals. Although most patients are asymptomatic, some
may expectorate the contents of the cyst or develop symptoms related to compres-
sion of the surrounding structures. Surgical excision of the cyst is the treatment of
choice whenever feasible, because the parasite can be removed completely and
the patient cured.
83
The surgical options for lung cysts include lobectomy, wedge
resection, pericystectomy, intact endocystectomy, and capitonnage. Medical therapy
with benzimidazoles is valuable in disseminated disease, including secondary lung or
pleural hydatidosis, in patients who are poor surgical risks, and when there is intrao-
perative spillage of hydatid fluid.
84
PULMONARYAMEBIASIS
Tissue amebicides are effective treatment (level of evidence: moderate).
Surgical management is reserved for patients who have advanced disease (level
of evidence: moderate).
Ranganathan & Sonnappa 148
Amebiasis caused by Entameba histolytica is endemic in the tropical countries. The
lungs are the second most common extraintestinal site after amebic liver abscess.
Pleuropulmonary amebiasis most often is a consequence of the direct extension of
an amebic liver abscess manifested by consolidation, lung abscess, pleural effu-
sion/empyema or hepato-bronchial fistula. Tissue amebicides such as metronidazole,
chloroquine, and dehydroemetine are effective in most patients who have pulmonary
disease.
85,86
Percutaneous pleural drainage and surgical decortication have a role in
patients who have advanced disease.
87,88
TROPICAL EOSINOPHILIA
A 3-week course of diethylcarbamazine is recommended (level of evidence:
moderate).
Tropical eosinophilia is a syndrome characterized by a generalized tissue reaction in
which pulmonary manifestations predominate. An underlying hypersensitivity reaction
to the filarial parasites Wuchereria bancrofti or Brugia malayi results in cough, breath-
lessness, wheeze, marked increase in peripheral eosinophilia, and eosinophilic pulmo-
nary infiltrates.
89,90
Treatment is with a 3-week course of diethylcarbamazine.
91,92
MANAGEMENT OF COMPLICATIONS OF RESPIRATORY INFECTIONS
Empyema
Use a chest drain with intrapleural fibrinolytics (level of evidence: high).
Use video-assisted thoracoscopic surgery (level of evidence: high).
A number of treatment options currently are available for empyema, including sys-
temic antibiotics alone or in combination with thoracocentesis; chest drain insertion,
with or without intrapleural fibrinolytics; and surgical techniques such as
video-assisted thoracoscopic surgery (VATS), mini-thoracotomy, and standard thora-
cotomy with decortication. All these treatment options are safe and effective. Chest
drain with intrapleural fibrinolytics, particularly urokinase,
93,94
and VATS
94,95
have
been shown to be effective primary approaches in the treatment of empyema, with
a shorter duration of hospital stay, which is used consistently as an outcome measure.
The failure rates are similar with both modalities of treatment. The cost of treatment
with intrapleural urokinase is around 25% cheaper than VATS, and, because the
expertise to perform VATS may not be universally available, intrapleural urokinase is
advocated as first-line management.
94
A meta-analysis comparing the results of nonoperative and primary operative
therapy for the treatment of pediatric empyema reviewed 67 studies.
96
Data were
aggregated from reports of children treated nonoperatively (3418 cases from 54 stud-
ies) and from children treated with a primary operative approach (363 cases from 25
studies). Data analysis showed that primary operative therapy was associated with
a lower mortality rate, lower re-intervention rate, shorter length of hospitalization, de-
creased time with a thoracostomy tube, and shorter course of antibiotic therapy,
compared with nonoperative therapy. The limitations of this analysis are that most
of the studies included were observational or retrospective case note reviews. The
observational data from the analysis show that the length of stay is similar for primary
fibrinolytic therapy (10.7 days), thoracotomy (10.6 days), and VATS (11.2 days). The
analysis also suggests that current surgical options for childhood empyema seem
safe, with no reported mortality and little morbidity, and that there is complete resolu-
tion of the disease, whatever the treatment.
Pneumonia and Other Respiratory Infections 149
Pneumatoceles
Pneumatoceles resolve without treatment (level of evidence: moderate).
Refractory cases require surgery (level of evidence: moderate).
Pneumatoceles are associated most frequently with staphylococcal pneumonia but
also are seen in pneumonias caused by S pneumoniae, H influenzae, E coli, and Kleb-
siella. They usually do not produce any additional symptoms to the underlying infective
process and regress spontaneously.
97,98
Surgical management, including drainage,
resection, or decortication, is required only in refractory cases or those that are
symptomatic.
98
Lung Abscess
Lung abscess resolves with a prolonged course of antibiotics (level of evidence:
moderate).
Abscess drainage hastens recovery (level of evidence: moderate).
Lung abscesses coexisting with necrotizing pneumonia or empyema usually do not
require surgical drainage and resolve with a prolonged course of antibiotics adminis-
tered for the pneumonic process.
99
In the last decade, however, there has been
increasing interest in the early use of interventional radiology for the aspiration of
lung abscesses, with or without placement of an external drain, as a way of hastening
recovery and decreasing hospital stay. Surgical resection of the affected lobe is asso-
ciated with significant morbidity and is very rarely advocated.
100,101,102
Bronchopleural Fistulae and Pyopneumothorax
Bronchopleural fistula resolves with continued drainage (level of evidence:
moderate).
Surgical management is useful in protracted cases (level of evidence: moderate).
Bronchopleural fistulae associated with necrotizing pneumonias and empyema
usually are peripheral and resolve with continued chest drainage.
103
Sometimes,
however, they are slow to resolve, and surgical management must be considered.
Talc pleurodesis and limited decortication with muscle flap around the bronchopleural
fistula have been used successfully in protracted cases.
104,105
REFERENCES
1. Wardlaw T, Salama P, Johansson EW, et al. Pneumonia: the leading killer of chil-
dren. Lancet 2006;368(9541):104850.
2. Williams BG, Gouws E, Boschi-Pinto C, et al. Estimates of world-wide distribution
of child deaths from acute respiratory infections. Lancet Infect Dis 2002;2(1):
2532.
3. World Health Organization. The World Health Organization report 2005.
Available at: http://www.who.int/whr/en. 2005. Accessed July 2008.
4. Jokinen C, Heiskanen L, Juvonen H, et al. Incidence of community-acquired
pneumonia in the population of four municipalities in eastern Finland. Am J Epi-
demiol 1993;137(9):97788.
5. McCracken GH Jr. Etiology and treatment of pneumonia. Pediatr Infect Dis J
2000;19(4):3737.
6. World Health Organisation. The management of acute respiratory infections in
children. practical guidelines for outpatient care. Geneva: WHO; 1995.
Ranganathan & Sonnappa 150
7. Palafox M, Guiscafre H, Reyes H, et al. Diagnostic value of tachypnoea in
pneumonia defined radiologically. Arch Dis Child 2000;82(1):415.
8. Heiskanen-Kosma T, Korppi M, Jokinen C, et al. Etiology of childhood pneumo-
nia: serologic results of a prospective, population-based study. Pediatr Infect Dis
J 1998;17(11):98691.
9. Michelow IC, Olsen K, Lozano J, et al. Epidemiology and clinical characteristics
of community-acquired pneumonia in hospitalized children. Pediatrics 2004;
113(4):7017.
10. Wubbel L, Muniz L, Ahmed A, et al. Etiology and treatment of community-
acquired pneumonia in ambulatory children. Pediatr Infect Dis J 1999;18(2):
98104.
11. Juven T, Mertsola J, Waris M, et al. Etiology of community-acquired pneumonia
in 254 hospitalized children. Pediatr Infect Dis J 2000;19(4):2938.
12. British Thoracic Society. British Thoracic Society guidelines for the management
of community acquired pneumonia in childhood. Thorax 2002;57(Suppl I):i124.
13. Pio A. Standard case management of pneumonia in children in developing
countries: the cornerstone of the Acute Respiratory Infection Programme. Bull
World Health Organ 2003;81(4):298300.
14. Kumar P, McKean MC. Evidence based paediatrics: review of BTS guidelines for
the management of community acquired pneumonia in children. J Infect 2004;
48(2):1348.
15. Chang CC, Cheng AC, Chang AB. Over-the-counter (OTC) medications to re-
duce cough as an adjunct to antibiotics for acute pneumonia in children and
adults. Cochrane Database Syst Rev 2007;(4):CD006088.
16. Paludo C, Zhang L, Lincho CS, et al. Chest physical therapy for children hospi-
talized with acute pneumonia: a randomized controlled trial. Thorax 2008;63(9):
7914.
17. Aggarwal R, Sentz J, Miller MA. Role of zinc administration in prevention of child-
hood diarrhea and respiratory illnesses: a meta-analysis. Pediatrics 2007;
119(6):112030.
18. Swingler GH, Hussey GD, Zwarenstein M. Randomised controlled trial of clinical
outcome after chest radiograph in ambulatory acute lower-respiratory infection
in children. Lancet 1998;351(9100):4048.
19. Davies HD, Wang EE, Manson D, et al. Reliability of the chest radiograph in the
diagnosis of lower respiratory infections in young children. Pediatr Infect Dis J
1996;15(7):6004.
20. Anonymous. Pneumonia in childhood. Lancet 1988;1(8588):7413.
21. Banya WA, ODempsey TJ, McArdle T, et al. Predictors for a positive blood cul-
ture in African children with pneumonia. Pediatr Infect Dis J 1996;15(4):2927.
22. Zar HJ, Hanslo D, Apolles P, et al. Induced sputum versus gastric lavage for
microbiological confirmation of pulmonary tuberculosis in infants and young
children: a prospective study. Lancet 2005;365(9454):1304.
23. Vuori-Holopainen E, Peltola H. Reappraisal of lung tap: review of an old method
for better etiologic diagnosis of childhood pneumonia. Clin Infect Dis 2001;32(5):
71526.
24. Falade AG, Mulholland EK, Adegbola RA, et al. Bacterial isolates from blood and
lung aspirate cultures in Gambian children with lobar pneumonia. Ann Trop
Paediatr 1997;17(4):3159.
25. Vuori-Holopainen E, Salo E, Saxen H, et al. Etiological diagnosis of childhood
pneumonia by use of transthoracic needle aspiration and modern microbiolog-
ical methods. Clin Infect Dis 2002;34(5):58390.
Pneumonia and Other Respiratory Infections 151
26. Smyth A, Carty H, Hart CA. Clinical predictors of hypoxaemia in children with
pneumonia. Ann Trop Paediatr 1998;18(1):3140.
27. Dhawan A, Narang A, Singhi S. Hyponatraemia and the inappropriate ADH
syndrome in pneumonia. Ann Trop Paediatr 1992;12(4):45562.
28. Straus WL, Qazi SA, Kundi Z, et al. Antimicrobial resistance and clinical effec-
tiveness of co-trimoxazole versus amoxycillin for pneumonia among children
in Pakistan: randomised controlled trial. Pakistan Co-trimoxazole Study Group.
Lancet 1998;352(9124):2704.
29. Kabra SK, Lodha R, Pandey RM. Antibiotics for community acquired pneumonia
in children. Cochrane Database Syst Rev 2006;3:CD004874.
30. Schrag SJ, McGee L, Whitney CG, et al. Emergence of Streptococcus pneumo-
niae with very-high-level resistance to penicillin. Antimicrobial Agents Chemo-
ther 2004;48(8):301623.
31. Low DE, Pichichero ME, Schaad UB. Optimizing antibacterial therapy for com-
munity-acquired respiratory tract infections in children in an era of bacterial re-
sistance. Clin Pediatr (Phila) 2004;43(2):13551.
32. Whitney CG, Farley MM, Hadler J, et al. Increasing prevalence of multidrug-re-
sistant Streptococcus pneumoniae in the United States. N Engl J Med 2000;
343(26):191724.
33. Deeks SL, Palacio R, Ruvinsky R, et al. Risk factors and course of illness among
children with invasive penicillin-resistant Streptococcus pneumoniae. The Strep-
tococcus pneumoniae Working Group. Pediatrics 1999;103(2):40913.
34. Friedland IR. Comparison of the response to antimicrobial therapy of penicillin-
resistant and penicillin-susceptible pneumococcal disease. Pediatr Infect Dis J
1995;14(10):88590.
35. Tan TQ, Mason EO Jr, Barson WJ, et al. Clinical characteristics and outcome of
children with pneumonia attributable to penicillin-susceptible and penicillin-non-
susceptible Streptococcus pneumoniae. Pediatrics 1998;102(6):136975.
36. Doern GV, Jones RN, Pfaller MA, et al. Haemophilus influenzae and Moraxella
catarrhalis from patients with community-acquired respiratory tract infections:
antimicrobial susceptibility patterns from the SENTRY Antimicrobial Surveillance
Program (United States and Canada, 1997). Antimicrob Agents Chemother
1999;43(2):3859.
37. Gorak EJ, Yamada SM, Brown JD. Community-acquired methicillin-resistant
Staphylococcus aureus in hospitalized adults and children without known risk
factors. Clin Infect Dis 1999;29(4):797800.
38. Gang RK, Sanyal SC, Mokaddas E, et al. Rifampicin as an adjunct to vancomy-
cin therapy in MRSA septicaemia in burns. Bur 1999;25(7):6404.
39. Mulholland K, Hilton S, Adegbola R, et al. Randomised trial of Haemophilus
influenzae type-b tetanus protein conjugate vaccine [corrected] for preven-
tion of pneumonia and meningitis in Gambian infants. Lancet 1997;
349(9060):11917.
40. Levine OS, Lagos R, Munoz A, et al. Defining the burden of pneumonia in
children preventable by vaccination against Haemophilus influenzae type b.
Pediatr Infect Dis J 1999;18(12):10604.
41. Gessner BD, Sutanto A, Linehan M, et al. Incidences of vaccine-preventable
Haemophilus influenzae type b pneumonia and meningitis in Indonesian chil-
dren: hamlet-randomised vaccine-probe trial. Lancet 2005;365(9453):4352.
42. Black S, Shinefield H, Fireman B, et al. Efficacy, safety and immunogenicity of
heptavalent pneumococcal conjugate vaccine in children. Northern California
Ranganathan & Sonnappa 152
Kaiser Permanente Vaccine Study Center Group. Pediatr Infect Dis J 2000;19(3):
18795.
43. Klugman KP, Madhi SA, Huebner RE, et al. A trial of a 9-valent pneumococcal
conjugate vaccine in children with and those without HIV infection. N Engl J
Med 2003;349(14):13418.
44. Cutts FT, Zaman SM, Enwere G, et al. Efficacy of nine-valent pneumococcal con-
jugate vaccine against pneumonia and invasive pneumococcal disease in The
Gambia: randomised, double-blind, placebo-controlled trial. Lancet 2005;
365(9465):113946.
45. Obaro SK, Madhi SA. Bacterial pneumonia vaccines and childhood pneumonia:
are we winning, refining, or redefining? Lancet Infect Dis 2006;6(3):15061.
46. Whitney CG, Pilishvili T, Farley MM, et al. Effectiveness of seven-valent pneumo-
coccal conjugate vaccine against invasive pneumococcal disease: a matched
case-control study. Lancet 2006;368(9546):1495502.
47. Cohen R, Levy C, de La RF, et al. Impact of pneumococcal conjugate vaccine
and of reduction of antibiotic use on nasopharyngeal carriage of nonsusceptible
pneumococci in children with acute otitis media. Pediatr Infect Dis J 2006;
25(11):10017.
48. Mulholland K. Childhood pneumonia mortalitya permanent global emergency.
Lancet 2007;370(9583):2859.
49. Grove RD, Hetzel AM. Vital statistics rates in the United States 19401960.
Washington DC: US National Center for Health Statistics; 1968. 2008.
50. Bryce J, Boschi-Pinto C, Shibuya K, et al. WHO estimates of the causes of death
in children. Lancet 2005;365(9465):114752.
51. Jones G, Steketee RW, Black RE, et al. How many child deaths can we prevent
this year? Lancet 2003;362(9377):6571.
52. Sazawal S, Black RE. Effect of pneumonia case management on mortality in
neonates, infants, and preschool children: a meta-analysis of community-based
trials. Lancet Infect Dis 2003;3(9):54756.
53. Pandey MR, Sharma PR, Gubhaju BB, et al. Impact of a pilot acute respiratory
infection (ARI) control programme in a rural community of the hill region of
Nepal. Ann Trop Paediatr 1989;9(4):21220.
54. Pandey MR, Daulaire NM, Starbuck ES, et al. Reduction in total under-five
mortality in western Nepal through community-based antimicrobial treatment
of pneumonia. Lancet 1991;338(8773):9937.
55. WHO. Programme for the control of acute respiratory infections. Technical basis
for the WHO recommendations on the management of pneumonia in children at
first level health facilities. Geneva, Switzerland: World Health Organization;
1991.
56. Kielmann AA, Taylor CE, DeSweemer C, et al. The Narangwal experiment on
interactions of nutrition and infections: II. Morbidity and mortality effects. Indian
J Med Res 1978;68(Suppl):2141.
57. Mtango FD, Neuvians D. Acute respiratory infections in children under five
years. Control project in Bagamoyo District, Tanzania. Trans R Soc Trop Med
Hyg 1986;80(6):8518.
58. Khan AJ, Khan JA, Akbar M, et al. Acute respiratory infections in children: a case
management intervention in Abbottabad District, Pakistan. Bull World Health
Organ 1990;68(5):57785.
59. World Health Organization. Case management of acute respiratory infections in
children: intervention studies. WHO/ARI/88 2. Geneva: WHO; 1998.
Pneumonia and Other Respiratory Infections 153
60. Bang AT, Bang RA, Tale O, et al. Reduction in pneumonia mortality and total
childhood mortality by means of community-based intervention trial in Gadchir-
oli, India. Lancet 1990;336(8709):2016.
61. Fauveau V, Stewart MK, Chakraborty J, et al. Impact on mortality of a commu-
nity-based programme to control acute lower respiratory tract infections. Bull
World Health Organ 1992;70(1):10916.
62. Roesin R, Sutanto A, Sastra K. ARI intervention study in Kediri, Indonesia
(a summary of study results). Bull Int Union Tuberc Lung Dis 1990;65(4):23.
63. CATCHUP study group. Clinical efficacy of co-trimoxazole versus amoxicillin
twice daily for treatment of pneumonia: a randomised controlled clinical trial in
Pakistan. Arch Dis Child 2002;86(2):1138.
64. MulhollandEK, Falade AG, Corrah PT, et al. Arandomizedtrial of chloramphenicol
vs. trimethoprim-sulfamethoxazole for the treatment of malnourished children with
community-acquired pneumonia. Pediatr Infect Dis J 1995;14(11):95965.
65. Campbell H, Byass P, Forgie IM, et al. Trial of co-trimoxazole versus procaine
penicillin with ampicillin in treatment of community-acquired pneumonia in
young Gambian children. Lancet 1988;2(8621):11824.
66. Sidal M, Oguz F, Unuvar A, et al. Trial of co-trimoxazole versus procaine penicil-
lin G and benzathin penicillin 1 procaine penicillin G in the treatment of child-
hood pneumonia. J Trop Pediatr 1994;40(5):3014.
67. Hazir T, Fox LM, Nisar YB, et al. Ambulatory short-course high-dose oral amox-
icillin for treatment of severe pneumonia in children: a randomised equivalency
trial. Lancet 2008;371(9606):4956.
68. Asghar R, Banajeh S, Egas J, et al. Chloramphenicol versus ampicillin plus gen-
tamicin for community acquired very severe pneumonia among children aged
259 months in low resource settings: multicentre randomised controlled trial
(SPEAR study). BMJ 2008;336(7635):804.
69. Hazir T, Qazi SA, Bin NY, et al. Comparison of standard versus double dose of
amoxicillin in the treatment of non-severe pneumonia in children aged 259
months: a multi-centre, double blind, randomised controlled trial in Pakistan.
Arch Dis Child 2007;92(4):2917.
70. Maher D, Raviglione M. Global epidemiology of tuberculosis. Clin Chest Med
2005;26(2):16782.
71. Atkinson P, Taylor H, Sharland M, et al. Resurgence of paediatric tuberculosis in
London. Arch Dis Child 2002;86(4):2645.
72. Shah NS, Harrington T, Huber M, et al. Increased reported cases of tuberculosis
among children younger than 5 years of age, Maricopa County, Arizona, 2002
2003. Pediatr Infect Dis J 2006;25(2):1515.
73. Tuberculosis Coalition for Technical Assistance. International standards
for tuberculosis care. 2008. Available at: www.istcweb.org/materials.html.
Accessed July 2008.
74. Smuts NA, Beyers N, Gie RP, et al. Value of the lateral chest radiograph in tuber-
culosis in children. Pediatr Radiol 1994;24(7):47880.
75. Swingler GH, du TG, Andronikou S, et al. Diagnostic accuracy of chest radiog-
raphy in detecting mediastinal lymphadenopathy in suspected pulmonary tuber-
culosis. Arch Dis Child 2005;90(11):11536.
76. Abadco DL, Steiner P. Gastric lavage is better than bronchoalveolar lavage for
isolation of Mycobacterium tuberculosis in childhood pulmonary tuberculosis.
Pediatr Infect Dis J 1992;11(9):7358.
77. Ranganathan S, Connell T, Curtis N. Interferon-gamma release assays in
childrenno better than tuberculin skin testing? J Infect 2007;54(4):4123.
Ranganathan & Sonnappa 154
78. Connell TG, Curtis N, Ranganathan SC, et al. Performance of a whole blood
interferon gamma assay for detecting latent infection with Mycobacterium tuber-
culosis in children. Thorax 2006;61(7):61620.
79. Schaaf HS, Parkin DP, Seifart HI, et al. Isoniazid pharmacokinetics in children
treated for respiratory tuberculosis. Arch Dis Child 2005;90(6):6148.
80. Simoes EA, Cherian T, Chow J, et al. Acute respiratory infections in children. In:
Jamieson DT, Breman JG, Measham AR, et al, editors. Disease control priorities
in developing countries. New York: Oxford University Press; 2006. p. 48398.
81. Management of children with pneumonia and HIV in low-resource settings. Re-
port of a consultative meeting. Harare, Zimbabwe, 2003. Geneva: World Health
Organization; 2004.
82. McNally LM, Jeena PM, Gajee K, et al. Effect of age, polymicrobial disease, and
maternal HIV status on treatment response and cause of severe pneumonia in
South African children: a prospective descriptive study. Lancet 2007;
369(9571):144051.
83. Qian ZX. Thoracic hydatid cysts: a report of 842 cases treated over a thirty-year
period. Ann Thorac Surg 1988;46(3):3426.
84. Kilani T, El HS. Pulmonary hydatid and other lung parasitic infections. Curr Opin
Pulm Med 2002;8(3):21823.
85. Cohen HG, Reynolds TB. Comparison of metronidazole and chloroquine for the
treatment of amoebic liver abscess. A controlled trial. Gastroenterology 1975;
69(1):3541.
86. Cameron EW. The treatment of pleuropulmonary amebiasis with metronidazole.
Chest 1978;73(5):64750.
87. Ibarra-Perez C, Selman-Lama M. Diagnosis and treatment of amebic empy-
ema: report of eighty-eight cases. Am J Surg 1977;134(2):2837.
88. Ibarra-Perez C. Thoracic complications of amebic abscess of the liver: report of
501 cases. Chest 1981;79(6):6727.
89. Parab PB, Samuel AM, Udwadia FE, et al. Hypersensitivity reaction in tropical
eosinophilia. Indian J Med Res 1979;69:1227.
90. Ottesen EA, Nutman TB. Tropical pulmonary eosinophilia. Annu Rev Med 1992;
43:41724.
91. Ganatra RD, Sheth UK, Lewis RA. Diethylcarbamazine (Hetrazan) in tropical
eosinophilia. Indian J Med Res 1958;46(2):20522.
92. Pinkston P, Vijayan VK, Nutman TB, et al. Acute tropical pulmonary eosinophilia.
Characterization of the lower respiratory tract inflammation and its response to
therapy. J Clin Invest 1987;80(1):21625.
93. Thomson AH, Hull J, Kumar MR, et al. Randomised trial of intrapleural urokinase
in the treatment of childhood empyema. Thorax 2002;57(4):3437.
94. Sonnappa S, Cohen G, Owens CM, et al. Comparison of urokinase and video-
assisted thoracoscopic surgery for treatment of childhood empyema. Am
J Respir Crit Care Med 2006;174(2):2217.
95. Kurt BA, Winterhalter KM, Connors RH, et al. Therapy of parapneumonic
effusions in children: video-assisted thoracoscopic surgery versus conven-
tional thoracostomy drainage. Pediatrics 2006;118(3):e54753 [Epub 2006
Aug 14].
96. Avansino JR, Goldman B, Sawin RS, et al. Primary operative versus nonopera-
tive therapy for pediatric empyema: a meta-analysis. Pediatrics 2005;115(6):
16529.
97. Victoria MS, Steiner P, Rao M. Persistent postpneumonic pneumatoceles in
children. Chest 1981;79(3):35961.
Pneumonia and Other Respiratory Infections 155
98. Imamoglu M, Cay A, Kosucu P, et al. Pneumatoceles in postpneumonic empy-
ema: an algorithmic approach. J Pediatr Surg 2005;40(7):11117.
99. Asher MI, Spier S, Beland M, et al. Primary lung abscess in childhood: the long-
term outcome of conservative management. Am J Dis Child 1982;136(6):4914.
100. van Sonnenberg E, DAgostino HB, Casola G, et al. Lung abscess: CT-guided
drainage. Radiology 1991;178(2):34751.
101. Yen CC, Tang RB, Chen SJ, et al. Pediatric lung abscess: a retrospective review
of 23 cases. J Microbiol Immunol Infect 2004;37(1):459.
102. Chan PC, Huang LM, Wu PS, et al. Clinical management and outcome of
childhood lung abscess: a 16-year experience. J Microbiol Immunol Infect
2005;38(3):1838.
103. Balfour-Lynn IM, Abrahamson E, Cohen G, et al. BTS guidelines for the manage-
ment of pleural infection in children. Thorax 2005;60(Suppl 1):i121.
104. Puskas JD, Mathisen DJ, Grillo HC, et al. Treatment strategies for bronchopleu-
ral fistula. J Thorac Cardiovasc Surg 1995;109(5):98995.
105. Hallows MR, Parikh DH. Surgical management of children with pyopneumothor-
ax: serratus anterior digitation flap. J Pediatr Surg 2004;39(7):11224.
Ranganathan & Sonnappa 156
Bronchi ectasi s
i n Chi l dren
Gregory J. Redding, MD
a,b,
*
Bronchiectasis is a chronic disease of the conducting airways that produces persis-
tent productive cough, recurrent respiratory infectious exacerbations, and obstructive
lung disease in children and adults. The hallmarks of bronchiectasis are stasis of
infected airway secretions; reduced airway mucus clearance; and regional or diffuse
airway wall dilation, thickening, and destruction with loss of airway structural integrity.
Bronchiectasis is associated with a prolonged neutrophilic inflammatory and secre-
tory response within the airways, producing a wet sounding cough in infants and
young children and mucopurulent sputum expectoration in older children. Bronchiec-
tasis is diagnosed by characteristic images of airways obtained with high-resolution
computerized tomographic scans of the chest.
1
Bronchiectasis is most commonly associatedwithcysticfibrosis (CF) inindustrialized
countries, although there are many etiologies for bronchiectasis unrelated to CF. The
pathogenic mechanisms that predispose to bronchiectasis range from narrowing of
proximal airways (eg, airway compression, intraluminal obstruction) to injury of con-
ducting airways after viral, bacterial, and some fungal infections. Underlying conditions
that affect pulmonary host defenses, suchasCF, primary ciliary dyskinesia, andprimary
and acquired immunodeficiencies, also lead to bronchiectasis. Clinical evaluation in-
cludes identifyinganunderlyingconditionthat canbetreatedwithspecific andsupport-
ive care anddisorders that affect not only the lungs but other organs as well. Conditions
and diseases that predispose to bronchiectasis are listed in Box 1.
This article focuses on the grading and recommendations for chronic therapies of
bronchiectasis caused by CF- and nonCF-related conditions. Chronic therapies do
not necessarily mean daily therapies. For example, aerosol tobramycin is adminis-
tered to children who have CF every other 28-day period but on a regular basis long
Funding was provided in part by the Maternal Child Health Bureau (grant T72MC000007).
There are no financial conflicts of interest pertaining to this article.
a
Department of Pediatrics, University of Washington School of Medicine, Health Sciences, RR
314, Box 356320, 1959 NE Pacific Street Seattle, WA 98195-6320, USA
b
Pulmonary Division, Seattle Childrens Hospital, Room A-5937, 4800 Sand Point Way NE,
Health Sciences, RR 314, Box 356320, 1959 NE Pacific Street Seattle, WA, USA
* Pulmonary Division, Seattle Childrens Hospital, Room A-5937, 4800 Sand Point Way NE,
Seattle, WA, USA.
E-mail address: gredding@u.washington.edu
KEYWORDS
Cystic fibrosis
Bronchiectasis
Children
Lung treatments
Pediatr Clin N Am 56 (2009) 157171
doi:10.1016/j.pcl.2008.10.014 pediatric.theclinics.com
0031-3955/08/$ see front matter 2009 Published by Elsevier Inc.
term.
2
Chronic therapy even might include regular hospitalization for inpatient treat-
ment, but the scope of this article is to focus on outpatient treatment and not include
as-needed treatment for mild or severe pulmonary exacerbations associated with
bronchiectasis. The grading process, as described by the Grade Working Group,
3
in-
cludes quality of evidence, pertinent outcomes of treatment that are disease specific
and relevant to children, and their benefits relative to potential risks. Quality of evi-
dence depends on study design and quality, direct relevance of evidence to the clin-
ical problem, and consistency of findings among studies. Readers are directed to the
Cochrane Collaborations database of systematic reviews.
4
These reviews address
clinical treatments for specific conditions, search the literature for large and small clin-
ical randomized controlled trials (RCTs), and render decisions as to whether publica-
tions are numerous and rigorous enough to make recommendations about treatment
practices. Chronic therapies for bronchiectasis that have Cochrane reviews com-
pleted are listed in Table 1.
Bronchiectasis unrelated to CF has been considered an orphan disease based on
a low prevalence compared with CF in developed countries.
5
Much more research
about treatments has been conducted among patients who have CF than for bronchi-
ectasis attributable to other etiologies. As a result, most research evaluating therapies
for idiopathic bronchiectasis has been conducted in adults rather than in children and
it is debatable whether this information can be extrapolated to younger patients.
Idiopathic bronchiectasis is more prevalent than CF-related disease in certain high-
risk groups, such as indigenous populations, and in developing countries.
68
There
are no treatment RCTs in children belonging to these high-risk groups.
Box1
Conditions that predispose to bronchiectasis in children
Proximal airway narrowing
Airway wall compression (ie, vascular ring, adenopathy impinging on airways)
Airway intraluminal obstruction (eg, inhaled foreign body, granulation tissue)
Airway stenosis and malacia
Airway injury
Bronchiolitis obliterans (eg, postviral, after lung transplantation)
Recurrent pneumonitis or pneumonia (eg, pneumococcal pneumonia, aspiration
pneumonia)
Altered pulmonary host defenses
CF
Ciliary dyskinesia
Impaired cough (eg, neuromuscular weakness conditions)
Altered immune states
Primary abnormalities (eg, hypogammaglobulinemia)
Secondary abnormalities (eg, HIV infection, immunosuppressive agents)
Other
Allergic bronchopulmonary aspergillosis
Plastic bronchitis
Redding 158
Bronchiectasis in this article refers to CF-related and nonCF-related disease
based on the relatively unique pathophysiology of CF and the amount of research
published on therapies for this condition. This is an oversimplified designation, how-
ever. Treatment for different etiologies of nonCF-related bronchiectasis needs to be
individualized based on the etiology of the disease. This is particularly true for under-
lying conditions, such as immunodeficiencies. For example, there are differences be-
tween postinfectious bronchiectasis, in which distribution of initial airway injury
dictates distribution of bronchiectasis, and primary ciliary dyskinesia, in which the
defect in ciliary function is distributed evenly throughout the conducting airways.
The endobronchial pathogens related to bronchiectasis resulting from chronic aspi-
ration differ from those in children who have bronchiectasis associated with primary
hypogammaglobulinemia.
9,10
The most substantial differences may exist between
idiopathic or postinfectious bronchiectasis and bronchiectasis attributable to CF.
These include differences in airway pathogens and the age at which they are ac-
quired, sputum rheologic and transport properties, airway hydration, distribution of
disease, sputum DNA content, extrapulmonary contributors to disease (eg, pancre-
atic insufficiency), and overall progressive nature of the disease.
1113
These differ-
ences may result in different efficacies for some of the chronic therapies directed
toward bronchiectasis.
Table1
Chronic pulmonary therapies for bronchiectasis related and unrelated to cystic fibrosis
Treatment Category Cystic Fibrosis
Non^Cystic Fibrosis^Related
Bronchiectasis
Long-term antibiotics
Aerosol 2003
Oral 2004, 2006 2007
Airway hydration
Hypertonic saline 2005 2006
Mannitol 2002
Mucoactive drugs
DNase 2003 2001
N-acetylcysteine
Anti-inflammatory drugs
Oral corticosteroids 2000 2001
Inhaled corticosteroids 2000
Nonsteroidal agents 2007 2007
Chest physiotherapy 2005 1998
Vaccine
Influenza
Pneumococcal
2000 2007
2007
Bronchodilator 2005
Adrenergics
Anticholinergic
Leukotriene antagonists
2005
2001
2000
Oxygen
Surgical resection
2008 2000
Date of Cochrane review.
Bronchiectasis in Children 159
CLINICAL COURSE OF BRONCHIECTASIS AND EFFECT OF MANAGEMENT PROGRAMS
The natural course of bronchiectasis is dictated by the underlying etiology, severity at
the time of diagnosis, and impact of proactive management programs in specialized
centers of expertise. National guidelines for care have been developed by the Cystic
Fibrosis Foundation addressing all aspects of the disease management on a quarterly
basis to diagnose new infections, nutritional depletion, psychosocial aspects of
chronic progressive disease, adherence to treatment plans, and associated CF-re-
lated conditions, (eg, diabetes mellitus) that may arise at different ages.
14
In patients
who have CF, the median age of survival has significantly increased over time
(Fig. 1).
15
Similar programs have been developed for primary ciliary dyskinesia in pe-
diatric pulmonary referral centers. In children who have ciliary dyskinesia, a proactive
management regimen that included medical evaluations every 3 months led to stabi-
lizing the progressive decline in lung functions over a median interval of 7 years.
16
The
relative contribution of each treatment to the overall improvement in outcomes is dif-
ficult to assess, but longitudinal studies demonstrate that comprehensive proactive
management programs improve pulmonary outcomes of children and adults with
these diagnoses.
In children who have idiopathic bronchiectasis, there is a spectrumof airway disease
andinjury at the time of diagnosis. Differentiation between radiographic features of cy-
lindric and saccular bronchiectasis is made assuming that the former might be re-
versible and that the latter, even with medical therapy, is not. Several published
series have cited complete resolution of symptoms related to idiopathic bronchiectasis
over time.
8,17
Radiographic resolution of bronchiectasis can occur shortly after pneu-
mococcal pneumonia and after chronic foreign body removal.
18
In contrast, idiopathic
bronchiectasis in childhood can also progress by extension to newareas and by evolv-
ing into irreversible saccular changes in previously involved lung regions.
19,20
The pres-
ence, extension, and progression of airway obstruction in children who have idiopathic
Median Predicted Survival Age, 1985-2006
Year
24
26
28
30
32
34
36
38
40
42
'85 '89 '91 '93 '95 '97 '99 '01 '03 '05
M
e
d
i
a
n
S
u
r
v
i
v
a
l
A
g
e
(
Y
e
a
r
s
)
'06 '04 '02 '00 '98 '96 '92 '88 '87 '86 '90 '94
Fig.1. The median predicted survival was 36.9 years for 2006. The data are based on the ages
of patients who have CF in the Cystic Fibrosis Foundation Registry and the mortality distri-
bution of the deaths in 2006. The 95% confidence indicators are noted for each year. In
2006, the median predicted survival was between 34.4 and 41.4 years. (Adapted from Cystic
Fibrosis Foundation. Cystic fibrosis foundation patient registry. 2006 annual data report to
the center directors. Bethesda (MD): Cystic Fibrosis Foundation; 2007; with permission.)
Redding 160
bronchiectasis vary with extent and distribution of disease but progress more slowly
than in children who have CF. This is illustrated in Fig. 2 based on longitudinal trends
in best lung function (forced expiratory volume in 1 second [FEV
1
]) assessed annually
among children with CF- and nonCF-related bronchiectasis.
11
Comprehensive man-
agement programs have been recommended for idiopathic bronchiectasis of child-
hood similar to those for CF and ciliary dyskenesia.
6
Long-term results of such
programs for idiopathic bronchiectasis have not been evaluated, however.
SPECIFIC THERAPIES
Individual treatments for bronchiectasis fall into several larger categories as depicted
in Table 1. Those that have been addressed by the Cochrane database and the date of
the report are also noted in Table 1. These include prevention and reduction of infec-
tion, enhanced mucus clearance, improvements in sputum rheology, treatment of re-
versible airway obstruction if present, improved respiratory muscle strength and
endurance, and reductions in airway inflammation. For severe disease, lung transplan-
tation is an option for patients who have CF.
21
Surgical resection of localized bron-
chiectatic regions also is a treatment option.
A recent report by the Pulmonary Therapies Committee of the Cystic Fibrosis Foun-
dation graded the quality of evidence in the literature pertaining to chronic treatments
for CF-related lung disease.
22
As part of that evidence-based process, the committee
assessed treatment effects based on whether patients had mild or severe lung disease
at the onset of treatment. This valuable distinction has not been made for other etiol-
ogies of bronchiectasis. The reader is directed to that publication to review how effi-
cacies of different therapies differ between mild and severe bronchiectasis
attributable to CF. In addition, published studies use various short- and long-term
outcome measures to assess the utility of different treatments. For purposes of this
article, a long-term outcome has been chosen arbitrarily is one measured over at least
a 6-month interval. Lung-related and extrapulmonary outcome measures described
for the treatment of chronic bronchiectasis are listed in Box 2.
Fig. 2. Linear mixed-model estimated FEV
1
among children with bronchiectasis and children
with CF using best FEV
1
data (dotted line) and all annual data (solid line) using FEV
1
as a per-
cent predicted value obtained longitudinally. (From Twiss J, Stewart AW, Byrnes CA. Longi-
tudinal pulmonary function of childhood bronchiectasis and comparison with cystic fibrosis.
Thorax 2006;61:417; with permission.)
Bronchiectasis in Children 161
Antimicrobial Therapy
Chronic antibiotic therapy directed toward endobronchial pathogens producing infec-
tion, inflammation, and secretion production in patients who have bronchiectasis have
been studied in CF- and nonCF-related bronchiectasis.
3,2330
The treatments have
been targeted toward specific pathogens, such as Pseudomonas and Staphylococ-
cus, and for idiopathic bronchiectasis, Haemophilus influenzae non-type B. Aerosol
treatment with tobramycin for Pseudomonas endobronchial infection in children
who have CF, reported in seven RCTs, has led to short- and long-term benefits, in-
cluding improvement in lung functions, reduction in acute exacerbations and days
of hospitalization, and reduced rate of decline in lung functions for longer than 32
months.
3,28,29,3133
The risk for producing resistant strains of Pseudomonas exists
for up to 30% of patients, compared with 17% of patients in the control group, but oc-
curs infrequently enough that benefits outweigh the risks.
29
Aerosol tobramycin is rec-
ommended as a chronic therapy for mild to severe lung disease related to CF in
children with documented Pseudomonas endobronchial infection.
22
Use of inhaled colistin has been less well studied, and its role is based on two RCTs
of short duration (4890 days).
34,35
In a randomized trial, colistin administered by in-
halation initially over 4 weeks and subsequently over 5 months did not improve
FEV
1
, in contrast to a mean 7% improvement with aerosolized tobramycin over the
same duration in children with CF.
35
Additional aerosolized antibiotics directed toward
Pseudomonas, such as aztreonam, are currently in clinical trials in patients who have
CF.
36
A systematic review of five RCTs using antistaphycoccal treatment for existing
Box 2
Outcome variables for treatment of bronchiectasis
Lung-related
Spirometry: forced vital capacity
FEV
1
Rate of decline in FEV
1
Time to first acute exacerbation after onset of therapy
Exacerbation frequency per time interval
Number of antibiotic courses
Days of hospital treatment of pulmonary status
Sputum volume
Sputum viscoelasticity
Airway reactivity (methacholine responsiveness)
Sputum neutrophils and cytokine levels
Extrapulmonary
Weight velocity
Bacterial density in sputum
C-reactive protein
Days of lost work
Quality of life assessment
Redding 162
bronchiectasis with staphylococcal infection in patients who have CF found that no
outcome was consistently improved.
37
Eradication of Staphylococcus from sputum
was most commonly described, but reductions in cough frequency, respiratory exac-
erbations, and antibiotic courses were not consistently demonstrated across studies.
Use of continuous (>200 days per year) antistaphylococcal antibiotics was associated
with a significantly higher rate of new-onset Pseudomonas airway colonization than
was intermittent antistaphylococcal therapy in young children who had CF.
38
The lat-
ter antibiotic has not been recommended for use on a chronic basis in children who
have CF based on this risk compared with the modest reported benefits.
22
Oral macrolide therapy has been studied with the rationale that this class of antibi-
otics has anti-inflammatory and antisecretogogue properties in addition to antimicro-
bial properties and that the former may be a more important mechanism of efficacy.
39
Three RCTs involving adults and children who had CF have reported a consistent and
modest improvement in FEV
1
values (average of 5.8%) when oral macrolides are
administered daily to three times per week over a 3- to 6-month period.
27,30,40,41
The study by Wolter and colleagues
30
also reported a reduction in hospital days
and serum C-reactive protein levels and a reduced rate of decline in lung functions
over a 3-month interval among adults with CF. Azithromycin administered two times
per week over 6 months reduced use of oral antibiotics for acute exacerbations and
improved quality-of-life survey results but did not affect lung functions among adults
who had nonCF-related bronchiectasis.
26
Two small, short-term, randomized studies
in children with nonCF-related bronchiectasis found no changes in lung function but
reduced airway hyperreactivity and reduced proinflammatory cytokine levels in
bronchoalveolar lavage after 3 months of roxithromycin and clarithromycin,
respectively.
42,43
Among children with nonCF-related bronchiectasis, there have been no long-term
RCTs using antibiotics by any route on a chronic basis. Antipseudomonal treatment in
nonCF-related bronchiectasis is limited to adults and some older children with non
CF-related bronchiectasis because the age acquisition of Pseudomonas is later than
among children who have CF.
44,45
In these older age groups, Pseudomonas eradica-
tion can occur with 4-week courses of aerosolized tobramycin.
46
Short-term (weeks)
of therapy with amoxicillin reduced sputum volume and improved lung function in chil-
dren with nonCF-related bronchiectasis.
24
Daily amoxicillin over 32 weeks reduced
time away from work and daily expectorated sputum volume but did not influence
exacerbation rates in adults with nonCF-related bronchiectasis.
25
Airway Hydration, Mucolytic Treatment, and Chest Physiotherapy
Reduced periciliary airway lining fluid is considered a primary pathogenic mechanism
in CF that impairs mucus clearance by reducing the function of airway cilia.
12
In addi-
tion, rheologic and transport properties of mucus are abnormal in patients who have
CF and patients who have ciliary dyskinesia, more so than among children who have
idiopathic bronchiectasis.
47
Therapies that hydrate the airway and airway mucus and
those that modify mucus rheology in a way that improves mucus transport have been
studied in CF- and nonCF-related bronchiectasis.
Airway hydration has been accomplished with inhalation of hypertonic (6%7% sa-
line), which draws water from cells and tissues into the airway lumen as a result of its
hyperosmolality. Use of 7% saline daily for 48 weeks in an RCT involving adults and
children who had CF led to a reduction in exacerbations and improvement in FEV
1
but no change in the rate of decline in FEV
1
compared with controls.
48
Short-term
use of 6% inhaled saline over a 2-week period in patients who had CF improved
Bronchiectasis in Children 163
FEV
1
, suggesting that the effect is rapid in onset.
49
The risk for bronchospasm, which
can occur with inhalation of hyperosmolar agents, is substantially reduced with pre-
treatment with albuterol.
50
Inhaled dry powder mannitol is an alternative hydrating
agent that improves secretion clearance in a dose-dependent manner (160480 mg
per inhalation) acutely among adults who have nonCF-related bronchiectasis.
51
In
several short-term (2-week) studies, inhaled mannitol increased FEV
1
by 7% in adults
who had CF and improved quality of life in surveys among adult patients who had non
CF-related bronchiectasis.
52,53
Long-term studies using RCT designs are needed to
see if this mannitol proves as useful as hypertonic saline to improve secretion
clearance in CF- and nonCF-related bronchiectasis.
54
Mucolytic agents directly alter physical viscoelastic and transport properties of mu-
cus, which are abnormal among children and adults who have CF and primary ciliary
dyskinesia.
47
The most studied agent is dornase-a or recombinant human DNase,
which degrades extracellular polymers of DNA derived from inflammatory cell break-
down and debris. Used for periods of 6 days to 96 weeks, inhaled DNase once or twice
per day increases FEV
1
, reduces hospitalizations, improves quality of life, and reduces
the decline in lung functions associated with bronchiectasis attributable to CF.
32,5560
Nine long-term RCTs have demonstrated the consistency of this finding in patients
who had mild and severe lung disease attributable to CF, and the daily use of DNase
to improve mucus clearance is recommended for both groups of patients who have
CF.
22
In contrast to these findings, the use of DNase among adults with nonCF-related
bronchiectasis has not provided any benefit. ODonnell
61
reported the one RCT of
twice-daily DNase, compared with placebo, for 24 weeks among adults who had
idiopathic bronchiectasis. Patients receiving DNase had significantly more protocol-
defined exacerbations, a greater annual rate of decline in FEV
1
, and more days of an-
tibiotic use compared with patients receiving placebo. The reasons for these findings
are not clear, although in vitro sputum transportability is worsened by DNase when
sputum samples from adults who had idiopathic bronchiectasis were tested.
62
These
results underscore the need for clinical trials in nonCF-related bronchiectasis without
extrapolation of results from patients who have CF.
N-acetylcysteine disrupts sulfide bonds and thereby reduces the viscosity of puru-
lent mucus sampled fromchildren who have CF. It has been studied in a small number
of children who have CF over short periods. Although modest improvements were
noted compared with placebo-treated patients over 12 weeks, the changes in lung
function were small.
63,64
Given the impact of DNase for patients who have CF, N-ace-
tylcysteine is not a long-term treatment of choice as a mucolytic agent.
Chest physiotherapy (CPT) includes multiple techniques to improve mucus clear-
ance in conjunction with spontaneous or directed cough. Short-term studies have
been reported comparing CPT with no CPT, often in a hospital setting, and also com-
paring different CPT techniques with one another among patients who have CF and
adults who have idiopathic bronchiectasis. Short-term outcomes of benefit include
volume, weight, and viscoelasticity of sputum, but long-term studies have not consis-
tently demonstrated the benefit of this therapy in patients who have CF.
65
CPT using
positive expiratory devices has recently been reviewed by the Cochrane collaboration
separately.
66
Those studies of sufficient quality were conducted over 3 months and
failed to show an improvement in FEV
1
values. Of note, patients who had CF preferred
these devices and also self-directed therapies more than conventional CPT tech-
niques.
67
Among adults who have chronic obstructive lung disease and bronchiecta-
sis, there have not been enough or sufficient quality studies to assess the impact of
CPT techniques on long-term outcomes.
68
Redding 164
ANTI-INFLAMMATORYAGENTS
Therapies for bronchiectasis have been designed to reduce chronic neutrophilic in-
flammation in addition to eradicating infection. Corticosteroids and nonsteroidal
anti-inflammatory treatment have been studied. The use of long-term oral corticoste-
roids (12 mg/kg every other day) consistently increased FEV
1
and reduced the rate of
decline in lung function over 4 years in children who had CF.
6971
The largest of these
RCTs also reported adverse side effects, however, which included abnormalities in
glucose metabolism, reduced height velocity, and cataracts.
70
Risks therefore
outweighed the reported benefits, and long-term corticosteroids are thus not recom-
mended to treat CF-related bronchiectasis. Inhaled corticosteroids have also been
studied in hopes of reducing systemic side effects associated with oral corticoste-
roids. Seven RCTs with a duration of up to 6 months involving children and adults
who had CF have been reported using different compounds at various doses.
72
No im-
provements in lung functions, time to exacerbations, or decline in lung functions over
time occurred in any of the studies.
Use of nonsteroidal anti-inflammatory agents also has potential to reduce neutro-
philic airway inflammation without the side effects of oral corticosteroid therapy. Kon-
stan and colleagues
73
reported a reduction in the rate of lung function decline and
improved weight gain but no change in the frequency of pulmonary exacerbations
when high doses of ibuprofen given twice daily were used for 4 years in children
who had CF. Change in the rate of decline in FEV
1
produced by ibuprofen is illustrated
in Fig. 3. An additional trial has reported similar findings.
74
Severe gastrointestinal
bleeding in less than 1% of patients receiving drug was considered an acceptable
risk compared with the benefits of long-term use among patients who have mild
pulmonary disease.
75
Long-term oral steroid therapy has not been studied in idiopathic bronchiectasis.
Steroids are indicated in the treatment of allergic bronchopulmonary aspergillosis,
whether bronchiectasis is present or absent. Steroid therapy for bronchiectasis in chil-
dren is therefore etiology specific. Among children who have idiopathic
Fig. 3. Estimated average change from baseline FEV
1
as percentage of predicted value over
5 years between patients who had CF and were treated or not treated with high-dose ibu-
profen, based on Cystic Fibrosis Foundation Registry data from 1996 through 2002. (From
Konstan MW, Schluchter MD, Xue W, et al. Clinical use of ibuprofen is associated with slower
FEV
1
decline in childre with cystic fibrosis. Am J Respir Crit Care Med 2007;176(11):10849;
with permission. Copyright 2007, American Thoracic Society.)
Bronchiectasis in Children 165
bronchiectasis, no long-term RCTs have been conducted to assess the effects of in-
haled corticosteroids or oral ibuprofen.
76
OTHER THERAPIES
Remarkably, there are insufficient RCTs to grade the evidence for many pulmonary
therapies for bronchiectasis in children who do not have CF. These therapies include
short- and long-acting b-adrenergic agonists, nonsteroidal anti-inflammatory agents,
leukotriene receptor antagonists, pneumococcal vaccines, and annual influenza
vaccines.
7781
Among adults who have bronchiectasis, only subpopulations of
Box 3
Summary of long-termtreatment recommendations for childhood
1. Comprehensive interdisciplinary chronic disease management programs should treat
children with bronchiectasis (CF- and nonCF-related bronchiectasis).
Grade: low evidence; evidence: cohort studies
2. Pathogen-directed aerosolized tobramycin treatment should be used long termon a regular
basis to improve the course of CF-related bronchiectasis.
Grade: high; evidence: Cochrane reviews, RCTs
3. Oral macrolide antibiotic use short term (up to 6 months) improves lung function among
children with CF-related bronchiectasis.
Grade: moderate; evidence: Cochrane reviews, few RCTs
4. Long-termantibiotic use (oral or aerosolized) in children with nonCF-related bronchiectasis
has not been studied enough to warrant routine use.
Grade: extremely low; evidence: no RCTs or cohort studies
5. Hypertonic saline administered by inhalation used long term (48 weeks) improves lung
function and is safer when used with pretreatment bronchodilator therapy among children
who have CF.
Grade: moderate; evidence: Cochrane review, few RCTs
6. Nebulized dornase-a improves multiple pulmonary outcomes of children who have CF and is
indicated for long-term use.
Grade: high; evidence: Cochrane review, RCTs
7. The risks for long-term oral corticosteroid use outweigh pulmonary benefits in the
treatment of CF-related bronchiectasis.
Grade: moderate; evidence: RCTs
8. High-dose ibuprofen therapy reduces the rate of decline among children with mild CF-
related bronchiectasis and is indicated for long-term use.
Grade: moderate; evidence: Cochrane reviews, few RCTs
9. Mucolytic agents, airway hydrating treatments, anti-inflammatory therapy, CPT, and
bronchodilator therapy have not been studied sufficiently long term in children with non
CF-related bronchiectasis to merit their routine use.
Grade: low; evidence: no RCTs
Redding 166
patients with bronchial hyperreactivity respond to chronic bronchodilator treatment.
78
Although far more patients who have bronchiectasis are treated medically than in the
past, there are no randomized trials to compare medical therapy versus surgical
removal of bronchiectatic regions.
82
Surgery remains a consideration when bronchi-
ectasis is localized to one lobe.
The chronic therapy for bronchiectasis for children who have CF and those who do
not have CF has been additive as new modalities are studied. The sequence of albu-
terol, hypertonic saline, DNAase, and aerosol antibiotic treatments two to three times
per day constitutes an increasing burden of care for patients and families. The addi-
tivity or synergy of these different therapies has not been demonstrated, nor has the
importance of each therapy relative to the others been studied. Data addressing
efficacy of different combinations of therapies for nonCF-related bronchiectasis in
children are nonexistent. Although it has become customary for patients who have
CF to use multiple therapies for bronchiectasis determined at referral CF centers,
the same is not true for nonCF-related bronchiectasis. A similar network for children
with nonCF-related bronchiectasis is necessary if treatments for this group of
children are to be studied and recommendations for treatment are to be derived.
SUMMARY
A summary of the recommendations and graded evidence for long-term treatment of
CF- and nonCF-related bronchiectasis is provided in Box 3. Bronchiectasis is
a chronic airway condition that responds to multiple modalities of chronic treatment
directed toward airway infection, inflammation, hydration, and mucus stasis. Rigorous
studies addressing treatment of bronchiectasis in children who have CF have led to
standards of care that are widely practiced. Similar data for children who have bron-
chiectasis unrelated to CF is lacking. Although approaches to chronic treatment are
extrapolated from studies pertaining to CF in children and nonCF-related bronchiec-
tasis in adults, treatments may not produce the same responses or benefits for chil-
dren with nonCF-related bronchiectasis. Studies directed toward this condition
have an impact, particularly in the developing world and among children with other
underlying conditions in industrialized countries.
ACKNOWLEDGMENTS
The author thanks Holly Kaopuiki for her assistance in preparing the manuscript and
figures for publication.
REFERENCES
1. Westcott JL. Bronchiectasis. Radiol Clin North Am 1991;29:103142.
2. Murphy TD, Anbar RD, Lester LA, et al. Treatment with tobramycin solution for
inhalation reduces hospitalizations in young CF subjects with mild lung disease.
Pediatr Pulmonol 2004;38:31420.
3. Grade Working Group. Education and debategrading quality of evidence and
strength of recommendations. BMJ 2007;328:18.
4. Available at: http://www.cochrane.org/reviews.
5. Callahan CW, Redding GJ. Bronchiectasis in children: orphan disease or
persistent problem? Pediatr Pulmonol 2002;33:4926.
6. Chang AB, Grimwood K, Mulholland EK, et al. Bronchiectasis in indigenous
children in remote Australian communities. Med J Aust 2002;177:2004.
Bronchiectasis in Children 167
7. Edwards EA, Asher MI, Byrnes CA. Paediatric bronchiectasis in the twenty-first
century: experience of a tertiary childrens hospital in New Zealand. J Paediatr
Child Health 2003;39:1117.
8. Singleton R, Morris A, Redding G, et al. Bronchiectasis in Alaska Native children:
causes and clinical courses. Pediatr Pulmonol 2000;29:1827.
9. Brook I, Finegold SM. Bacteriology of aspiration pneumonia in children. Pediatrics
1980;65:111520.
10. Lischner HW, Huang NN. Respiratory complications of primary hypogammaglo-
bulinemia. Pediatr Ann 1977;6:51425.
11. Twiss J, Stewart AW, Byrnes CA. Longitudinal pulmonary function of childhood
bronchiectasis and comparison with cystic fibrosis. Thorax 2006;61:4148.
12. Gibson RL, Burns JL, Ramsey BW. Pathophysiology and management of pul-
monary infections in cystic fibrosis. Am J Respir Crit Care Med 2003;168:
91851.
13. Chang AB, Redding GJ, Bronchiectasis. In: Chernick V, Boat TF, Wilmott RW, et al,
editors. Disorders of the respiratory tract in children, vol 7. Philadelphia: Elsevier
Inc., 2006. p. 46377.
14. Aitken ML, Bergman D, Bolek J, et al. Clinical practice guidelines for cystic fibro-
sis. Bethesda (MD): Cystic Fibrosis Foundation; 1997.
15. Cystic Fibrosis Foundation, Cystic Fibrosis Foundation patient registry. 2006
annual data report to the center directors, Bethesda (MD), 2007.
16. Ellerman A, Bisgaard H. Longitudinal study of lung function in a cohort of primary
ciliary dyskinesia. Eur Respir J 1997;10:23769.
17. Landau LI, Phelan PD, Williams HE. Ventilatory mechanics in patients with bron-
chiectasis starting in childhood. Thorax 1974;29:30412.
18. Gaillard EA, Carty H, Heaf D, et al. Reversible bronchial dilatation in children.
Comparison of serial high-resolution computed tomography scans of the lungs.
Eur J Radiol 2003;47:21520.
19. Clark NS. Bronchiectasis in childhood. BMJ 1963;1:808.
20. Wilson JF, Decker AM. The surgical management of childhood bronchiectasis.
Ann Surg 1982;195:35463.
21. Orens JB, Estenne M, Arcasoy S, et al. International guidelines for the selection of
lung transplant candidates: 2006 updatea consensus report from the
Pulmonary Scientific Council of the International Society for Heart and Lung
Transplantation. J Heart Lung Transplant 2006;25:74555.
22. Flume PA, OSullivan BP, Robinson KA, et al. Cystic fibrosis pulmonary guide-
lines: chronic medications for maintenance of lung health. Am J Respir Crit
Care Med 2007;176:95769.
23. Chang AB, Redding GJ, Everard ML. Chronic wet cough: protracted bronchitis,
chronic suppurative lung disease and bronchiectasis. Pediatr Pulmonol 2008;43:
51931.
24. Cole PJ, Roberts DE, Davies SF, et al. A simple oral antimicrobial regimen
effective in severe chronic bronchial suppuration associated with culturable Hae-
mophilus influenzae. J Antimicrob Chemother 1983;11:10913.
25. Currie DC, Garbett ND, Chan KL, et al. Double-blind randomized study of
prolonged higher-dose oral amoxicillin in purulent bronchiectasis. QJM 1990;
76:799816.
26. Cymbala AA, Edmonds LC, Bauer MA, et al. The disease-modifying effeccts of
twice-weekly oral azithromycin in patients with bronchiectasis. Treat Respir
Med 2005;4:11722.
Redding 168
27. Equi A, Balfour-Lynn IM, Bush A, et al. Long term azithromycin in children with
cystic fibrosis: a randomised, placebo-controlled crossover trial. Lancet 2002;
360:97884.
28. MacLusky IB, Gold R, Corey M, et al. Long-term effects of inhaled tobramycin in
patients with cystic fibrosis colonized with Pseudomonas aeruginosa. Pediatr
Pulmonol 1989;7:428.
29. Ramsey BW, Pepe MS, Quan M, et al. Cystic Fibrosis Inhaled Study Group. Inter-
mittent administration of inhaled tobramycin in patients with cystic fibrosis. N Engl
J Med 1999;340:2330.
30. Wolter J, Seeney S, Bell S, et al. Effect of long term treatment with azithromy-
cin on disease parameters in cystic fibrosis: a randomised trial. Thorax 2002;
57:2126.
31. Ramsey BW, Astley SJ, Aitken ML, et al. Efficacy and safety of short-term admin-
istration of aerosolised recombinant human deoxyribonuclease in patients with
cystic fibrosis. Am Rev Respir Dis 1993;148:14551.
32. Ramsey BW, Dorkin HL, Eisenberg JD, et al. Efficacy of aerosolized tobramycin in
patients with cystic fibrosis. N Engl J Med 1993;328:17406.
33. Wiesemann HG, Steinkamp G, Ratjen F, et al. Placebo-controlled, double-blind,
randomized study of aerosolized tobramycin for early treatment of Pseudomonas
aeruginosa colonization in cystic fibrosis. Pediatr Pulmonol 1998;25:8892.
34. Adeboyeku D, Scott S, Hodson ME. Open follow-up study of tobramycin nebulis-
er solution and colistin patients with cystic fibrosis. J Cyst Fibros 2006;5:2613.
35. Hodson ME, Gallagher CG, Govan JRW. A randomised clinical trial of nebulilsed
tobramycin or colistin in cystic fibrosis. Eur Respir J 2002;20:65864.
36. Gibson RL, Retsch-Bogart GZ, Oermann C, et al. Microbiology, safety, and phar-
macokinetics of aztreonam lysinate for inhalation in patients with cystic fibrosis.
Pediatr Pulmonol 2006;41:65665.
37. McCaffery K, Olver RE, Franklin M, et al. Systematic review of antistaphylococcal
antibiotic therapy in cystic fibrosis. Thorax 1999;54:3803.
38. Ratjen F, Comes G, Paul K, et al. Effect of continuous antistaphylococcal therapy
on the rate of P. aeruginosa acquisition in patients with cystic fibrosis. Pediatr
Pulmonol 2001;31:136.
39. Bush A, Rubin BK. Macrolides as biological response modifiers in cystic fibrosis
and bronchiectasis. Semin Respir Crit Care Med 2003;24:73747.
40. Saiman L, Marshall BC, Mayer-Hamblett N, et al. Azithromycin in patients with
cystic fibrosis chronically infected with Pseudomonas aeruginosa: a randomized
controlled trial. JAMA 2003;290:174956.
41. Southern KW, Barker PM, Solis A. Macrolide antibiotics for cystic fibrosis.
Cochrane Database Syst Rev 2004;(2):CD002203.
42. Koh YY, Lee MH, Sun YH, et al. Effect of roxithromycin on airway responsiveness
in children with bronchiectasis: a double-blind, placebo-controlled study. Eur
Respir J 1997;10:9949.
43. Yalcin E, Kiper N, Ozcelik U, et al. Effects of clarithromycin on inflammatory pa-
rameters and clinical conditions in children with bronchiectasis. J Clin Pharm
Ther 2006;31:4955.
44. Noone PG, Leigh MW, Sannuti A, et al. Primary ciliary dyskinesiadiagnostic and
phenotypic features. Am J Respir Crit Care Med 2004;169:45967.
45. Rosenfeld M, Gibson RL, McNamara S, et al. Early pulmonary infection, inflam-
mation, and clinical outcomes in infants with cystic fibrosis. Pediatr Pulmonol
2001;32:35666.
Bronchiectasis in Children 169
46. Barker AJ, Couch L, Fiel SB, et al. Tobramycin solution for inhalation reduces
sputum Pseudomonas aeruginosa density in bronchiectasis. Am J Respir Crit
Care Med 2000;162:4815.
47. Bush A, Payne D, Pike S, et al. Mucus properties in children with primary ciliary
dyskinesia: comparison with cystic fibrosis. Chest 2006;129:11823.
48. Elkins MR, Robinson M, Rose BR, et al. A controlled trial of long-term inhaled
hypertonic saline in patients with cystic fibrosis. N Engl J Med 2006;354:
22940.
49. Eng PA, Morton J, Douglass JA, et al. Short-term efficacy of ultrasonically nebu-
lized hypertonic saline in cystic fibrosis. Pediatr Pulmonol 1996;21:7783.
50. Delvaux M, Henket M, Lau L, et al. Nebulised salbutamol administered during
sputum induction improves bronchoprotection in patients with asthma. Thorax
2004;59:1115.
51. Daviskas E, Anderson SD, Eberl S, et al. Effect of increasing doses of mannitol on
mucus clearance in patients with bronchiectasis. Eur Respir J 2008;31:76572.
52. Daviskas E, Anderson SD, Gomes K, et al. Inhaled mannitol for the treatment of
mucociliary dysfunction in patients with bronchiectasis: effect on lung function,
health status and sputum. Respirology 2005;10:4656.
53. Jaques A, Daviskas E, Turton JA, et al. Inhaled mannitol improves lung function in
cystic fibrosis. Chest 2008;133:138896.
54. Wills PJ, Greenstone M. Inhaled hyperosmolar agents for bronchiectasis.
Cochrane Database Syst Rev 2006;(2):CD002996.
55. Fuchs HJ, Borowitz DS, Christiansen DH, et al. Pulmozyme Study Group. Effect of
aerosolized recombinant human DNase on exacerbations of respiratory symp-
toms and on pulmonary function in patients with cystic fibrosis. N Engl J Med
1994;331:63742.
56. Furuya MEY, Lezana-Fernandez JL, Vargas MH, et al. Efficacy of human re-
combinant DNase in pediatric patients with cystic fibrosis. Arch Med Res
2001;32:304.
57. Laube BL, Auci RM, Shields DE, et al. Effect of rhDNase on airflow obstruction
and mucociliary clearance in cystic fibrosis. Am J Respir Crit Care Med 1996;
153:75260.
58. Quan JM, Tiddens HAWM, Sy JP, et al. A two-year randomized placebo-con-
trolled trial of dornase alfa in young patients with cystic fibrosis with mild lung
function abnormalities. J Pediatr 2001;139:81320.
59. Ranasinha C, Assoufi B, Shak S, et al. Efficacy and safety of short-term adminis-
tration of aerosolised recombinant human DNase I in adults with stable stage
cystic fibrosis. Lancet 1993;342:199202.
60. Shah PL, Scott SF, Knight RA, et al. In vivo effects of recombinant human DNase I
on sputum in patients with cystic fibrosis. Thorax 1996;51:11925.
61. ODonnell AE, Barker AF, Ilowite JS, et al. Treatment of idiopathic bronchiectasis
with aerosolized recombinant human DNase I. rhDNase Study Group. Chest
1998;113:132934.
62. Wills PJ, Wodehouse T, Corkery K, et al. Short-term recombinant human DNase in
bronchiectasis. Effect on clinical state and in vitro sputum transportability. Am J
Respir Crit Care Med 1996;154:4137.
63. Ratjen F, Wonne R, Posselt HG, et al. A double-blind placebo controlled trial with
oral ambroxol and N-acetylcysteine for mucolytic treatment in cystic fibrosis. Eur
J Pediatr 1985;144:3748.
Redding 170
64. Stafanger G, Garne S, Howitz P, et al. The clinical effect and the effect on the
ciliary motility of oral N-acetylcysteine in patients with cystic fibrosis and primary
ciliary dyskinesia. Eur Respir J 1988;1:1617.
65. Jones AP, Rowe BH. Bronchopulmonary hygiene physicial therapy for chronic ob-
structive pulmonary disease and bronchiectasis. Cochrane Database Syst Rev
2000;(2):CD000045.
66. Elkins MR, Jones A, Van der Schans C. Positive expiratory pressure physiother-
apy for airway clearance in people with cystic fibrosis. Cochrane Database
Syst Rev 2006;(2):CD003147.
67. Main E, Prasad A, Schans C. Conventional chest physiotherapy compared to
other airway clearance techniques for cystic fibrosis. Cochrane Database Syst
Rev 2005;(1):CD002011.
68. McCool FD, Rosen MJ. Nonpharmacologic airway clearance therapies. Chest
2006;129:250S9S.
69. Auerbach HS, Williams M, Kirkpatrick JA, et al. Alternate-day prednisone reduces
morbidity and improves pulmonary function in cystic fibrosis. Lancet 1985;2:
6868.
70. Eigen H, Rosenstein BJ, FitzSimmons S, et al. A multicenter study of alternate-
day prednisone therapy in patients with cystic fibrosis. Cystic Fibrosis Foundation
Prednisone Trial Group. J Pediatr 1995;126:51523.
71. Greally P, Hussain MJ, Vergani D, et al. Interleukin-1a, soluble interleukin-2 recep-
tor, and IgG concentrations in cystic fibrosis treated with prednisolone. Arch Dis
Child 1994;71:359.
72. Dezateux C, Walters S, Balfour-Lynn I. Inhaled corticosteroids for cystic fibrosis.
Cochrane Database Syst Rev 2000;(2):CD001915.
73. Konstan MW, Byard PJ, Hoppel CL, et al. Effect of high-dose ibuprofen in patients
with cystic fibrosis. N Engl J Med 1995;332:84854.
74. Sordelli DO, Macri CN, Maillie AJ, et al. A preliminary study on the effect of anti-
imflammatory treatment in cystic fibrosis patients with Pseudomonas aeruginosa
lung infection. Int J Immunopathol Pharmacol 1994;7:10917.
75. Konstan MW, Hoppel CL, Chai B, et al. Ibuprofen in children with cystic fibrosis:
pharmacokinetics and adverse effects. J Pediatr 1991;118:95664.
76. Kapur N, Chang AB. Oral non steroid anti-inflammatories for children and adults
with bronchiectasis. Cochrane Database Syst Rev 2007;(4):CD006427.
77. Franco F, Sheikh A, Greenstone M. Short acting beta-2 agonists for bronchiecta-
sis. Cochrane Database Syst Rev 2003;(3):CD003572.
78. Halfhide C, Evans HJ, Couriel J. Inhaled bronchodilators for cystic fibrosis.
Cochrane Database Syst Rev 2005;(4):CD003428.
79. Chang CC, Morris PS, Chang AB. Influenza vaccine for children and adults with
bronchiectasis. Cochrane Database Syst Rev 2007;(3):CD006218.
80. Chang CC, Singleton RJ, Morris PS, et al. Pneumococcal vaccines for children and
adults with bronchiectasis. Cochrane Database Syst Rev 2007;(2):CD006316.
81. Corless JA, Warburton CJ. Leukotriene receptor antagonists for non-cystic
fibrosis bronchiectasis. Cochrane Database Syst Rev 2000;(4):CD002174.
82. Corless JA, Warburton CJ. Surgery versus non-surgical treatment for bronchiec-
tasis. Cochrane Database Syst Rev 2000;(4):CD002180.
Bronchiectasis in Children 171
Aspi rati on Lung
Di sease
Fernando M. de Benedictis, MD
a,
*,Virgilio P. Carnielli, MD
b
,
Diletta de Benedictis, MD
c
The term aspiration lung disease describes several clinical syndromes. At one end of
the spectrum is massive aspiration, usually of gastric contents, that causes acute
symptoms and, occasionally, respiratory failure, whereas at the other end of the spec-
trumis chronic lung aspiration (CLA), which is repeated passage of food, gastric reflux,
or saliva into the subglottic airways that causes chronic or recurrent respiratory
symptoms.
13
CLA has myriad causes and related factors. Clinical findings mainly depend on the
amount and nature of the aspirated material, the frequency of aspiration, and the host
response. Over the past 2 decades, significant advances have been made in under-
standing the mechanisms underlying dysphagia, gastroesophageal function, and air-
way protective reflexes and newdiagnostic techniques have been introduced. Despite
this, characterizing the presence or absence of aspiration, and under what circum-
stances a child might be aspirating what, is extremely challenging, and many children
are still not adequately diagnosed or treated for aspiration until permanent lung
damage has occurred.
ACUTE LUNG ASPIRATION
Disease Mechanisms
Acute lung aspiration is essentially lung injury caused by inhalation of gastric contents.
In 1946, Mendelson
4
described patients who aspirated when receiving general anes-
thesia and first proved that acid is toxic to the respiratory tract. Further studies in hu-
mans and animal models showed that aspiration of acidic contents (pH <2.5) into the
a
Division of Pediatric Medicine, Department of Pediatrics, Salesi Childrens University Hospital,
11 via Corridoni, 1-60123, Ancona, Italy
b
Division of Neonatology, Department of Neonatal Medicine, Salesi Childrens University
Hospital,11 via Corridoni, 1-60123, Ancona, Italy
c
Department of Pediatrics, Postgraduate School of Pediatrics, S. Maria della Misericordia
Hospital, University of Perugia, S. Andrea delle Fratte, 1-06156, Perugia, Italy
* Corresponding author.
E-mail address: debenedictis@ao-salesi.marche.it (F.M. de Benedictis).
KEYWORDS
Aspiration
Gastroesophageal reflux
Lung disease
Children
Pediatr Clin N Am 56 (2009) 173190
doi:10.1016/j.pcl.2008.10.013 pediatric.theclinics.com
0031-3955/08/$ see front matter 2009 Elsevier Inc. All rights reserved.
lungs causes mucosal desquamation, damage to alveolar lining cell and capillaries,
and acute neutrophil inflammation. Impaired respiratory tract defenses predispose
to secondary pulmonary infection, with the risk increasing with prolonged hospitaliza-
tion, enteral tube feeding, endotracheal intubation, and use of antacid drugs.
Assessment and Diagnosis
The diagnosis of acute aspiration is mainly clinical and usually involves witnessed in-
halation of vomit or tracheal suctioning of gastric contents. Even in the absence of
such events, however, a high suspicion index should be maintained when clinical
and radiographic findings are compatible with aspiration. Early bronchoscopy may
help to define the type of aspiration (ie, liquid versus particulate material) and improve
clinical assessment.
5
Clinical signs of acute aspiration include coughing, wheezing, chest discomfort, and
fever. More dramatically, cyanosis, pulmonary edema, and rapid progression to
severe respiratory distress syndrome may occur in cases of massive aspiration.
Although high mortality was once reported with massive aspiration, recent studies es-
timated a mortality rate of 5% in children and no deaths when three or fewer lobes
were involved.
6
Management
Apart from immediate unblocking of airways in case of massive aspiration and general
supportive care measures, further aspiration must be prevented. The benefits of arti-
ficial airway and oral or nasogastric tube placement should be weighed with caution
against the increased risk for aspiration because of their effect on swallowing. Admin-
istering antacids or sucralfate to raise the stomach pH increases bacterial colonization
in the stomach but not in the respiratory tract, and thus does not increase the risk for
ventilator-associated pneumonia.
7
The use of corticosteroids is controversial, with
some studies proving efficacy, especially when given close to the time of massive as-
piration, and others the opposite;
8
given such uncertainty, their use is not generally
recommended. Finally, there is some evidence that bronchoalveolar lavage (BAL)
with normal saline and surfactant may have clinical value in treating severe aspiration
syndrome in children.
9
Should deterioration occur with some or all of these measures, infection ought to be
suspected. Although it does not usually play a primary role in aspiration of gastric con-
tents, the rate of superimposed infection is high. Antibiotics should be withheld unless
there are reasonably clear signs of infection. Antibiotic therapy should be selected on
the basis of aspiration pneumonia bacteriology, which mainly depends on the presence
or absence of preexisting disease, the patients age, and prior use of antibiotics.
10
CHRONIC LUNG ASPIRATION
Small-volume aspiration into the lungs is relatively common, even in healthy subjects
when normal airway protective mechanisms are impaired, bypassed, or over-
whelmed.
11
Whether intermittent or persistent, CLA may occur in some children
only coincidentally with other stressors, such as upper respiratory tract infection.
CLA may present with chronic cough, wheeze, noisy breathing, choking during feed-
ing, recurrent episodes of pneumoniaor bronchitis, andfailuretothrive.
12,13
Chronicas-
piration often results in progressive lungdisease, bronchiectasis, andrespiratory failure
and is a major cause of death in children with severe neurologic disorders.
14
There is no
goldstandard test for diagnosingCLA, anddeterminingwhether aspirationis asignif-
icant cause of respiratory disease remains a challenge in pediatric medicine.
de Benedictis et al 174
Disease Mechanisms
In subjects with CLA, more than one mechanism may be involved and separating out
mechanisms is often difficult. Pulmonary aspiration may occur as a result of swallow-
ing dysfunction, gastroesophageal reflux (GOR), or inability to protect the airway
adequately from oral secretions. Furthermore, a tracheoesophageal fistula should
always be considered and excluded.
15
Aspiration attributable to swallowing dysfunction
Normal swallowing, a complex process requiring coordinated voluntary and involun-
tary actions, involves the mouth, pharynx, larynx, and esophagus in different phases.
The maturation of oral and pharyngeal anatomy and the evolution of the suckling pro-
cess develop parallel to the development of the brain and the nervous system. Ana-
tomic abnormalities and intrinsic dysfunction in the effectiveness, duration, or timing
of any of these components can result in direct aspiration.
Although children with neurologic disease are at high risk for aspiration, the inability
to coordinate swallowing can be a problem in normal infants, especially those born
prematurely.
16
In such cases, cricopharyngeal incoordination is attributable to
delayed maturation of swallowing reflexes; it has been suggested that it appears
more frequently in young infants with bronchiolitis.
17
A recent retrospective study in
children with documented swallowing dysfunction showed that multisystem involve-
ment (ie, medical conditions affecting more than one organ system) was highly asso-
ciated with aspiration pneumonia.
18
Reflux aspiration
An association between GOR and respiratory symptoms is well documented,
19,20
but
a causal relation is difficult to determine in an individual child.
21,22
Possible mecha-
nisms involved in this relation are listed in Box 1. In a study evaluating the relation be-
tween aspiration and recurrent respiratory tract infections in children with neurologic
disability, Morton and colleagues
23
found that oral and pharyngeal motor problems
were the major cause of respiratory involvement and that GOR without a coexisting
swallowing dysfunction was less likely to cause respiratory tract infection. Despite
these findings emphasizing the role of swallowing dysfunction in children with neuro-
logic disability, patients with GOR have significantly reduced laryngopharyngeal
Box1
Mechanisms for the association of gastroesophageal reflux and respiratory disease
GOR causing respiratory disease
Aspiration
Direct effect: tracheitis, bronchitis, pneumonia, atelectasis
Indirect effect: inflammation predisposing to airway hyperreactivity
Reflex mechanism: esophagus-airway reflex
Respiratory disease causing GOR
Diaphragm flattening and changes in transthoracic pressure gradient
Decreased lower esophageal sphincter pressure attributable to medication (ie,
theophylline)
Additive effect of chest physiotherapy
Aspiration Lung Disease 175
sensitivity because of repeated exposure of mucosa to small amounts of acid; this
could potentially result in an increased risk for aspiration.
24
Salivary aspiration
Chronic saliva aspiration is the least commonly recognized form of aspiration and is
usually not diagnosed before development of significant lung injury.
3
The oral cavity
contains potentially pathogenic organisms that, when aspirated in sufficient quantity,
can cause recurrent pneumonia or pulmonary abscess.
10
Most neurologically im-
paired children who aspirate saliva do so because of severe swallowing incoordination
and reduced laryngopharyngeal sensitivity rather than excessive production of
saliva.
25
Assessment
As for any pediatric patient, clinical evaluation is the cornerstone of the general
assessment in children with suspected aspiration. A careful evaluation of the patients
history and physical findings should enable the clinician to proceed with appropriate
diagnostic studies in a rational staged fashion. Particular conditions that predispose
the child to aspirate should be considered in the initial assessment (Box 2). In any
case, because of the complex nature of chronic aspiration, a multidisciplinary
approach is mandatory.
Clinical assessment
When aspiration is suspected, the case history should focus on the timing of symptoms
in relation to feeding and position changes, choking, gagging, spitting or vomiting, ex-
cessive salivation, apnea, and bradycardia; coughing and wheezing should also be in-
vestigated in detail. Coughing and gagging may be minimal or absent in children with
a depressed cough reflex, however, as in neurologically impaired subjects (ie, silent
aspiration).
Dysmorphic features (ie, micrognathia, macroglossia), which may be associated
with structural airway problems, and anatomic abnormalities (ie, cleft palate) should
be carefully sought during the clinical examination. Observation of the child during
feeding is essential to detect excess drooling, difficulty with sucking, or swallowing
with or without associated coughing or choking and, occasionally, nasopharyngeal
reflux.
Imaging studies
Plain chest radiographs and high-resolution computed thomography (HRCT) are com-
monly used in the evaluation of children suspected of aspiration. Although not diag-
nostic tests for aspiration, they are useful indicators of lung injury and may also
document disease progression or resolution over time.
26,27
Chest radiograph
On radiographs, CLA typically presents as hyperaeration, peribronchial thickening,
subsegmental or segmental infiltrates, and atelectasis. Bronchiectasis may also be
seen. Basilar and superior segments of lower lobes, in addition to posterior upper
lobe segments, are most involved. Chest radiographs are not sufficiently sensitive
to detect the subtle changes that occur in early lung injury, however.
High-resolution CT
Chest HRCT is more sensitive in the detection of early airway and parenchymal
disease in pediatric patients. In a child with a suggestive history, the combination of
airway and parenchymal findings in a distribution pattern that is consistent with aspi-
ration can be interpreted as evidence of lung injury caused by CLA. Such findings as
de Benedictis et al 176
bronchial thickening, air trapping, bronchiectasis, ground-glass opacities, and centri-
lobular opacities (tree-in-bud), although not specific for aspiration, are common in
children who chronically aspirate and may indicate a diagnosis.
Diagnosis
By assessing oral motor skills, clinical evaluation of swallowing may provide important
information to the clinician but is insufficient to assess aspiration risk accurately.
28
Over
the years, newtechniques have been introduced and their role for supporting the diag-
nosis of lung aspiration has been better defined. The accuracy of some diagnostic
methods andcomparisonamongthemstill needtobeascertainedinchildren, however.
Box 2
Conditions predisposing to aspiration lung disease
Anatomic
Micrognathia
Macroglossia
Cleft palate
Laryngeal cleft
Tracheoesophageal fistula
Vascular rings
Functional
Achalasia (cricopharyngeal, esophageal)
GOR
Collagen vascular disease (scleroderma, dermatomyositis)
Tumors, masses, foreign body
Mechanical
Nasoenteric tube
Endotracheal tube
Tracheostomy
Neuromuscular
Depressed consciousness (eg, general anesthesia, drug intoxication, head trauma, seizures,
central nervous system infection)
Prematurity (immaturity of swallowing)
Cerebral palsy
Increased intracranial pressure
Vocal cord paralysis
Dysautonomia
Muscular dystrophy
Myasthenia gravis
Polyradiculoneuritis
Werding-Hoffmann disease
Aspiration Lung Disease 177
Aspiration attributable to swallowing dysfunction
Videofluoroscopic swallowstudy (VFSS) is considered the gold standard for assessing
the oral, pharyngeal, and esophageal phases of swallowing. Although a normal VFSS
cannot entirely rule out aspiration because it is episodic in nature, it visualizes an
extensive range of swallowing abnormalities (ie, premature spillage of the food bolus
before the swallow, delayed swallow reflex, postswallow residue, laryngeal penetra-
tion, aspiration into the trachea with or without cough clearance, impaired passage
into the esophagus, regurgitation of swallowed food).
29
When the accuracy of clinical
evaluation was compared with VFSS, a sensitivity of 92% and 33% in detecting aspi-
ration on a clinical basis was found for fluids and solids, respectively.
30
The inter- and
intraobserver reliability of VFSS for the different parameters of swallowing is generally
poor, except for detection of penetration or aspiration events.
31
The strengths and lim-
itations of VFSS, and of other techniques, are summarized in Table 1.
Fiberoptic endoscopic evaluation of swallowing (FEES) enables direct visualization
of the oral and pharyngeal phases but does not reveal events after pharyngeal con-
traction.
32
FEES is as sensitive as VFSS and has similar,
33
or even superior,
34
inter-
and intraobserver reliability rates in detecting laryngeal penetration or aspiration
events. Because FEES and VFSS provide different information, they should be consid-
ered complementary in the clinical assessment of a patient with suspect aspiration.
Indeed, both studies can optimally assess feeding procedures with different consis-
tencies and the effectiveness of implemented swallowing techniques.
As a test for CLA of various types, a quantitative index of lipid-laden alveolar
macrophages (LLAMs) in BAL samples was repeatedly calculated, but results were
conflicting. The index often yielded positive values in subjects with nonaspiration-
related acute or chronic lung diseases (ie, fat embolism, oil infusions, cystic fibrosis,
bronchiolitis obliterans) or in healthy people.
3544
Cutoffs ranged from 67 to 200,
and each institution was advised to determine its own LLAM index cutoff value.
45
A major limitation for using LLAM as a marker of CLA caused by swallowing dysfunc-
tion is that GOR was not consistently evaluated as a possible confounder in the var-
ious studies.
46
Table 2 illustrates the variability in assessments of the utility of
a LLAM index in the diagnosis of CLA.
Reflux aspiration
Monitoring of esophageal pH for 24 hours has long been considered the standard di-
agnostic tool for GOR. This method is unable to recognize superimposed acid events
that occur after a pH decrease but before pH normalization, however, which may con-
stitute up to 38%of acid reflux events.
47
In addition, it does not document the nonacid
reflux of all kinds of fluids from the stomach to the esophagus that can be aspirated
and cause lung disease.
48
It is therefore unlikely that simple detection of acid reflux
alone is adequate for the diagnostic evaluation of CLA.
Multichannel intraluminal impedance and pH monitoring (MII-pH) has been increas-
ingly studied for its ability to detect anterograde and retrograde passage of acid, non-
acid, and gaseous material. By measuring changes in electrical impedance at multiple
levels of the esophagus, the movement of a fluid or air bolus is detected; pH is mea-
sured simultaneously, thus differentiating between acidic and nonacidic material.
49
MII-pH studies found that children with GOR have a high proportion of nonacid reflux,
predominantly in postprandial periods.
47,48
Nonacid reflux detected by MII-pH highly
correlated with persistent respiratory symptoms in young children on antacid medica-
tions, and may therefore be an important predictor of respiratory disease.
50
MII-pH
also detects much more pharyngeal-level reflux than pH monitoring alone; indeed,
most of these events are gaseous refluxes with and without minor pH decreases.
51
de Benedictis et al 178
Table1
Summary of diagnostic tests of aspiration
Evaluation Benefits Limitations
Chest radiograph Inexpensive and widely
available
Insensitive to subtle
changes of lung injury
HRCT Sensitive in detecting lung injury
Assesses progression of lung
injury over time
Radiation exposure
Expensive
VFSS Evaluates all phases of
swallowing
Evaluates multiple consistencies
Limited evaluation
of anatomy
Radiation exposure
Intra- and interobserver
variability
Expensive
FEES Evaluates functional anatomy
Evaluates multiple consistencies
Assesses aspiration in children not
feeding orally
Can be performed at bedside
No radiation exposure
Blind to events after
pharyngeal contraction
Intra- and interobserver
variability
Invasive
Expensive
BAL Evaluates anatomy of upper and
lower airways
Sampling for multiple cytologic
and microbiologic tests
Poor reproducibility and
difficult interpretation
of LLAM index
Invasive
Expensive
Esophageal pH
monitoring
Detects acid reflux events
Normative data in children
Blind to most reflux events
Poor relation between
reflux and aspiration
Somewhat invasive
Esophageal impedance
monitoring
Detects acid and nonacid reflux
events
Detects proximal reflux events
Lack of normative data for
children
Somewhat invasive
Expensive and cumbersome
to interpret
Not widely available
Gastroesophageal
scintigraphy
Performed under physiologic
conditions
Low radiation exposure
Variable sensitivity
Does not differentiate
between direct and
reflux aspiration
Barium esophagram Useful in detecting anatomic
problems
May yield information on
esophageal motility
Low sensitivity
Evaluates one moment
in time
Radionuclide
salivagram
No need of food bolus challenge
Low radiation exposure
Unknown sensitivity
Evaluates one moment
in time
Abbreviation: LLAM, lipid-laden alveolar macrophages.
Modified from Boesch RP, Daines C, Willging JP, et al. Advances in the diagnosis and manage-
ment of chronic pulmonary aspiration in children. Eur Respir J 2006;28:850; with permission.
Aspiration Lung Disease 179
Table 2
Summary of evidence regarding lipid-laden alveolar macrophage index in children
Reference Comparison Groups Subjects (n) Age Mean (Range) LLAM Index Mean (Range)
Nussbaum et al
36
Chronic pulmonary disorders without GOR 41 7 years (30 days14 years) 8 (19%)
a
Chronic pulmonary disorders with GOR 74 6 years (23 days12 years) 63 (85%)
a
Colombo and Hallberg
37
Not suspected of food aspiration 23 4.3 years (1 month25 years) 21 (072)
Suspected of food aspiration 22 2.2 years (1 month12 years) 139 (86241)
Moran et al
38
Lactose assay negative 25 Newborns 121
Lactose assay positive 18 Newborns 204
Bauer and Lyrene
39
Not chronic pulmonary aspiration 87 2.8 years 44 (0170)
Chronic pulmonary aspiration 26 (2 weeks15 years) 104 (20233)
Knauer-Fischer and
Ratjen
40
Surgical controls 18 8.6 years (315 years) 60 (35106)
Pulmonary disease without aspiration 18 8.2 years (116 years) 119 (74178)
Ahrens et al
41
Surgical controls 20 5.3 years (18175 months) 37 (5188)
Recurrent pneumonia without GOR 14 3.4 years (10117 months) 29 (5127)
Chronic lung disease and GOR 32 3.4 years (621 months) 117 (10956)
Sacco et al
42
Respiratory symptoms, pH negative 9 4.6 years (16136 months) 12 (350)
Respiratory symptoms, pH positive 11 6.6 years (10145 months) 52 (5105)
Kazachkov et al
43
Healthy adult controls 8 26 4 years 1
b
Chronic respiratory symptoms 21 2.3 years (294 months) 7
b
CF, uninfected 24 3.5 years (1143 months) 19
b
Furuya et al
44
No respiratory symptoms, no suspicion
of aspiration
41 4.4 years (5168 months) 108 (5248)
Pulmonary disease without suspicion
of aspiration
30 5.1 years (1192 months) 187 (50291)
Pulmonary disease and suspicion of aspiration 41 1.6 years (1132 months) 233 (145305)
Abbreviation: CF, cystic fibrosis.
a
Number and percentage of patients who had LLAM in BAL fluid.
b
Different semiquantitative method was used to calculate the LLAM index.
d
e
B
e
n
e
d
i
c
t
i
s
e
t
a
l
1
8
0
Because of these characteristics, MII-pH has the potential to become the new gold
standard for identifying children at risk for reflux aspiration.
52
At present, the major lim-
itation of this method is lack of normative pediatric data.
Studies attempting to compare LLAM index values in children with chronic respira-
tory symptoms with and without documented GOR showed even wider variability than
studies for direct aspiration. As a confirmatory method for reflux aspiration, Moran and
colleagues
38
used a lactose assay in the trachea of intubated neonates who were re-
ceiving lactose-containing orogastric feeds. They found that the LLAM index differen-
tiates well between neonates with positive and negative assays. At an index threshold
of 100, sensitivity and specificity were 100% and 22%, respectively, whereas at
a threshold of 150, they were 73% and 84%, respectively. The relation between
LLAM index and GOR as determined by MII-pH has not been investigated, but data
would be useful, given the limitations of esophageal pH monitoring alone. Currently,
there is insufficient evidence to support the diagnosis of reflux aspiration using the
LLAM index, largely because of the difficulty in establishing a causal link between
GOR and lung aspiration.
3
Gastroesophageal scintigraphy (milk scan) is regarded as a physiologic test for
detecting reflux and aspiration. After ingestion of a meal mixed with technetium 99m
sulfur colloid, serial images are taken to detect tracer activity in the lung parenchyma.
Sensitivity is questionable, and it does not clearly differentiate between direct and re-
flux aspiration.
5355
One recent study showed that pulmonary aspiration as demon-
strated by overnight scintigraphy was common in children with refractory
respiratory symptoms and suggested that GOR might be the underlying cause; inter-
estingly, 76% of patients with abnormal scintigraphy had normal pH study results,
whereas half of the patients with an abnormal pH study had aspiration.
56
This study
confirms that a normal intraesophageal pH study does not rule out GOR, whereas
an abnormal pH study does not necessarily confirm aspiration.
A barium esophagram was also used to evaluate GOR or aspiration. This test is not
reliable because the brief observation time renders it relatively insensitive for both. The
esophagram is most useful for detecting anatomic anomalies, including vascular rings
and tracheoesophageal fistulae, and may yield qualitative information on esophageal
motility.
57
Salivary aspiration
In children who continue to have symptoms of aspiration despite cessation of oral
feeding and GOR treatment, an evaluation of salivary aspiration is warranted. In con-
trast, children with significant sialorrhea; choking on secretions; severe neurologic im-
pairment; laryngotracheoesophageal cleft; vocal cord paralysis; coloboma, heart
defects, atresia choanae, retardation of growth and development, genitourinary prob-
lems, and ear abnormalities (CHARGE) association; Moebius, West or Pfeiffer syn-
drome; or congenital high airway obstruction syndrome (CHAOS) should undergo
evaluation for salivary aspiration earlier in the diagnostic process because there is
a much higher likelihood of salivary aspiration with these conditions.
3
Radionuclide salivagrams are performed by placing a small quantity of radiotracer
into the mouth and recording serial images until the oropharynx is cleared of the radio-
tracer. Activity in the major airways and lung parenchyma indicates aspiration. In ret-
rospective studies, the prevalence of positive salivagrams in children suspected of
aspiration is reported to range from 26% to 73%,
5860
but, unfortunately, no confirma-
tory tests were performed. Although a radionuclide salivagram is considered the most
sensitive test for salivary aspiration, further evaluation regarding its accuracy is
needed.
Aspiration Lung Disease 181
FEES with sensory testing (ST) directly visualizes pooled laryngeal secretions, and
impending aspiration is determined by diminished laryngeal sensitivity. Laryngeal sen-
sitivity is quantified by applying graded bursts of air to the aryepiglottic fold and reg-
istering the threshold pressure that elicits the laryngeal reflex. As seen in adults,
pediatric patients with an increased laryngopharyngeal sensory threshold have a sig-
nificantly higher likelihood of laryngeal penetration and aspiration during a feeding
assessment.
61,62
Management
In general, current management decisions for children who aspirate have to optimize
oral nutrition and hydration and reduce the risk for aspiration to preserve pulmonary
integrity (Box 3; Table 3).
Aspiration attributable to swallowing dysfunction
Pediatric dysphagia is usually a complex disorder in which biologic (ie, structural ab-
normalities, neurologic or metabolic conditions) and behavioral aspects mutually inter-
act.
63
A multidisciplinary approach with a team of pediatricians, otolaryngologists,
neurologists, psychologists, gastroenterologists, pulmonologists, and surgeons is of-
ten necessary for management of this disorder.
For dysphagic subjects, an initial plan for feeding intervention can be started with
the help of a specialized nurse during the VFSS or FEES. Compensatory strategies,
such as positioning, chin tuck, and different consistency feeds, can be gradually
implemented. Although restricting oral water ingestion is anecdotally accepted as
a useful measure, no trials have adequately evaluated the pulmonary effects of this
measure in children with primary aspiration of thin fluids.
64
For children who are unable to ingest sufficient calories safely by mouth, percutane-
ous or surgical placement of a feeding gastrostomy or jejunostomy may be needed.
Despite normal clinical history and preoperative radiologic and pH studies, GOR
can become apparent in neurologically impaired children after gastrostomy tube
placement. The benefit of a routine antireflux procedure at the time of gastrostomy
tube placement in children with neurologic impairment is the subject of debate. In-
deed, such a procedure may prevent postoperative GOR and help to avoid the
need for a subsequent surgical procedure, but it is associated with high morbidity
and mortality. Although there is little evidence that morbidity or mortality increased
in patients without GOR who did not undergo preventive fundoplication, it is generally
accepted that neurologically impaired children with symptomatic GOR and swallow-
ing dysfunction should undergo an antireflux procedure at the time of feeding tube
placement.
65
Previous exclusion of GOR is therefore needed to establish optimal in-
tervention strategies.
66
Cricopharyngeal achalasia is a specific cause of CLA and
may be resolved successfully by cricopharyngeal myotomy.
67
Box 3
What do I do when a child with suspected aspiration presents?
1. Carefully evaluate for symptoms and signs of aspiration in addition to risk factors for
aspiration (see text and Boxes 1and 2). (grade: recommended with benefits, moderate;
quality of evidence: cohort studies)
2. Perform diagnostic tests for aspiration (type of test; see Tables 1and 2). (grade:
recommended with benefits, moderate; quality of evidence: variable depending on type of
tests)
3. Manage aspiration.
de Benedictis et al 182
Reflux aspiration
Dietary measures have been recommended for treatment of GOR and make good
sense. They include restricting fluids and providing texture-modified diets or thick-
ened feeds. In a randomized, placebo-controlled, crossover study, Wenzl and col-
leagues
68
showed that thickened feeding significantly decreased the frequency and
Table 3
Management of aspiration lung disease
Type of Intervention Recommendation
a
Grading of
Recommendation
Quality of Supporting
Evidence
Aspiration related to dysphagia
Compensatory
strategies
(eg, positioning,
chin tuck)
Probably
recommended:
trade-off
Moderate Case series
Restriction of
water
Not recommended:
uncertain trade-off
Extremely
low
Systematic review: no
data in children
Gastrostomy/
jejunostomy
Recommended:
benefits
Moderate Case series
Reflux aspiration
Dietary measures
(eg, restricting
fluids, thickened
feeds)
Probably
recommended:
trade-off
Moderate Case series and one
RCT: limited to the
effect on
regurgitation
Prokinetic agents
(domperidone,
erythromycin)
Not recommended:
uncertain
trade-off
Low RCTs: limited to the
effect on GOR
Acid-reducing
agents (H
2
antagonists, PPIs)
Probably
recommended:
trade-off
Moderate Case series: limited to
the effect on GOR
Fundoplication Recommended:
benefits
High Case series
Salivary aspiration
Anticholinergics Not recommended:
uncertain
trade-off
Low Case series and one
DBPCT: limited to
control of sialorrhea
Botulinum toxin Probably
recommended:
uncertain trade-off
Moderate case series and 1 RCT:
limited to control of
sialorrhea
Salivary gland duct
ligation
Not recommended:
uncertain trade-off
Low Case series: limited to
control of sialorrhea
Tracheostomy Not recommended:
uncertain trade-off
Low Case series
For many interventions, there is little high-quality evidence in children, and even less with respect
to magnitude of benefit on symptoms of aspiration.
Abbreviations: DBPCT, double-blind placebo-controlled trial; PPIs, proton pump inhibitors; RCT,
randomized controlled trial.
a
Recommendation involves a trade-off between benefits and harms and is based on diagnostic
tests showing evidence of type of aspiration present.
Aspiration Lung Disease 183
amount of regurgitation. This effect was caused by reduction in the number and height
of nonacid reflux, whereas the occurrence of acid reflux was not reduced. Unfortu-
nately, the effect of dietary measures on CLA lacks rigorous scientific backing.
Alginate-containing antacids form a raft that floats on the surface of the stomach
contents, which should reduce reflux. Recent assessment of the effect of such a mea-
sure on GOR questions its efficacy at preventing reflux.
69
Over theyears, different prokineticagents havebeenusedfor treatment of GOR. With
the withdrawal of cisapride andthe unacceptable side effects of metoclopramide,
70
the
common prokinetic agents include domperidone and erythromycin. Domperidone,
a peripheral D
2
-receptor antagonist that increases motility and gastric emptying,
showed little efficacy in the reduction of reflux symptoms in children
71
and has not
been evaluated for the treatment of reflux aspiration. Erythromycin increases gastroin-
testinal motility by acting directly on motilin (a hormone secreted into the gastrointesti-
nal tract duringtimes of fasting) receptors. Trials involving erythromycin at antimicrobial
or lowdoses havemainly focusedonit use inprematureneonates andinfants withfeed-
ing intolerance. Conflicting results in terms of efficacy were obtained.
72,73
Gastric acidsuppressants are widely usedfor treatment of GOR. Ranitidine, anantag-
onist of the H
2
receptors of gastric parietal cells, showed greater efficacy in patients with
mild GOR than in patients with severe GOR.
74
Proton pump inhibitors (ie, omeprazole,
lansoprazole) reduce gastric acid secretion and increase the intragastric pH; their supe-
riority over H
2
-receptor antagonists for treatment of GOR has been repeatedly demon-
strated.
75
Although the efficacy of gastric acid suppressant has been established for
esophagitis, neither safety nor efficacy has been clearly demonstrated for CLA.
76
For
many children with GOR-related CLA, medical therapy does not reduce respiratory tract
injury, which is not surprising, given the predominance of nonacid reflux in children.
Fundoplication is currently the antireflux procedure of choice in children with persis-
tent or severe respiratory symptoms and reflux aspiration. GOR is eliminated in almost
all patients, and respiratory symptoms improve in most.
7779
Care must be taken to
identify the presence of significant esophageal dysmotility before tightening the
esophagogastric junction because this can result in significant accumulation of oral
secretions in the esophagus and an increased risk for aspiration.
3
In children with neu-
rologic impairment, some researchers recommend jejunostomy tube placement as
a primary procedure or after fundoplication failure.
80,81
Although this procedure solves
feeding problems and may improve the quality of life, reflux is not completely
eliminated and aspiration may continue.
Salivary aspiration
In neurologically impaired children, oral anticholinergic agents are used to treat sialor-
rhea symptoms. Glycopyrrolate effectively reduced salivation,
82
but whether the re-
duction persists beyond a few weeks remains to be ascertained. No studies have
investigated the effects of anticholinergic drugs on reducing CLA.
The effectiveness of salivary gland injection of botulinum toxin in controlling sialor-
rhea in children with cerebral palsy has been evaluated with good results, but further
research is needed to understand the range of responses fully.
8385
No study has
addressed the effects on CLA-associated respiratory symptoms.
Other potential options for reducing oral secretions are bilateral submandibular and
parotid duct ligation or submandibular gland excision with parotid duct ligation.
Although both approaches were reported to be effective in children,
86,87
prospective
trials are needed.
Children with salivary aspiration often receive tracheostomy because of their under-
lying medical conditions and for pulmonary toilette. Some studies suggested that the
de Benedictis et al 184
presence of a tracheostomy tube and impaired swallowing were associated,
88,89
but
this aspect has not been sufficiently evaluated in children.
Laryngotracheal separation eliminates all continuity between the respiratory and
digestive tracts by disconnecting the upper trachea from the larynx.
90
Although this
procedure definitively eliminates aspiration, there are several adverse sequelae.
FUTURE DIRECTIONS
Because of the invasive nature of FEES, a promising new method of assessing vocal
cord motion using glottic ultrasound was developed to evaluate dysphagia.
91
It may
allowfor the noninvasive study of pharyngeal and glottic reflexes that favor airway pro-
tection in infants. Further development of this technique is awaited.
Gastric pepsin assays on BAL fluid were evaluated as a specific test of GOR-related
aspiration, with variable results.
9294
Pepsin assay in saliva or sputum may provide
a promising noninvasive method to test for the proximal reflux of gastric contents,
but the experience with this technique is limited.
95
At present, many questions still remain unanswered, such as howmuch aspiration is
normal at different ages, whether different types of aspiration have different outcomes,
and how aspiration during childhood might affect future lung function. More research
is needed to shed further light on this heterogeneous and challenging condition of
pediatric medicine.
ACKNOWLEDGMENT
The authors thank Consuelo Ramacogi for her help in preparing the manuscript.
REFERENCES
1. Colombo JL, Sammut PH. Aspiration syndromes. In: Taussig LM, Landau LI, ed-
itors. Pediatric respiratory medicine. St. Louis (MO): Mosby; 1999. p. 43543.
2. Marick PE. Aspiration pneumonitis and aspiration pneumonia. N Engl J Med
2001;344(9):66571.
3. Boesch RP, Daines C, Willging JP, et al. Advances in the diagnosis and man-
agement of chronic pulmonary aspiration in children. Eur Respir J 2006;
28(4):84661.
4. Mendelson CL. The aspiration of the stomach contents into the lungs during
obstetric anaesthesia. Am J Obstet Gynecol 1946;52:191205.
5. Campinos L, Duvall G, Couturier M, et al. The value of early fibreoptic bron-
choscopy after aspiration of gastric contents. Br J Anaesth 1983;55(11):
11035.
6. Hickling KG, Howard R. A retrospective survey of treatment and mortality in
aspiration pneumonia. Intensive Care Med 1988;14(6):61722.
7. Bonten MJ, Gaillard CA, van der Geest S, et al. The role of intragastric acidity and
stress ulcus prophylaxis on colonization and infection in mechanically ventilated
ICU patients. A stratified, randomized, double-blind study of sucralfate versus
antacids. Am J Respir Crit Care Med 1995;152(6):182534.
8. de Benedictis FM, Canny GJ, Levison H. The role of corticosteroids in respiratory
diseases of children. Pediatr Pulmonol 1996;22(1):4457.
9. Marraro GA, Luchetti M, Spada C, et al. Selective medicated (normal saline and
exogenous surfactant) bronchoalveolar lavage in severe aspiration syndrome in
children. Pediatr Crit Care Med 2007;8(5):47681.
Aspiration Lung Disease 185
10. Brook I, Finegold SM. Bacteriology of aspiration pneumonia in children. Pediat-
rics 1980;65(6):111520.
11. Gleeson K, Eggli DF, Maxwell SL. Quantitative aspiration during sleep in normal
subjects. Chest 1997;111(5):126672.
12. Owayed AF, Campbell DM, Wang EEL. Underlying causes of recurrent pneumo-
nia in children. Arch Pediatr Adolesc Med 2000;154(2):1904.
13. Lodha R, Puranik M, Natchu UCM, et al. Recurrent pneumonia in children: clinical
profile and underlying causes. Acta Paediatr 2002;91(11):11703.
14. Gillies JD, Seshia SS. Vegetative state following coma in childhood: evolution and
outcome. Dev Med Child Neurol 1980;22(5):6428.
15. Goyal A, Jones MO, Couriel JM, et al. Oesophageal atresia and tracheo-oeso-
phageal fistula. Arch Dis Child Fetal Neonatal Ed 2006;91(5):3814.
16. Sheikh S, Allen E, Shell R, et al. Chronic aspiration without gastroesophageal re-
flux as a cause of chronic respiratory symptoms in neurologically normal infants.
Chest 2001;120(4):11905.
17. Khoshoo V, Edell D. Previously healthy infants may have increased risk of
aspiration during syncytial viral bronchiolitis. Pediatrics 1999;104(6):
138990.
18. Weir K, McMahon S, Barry L, et al. Oropharyngeal aspiration and pneumonia in
children. Pediatr Pulmonol 2007;42(11):102431.
19. Chen PH, Chang MH, Hsu SC. Gastroesophageal reflux in children with chronic
recurrent bronchopulmonary infection. J Pediatr Gastroenterol Nutr 1991;13(1):
1622.
20. Orenstein SR. An overview of reflux-associated disorders in infants: apnea, lar-
yngospasm, and aspiration. Am J Med 2001;111(Suppl 3):60S3S.
21. Harding SM. Recent clinical investigations examining the association of
asthma and gastroesophageal reflux. Am J Med 2003;115(Suppl 3A):
39S44S.
22. Weinberger M. Gastroesophageal reflux disease is not a significant cause of lung
disease in children. Pediatr Pulmonol Suppl 2004;26:197200.
23. Morton RE, Wheatley R, Minford J. Respiratory tract infections due to direct and
reflux aspiration in children with severe neurodisability. Dev Med Child Neurol
1999;41(5):32934.
24. Phua SY, McGarvey LP, Ngu MC, et al. Patients with gastro-oesophageal reflux
disease and cough have impaired laryngopharyngeal mechanosensitivity. Thorax
2005;60(6):48891.
25. Hussein I, Kershaw AE, Tahmassebi JF, et al. The management of drooling in chil-
dren and patients with mental and physical disabilities: a literature review. Int
J Paediatr Dent 1998;8(1):311.
26. Rossi UG, Owens CM. The radiology of chronic lung disease in children. Arch Dis
Child 2005;90(6):6017.
27. Kuhn JP, Brody AS. High-resolution CT of pediatric lung disease. Radiol Clin
North Am 2002;40(1):89110.
28. McCullough GH, Wertz RT, Rosenbek JC, et al. Inter- and intrajudge reliability
of a clinical examination of swallowing on adults. Dysphagia 2000;15(2):
5862.
29. Martin-Harris B, Logemann JA, McMahon S, et al. Clinical utility of the modified
barium swallow. Dysphagia 2000;15(3):13641.
30. DeMatteo C, Matovich D, Hjartarson A. Comparison of clinical and videofluoro-
scopic evaluation of children with feeding and swallowing difficulties. Dev Med
Child Neurol 2005;47(3):14957.
de Benedictis et al 186
31. Stoeckli SJ, Huisman TA, Seifert B, et al. Interrater reliability of videofluoroscopic
swallow evaluation. Dysphagia 2003;18(1):537.
32. Leder SB, Karas DE. Fiberoptic endoscopic evaluation of swallowing in the pedi-
atric population. Laryngoscope 2000;110(7):11326.
33. Colodny N. Interjudge and intrajudge reliabilities in fiberoptic endoscopic evalu-
ation of swallowing (FEES) using the penetration-aspiration scale: a replication
study. Dysphagia 2002;17(4):30815.
34. Kelly AM, Drinnan MJ, Leslie P. Assessing penetration and aspiration: how do vid-
eofluoroscopy and fiberoptic endoscopic evaluation of swallow compare? Laryn-
goscope 2007;117(10):17237.
35. Corwin RW, Irwin RS. The lipid-laden alveolar macrophage as a marker of aspira-
tion in parenchymal lung disease. Am Rev Respir Dis 1985;132(3):57681.
36. Nussbaum E, Maggi JC, Mathis R, et al. Association of lipid-laden macrophages
and gastroesophageal reflux in children. J Pediatr 1987;110(2):1904.
37. Colombo JL, Hallberg TK. Recurrent aspiration in children: lipid-laden alveolar
macrophage quantitation. Pediatr Pulmonol 1987;3(2):869.
38. Moran JR, Block SM, Lyerly AD, et al. Lipid-laden alveolar macrophage and lac-
tose assay as markers of aspiration in neonates with lung disease. J Pediatr 1988;
112(4):6435.
39. Bauer ML, Lyrene RK. Chronic aspiration in children: evaluation of the lipid-laden
macrophage index. Pediatr Pulmonol 1999;28(2):94100.
40. Knauer-Fischer S, Ratjen F. Lipid-laden macrophages in bronchoalveolar lavage
fluid as a marker for pulmonary aspiration. Pediatr Pulmonol 1999;27(6):41922.
41. Ahrens P, Noll C, Kitz R, et al. Lipid-laden alveolar macrophages (LLAM): a useful
marker of silent aspiration in children. Pediatr Pulmonol 1999;28(2):838.
42. Sacco O, Fregonese B, Silvestri M, et al. Bronchoalveolar lavage and esophageal
pH monitoring data in children with difficult to treat respiratory symptoms.
Pediatr Pulmonol 2000;30(4):3139.
43. Kazachkov MY, Muhlebach MS, Livasy CA, et al. Lipid-laden macrophage index
and inflammation in bronchoalveolar lavage fluids in children. Eur Respir J 2001;
18(5):7905.
44. Furuya ME, Moreno-Cordova V, Ramirez-Figueroa JL, et al. Cutoff value of lipid
laden alveolar macrophages for diagnosing aspiration in infants and children.
Pediatr Pulmunol 2007;42(5):4527.
45. Colombo JL, Hallberg TK. Pulmonary aspiration and lipid-laden macrophages: in
search of gold (standards). Pediatr Pulmonol 1999;28(2):7882.
46. Ding Y, Simpson PM, Schellhase DE, et al. Limited reliability of lipid-laden mac-
rophage index restricts its use as a test for pulmonary aspiration: comparison
with a simple semiquantitative assay. Pediatr Dev Pathol 2002;5(6):5518.
47. Shay SS, Johnson LF, Richter JE. Acid reflux: a review, emphasizing detection by
impedance, manometry, and scintigraphy, and the impact on acid clearing path-
ophysiology as well as interpreting the pH record. Dig Dis Sci 2003;48(1):19.
48. Wenzl TG, Moroder C, Trachterna M, et al. Esophageal pH monitoring and imped-
ance measurement: a comparison of two diagnostic tests for gastroesophageal
reflux. J Pediatr Gastroenterol Nutr 2002;34(5):51923.
49. Condino AA, Sondheimer J, Pan Z, et al. Evaluation of infantile acid and nonacid
gastroesophageal reflux using combined pH monitoring and impedance mea-
surement. J Pediatr Gastroenterol Nutr 2006;42(1):1621.
50. Rosen R, Nurko S. The importance of multichannel intraluminal impedance in the
evaluation of children with persistent respiratory symptoms. Am J Gastroenterol
2004;99(12):24528.
Aspiration Lung Disease 187
51. Kawamura O, Aslam M, Rittmann T, et al. Physical and pH properties of gastro-
esophagopharyngeal refluxate: a 24-hour simultaneous ambulatory impedance
and pH monitoring study. Am J Gastroenterol 2004;99(6):100010.
52. Tutuian R, Castell DO. Use of multichannel intraluminal impedance to document
proximal esophageal and pharyngeal nonacidic reflux episodes. Am J Med 2003;
115(Suppl 3A):119S23S.
53. McVeagh P, Howman-Giles R, Kemp A. Pulmonary aspiration studied by radionu-
clide milk scanning and barium swallow roentgenography. Am J Dis Child 1987;
141(8):91721.
54. Fawcett HD, Hayden CK, Adams JC, et al. How useful is gastroesophageal reflux
scintigraphy in suspected childhood aspiration? Pediatr Radiol 1988;18(4):
3113.
55. Baikie G, South MJ, Reddihough DS, et al. Agreement of aspiration tests using
barium videofluoroscopy, salivagram, and milk scan in children with cerebral
palsy. Dev Med Child Neurol 2005;47(2):8693.
56. Ravelli AM, Panarotto MB, Verdoni L, et al. Pulmonary aspiration shown by scin-
tigraphy in gastroesophageal reflux-related respiratory disease. Chest 2006;
130(5):15206.
57. Meyers WF, Roberts CC, Jhonson DG, et al. Value of tests for evaluation of gas-
troesophageal reflux in children. J Pediatr Surg 1985;20(5):51520.
58. Bar-Sever Z, Connolly LP, Treves ST. The radionuclide salivagram in children with
pulmonary disease and a high risk of aspiration. Pediatr Radiol 1995;25(Suppl 1):
S1803.
59. Levin K, Colon A, DiPalma J, et al. Using the radionuclide salivagramto detect pul-
monary aspiration and esophageal dysmotility. Clin Nucl Med 1993;18(2):1104.
60. Cook SP, Lawless S, Mandell GA, et al. Theuse of thesalivagramin theevaluation of
severe and chronic aspiration. Int J Pediatr Otorhinolaryngol 1997;41(3):35361.
61. Thompson DM. Laryngopharyngeal sensory testing and assessment of airway
protection in pediatric patients. Am J Med 2003;115(Suppl 3A):166S8S.
62. Perlman PW, Cohen MA, Setzen M, et al. The risk of aspiration of pureed food as
determined by flexible endoscopic evaluation of swallowing with sensory testing.
Otolaryngol Head Neck Surg 2004;130(1):803.
63. Burklow KA, Phelps AN, Schultz JR, et al. Classifying complex pediatric feeding
disorders. J Pediatr Gastroenterol Nutr 1998;27(2):1437.
64. Weir K, McMahon S, Chang AB. Restriction of oral intake of water for aspi-
ration lung disease in children. Cochrane Database Syst Rev 2005;4:
CD005303.
65. Burd RS, Price MR, Whalen TV. The role of protective antireflux procedures in
neurologically impaired children: a decision analysis. J Pediatr Surg 2002;
37(3):5006.
66. Del Buono R, Wenzl TG, Rawat D, et al. Acid and nonacid gastro-oesophagel re-
flux in neurologically impaired children: investigation with the multiple intraluminal
impedance procedure. J Pediatr Gastroenterol Nutr 2006;43(3):3315.
67. Muraji T, Takamizawa S, Satoh S, et al. Congenital cricopharyngeal achalasia: di-
agnosis and surgical management. J Pediatr Surg 2002;37(5):E12.
68. Wenzl TG, Schneider S, Scheele F, et al. Effects of thickened feeding on gastro-
esophageal reflux in infants: a placebo-controlled crossover study using intralu-
minal impedance. Pediatrics 2003;111(4):e3559.
69. Del Buono R, Wenzel TG, Ball G, et al. Effect of Gaviscon Infant on gastro-oeso-
phageal reflux in infants assessed by combined intraluminal impedance/pH. Arch
Dis Child 2005;90(5):4603.
de Benedictis et al 188
70. Chicella MF, Batres LA, Heesters MS, et al. Prokinetic drug therapy in children:
a review of current options. Ann Pharmacother 2005;39(4):70611.
71. Pritchard DS, Baber N, Stephenson T. Should domperidone be used for the treat-
ment of gastro-oesophageal reflux in children? Systematic review of randomized
controlled trials in children aged 1 month to 11 years old. Br J Clin Pharmacol
2005;59(6):7259.
72. Costalos C, Gounaris A, Varhalama E, et al. Erythromycin as a prokinetic agent in
preterm infants. J Pediatr Gastroenterol Nutr 2002;34(1):135.
73. Ng SC, Gomez JM, Rajaduri VS, et al. Establishing enteral feeding in preterm in-
fants with feeding intolerance: a randomized controlled study of low-dose eryth-
romycin. J Pediatr Gastroenterol Nutr 2003;37(5):5548.
74. Kelly DA. Do H2 receptor antagonists have a therapeutic role in childhood?
J Pediatr Gastroenterol Nutr 1994;19(3):2706.
75. Keady S. Update on drugs for gastro-oesophageal reflux disease. Arch Dis Child
Educ Pract Ed 2007;92(4):ep1148.
76. Hassal E. Decisions in diagnosing and managing chronic gastroesophageal re-
flux disease in children. J Pediatr 2005;146(Suppl 3):S312.
77. Mattioli G, Sacco O, Repetto P, et al. Necessity for surgery in children with gastro-
oesophageal reflux and supraoesophageal symptoms. Eur J Pediatr Surg 2004;
14(1):713.
78. Kawahara H, Okuyama H, Kubota A, et al. Can laparoscopic antireflux surgery
improve the quality of life in children with neurologic and neuromuscular handi-
caps? J Pediatr Surg 2004;39(12):17614.
79. Esposito C, Langer JC, Schaarschmidt K, et al. Laparoscopic antireflux proce-
dures in the management of gastroesophageal reflux following esophageal
atresia repair. J Pediatr Gastroenterol Nutr 2005;40(3):34951.
80. Wales PW, Diamond IR, Dutta S, et al. Fundoplication and gastrostomy versus
image-guided gastrojejunal tube for enteral feeding in neurologically impaired
children with gastroesophageal reflux. J Pediatr Surg 2002;37(3):40712.
81. Esposito C, Settimi A, Centonze A, et al. Laparoscopic-assisted jejunostomy: an
effective procedure for the treatment of neurologically impaired children with
feeding problems and gastroesophageal reflux. Surg Endosc 2005;19(4):5014.
82. Mier RJ, Bachrach SJ, Lakin RC, et al. Treatment of sialorrhea with glycopyrrolate:
a double-blind, dose-ranging study. Arch Pediatr Adolesc Med 2000;154(12):
12148.
83. Jongerius PH, van den Hoogen FJ, van Limbeek J, et al. Effect of botulinum toxin
in the treatment of drooling: a controlled clinical trial. Pediatrics 2004;114(3):
6207.
84. Hassin-Baer S, Scheuer E, Buchman AS, et al. Botulinum toxin injections for
children with excessive drooling. J Child Neurol 2005;20(2):1203.
85. Reid SM, Johnstone BR, Wetsbury C, et al. Randomized trial of botulinum toxin
injections into the salivary glands to reduce drooling in children with neurological
disorders. Dev Med Child Neurol 2008;50:1238.
86. Gerber ME, Gaugler MD, Myer CM 3rd, et al. Chronic aspiration in children. When
are bilateral submandibular gland excision and parotid duct ligation indicated?
Arch Otolaryngol Head Neck Surg 1996;122(12):136871.
87. Stern Y, Feinmesser R, Collins M, et al. Bilateral submandibular gland excision
with parotid duct ligation for treatment of sialorrhea in children: long-term results.
Arch Otolaryngol Head Neck Surg 2002;128(7):8013.
88. Elpern EH, Scott MG, Petro L, et al. Pulmonary aspiration in mechanically
ventilated patients with tracheostomies. Chest 1994;105(2):5636.
Aspiration Lung Disease 189
89. Abraham SS, Wolf EL. Swallowing physiology of toddlers with long-term
tracheostomies: a preliminary study. Dysphagia 2000;15(3):20612.
90. Takamizawa S, Tsugawa C, Nishijima E, et al. Laryngotracheal separation for in-
tractable aspiration pneumonia in neurologically impaired children: experience
with 11 cases. J Pediatr Surg 2003;38(6):9757.
91. Jadcherla SR, Gupta A, Stoner E, et al. Pharyngeal swallowing: defining pharyn-
geal and upper esophageal sphincter relationships in human neonates. J Pediatr
2007;151(6):597603.
92. Krishnan U, Mitchell JD, Messina I, et al. Assay of tracheal pepsin as a marker of
reflux aspiration. J Pediatr Gastroenterol Nutr 2002;35(3):3038.
93. Farrell S, McMaster C, Gibson D, et al. Pepsin in bronchoalveolar lavage fluid:
a specific and sensitive method of diagnosing gastro-oesophageal reflux-related
pulmonary aspiration. J Pediatr Surg 2006;41(2):28993.
94. Starosta V, Kitz R, Hartl D, et al. Bronchoalveolar pepsin, bile acids, oxidation,
and inflammation in children with gastroesophageal reflux disease. Chest 2007;
132(5):155764.
95. Potluri S, Friedenberg F, Parkman HP, et al. Comparison of a salivary/sputum
pepsin assay with 24-hour esophageal pH monitoring for detection of gastric re-
flux into the proximal esophagus, oropharynx, and lung. Dig Dis Sci 2003;48(9):
18137.
de Benedictis et al 190
Asthma i n Chi l dhood
Paul D. Robinson, MBChB, MRCPCH, FRACP
a,b,
*,
Peter Van Asperen, MBBS, MD, FRACP
a,b
Asthma is the most common chronic disease in childhood, with a prevalence of 10%
to 30%.
1
Many of the current recommendations for management of asthma in children
are based on studies in the adult asthmatic population, and there is a paucity of pub-
lished pediatric data. The available literature can be divided into two main age groups,
children younger than 12 years, and those aged 12 years and older (adults and ado-
lescents). Although adult and adolescent asthma are comparable, adult asthma is dif-
ferent from pediatric asthma (age < 12 years) in many important ways, and
consequently it may not be appropriate to extrapolate adult evidence to pediatric
management. This article reviews the available pediatric evidence and provides evi-
dence-based recommendations for management, based on recent American Thoracic
Society grading recommendations (Table 1).
2
A number of guidelines exist for asthma
management, but for consistency this article refers primarily to the National Asthma
Council guidelines, recently updated and published in Australia.
3
Management of
asthma is divided into the management of acute exacerbations (Tables 15) and inter-
val management (Tables 610).
DIAGNOSIS AND MISDIAGNOSIS
Wheeze and dyspnea, with or without cough, are the core symptoms of asthma, but
because these individual respiratory symptoms are common in children, asthma fre-
quently is misdiagnosed. Parents may misinterpret other respiratory sounds, such
as stridor and rattle, as wheeze. The relationship between cough and asthma also is
complex.
4
Isolated persistent cough is rarely asthma. A number of important differen-
tial diagnoses exist and should be considered (see Table 2)
3,5
if other features of
asthma are not present or if an inappropriate response to treatment is seen. A more
detailed discussion of each of these conditions is beyond the scope of this article.
a
Department of Respiratory Medicine, The Childrens Hospital at Westmead, Westmead,
Sydney, Australia
b
The Childrens Hospital at Westmead Clinical School, Discipline of Paediatrics and Child
Health, Faculty of Medicine, University of Sydney, Westmead, Sydney, Australia
* Corresponding author. Department of Respiratory Medicine, The Childrens Hospital at
Westmead, Locked Bag 4001, Westmead, NSW, 2145, Sydney, Australia.
E-mail address: paulr3@chw.edu.au (P.D. Robinson).
KEYWORDS
Asthma
Pediatrics
Management
Pediatr Clin N Am 56 (2009) 191226
doi:10.1016/j.pcl.2008.10.008 pediatric.theclinics.com
0031-3955/08/$ see front matter. Crown Copyright 2009 Published by Elsevier Inc. All rights reserved.
Table1
TheAmerican Thoracic Society grading recommendations
Grade of Recommendation Clarity of Risk/Benefit Quality of Supporting Evidence Implications
Strong recommendation:
High-quality evidence
Benefits clearly outweigh harms
and burdens or vice versa
Consistent evidence from
well-performed randomized,
controlled trials or exceptionally
strong evidence from unbiased
observational studies
Recommendation can apply to most
patients in most circumstances.
Further research is very unlikely to
change our confidence in the
estimate of effect.
Strong recommendation:
Moderate-quality evidence
Benefits clearly outweigh harms
and burdens or vice versa
Evidence from randomized, controlled
trials with important limitations
(inconsistent results, methodologic
flows, indirect or imprecise), or unusually
strong evidence from unbiased
observational studies
Recommendation can apply to most
patients in most circumstances.
Further research (if performed) is
likely to have an important impact
on our confidence in the estimate
of effect and may change the
estimate.
Strong recommendation:
Low-quality evidence
Benefits clearly outweigh harms
and burdens or vice versa
Evidence for at least one critical
outcome from observational
studies, from randomized,
controlled trials with serious
flaws, or indirect evidence
Recommendation may change when
higher-quality evidence becomes
available. Further research (if
performed) is likely to have an
important impact on our
confidence in the estimate of effect
and is likely to charge the estimate.
Strong recommendation:
Very low-quality evidence
(very rarely applicable)
Benefits clearly outweigh harms
and burdens or vice versa
Evidence for a least one of the
critical outcomes from
unsystematic clinical
observations or very
indirect evidence
Recommendation may change when
higher-quality evidence becomes
available; any estimate of effect, for
at least one critical outcome, is very
uncertain.
Weak recommendation:
High-quality evidence
Benefits closely balanced with
harms and burdens
Consistent evidence from
well-performed randomized,
controlled trials or exceptionally
strong evidence from unbiased
observational studies
The best action may differ depending
on circumstances, patient
characteristics, or societal values.
Further research is very unlikely to
change our confidence in the
estimate of effect.
R
o
b
i
n
s
o
n
&
V
a
n
A
s
p
e
r
e
n
1
9
2
Weak recommendation:
Moderate-quality evidence
Benefits closely balanced with
harms and burdens
Evidence from randomized,
controlled trials with important
limitations (inconsistent results.
methodologic flaws, indirect or
imprecise), or unusually strong
evidence from unbiased
observational studies
Alternative approaches are likely to
be better for some patients under
some circumstances. Further
research (if performed) is likely to
have an important impact on our
confidence in the estimate of effect
and may change the estimate.
Weak recommendation:
Low-quality evidence
Uncertainty in the estimates of benefits
harms, and burdens; benefits may be
closely balanced with harms and
burdens
Evidence for at least one critical
outcome from observations
studies, from randomized, controlled
trials with serious
flaws, or indirect evidence
Other alternatives may be equally
reasonable. Further research is very
likely to have an important impact
on our confidence in the estimate
of effect and is likely to change the
estimate.
Weak recommendation:
Very low quality evidence
Major uncertainty in the estimates
of benefits, harms, and burdens;
benefits may or may not be
balanced with harms and burdens
Evidence for at least one critical
outcome from unsystematic
clinical observations or very
indirect evidence
Other alternatives may be equally
reasonable. Any estimate of effect,
for at least one critical outcome, is
very uncertain.
From Schunemann HJ, Jaeschke R, Cook DJ, et al. An official ATS statement: grading the quality of evidence and strength of recommendations in ATS guidelines
and recommendations. Am J Respir Crit Care Med 2006;174:612; with permission. Copyright 2006, American Thoracic Society.
A
s
t
h
m
a
i
n
C
h
i
l
d
h
o
o
d
1
9
3
MANAGEMENT OF ACUTE ASTHMA
Assessing Severity
Assessment of severity (see Table 3) determines subsequent treatment. The evidence
and grading of the approach and options of managing acute asthma are summarized
in Table 4. Treatment of acute asthma is based on the underlying pathophysiology,
attempting to reverse bronchoconstriction, airway inflammation, and mucus
production.
Oxygen
If a patient is in acute distress, oxygen (to maintain oxygen saturations R 95%) and
a short-acting beta-2 agonist (SABA) should be given immediately. Subsequent salbu-
tamol administration may precipitate further desaturation via pulmonary vasodilatation
in areas of poorly ventilated lung. The value of initial oxygen saturation as a predictor of
Table 2
Important differential diagnoses in pediatric asthma
Condition Characteristics
Transient infant wheezing
(eg, recurrent bronchiolitis)
Onset in infancy
No associated atopy
Associated with maternal smoking
Cystic fibrosis Recurrent wheeze and failure to thrive
Primary ciliary dyskinesia Associated recurrent otitis media and sinusitis
Initial oxygen requirement postnatally
Situs inversus in 50%
Chronic bronchitis (viral or bacterial) Persistent moist cough in combination with wheeze
Purulent sputum suggests bacterial cause
Structural abnormality
(eg, tracheomalacia, bronchomalacia)
Onset usually from or shortly after birth
but occasionally later
Vocal cord dysfunction High-pitched inspiratory stridor and dyspnea
May be spontaneous or exercise induced
Blunting of inspiratory volume loop on spirometry
Inhaled foreign body Sudden onset
Differential air entry or wheeze on examination
Cardiac failure Associated with congenital or acquired heart
disease (eg, dilated cardiomyopathy after viral
infection)
Eosinophilic lung disorders including
allergic bronchopulmonary
aspergillosis
Skin prick test positivity to Aspergillus fumigatus
Raised serum IgE
Infiltrates on chest radiograph
Anxiety causing hyperventilation No wheeze audible
Spirometry at the time of symptoms may help
distinguish
Exertional dyspnea No respiratory symptoms other than with exercise
Exercise testing may distinguish
Milk aspiration/cough during feeds Symptomatic particularly with liquids
Associated with developmental delay
Data from National Asthma Council Australia. Asthma management handbook. 2006. Available at:
www.nationalasthma.org.au; and Weinberger M, Abu-Hasan M. Pseudo-asthma: when cough,
wheezing, and dyspnea are not asthma. Pediatrics 2007;120:85564.
Robinson & Van Asperen 194
subsequent hospitalization remains controversial.
6,7
Intensity of wheeze is a poor
predictor.
Beta-2 Agonists
Selective beta-2 agonists (salbutamol) have been the mainstay of acute asthma man-
agement sincethelate1970s. Frequency of administrationis determinedby theseverity
of the exacerbation (see Table 5). Continuous use of SABAhas been shown to be more
effective thanintermittent regimens insevereexacerbations
8
andtoreduce hospitaliza-
tion (RR, 0.64; 95% confidence interval [CI], 0.50.9), resulting in a modest improve-
ment in lung function at 2 to 3 hours. This benefit was not seen in mild or moderate
asthma. Only one of the eight relatively small randomized, control trials (RCTs) included
was pediatric
9
(n 5 70, age 218 years) and studied children who had moderate to
severe asthma. It found no difference in hospitalization rates or time spent in the emer-
gency department. Excluded from the analysis was an RCT in a more severe pediatric
asthma cohort (n 517) admittedto intensive care, which demonstrated a benefit in clin-
ical status and hospital stay.
10
Ameta-analysis of 25 RCTs, including 21 pediatric stud-
ies and more than 2000 children,
11
demonstrated that in acute asthma spacers were as
effective as nebulizers in limiting hospitalization rates and reducing the time spent in
emergency department (0.47 hours; 95% CI, 0.58 to 0.37). The role of spacers
in life-threatening asthma has yet to be investigated.
Table 3
Initial assessment of acute asthma
Symptom Mild Moderate
Severe or
Life-Threatening
a
Confused/drowsy No No Agitated or altered
consciousness
Oximetry on
presentation (SaO
2
)
94% 94%90% Less than 90%
Talks in Sentences Phrases Words or unable
to speak
Pulse rate Less than
100 beats/min
100200
beats /min
More than
200 beats/min
Central cyanosis Absent Absent Likely to be present
Wheeze intensity Variable Moderate
to loud
Often quiet
PEF
b
More than 60%
predicted or
personal best
40%60%
predicted
or personal
best
Less than 40%
predicted or
personal best or
unable to perform
FEV
1
More than 60%
predicted
40%60%
predicted
Less than 40%
predicted or
unable to perform
a
Any of these features indicates that the episode is severe. The absence of any feature does not
exclude a severe attack.
b
Children under 7 years old are unlikely to perform PEF or spirometry reliably during an acute
episode. These tests usually are not used in the assessment of acute asthma in children.
From National Asthma Council Australia. Asthma management handbook. 2006. Available at:
www.nationalasthma.org.au; with permission.
Asthma in Childhood 195
Table 4
Grading of evidence and recommendations for acute asthma management in children
Medication Recommendation
Grading of Recommendation
(Based on Evidence of Benefit)
Quality of Supporting
Evidence
SABA Recommended as first-line bronchodilator Strong High
Anticholinergics Multiple doses beneficial in severe asthma Strong Moderate
Corticosteroids
Inhaled May be an alternative in mild asthma. High dose
required if given.
Strong Moderate
Oral Beneficial in acute asthma not responding to SABA Strong High
Intravenous salbutamol Beneficial in severe or life-threatening asthma Strong Moderate
Intravenous aminophylline Alternative to IV salbutamol in severe
or life-threatening asthma
Strong Moderate
Magnesium sulfate
Inhaled Unclear role in severe asthma Weak Moderate
Intravenous Beneficial in severe or life-threatening asthma Strong High
Heliox May have a role in medication delivery but insufficient
evidence to recommend currently
Weak Moderate
Noninvasive ventilation May have a role in life-threatening asthma to prevent
intubation
Weak Low
Leukotriene receptor antagonists May have a role in mild to moderate acute asthma but
further studies are required
Weak Low
Antibiotics No indication for routine use Weak Low
Education Recommended but little evidence for improved
outcome
Weak High
Physiotherapy May be of benefit in resolving stage of hypersecretory
asthma
Weak Low
Spacers Spacer delivery of inhaled medications is recommended
for all but life-threatening acute asthma
Strong High
R
o
b
i
n
s
o
n
&
V
a
n
A
s
p
e
r
e
n
1
9
6
Anticholinergic Agents
Anticholinergic agents (ipratropium bromide, atropine sulfate) produce a weaker bron-
chodilation response with a slower onset of action (3090 minutes versus 515 min-
utes)
12
but, by relieving cholinergic bronchomotor tone and secretions, have
a beneficial effect when added to beta-agonist therapy in acute asthma. Meta-analysis
of eight high-quality pediatric RCTs demonstrated that a single dose of an anticholin-
ergic agent was insufficient to reduce hospital admission rate for any grade of severity
(although in severe attacks persisting to 120 minutes, a benefit in lung function was
seen).
13
In severe exacerbations in school-age children, multiple doses reduced hos-
pital admission rates by 25%(number needed to treat [NNT], 7; 95%CI, 520) and ad-
ditional bronchodilator use by 19%. No benefit was seen for mild attacks. The
suggested benefit in moderate acute asthma may be skewed by the response in
the severe subset and is insufficient to allow recommendation. There is a paucity of
studies in children of preschool age.
The role of anticholinergics in wheezy children under the age of 2 years, excluding
those who have bronchiolitis and chronic lung disease of prematurity, remains ques-
tionable. Parental preference and improvement in some (eg, clinical scores at 24
hours, additional treatment) but not all outcomes (eg, respiratory rate, need for oxygen
supplementation, hospital stay), when given with or without beta-agonist, are not
sufficient to recommend the use of an anticholinergic agent in this population.
14
Corticosteroids
Although bronchoconstriction is best targeted with beta-2 agonists, the airway edema
and secretions that accompany an acute exacerbation respond to systemic cortico-
steroid therapy. Considerable research effort has concentrated on the best route of
administration, timing, and dose of corticosteroid. Corticosteroids are recommended
for asthma exacerbations that are incompletely responsive to inhaled beta-agonists.
Doubling the dose of inhaled corticosteroids (ICS) at the onset of an exacerbation is
ineffective in improving lung function and controlling symptoms (n 5 28, age 614
years).
15
A review of published pediatric studies concluded that ICS given at high
doses (eg, 1600 mg/d of budesonide) seem to have a modest benefit compared with
placebo but are inferior to oral corticosteroids (OCS) in preventing hospitalization in
more severe attacks.
16
The most commonly used OCS is prednisolone, often chosen
because of its palatability
17
rather than because of comparative OCS data. Only one
pediatric RCT has examined differing doses of prednisolone, in a mild to moderate se-
verity cohort, and found no difference between 0.5, 1.0, and 2.0 mg/kg/d.
18
Meta-
analysis of adult RCT data in severe asthma has shown no benefit from higher doses
of corticosteroids, although these trials primarily examined intravenous (IV) adminis-
tration.
19
At present, the recommended dose of oral prednisolone is 1 mg/kg every
12 to 24 hours (maximumdose, 50 mg) depending on progress.
20
The optimal duration
of treatment also is unclear. A single dose of OCS on admission has failed to show
consistent benefit.
21,22
A recent pediatric RCT comparing 3- and 5-day courses
demonstrated equivalent efficacy.
23
Currently a 3-day course is recommended,
lengthened to 5 days in more severe exacerbations.
20
Early administration of OCS, within the first hour of arrival, has been shown to
reduce admission rates in children (three RCTs; OR, 0.24; 95% CI, 0.110.53).
24
To
date, however, parent-initiated OCS has not been demonstrated to improve out-
comes, as evaluated by unscheduled medical visits,
25
but further trials are required
to establish firm recommendations. OCS in children are as effective as parenteral
dosing,
26
are more cost effective, and are more convenient but rely on the childs
Asthma in Childhood 197
Table 5
Initial management of children who have acute asthma
Treatment Mild Episode Moderate Episode Severe or Life-Threatening Episode
Hospital admission necessary Probably not required Probably required Yes
Consider intensive care
Supplementary oxygen Probably not required May be required. Monitor SaO
2
Required. Monitor SaO
2
. Arterial blood
gases may be required.
Salbutamol (100 mg per puff)
a
46 puffs (children < 6 years) or
812 puffs (children R6 years).
Review in 20 minutes
6 puffs (children < 6 years) or
12 puffs (children R 6 years)
If initial response is inadequate,
repeat at 20-minute intervals
for two further doses; then
give every 14 hours.
6 puffs (children < 6 years) or 12 puffs
(children R6 years) every 20 minutes
for three doses in first hour.
If episode is life threatening, use
continuous nebulized salbutamol.
If no response, bolus IV salbutamol
(15 mg/kg) over 10 minutes, then
1 mg/kg/min thereafter.
Ipratropium (20 mg per puff) Not necessary Optional 2 puffs (children < 6 years) or 4 puffs
(children R6 years) every 20 minutes
for three doses in first hour or use
nebulized ipratropium
Systemic corticosteroids Yes (consider) Oral prednisolone (1 mg/kg daily
for up to 3 days)
Oral prednisolone (1 mg/kg/dose) daily
for up to 5 days
Methylprednisolone IV (1 mg/kg) every
6 hours on day 1, every 12 hours on
day 2, then daily
R
o
b
i
n
s
o
n
&
V
a
n
A
s
p
e
r
e
n
1
9
8
Magnesium No No Magnesium sulfate 50% 0.1 mL/kg (50
mg/kg) IV over 20 minutes, then 0.06
mL/kg/h (30 mg/kg/h): target serum
1.52.5 mmol/L
Aminophylline No No Only in intensive care: loading dose:
10 mg/kg;
maintenance: 1.1 mg/kg/h if < 9 years
or 0.7 mg/kg/h if R 9 years
Chest radiograph Not necessary unless
focal signs present
Not necessary unless
focal signs present
Necessary if no response to initial therapy
or pneumothorax is suspected
Observations Observe for 20 minutes
after dose
Observe for 1 hour
after last dose
Arrange for admission to hospital
a
In children who have severe acute asthma that does not respond to initial treatment with inhaled SABA, bolus IV salbutamol (15 mg/kg) is effective and can avoid
the need for continuous IV salbutamol and ICU admission.
From National Asthma Council Australia. Asthma management handbook. 2006. Available at: www.nationalasthma.org.au; with permission.
A
s
t
h
m
a
i
n
C
h
i
l
d
h
o
o
d
1
9
9
Table 7
Assessment of asthma control
Parameters
Level of Control
Good Fair Poor
Daytime symptoms None < 3 days/wk R 3 days/wk
Night-time symptoms Not wakened % 1 night/wk > 1 night/wk
Physical activity Normal Normal Restricted
Exacerbations None Mild, infrequent Moderate, severe
frequent
Missed school/work
because of asthma
None None Any
Reliever use
a
None < 3 doses/wk R 3 doses/wk
b
FEV
1
b
FEV
1
/FVC Normal R 90% personal best < 90% personal best
b
PEF Normal R 90% personal best < 90% personal best
a
Does not include one dose per day for prevention of exercise-induced symptoms.
b
Applicable to adults and older children. Lung function parameters are not appropriate measures
of asthma control in younger children.
From National Asthma Council Australia. Asthma management handbook. 2006. Available at:
www.nationalasthma.org.au; with permission.
Table 6
Assessment of severity of interval asthma
Severity Level
Daytime
Symptoms
Between
Exacerbations
Night-Time
Symptoms
Between
Exacerbations Exacerbations PEF or FEV
1
a
PEF Variability
b
Infrequent
intermittent
None None Brief, mild
Occur <
every 46
weeks
> 80%
predicted
< 20%
Frequent
intermittent
None None > Two per
month
At least 80%
predicted
< 20%
Mild
persistent
More than
once per
week but
not every
day
More than
twice per
month but
not every
week
May affect
activity and
sleep
At least 80%
predicted
20%30%
Moderate
persistent
Daily More than
once per
week
At least twice
per week;
restrict
activity or
affect sleep
60%80%
predicted
> 30%
Severe
persistent
Continual Frequent Frequent;
restrict
activity
%60%
predicted
> 30%
An individuals asthma pattern (infrequent intermittent, frequent intermittent, mild persistent, or
severe persistent) is determined by the level in the table that corresponds to the most severe fea-
ture present. Other features associated with that pattern need not be present.
a
Predicted values are based on age, sex, and height.
b
Difference between morning and evening values.
From National Asthma Council Australia. Asthma management handbook. 2006. Available at:
www.nationalasthma.org.au; with permission.
Robinson & Van Asperen 200
tolerating and retaining the dose. IV corticosteroids should be used in patients who are
unlikely to tolerate OCS (ie, children experiencing severe exacerbation). Benefit is
seen by 4 to 6 hours.
24
A single dose of oral or intramuscular (IM) dexamethasone
(0.6 mg/kg to a maximum of 1518 mg) was comparable to a 5-day course of oral
prednisolone (2 mg/kg/d) in three pediatric RCTs (total n 5 324),
27,28,29
although sys-
temic side effects may be more common with IM long-acting corticosteroids.
17
OCS
also have been shown to reduce relapse rates,
24
although this meta-analysis included
only one pediatric RCT.
30
High-dose ICS regimens on discharge from hospital have
shown efficacy similar to OCS but are not as cost effective.
31
Intravenous Bronchodilators
First-line IV bronchodilator therapy in severe acute asthma not improving with inhaled
beta-agonist and OCS therapy remains controversial. Guidelines recommend IV sal-
butamol as the first-line agent; it is preferred because of its better safety profile, but
the lack of clear evidence has led to the continuing widespread use of aminophylline.
32
Intravenous salbutamol
IV salbutamol has been shown to improve clinical outcome in comparison with placebo
in individual pediatric RCTs both as an infusion
33
and as a bolus of 15 mg/kg.
34,35
Although an attempted meta-analysis of the adult and pediatric data failed to demon-
strate improvement,
36
the conclusions of this meta-analysis have been criticized.
37
Intravenous aminophylline
Meta-analysis of seven pediatric RCTs (n 5 380 patients, mean age 59 years) in
severe acute asthma demonstrated improvements in lung function and clinical symp-
toms with IV aminophylline infusion,
38
but the analysis is affected significantly by the
results of the largest RCT (n 5179), the only RCT to show benefit.
39
A recent pediatric
RCT (n 544) directly comparing aminophylline and salbutamol (an IV salbutamol bolus
of 15 mg/kg versus IV aminophylline infusion) demonstrated no difference in efficacy in
the first 2 hours of treatment
37
but found a 30% reduction in hospital stay in the am-
inophylline group. Repeat IV aminophylline boluses have demonstrated no additional
benefit over standard treatment (n 5 60, age 25 years).
40
Magnesium sulfate
Magnesium is a potential therapeutic agent in asthma because of its bronchodilating
effect on smooth muscle cells
41
and reduction of the neutrophilic burst associated
with inflammation.
42
In a meta-analysis of five pediatric RCTs (n 5182, age 118 years),
IVmagnesiumsulfate decreasedhospitalizations (OR, 0.29; 95%CI, 0.140.59; NNT, 4;
95%CI, 38) and improved pulmonary function and symptomscores, despite variation
in dosage (2575 mg/kg).
43
Another predominantly adult meta-analysis that included
two pediatric RCTs (n 578 subject age 118 years in a total of 665 subjects) confirmed
its safe and beneficial role in severe acute asthma.
44
Meta-analysis of trials of inhaled
magnesium sulfate, including two pediatric RCTs (n 5 102), demonstrated significant
improvements in lung function only in severe acute asthma and no difference in hospi-
talization.
45
The comparative benefit of bolus IV salbutamol and bolus IV magnesium
sulfate is yet to be established.
Other Therapies
Heliox (helium/oxygen mixture) has lower gas density and higher viscosity, decreasing
flow resistance and enhancing airway penetration. A meta-analysis including three
pediatric RCTs demonstrated a potential benefit for heliox as a stand-alone therapy
in severe acute asthma, but sample sizes were small.
46
In a recent pediatric RCT
Asthma in Childhood 201
Table 8
Table of grading of evidence and recommendations for interval asthma management in children
Medication Recommendation
Grading of Recommendation
(Based on Evidence of Benefit) Quality of Supporting Evidence
Cromones (sodium cromoglycate
and nedocromil sodium)
Alternative to inhaled corticosteroid
in frequent intermittent and mild
persistent asthma. May be
beneficial in exercise-induced
asthma.
Weak Moderate
Leukotriene receptor antagonists Beneficial as sole therapy in frequent
intermittent or mild persistent
asthma. May be beneficial in
exercise-induced asthma or
allergic rhinitis.
Strong High
Corticosteroids
Inhaled corticosteroids Recommended for persistent asthma Strong High
Oral corticosteroids Severe asthma not responsive to
maximal inhaled therapy
Weak Very weak
Long-acting beta-agonists Should be considered as an
add-on therapy
Weak Moderate
Steroid-weaning agents
Immunosuppressive agents No evidence of efficacy
in pediatric patients
Weak Very low
Intravenous immunoglobulin Limited role in pediatric asthma.
May be beneficial if co-existent
immunodeficiency
Weak Low
Omalizumab Role in asthma management is
not well defined in pediatrics.
Expensive
Weak Moderate
R
o
b
i
n
s
o
n
&
V
a
n
A
s
p
e
r
e
n
2
0
2
Allergen immunotherapy
(subcutaneous)
Potential benefit in children
suspected of having allergen-
triggered disease, when allergen
avoidance has been ineffective
or is not possible
Weak Strong
Macrolides Some adult data but no evidence
of efficacy in pediatric asthma
Weak Very low
Xanthines Alternative in mild persistent asthma
when inhaled corticosteroids
are not available
Weak Strong
Ketotifen Alternative in mild persistent
asthma when inhaled
corticosteroids are not available
Weak Moderate
Dietary manipulation Current evidence does not
support use in asthma
Weak Low
Complementary alternative
medicine
Current evidence does not support
use in asthma
Weak Low
Allergen avoidance Some patients may benefit, but
there is insufficient evidence
to recommend routinely
Weak High
Prevention strategies
Primary Current evidence does not support
the use of preventative strategies
in asthma
Weak High
Secondary Weak Moderate
Tertiary Weak High
Vaccination (influenza
and pneumococcus)
Weak Moderate
Education Recommended for all asthma patients Strong High
Psychotherapy May be beneficial in a subset
of patients
Weak Moderate
A
s
t
h
m
a
i
n
C
h
i
l
d
h
o
o
d
2
0
3
(n 530, age 218years), however, heliox usedas a facilitator of aerosol delivery in mod-
eratetosevereexacerbations providedsignificant improvement inclinical scores at 2to
4 hours and improved discharge rates at 12 hours.
47
Continuous positive airways pressure often is used in an attempt to avoid intubation
and ventilation in exhausted patients who have life-threatening asthma. Its role in
asthma remains controversial despite interesting and promising results. Significant
improvements in hospitalization rate, discharge from emergency department, pulmo-
nary function, and respiratory rate have been reported by the sole RCT included in a re-
cent adult meta-analysis.
48
There have been no RCTs to date in pediatric populations,
although published case reports of benefit exist.
49
Table 9
Management algorithm for chronic asthma
From National Asthma Council Australia. Asthma management handbook. 2006. Available at:
www.nationalasthma.org.au; with permission.
Table10
Equivalent corticosteroid dosing
Dose Level
Daily ICS Dose
CIC
a
BDP^HFA
b
FP
b
BUD
b
Low 80160 mg 100200 mg 100200 mg 200400 mg
Medium 160320 mg 200400 mg 200400 mg 400800 mg
High R320 mg > 400 mg > 400 mg > 800 mg
Abbreviations: BDP-HFA, beclomethasone dipropionate; BUD, budesonide; CIC, ciclesonide; FP,
fluticasone propionate.
a
Ex actuator dose.
b
Ex valve dose.
From National Asthma Council Australia. Asthma management handbook. 2006. Available at:
www.nationalasthma.org.au; with permission.
Robinson & Van Asperen 204
Leukotrienes are proinflammatory mediators involved in both early and late asth-
matic airway responses to allergen challenge. Leukotriene receptor antagonists
(LTRAs) inhibit a part of the asthmatic inflammatory response that is relatively unaf-
fected by OCS
50
and also provide some degree of bronchodilation. Onset of benefit
has been shown to occur at 10 minutes with IV administration and within 2 hours
with oral administration.
51
An RCT in preschool children demonstrated benefit in respi-
ratory rate and symptoms scores for up to 4 hours and reduced OCS use at 1 hour
(20.8% versus 38.5%) in comparison with placebo when LTRAs were given with the
first dose of SABA.
52
A short course of LTRAs (given for 7 days or until symptoms
had resolved for 48 hours) introduced at the first sign of an asthma exacerbation
has been shown to have a beneficial effect in intermittent asthma, with a modest re-
duction in health care utilization, symptoms, and time off school/work.
53
Although
these results are promising, the current evidence is insufficient to recommend the
routine use of LTRAs in acute asthma.
There is a paucity of evidence to support the use of antibiotics in the routine
management of acute asthma,
54
because most exacerbations are triggered by viral
infections. Antibiotics should be reserved for cases in which infection with an antibi-
otic-responsive organism (bacterial, Mycoplasma) is suspected.
Other Aspects of Treatment
Chest radiographs are indicated only for first presentations of asthma, when there are
atypical clinical features (to investigate for important differential diagnoses) or focal
signs on examination (collapse, consolidation, or pneumothorax), or when there are
severe exacerbations with a lack of response to initial treatment.
The difficulty of performing reproducible spirometry and peak expiratory flow (PEF)
in young children means that, despite being listed in severity-assessment guidelines,
lung function tests rarely are used during the initial assessment of acute asthma in
children.
Arterial blood gases also rarely are used in pediatrics, apart from life-threatening
exacerbations.
3
Free-flowing venous blood gases, taken at the time of intravenous
cannulation, provide an accurate assessment of PCO
2
, which may indicate impending
exhaustion if in the normal range (3545 mm Hg).
Education of parents and children attending the emergency department with acute
exacerbations is part of routine management in many centers, although on systematic
review an improvement in subsequent emergency department visits, hospitalization,
or unscheduled medical reviews was not demonstrated, despite eight pediatric
RCTs and large numbers (n 5 1407).
55
Physiotherapy should be avoided in the acute phase of an asthma exacerbation
because of the danger of precipitating clinical deterioration
56
but may be of benefit
in hypersecretory asthma in the recovery phase once bronchoconstriction has
improved.
57
INTERVAL ASTHMA MANAGEMENT
Assessing Severity
The grading of interval asthma severity and subsequent treatment are based on the
clinical features present before commencing treatment (see Table 6). This approach,
however, does not allowfor re-evaluation of severity once treatment has been started,
and control then is defined as the extent to which clinical features have been removed
by treatment (see Table 7). It is important to exclude modifiable factors, such as poor
adherence, incorrect inhaler technique, and smoking in adolescents, before this
Asthma in Childhood 205
assessment. Another important consideration is that asthma symptoms are not spe-
cific for asthma. The goals of management are a combination of good current control
(control of symptoms, no exercise limitation, and normal lung function, if the patient is
old enough to perform the test) and minimizing future risk (preventing decline in lung
function, preventing future exacerbations, and avoiding medication side effects). The
evidence for interval management of asthma is summarized in Table 8.
Specific practice points relevant to pediatric asthma management are highlighted in
the National Asthma Council guidelines:
3
It often is not possible to eradicate transient infant wheeze or intermittent viral-in-
duced wheezing in young children, and dose increases in an attempt to treat this
aspect are inappropriate.
One should avoid inappropriate dose increases made in an attempt to eradicate
cough completely.
Cough should not be used as a marker of control, in the absence of other
symptoms.
Symptoms are as reliable as PEF measurement in the monitoring of asthma
control.
PHARMACOLOGIC MANAGEMENT
Preventive Medications
The necessity and choice of preventive medications is determined by the initial sever-
ity assessment or the degree of control on the current medication (see Tables 4 and 5).
Nonsteroidal Agents
Nonsteroidal preventive medications include sodium cromoglycate, nedocromil
sodium, and LTRAs. All three are currently recommended as alternatives to ICS for
frequent intermittent or mild persistent asthma.
3
The use of sodium cromoglycate stretches back 35 years but has decreased sub-
stantially with the emergence of ICS, and recent systematic reviews (25 RCTs, 17 of
which were in a pediatric population) have demonstrated its inferiority to ICS.
58
Its
role in asthma remains contentious, however, after initial meta-analyses (24 pediatric
RCTs, n 5 1024), which concluded that insufficient evidence existed for benefit over
placebo, were strongly criticized.
59
Subsequent re-analysis of the data has demon-
strated a beneficial effect, particularly in older children who have asthma.
60
Having
been withdrawn from the British Thoracic Society guidelines in 2003, it has since
been reinstated as effective in children aged 512, but is not named in the corre-
sponding guideline.
Nedocromil sodium is also a cromone, a disodium salt of a pyranoquinolone dicar-
boxylic acid developed as an anti-inflammatory agent for the treatment of asthma.
61
A
recent systematic review of 15 pediatric RCTs (n 5 1422) concluded that the benefits
in lung function and symptomoutcomes suggested by short-termstudies was not rep-
licated consistently in longer-term trials. Despite its better side-effect profile, the lack
of direct comparison with ICS in RCTs has meant the evidence needed to clarify its
position in the treatment of chronic asthma is lacking.
62
This lack of data is in contrast
to the adult literature, which shows it to be an effective treatment for asthma.
63
The role of LTRAs such as montelukast and zafirlukast in interval asthma manage-
ment is of particular interest in pediatrics because montelukast can be administered
as a once-daily oral agent, potentially aiding compliance.
64
In a preschool cohort
(age 25 years) of 549 children who had predominantly virally induced intermittent
asthma, regular LTRA use reduced the rate of exacerbation over a 12-month treatment
Robinson & Van Asperen 206
period by 31.9% (1.60/year versus 2.34/year) and also reduced the need for ICS.
65
A
short course of a LTRA introduced at the first sign of infection also has been shown to
have benefit.
53
Regular low-dose ICS is not effective in reducing the exacerbation rate
or severity in this asthma subgroup,
66
and parent-initiated OCS does not reduce
hospitalization rates in preschoolers.
67
No direct comparison of LTRA and a short-
course of high-dose ICS, which may have a beneficial role, has been published to
date. Although the published data for zafirlukast in adolescents and adults largely
mirror those of montelukast, there is a paucity of data available in pediatric
populations.
In persistent asthma, the greatest benefit seems to be in cases of mild severity.
68
Large RCTs in preschool (n 5 689)
69
and school-age (n 5 336)
70
children have dem-
onstrated benefit in symptoms, SABA and OCS use, and lung function (in those old
enough to perform the test). These improvements were not documented for the sub-
groups that had moderate persistent asthma within these studies. For mild persistent
asthma, LTRA offers a clinical alternative to ICS, although ICS has a better effect on
lung function parameters.
71
ICS remains the more cost-effective option.
72,73
In mod-
erate persistent asthma, low-dose ICS is superior to LTRA, when the two are com-
pared directly, over a range of outcomes.
72,74,75,76
The clinical characteristics of
children more likely to respond to LTRAs are not clearly defined, but children who
have more frequent symptoms, increased inflammatory markers, and poorer lung
function are more likely to respond to ICS.
75,77
Although a predominantly adult sys-
tematic review (only 2 of 27 RCTs were pediatric) found modest improvements (equiv-
alent to increasing the ICS dose) when a LTRA was used as an add-on therapy to
ICS,
78
this finding was not replicated in a recent pediatric RCT, which showed
a increased exacerbation rate in the add-on group.
76
LTRAs may have a modest ste-
roid-sparing effect.
78
The equivalent data are lacking in pediatrics. A meta-analysis of
data concluding that the effect of an add-on LTRA was inferior to that of long-acting
beta-agonists (LABA)
79
contained only one pediatric RCT in abstract form, which
has been published since then
80
(n 5 80 of 6476). No formal comparison pediatric
RCTs have been published to date. There is emerging evidence of genetic polymor-
phisms that may influence the response to LTRAs.
81
Allergic rhinitis may coexist with asthma. LRTAs are superior to placebo,
82
equiva-
lent to antihistamines,
83
but inferior to nasal ICS in the treatment of allergic rhinitis.
84
A unified approach to treating the airway inflammation of both conditions is recom-
mended. Treatment of allergic rhinitis with nasal corticosteroids also has shown a trend
to improved asthma symptoms and forced expiratory volume in 1 second (FEV
1
) which
did not reach statistical significance (14 RCTs, 3 of which were pediatric).
85
A recent
adult RCT of asthmatics who had allergic rhinitis has demonstrated a pronounced
benefit of LRTA added to ICS, greater than the benefit achieved by doubling the
dose of ICS.
86
Inhaled Corticosteroids
ICS have formed the cornerstone of modern asthma management. Although not
shown to be effective in patients who have episodic virally induced exacerbations,
66
the beneficial effect of ICS in persistent asthma has been established for some
time.
87
A number of different ICS have been used, from the first ICS, beclomethasone,
to budesonide and, more recently, fluticasone, ciclesonide, and mometasone. (Initial
chlorofluorocarbon [CFC]-propelled metered-dose inhalers [MDI] have been
reformulated using hydroxyfluoroalkane [HFA] propellant, because of concerns about
the environmental impact of CFCs.)
Asthma in Childhood 207
Efficacy
Beclomethasone dipropionate was introduced in 1972. A meta-analysis of eight solely
pediatric RCTs (n 5 744, age R5 years) and four further RTCs that included children
found beclomethasone to be superior to placebo with respect to FEV
1
, symptoms,
and likelihood of exacerbations when used for at least 4 weeks.
88
Beclomethasone
seems to have a flat doseresponse curve at higher doses,
89
based on two main
RCTs, one of which was pediatric
90
(n 5177, age 616 years) comparing 400 mg/d ver-
sus 800 mg/d. The overall documented benefits in FEV
1
are small, however, and are of
uncertain clinical significance, because there was no benefit in symptoms or exacer-
bation rate. No differences between the doses were shown in the pediatric trial. Pre-
viously reported ability to wean OCS dose with beclomethasone must be interpreted
in the context of the time when the RCT was conducted (1970s) and the availability of
other treatment options. Subsequent development of a HFA-propelled beclometha-
sone MDI, with its improved solubility and smaller particle size delivery, has led to
improved drug delivery with consequent lower dose requirements.
Budesonide was introduced in 1980. Systematic review(11 pediatric RCTs, n 5926)
demonstrated clear benefit over placebo in mild to moderate persistent asthma.
91
No
dose-dependent effect above 100 to 200 mg/d was found for mild persistent asthma
(seven pediatric RCTs, n 5 726),
92
but an apparent further benefit (4% benefit in
predicted FEV
1
) in moderate-severe persistent asthma at doses of 800 mg/d has
been reported in the only pediatric RCT examining this subgroup.
93
No pediatric
RCTs have examined doses above 800 mg/d. A number of guidelines recommend
use at the same dosage as CFC beclomethasone, but there is a lack of quality RCT
data to support this recommendation (six pediatric RCTs of generally small numbers,
with the number of subjects ranging from 10 to 41).
94
Fluticasone was developed in 1990 and is available as an HFA-MDI and dry powder
inhaler (DPI), both alone and in combination with salmeterol. Systematic review
(75 RCTs including 8 pediatric RTCs, 5 of which had large sample sizes) has confirmed
the benefit of fluticasone in mild to moderate asthma with minimal additional benefit
from higher doses.
95
The finding of additional benefit of higher doses and an OCS-
sparing effect in severe asthma is based on adolescent and adult data and is not
definitive,
96
because no pediatric RCTs examined doses higher than 500 mg/d or
included children taking daily OCS. An equivalent or slightly superior effect to budeso-
nide or CFC-beclomethasone at half the dose was demonstrated on systematic re-
view (75 RCTs, 16 pediatric).
97
A newer HFA-beclomethasone aerosol has been
recommended at the same dose as fluticasone and was found to be equivalent in
an essentially adult meta-analysis.
98
The only pediatric RCT comparison to date
(n 5 280, age 512 years) also has demonstrated equivalent effect.
99
The two newest ICS are mometasone and ciclesonide. Mometasone is not currently
available as an MDI in Australia but has US Food and Drug Administration (FDA)
approval for children age 12 years and older. Ciclesonide is licensed in Australia for
children 12 years and older and in June 2008 became available for children age 4 years
and older, in line with the current FDA approval. Both drugs are approved for once-
daily use. Mometasone was introduced in 1999, and evidence from a number of adult
studies, some of which included adolescents, suggests a dose-dependent effect
up to 400 mg/d in moderate persistent asthma, with no apparent benefit at higher
doses.
100,101
An OCS-sparing effect has been documented at doses of 800/1600
mg /d.
102
Once-daily administration seems to be as effective as twice-daily administra-
tion at the same total daily dose. The one pediatric RCT to date in 296 children (age
411 years) who had mild to moderate persistent asthma showed benefit over
Robinson & Van Asperen 208
placebo, with equal efficacy of 100 mg once-daily (evening) dosing and 100 mg twice-
daily regimens.
103
Ciclesonide is the newest ICS. It has a small particle size with higher
lung deposition (52%) and lower oropharyngeal deposition (38%).
104
It is delivered as
a prodrug, des-ciclesonide, and is converted to the active drug primarily in the lungs.
Initial pediatric RCTs have shown efficacy equal to that of budesonide, at half the
budesonide dose, to 320 mg of ciclesonide administered once daily,
105,106
and to
equivalent doses of fluticasone.
107
Once-daily dosing seems to be effective.
105,106,108
Safety
Although ICS remain the treatment of choice for chronic asthma, there are concerns
about systemic side effects, such as hypothalamic-pituitary-adrenal axis suppression
and effects on linear growth, particularly at higher doses. On meta-analysis, beclome-
thasone administered at a dose of 200 mg twice daily for 7 to 12 months in mild to mod-
erate persistent asthma has been shown to cause a decrease in linear growth of 1.54
cm/y in children.
109
In the Childhood Asthma Management Plan (CAMP) study, bude-
sonide at doses of 200 to 400 mg/d caused a significant reduction in growth velocity, of
1.0 to 1.5 cm, over 3 to 5 years of treatment.
110
Catch-upgrowth seems to occur in sub-
sequent years if a lower maintenance dose is used,
111
and final adult height was unaf-
fected in a follow-up of the CAMP cohort.
112
Fluticasone, at half the budesonide and
beclomethasone dose, seems to have a comparable safety profile, although firm con-
clusions are difficult.
97
Adrenal suppression, as detected by urinary cortisol levels, has
been demonstrated at 800 to 3200 mg of budesonide,
92
and high doses of fluticasone
have been implicated in most (30 of 33) cases of adrenal crisis caused by ICS.
113
Local
side effects, such as oral candidiasis, pharyngitis, and hoarse voice can occur with
these ICS but generally are not a major issue in children, particularly if the drug is de-
livered via a spacer, which limits oropharyngeal deposition. Oral candidiasis occurred
in approximately 5% of patients taking fluticasone
95
and increased at higher doses.
96
Mometasone seems to have a similar safety profile. The ideal ICSshould have high pul-
monary deposition and residency time, lowsystemic bioavailability, and rapid systemic
clearance.
114
Ciclesonide with its low oral conversion rate (< 20%), very low systemic
bioavailability (< 1%), rapid degradation, high clearance rate, and high plasma protein
binding (> 99%) results in negligible systemic levels.
115
No adrenal suppression with
ciclesonide has been reported to date, even at high doses, and the rate of local side
effects is much better than with fluticasone.
116
Low-dose ICS have been shown often to provide optimal control for mild persistent
asthma and to reduce the risk of severe asthma exacerbations. When commencing
ICS therapy, initial low-dose ICS (see Table 10) is as effective as an initial high dose
and subsequent down titration (23 RCTs, including 5 pediatric and 4 infant RCTs).
117
Long-Acting Beta-Agonists
LABAs have a mechanism of action similar to that of SABA, but prolonged activation of
beta-2 receptors in bronchial smooth muscle results in a prolonged duration of action of
up to 12 hours. LABA monotherapy is inferior to ICS in mild to moderate asthma.
118
In
addition, no benefit in asthma control was documented when a LABA was added to
maintenance ICS in a moderate asthma cohort.
90
(The negative finding in this study
may reflect the actual population studied, rather than the intended target population, be-
cause the children in the study were controlled as well on low-dose ICS as on a doubled
dose of ICS or added LABA.) This lack of response to LABA in children is very different
from the response observed in adults;
119,120
in adults, LABA has demonstrated benefits
in a number of asthma control measures both in patients being treated with ICS
121
and in
Asthma in Childhood 209
ICS-na ve patients.
122
The apparent increase in exacerbations and lack of protective
effect with LABA use in pediatric populations has been well documented.
119,123
Concern about the safety of LABA has arisen also. Meta-analysis of RCTs with
LABA use longer than 3 months has documented an increased risk of severe and
life-threatening exacerbations, as well as increased asthma-related deaths, in both
adult and pediatric populations.
124
Particular populations identified as being at risk
were African Americans and steroid-nave patients. This concern led the US FDA Pul-
monary and Allergy Drugs Advisory Committee to strengthen its warning on all
LABAs.
125
Precipitating tachyphylaxis with regular LABA therapy and subsequent
lack of response to SABAs during exacerbations is a further concern. Currently,
LABA therapy is recommended only as add-on therapy for patients who have moder-
ate persistent asthma and who remain symptomatic despite moderate-dose ICS. The
exact recommended dose of ICS above which LABA treatment can be considered in
children remains unclear, because of the small number of available pediatric
RCTs.
90,121
Until more evidence exists to delineate better the indications for LABA
therapy, including the underlying mechanism for the different observed response in
children, these recommendations should be followed strictly.
There currently are two choices of combination inhaler: salmeterol/fluticasone avail-
able in an MDI and a DPI andeformoterol/ budesonide in an inspiratory flow-driven sus-
pension inhaler. Patient preference for the type of device may influence the physicians
decision when evaluating the choice of combination therapy. The fast onset of eformo-
terol, comparable to that of SABAs, has led to the development of a therapeutic strat-
egy with a single combination medication (eformoterol/budesonide), used as both
preventer andreliever medication. This has been demonstratedtoreduce exacerbation
rates in both adults and children (n 52760),
126
with pediatric benefit confirmed by sub-
analysis of the pediatric data (n 5 341).
127
Although not yet incorporated into guide-
lines, this approach remains a promising management strategy that may offer
improved compliance and a therapeutic option for adolescents who have difficult-to-
control, severe persistent asthma. The drug currently is not approved in Australia for
children under age 12 years.
Oral Corticosteroids and Other Immunosuppressive Agents
Five percent to 10%of persons who have severe persistent asthma are not responsive to
maximal inhaled therapy
128
and depend on OCS for adequate control. Although some
data comparing ICS and OCS dosages in adults are available,
129
equivalent data for
the pediatric population are lacking, and the side effects associated with regular OCS
are a concern. Potential side effects of regular OCS include osteoporosis, hypertension,
and secondary diabetes mellitus. A number of second-line immunosuppressive agents
(steroid-sparing agents) have been evaluated. Attempted systematic reviews of the ef-
ficacy of azathioprine,
130
chloroquine,
131
colchicine,
132
cyclosporine,
133
dapsone,
134
methotrexate
135
and gold
136
have been limited by a small number, if any, of acceptable
RCTs. NopediatricRCTs havebeenincluded. Small but statisticallysignificant decreases
in OCS have been demonstrated with gold, methotrexate, and cyclosporine, but the clin-
ical significanceof this observeddose response is unclear, especially given the additional
side-effect profileof theimmunosuppressivedrugs themselves. Thelongest studytodate
investigatingmethotrexate, 10mgweekly for 1year inadults, reporteda55%reductionin
OCS dose (compared with 4% in placebo) but no benefit in bone metabolism.
137
Immunoglobulins and Omalizumab Therapy
A number of small studies have examined the role of intravenous immunoglobulin
(IVIG) as a steroid-sparing agent. The positive results of initial open-label studies
Robinson & Van Asperen 210
have not been replicated in subsequent RCTs including children,
138,139
and its role in
asthma has been restricted. There also are safety concerns: one RCT was terminated
prematurely after 3 of 16 patients in the high-dose IVIG arm (2 mg/kg monthly for
7 months) developed aseptic meningitis.
139
IVIG may play a role in a subset
patients who have severe asthma with associated specific antibody deficiency,
140
but further research is needed.
Omalizumab is a humanized monoclonal antibody that forms complexes with circu-
lating free IgE and represents a potential therapy for allergic disease. It currently is the
only monoclonal antibody approved for asthma treatment and is included at step 5 in
the current Global Initiative for Asthma guidelines (2006). Its true role in asthma man-
agement remains unclear, however. As an add-on therapy to ICS, omalizumab dem-
onstrated benefits in symptom control and exacerbation rates in persistent asthma of
varying severity,
141
but no benefit in exacerbation rate or steroid dose was seen in per-
sons receiving regular OCS therapy. Only one RCT
142
has been conducted to date in
children under age 12 years (range, 512 years) who had mild to moderate persistent
asthma, and the results were similar. Omalizumab is an expensive drug, and its cost
effectiveness remains debated.
143,144
Further studies are needed in the pediatric pop-
ulation for better clarification of patients likely to respond. The modest ICS-sparing ef-
fect also needs to be compared formally with cheaper alternatives such as the addition
of LABA and LTRA.
Allergen Immunotherapy
Allergen immunotherapy is an evolving field, with both subcutaneous immunotherapy
(SCIT) and sublingual immunotherapy (SLIT) desensitization now available for com-
mon aeroallergens such as pollen, house dust mite (HDM), and cat. Although immuno-
therapy has been shown to be an effective treatment for insect allergy and allergic
rhinitis, its effectiveness and utility in the treatment of asthma are controversial.
On meta-analysis, in comparison with placebo, SCIT led to a reduction in asthma
symptoms and use of asthma medication, as well as allergen-specific bronchial hy-
per-responsiveness, but had no consistent effect on lung function (75 RCTs, including
38 RCTs limited to or including pediatric patients).
145
It remains unclear howSCIT per-
forms against other available therapies; the only comparison RCT, performed in
adults, suggests a response inferior to the response to ICS.
146
In a pediatric-specific
meta-analysis (nine RCTs including 441 children), SLIT was shown to be effective in
reducing asthma scores and reducing the need for rescue medication, but positive
findings were confined to SLIT with HDM extract, not in children treated with pollen
or grass extract.
147
No directly comparative studies in pediatric asthma have been
performed, although SLIT has been reported to be about 50% as efficacious as
SCIT for the treatment of allergic rhinitis in adults.
148
Of note, all SCIT and SLIT studies
to date included only patients who had mild/moderate asthma and examined mono-
therapy, not polytherapy with an allergen mixture. Although allergen immunotherapy
may provide therapeutic benefit in patients who have an identified extrinsic, clinically
unavoidable allergen, the risk of potentially fatal anaphylaxis (although rare) should be
considered carefully and discussed with the parents if SCIT is being considered. SLIT
has very few reported serious side effects and can be delivered at home. There cur-
rently is insufficient evidence to recommend SLIT or SCIT as a standard treatment
for pediatric asthma.
Other Anti-Inflammatory Medications
A number of agents with potential anti-inflammatory actions have been identified,
including macrolides, xanthines, and ketotifen. Small RCTs of macrolide therapy,
Asthma in Childhood 211
including one pediatric RCT (n 519),
149
have suggested a beneficial effect, but further
studies are necessary to delineate which patients are most likely to benefit.
150
Xan-
thines (eg, theophylline) have been shown on meta-analysis to improve symptom con-
trol and SABA use compared with placebo and seem to be similar in efficacy to
sodium cromoglycate but inferior to ICS (n 52734, 34 pediatric RCTs).
151
Concern re-
garding a potential negative impact on behavior and concentration has limited its use,
although these data are inconclusive; this concern is likely to be less of an issue now
that lower doses are being used.
151
Ketotifen, an antihistamine, has been shown to
improve asthma control in predominantly atopic, mild to moderate childhood asthma
when used alone or in combination with other therapies (meta-analysis of 26 pediatric
RCTs).
152
Benefit needs to be weighed against side effects such as sedation and
weight gain.
Other Medications
Gastroesophageal reflux is common in asthma
153,154
and often is asymptomatic.
154
Pediatric RCTs of gastroesophageal reflux treatment have documented statistically
significant improvements in clinical scores with treatment, but the clinical significance
is unclear.
154,155
Exercise-Induced Asthma
SABA administration before exercise confers significant protection for up to 3
hours.
156
A number of potential preventive therapies also have been shown to be
effective for symptoms not adequately controlled with this approach. ICS given for
at least 4 weeks were shown on meta-analysis (six RCTs of which four were pediatric,
total n 5 123, 102 pediatric subjects) to attenuate the fall in FEV
1
associated with ex-
ercise.
157
There currently is insufficient evidence to draw conclusions about shorter
durations of ICS treatment. Also of note, in a population with mild persistent
asthma,
158
there was a pronounced decrease in the exercise-induced fall in FEV
1
with 400 mg/d budesonide compared with 100 mg g/d, suggesting that a higher ICS
dose may be needed to negate exercise symptoms despite good control of other
symptoms. Nonsteroidal alternatives include sodium cromoglycate, nedocromil so-
dium, and LTRA. On meta-analysis (n 5 280, 60% pediatric), nedocromil sodium
has shown a consistent benefit in exercise-induced symptoms in both adults and chil-
dren age 6 years and older.
159
LRTAs have a beneficial effect in exercise-induced
asthma in children, with a significant reduction in FEV
1
fall
160,161,162,163
and onset of
action within two doses.
162
Recently a head-to-head comparison between different
therapies has been performed in a pediatric RCT (age 618 years, n 580), which con-
firmed the beneficial effect of regular therapy and suggested that the best protection is
offered by montelukast, either alone or in combination with budesonide.
164
NONPHARMACOLOGIC MANAGEMENT
Dietary
Epidemiologic studies have attempted to explain the increasing prevalence of allergic
diseases, especially in developed countries, and have examined a number of possible
dietary factors. Attempted meta-analysis of calorie-controlled diets
165
and selenium
supplementation
166
was limited by a lack of well-designed RCTs (only one was iden-
tified for either condition). Other RTCs, for fish oil supplements,
167
low or excluded
salt,
168
tartrazine exclusion,
169
and vitamin C supplementation,
170
included between
six and nine RCTs (two or fewer were pediatric) and failed to demonstrate any benefit.
Robinson & Van Asperen 212
Complementary Alternative Medicine
Complementary alternative medicine (CAM) is used commonly in pediatric asthma,
with an estimated 50% to 60% of children using CAM at any one time.
171
(Only half
of the cohort volunteered this information to their physician.) A lack of high-quality
RCTs and heterogeneity of practice has hampered meta-analysis. There currently is
no evidence to support the role of acupuncture,
172
homeopathy,
173
manual ther-
apy,
174
or various breathing techniques
175,176
in chronic asthma. A recent RCT of
breathing techniques in adults and adolescents who had mild persistent asthma docu-
mented impressive reductions in SABA use and ICS dose, although the lack of a true
control arm makes it hard to rule out a trial effect.
177
Inspiratory muscle training in
adults has demonstrated significant improvement in maximum inspiratory pressure,
but the most of the research has been conducted by a single research group, and
the clinical significance remains unclear.
178
A number of pediatric studies of physical
fitness training in chronic asthmatics have successfully demonstrated improved car-
diorespiratory fitness without deterioration in respiratory symptoms,
179
but whether
improved fitness translates into better quality of life or lung function remains unclear.
This finding, however, reinforces the overall aim of management in pediatric asthma,
namely to allow the child to live as normal a life as possible, including full participation
in activity.
Allergen Avoidance
Meta-analysis of studies using allergen-avoidance measures, including HDM reduc-
tion measures,
180
humidity control,
181
use of ionizers,
182
pet allergen control,
183
non-feather bedding,
184
and speleotherapy,
185
have failed to document any benefit
in asthma control.
Asthma Prevention
Asthma prevention can be divided into primary (preventing onset of established risk
factors), secondary (preventing development of asthma once established risk factors
have developed) and tertiary prevention (care of established asthma and preventing
exacerbations).
Potential environmental factors in asthma are supported by marked geographic and
temporal variation in asthma prevalence.
1
Initial studies of environmental manipulation
were promising, with HDM and food allergen avoidance measures in the first
12 months of life resulting in decreased sensitization and asthma diagnosis persisting
until the age of 8 years in a high-risk birth cohort in the Isle of Wight.
186
Subsequent
larger, multifaceted studies in Canada and Australia have failed to reproduce these
results. The Canadian Childhood Asthma Primary Prevention Study showed a benefit
in asthma symptoms but not bronchial hyper-responsiveness at 7 years,
187
whereas
the Australian Childhood Asthma Prevention Study failed to show any clinical benefit
at 5 years despite a 61% reduction in HDM and successful dietary manipulation.
188
Other current studies at earlier stages have yet to report positive results. The balance
of evidence at present does not support the benefit of avoidance of allergens in early
life on the subsequent development of asthma.
Breastfeeding currently is recommended for the first 6 months of life. There are
a number of advantages to breastfeeding, but its protective role against allergic dis-
ease remains controversial. Although studies of formula-fed infants have reported
higher rates of allergic disease, evidence does not support a protective effect on al-
lergy and asthma. A recent large RCT in a birth cohort (n 5 17,046) documented no
protective effect at age 6.5 years of prolonged or exclusive breast feeding.
189
The
Asthma in Childhood 213
link between antenatal and postnatal exposure to environmental tobacco smoke and
subsequent increased risk of asthma is well established.
190
No RCTs have been per-
formed to date, but avoidance of environmental tobacco smoke is strongly
recommended.
The Early Treatment of the Atopic Child study reported no overall benefit of
prolonged cetirizine (H1 receptor antagonist) treatment in infants who had atopic der-
matitis at 18-month posttreatment follow-up. Benefit was seen only in sensitized sub-
groups, persisting to 36 months in grass pollensensitized infants but only transiently
in those sensitized to HDM.
191
A subsequent study, the Early Prevention of Asthma in
Atopic Children study, specifically targeted these subgroups but failed to show any
benefit (UCB Pharma SA Belgium, unpublished data).
The rationale for tertiary prevention studies is the observation that a large number of
persistent asthma cases start early in life,
192
but the three trials conducted to date, at
differing ages or stages of asthma development, have had disappointing results. In-
termittent courses of ICS
193
and maintenance ICS,
194
for varying durations, in infants
who had recurrent wheeze demonstrated no difference in asthma prevalence. The
Childhood Asthma Management Program examined the effects of prolonged ICS or
nedocromil sodium treatment for 4 to 6 years in a large group of school-age (512
years) children who had mild to moderate persistent asthma. Although ICS resulted
in better symptom control, there was only a mild benefit in bronchial hyper-respon-
siveness and no effect on lung function outcome at the end of treatment.
110
Vaccination in asthma may prevent exacerbations and serious complications such
as pneumonia. Current guidelines recommend influenza vaccination for all children
who have asthma, but there is a lack of pediatric evidence to support this recommen-
dation.
195,196
In practice, vaccine coverage remains low despite the recommenda-
tion.
197
Pneumococcal vaccine has yet to demonstrate proven benefit in RCTs
198
but is now part of the routine vaccination schedule in many countries.
Other Aspects of Care
Education is a fundamental part of pediatric asthma management, including specific
components of care (eg, training in the optimal use of medications), review of inhaler
technique, and understanding of individualized written asthma-management plans.
Education in self-management strategies does improve asthma outcomes,
199
includ-
ing morbidity, but does not seem to improve quality of life.
200
Child-centered educa-
tion seems to offer greater benefit than caregiver-focused education.
200
Written
asthma-management plans, targeting symptom-based management rather than
PEF, are effective in reducing exacerbation rates.
201,202
Having health care workers
of patients ethnic groups may be beneficial in improving asthma outcomes.
203
The
evidence to support the role of family therapy or other psychologic interventions is lim-
ited,
204,205
but it may be a useful adjunct to care in certain children.
Spacers are required to deliver MDI medication effectively to younger children and
are recommended to optimize delivery for older children, particularly in preventive
therapy and in acute asthma. Small-volume spacers can be used from infancy with
facemasks and from age 3 years with mouthpieces. Large-volume spacers can be
used from 5 years of age. DPIs can be considered from the age of 6 years; breath-
actuated devices are more appropriate from the age of 8 years, depending on the
abilities and development of the individual child.
3
Noninvasive methods to monitor airway inflammation, including exhaled nitric ox-
ide, exhaled breath condensate, and induced sputum eosinophils, have shown bene-
fits in adults.
206
The first pediatric longitudinal studies now have been published.
These studies show a benefit in asthma control, and although there is not yet definitive
Robinson & Van Asperen 214
evidence for incorporating these measures into asthma-management guidelines,
these methods are promising tools for future management.
206,207
SUMMARY
Pediatric asthma is a common condition with a large health care burden. Despite the
large number of RCTs and meta-analyses conducted, there is a paucity of pediatric
evidence on which to base appropriate management guidelines, and data from adult
RCTs should not be extrapolated inappropriately to this younger age group. Consen-
sus guidelines based on a combination of available evidence and expert opinion do
exist, however, and these guidelines will continue to evolve as more conclusive pedi-
atric evidence becomes available. Although these guidelines should form the basis of
pediatric asthma management, important differential diagnoses and potentially
modifiable factors also should be considered before commencing or escalating treat-
ment. Recommendations based on the available pediatric evidence are summarized in
Tables 4 and 8.
REFERENCES
1. Asher MI, Montefort S, Bjorksten B, et al. Worldwide time trends in the preva-
lence of symptoms of asthma, allergic rhinoconjunctivitis, and eczema in child-
hood: ISAAC phases one and three repeat multicountry cross-sectional surveys.
Lancet 2006;368:73343.
2. Schunemann HJ, Jaeschke R, Cook DJ, et al. An official ATS statement: grading
the quality of evidence and strength of recommendations in ATS guidelines and
recommendations. Am J Respir Crit Care Med 2006;174:60514.
3. National Asthma Council Australia. Asthma management handbook. Melbourne:
National Asthma Council Australia Ltd.; 2006.
4. van Asperen PP. Cough and asthma. Paediatr Respir Rev 2006;7:2630.
5. Weinberger M, Abu-Hasan M. Pseudo-asthma: when cough, wheezing, and
dyspnea are not asthma. Pediatrics 2007;120:85564.
6. Geelhoed GC, Landau LI, Le Souef PN. Evaluation of SaO
2
as a predictor of out-
come in 280 children presenting with acute asthma. Ann Emerg Med 1994;23:
123641.
7. Keahey L, Bulloch B, Becker AB, et al. Initial oxygen saturation as a predictor of
admission in children presenting to the emergency department with acute
asthma. Ann Emerg Med 2002;40:3007.
8. Camargo CA Jr, Spooner CH, Rowe BH. Continuous versus intermittent beta-ag-
onists for acute asthma. Cochrane Database Syst Rev 2003;(4):Art. No.:
CD001115. DOI:10.1002/14651858.CD001115.
9. Khine H, Fuchs SM, Saville AL. Continuous vs intermittent nebulized albuterol for
emergency management of asthma. Acad Emerg Med. 1996;3:101924.
10. Papo MC, Frank J, Thompson AE. A prospective, randomized study of continu-
ous versus intermittent nebulized albuterol for severe status asthmaticus in chil-
dren. Crit Care Med 1993;21:147986.
11. Cates CJ, Crilly JA, Rowe BH. Holding chambers (spacers) versus nebulisers for
beta-agonist treatment of acute asthma. Cochrane Database Syst Rev
2006;(2):Art. No.: CD000052. DOI:10.1002/14651858.CD000052.pub2.
12. Sears MR. Inhaled beta agonists. Ann Allergy 1992;68:446.
13. Plotnick LH, Ducharme FM. Combined inhaled anticholinergics and beta2-
agonists for initial treatment of acute asthma in children. Cochrane Database
Syst Rev 2000;(3):Art. No.: CD000060. DOI:10.1002/14651858.CD000060.
Asthma in Childhood 215
14. Everard ML, Bara A, Kurian M, et al. Anticholinergic drugs for wheeze in children
under the age of two years. Cochrane Database Syst Rev 2005;(3):Art. No.:
CD001279. DOI:10.1002/14651858.CD001279.pub2.
15. Garrett J, Williams S, Wong C, et al. Treatment of acute asthmatic exacerbations
with an increased dose of inhaled steroid. Arch Dis Child 1998;79:127.
16. Hendeles L, Sherman J. Are inhaled corticosteroids effective for acute exacer-
bations of asthma in children? J Pediatr 2003;142:S2632.
17. Hendeles L. Selecting a systemic corticosteroid for acute asthma in young
children. J Pediatr 2003;142:S404.
18. Langton HS, Hobbs J, Reid F, et al. Prednisolone in acute childhood asthma:
clinical responses to three dosages. Respir Med 1998;92:5416.
19. Manser R, Reid D, Abramson M. Corticosteroids for acute severe asthma in hos-
pitalised patients. Cochrane Database Syst Rev 2001;(1):Art. No.: CD001740.
DOI:10.1002/14651858.CD001740.
20. van Asperen PP, Mellis CM, Sly PD. The role of corticosteroids in the manage-
ment of childhood asthma. Med J Aust 2002;176:16873.
21. Storr J, Barrell E, Barry W, et al. Effect of a single oral dose of prednisolone in
acute childhood asthma. Lancet 1987;1:87982.
22. Ho L, Landau LI, Le Souef PN. Lack of efficacy of single-dose prednisolone in
moderately severe asthma. Med J Aust 1994;160:7014.
23. Chang AB, Clark R, Thearle D, et al. Longer better than shorter? A multicentre
randomised contriol trial (RCT) of 5 vs 3 days of oral prednisolone for acute
asthma in children. Respirology 2007;12:A67 (12th Congress of the APSR/2nd
Joint Congress of the APSR/ACCP, 30 November4 December, Queensland,
Australia).
24. Rowe BH, Spooner C, Ducharme FM, et al. Early emergency department treat-
ment of acute asthma with systemic corticosteroids. Cochrane Database Syst
Rev 2001;(1):Art. No.: CD002178. DOI:10.1002/14651858.CD002178.
25. Vuillermin P, South M, Robertson C. Parent-initiated oral corticosteroid therapy
for intermittent wheezing illnesses in children. Cochrane Database Syst Rev
2006;(3):CD005311. DOI:10.1002/14651858.CD005311.pub2.
26. Becker JM, Arora A, Scarfone RJ, et al. Oral versus intravenous corticoste-
roids in children hospitalized with asthma. J Allergy Clin Immunol 1999;103:
58690.
27. Altamimi S, Robertson G, Jastaniah W, et al. Single-dose oral dexamethasone in
the emergency management of children with exacerbations of mild to moderate
asthma. Pediatr Emerg Care 2006;22:78693.
28. Gries DM, Moffitt DR, Pulos E, et al. A single dose of intramuscularly adminis-
tered dexamethasone acetate is as effective as oral prednisone to treat asthma
exacerbations in young children. J Pediatr 2000;136:298303.
29. Gordon S, Tompkins T, Dayan PS. Randomized trial of single-dose intramuscular
dexamethasone compared with prednisolone for children with acute asthma.
Pediatr Emerg Care 2007;23:5217.
30. Deshpande A, McKenzie SA. Short course of steroids in home treatment of
children with acute asthma. Br Med J (Clin Res Ed) 1986;293:16971.
31. Edmonds ML, Camargo CA Jr, Brenner BE, et al. Replacement of oral corticoste-
roids with inhaled corticosteroids in the treatment of acute asthma following
emergency department discharge: a meta-analysis. Chest 2002;121:1798805.
32. Parr JR, Salama A, Sebire P. A survey of consultant practice: intravenous salbu-
tamol or aminophylline for acute severe childhood asthma and awareness of
potential hypokalaemia. Eur J Pediatr 2006;165:3235.
Robinson & Van Asperen 216
33. Kirby C. Comparison of intravenous and inhaled salbutamol in severe acute
asthma. Pediatr Rev Commun 1988;3:6777.
34. Browne GJ, Penna AS, Phung X, et al. Randomised trial of intravenous salbuta-
mol in early management of acute severe asthma in children. Lancet 1997;349:
3015.
35. Browne GJ, Lam LT. Single-dose intravenous salbutamol bolus for managing
children with acute severe asthma in the emergency department: reanalysis of
data. Pediatr Crit Care Med 2002;3:11723.
36. Travers A, Jones AP, Kelly K, et al. Intravenous beta2-agonists for acute asthma
in the emergency department. Cochrane Database Syst Rev 2001;(1):Art. No.:
CD002988. DOI:10.1002/14651858.CD002988.
37. Roberts G, Newsom D, Gomez K, et al. Intravenous salbutamol bolus compared
with an aminophylline infusion in children with severe asthma: a randomised
controlled trial. Thorax 2003;58:30610.
38. Mitra A, Bassler D, Watts K, et al. Intravenous aminophylline for acute severe
asthma in children over two years receiving inhaled bronchodilators. Cochrane
Database Syst Rev 2005;(2):Art. No.: CD001276. DOI:10.1002/14651858.
CD001276.pub2.
39. Yung M, South M. Randomised controlled trial of aminophylline for severe acute
asthma. Arch Dis Child 1998;79:40510.
40. Silveira DR, Piva JP, Jose Cauduro MP, et al. Early administration of two intrave-
nous bolus of aminophylline added to the standard treatment of children with
acute asthma. Respir Med 2008;102:15661.
41. Gourgoulianis KI, Chatziparasidis G, Chatziefthimiou A, et al. Magnesium as
a relaxing factor of airway smooth muscles. J Aerosol Med 2001;14:3017.
42. Cairns CB, Kraft M. Magnesium attenuates the neutrophil respiratory burst in
adult asthmatic patients. Acad Emerg Med 1996;3:10937.
43. Cheuk DK, Chau TC, Lee SL. A meta-analysis on intravenous magnesium sul-
phate for treating acute asthma. Arch Dis Child 2005;90:747.
44. Rowe BH, Bretzlaff JA, Bourdon C, et al. Intravenous magnesium sulfate treat-
ment for acute asthma in the emergency department: a systematic review of
the literature. Ann Emerg Med 2000;36:18190.
45. Blitz M, Blitz S, Beasely R, et al. Inhaled magnesium sulfate in the treatment of
acute asthma. Cochrane Database Syst Rev 2005;(4):Art. No.: CD003898.
DOI:10.1002/14651858.CD003898.pub4.
46. Rodrigo G, Pollack C, Rodrigo C, et al. Heliox for nonintubated acute asthma pa-
tients. Cochrane Database Syst Rev 2006;(4):Art. No.: CD002884. DOI:10.1002/
14651858.CD002884.pub2.
47. Kim IK, Phrampus E, Venkataraman S, et al. Helium/oxygen-driven albuter-
ol nebulization in the treatment of children with moderate to severe asthma
exacerbations: a randomized, controlled trial. Pediatrics 2005;116:
112733.
48. RamFSF, Wellington SR, Rowe B, et al. Non-invasive positive pressure ventilation
for treatment of respiratory failure due to severe acute exacerbations of asthma.
Cochrane Database Syst Rev 2005;(3):Art. No.: CD004360. DOI:10.1002/
14651858.CD004360.pub3.
49. Haggenmacher C, Biarent D, Otte F, et al [Non-invasive bi-level ventilation in
paediatric status asthmaticus]. Arch Pediatr 2005;12:17857 [in French].
50. Dworski R, Fitzgerald GA, Oates JA, et al. Effect of oral prednisone on airway
inflammatory mediators in atopic asthma. Am J Respir Crit Care Med 1994;
149:9539.
Asthma in Childhood 217
51. Camargo CA Jr, Smithline HA, Malice MP, et al. A randomized controlled trial of
intravenous montelukast in acute asthma. Am J Respir Crit Care Med 2003;167:
52833.
52. Harmanci K, Bakirtas A, Turktas I, et al. Oral montelukast treatment of preschool-
aged children with acute asthma. Ann Allergy Asthma Immunol 2006;96:7315.
53. Robertson CF, Price D, Henry R, et al. Short-course montelukast for intermittent
asthma in children: a randomized controlled trial. Am J Respir Crit Care Med
2007;175:3239.
54. GrahamV, Lasserson TJ, Rowe BH. Antibiotics for acute asthma. Cochrane Data-
base Syst Rev 2001;(2):Art. No.: CD002741. DOI:10.1002/14651858.CD002741.
55. Haby MM, Waters E, Robertson CF, et al. Interventions for educating children
who have attended the emergency room for asthma. Cochrane Database Syst
Rev 2001;(1):Art. No.: CD001290. DOI:10.1002/14651858.CD001290.
56. Echeverria ZL, Tomico DR, Bracamonte BT, et al. Status asthmaticus: is respira-
tory physiotherapy necessary? Allergol Immunopathol (Madr) 2000;28:2901.
57. Asher MI, Douglas C, Airy M, et al. Effects of chest physical therapy on lung
function in children recovering from acute severe asthma. Pediatr Pulmonol
1990;9:14651.
58. Guevara JP, Ducharme FM, Keren R, et al. Inhaled corticosteroids versus
sodium cromoglycate in children and adults with asthma. Cochrane Database
Syst Rev 2006;(2):Art.No.: CD003558. DOI:10.1002/14651858.CD003558.pub2.
59. van der Wouden JC, Tasche MJA, Bernsen RMD, et al. Sodium cromoglycate for
asthma in children. Cochrane Database Syst Rev 2003;(3):Art. No.: CD002173.
DOI:10.1002/14651858.CD002173.
60. Stevens MT, Edwards AM, Howell JB. Sodium cromoglicate: an ineffective drug
or meta-analysis misused? Pharm Stat. 2007;6:12337.
61. Rainey DK. Evidence for the anti-inflammatory activity of nedocromil sodium.
Clin Exp Allergy 1992;22:9769.
62. Sridhar AV, McKean M. Nedocromil sodium for chronic asthma in children.
Cochrane Database Syst Rev 2006;(3):Art. No.: CD004108. DOI:10.1002/
14651858.CD004108.pub2.
63. Edwards AM, Stevens MT. The clinical efficacy of inhaled nedocromil sodium
(Tilade) in the treatment of asthma. Eur Respir J 1993;6:3541.
64. Maspero JF, Duenas-Meza E, Volovitz B, et al. Oral montelukast versus inhaled
beclomethasone in 6- to 11-year-old children with asthma: results of an open-la-
bel extension study evaluating long-term safety, satisfaction, and adherence
with therapy. Curr Med Res Opin 2001;17:96104.
65. Bisgaard H, Zielen S, Garcia-Garcia ML, et al. Montelukast reduces asthma ex-
acerbations in 2- to 5-year-old children with intermittent asthma. Am J Respir Crit
Care Med 2005;171:31522.
66. McKean M, Ducharme F. Inhaled steroids for episodic viral wheeze of childhood.
Cochrane Database Syst Rev 2000;(1):Art. No.: CD001107. DOI:10.1002/
14651858.CD001107.
67. Oommen A, Lambert PC, Grigg J. Efficacy of a short course of parent-initiated
oral prednisolone for viral wheeze in children aged 1-5 years: randomised con-
trolled trial. Lancet 2003;362:14338.
68. Becker A, Swern A, Tozzi CA, et al. Montelukast in asthmatic patients 6 years14
years old with an FEV1 > 75%. Curr Med Res Opin 2004;20:16519.
69. Knorr B, Franchi LM, Bisgaard H, et al. Montelukast, a leukotriene receptor
antagonist, for the treatment of persistent asthma in children aged 2 to 5 years.
Pediatrics 2001;108:E48.
Robinson & Van Asperen 218
70. Knorr B, Matz J, Bernstein JA, et al. Montelukast for chronic asthma in 6- to 14-
year-old children: a randomized, double-blind trial. Pediatric Montelukast Study
Group. JAMA 1998;279:11816.
71. Garcia Garcia ML, Wahn U, Gilles L, et al. Montelukast, compared with flutica-
sone, for control of asthma among 6- to 14-year-old patients with mild asthma:
the MOSAIC study. Pediatrics 2005;116:3609.
72. Ostrom NK, Decotiis BA, Lincourt WR, et al. Comparative efficacy and safety of
low-dose fluticasone propionate and montelukast in children with persistent
asthma. J Pediatr 2005;147:21320.
73. Stempel DA, Kruzikas DT, Manjunath R. Comparative efficacy and cost of
asthma care in children with asthma treated with fluticasone propionate and
montelukast. J Pediatr 2007;150:1627.
74. Sorkness CA, Lemanske RF, Jr., Mauger DT, et al. Long-term comparison of
3 controller regimens for mild-moderate persistent childhood asthma: the Pedi-
atric Asthma Controller Trial. J Allergy Clin Immunol 119:6472, 200.
75. Zeiger RS, Szefler SJ, Phillips BR, et al. Response profiles to fluticasone and
montelukast in mild-to-moderate persistent childhood asthma. J Allergy Clin
Immunol 2006;117:4552.
76. Jat GC, Mathew JL, Singh M. Treatment with 400 microg of inhaled budesonide
vs 200 microg of inhaled budesonide and oral montelukast in children with
moderate persistent asthma: randomized controlled trial. Ann Allergy Asthma
Immunol 2006;97:397401.
77. Szefler SJ, Phillips BR, Martinez FD, et al. Characterization of within-subject
responses to fluticasone and montelukast in childhood asthma. J Allergy Clin
Immunol 2005;115:23342.
78. Ducharme F, Schwartz Z, Kakuma R. Addition of anti-leukotriene agents to
inhaled corticosteroids for chronic asthma. Cochrane Database Syst Rev
2004;(1):Art. No.: CD003133. DOI:10.1002/14651858.CD003133.pub2.
79. Ducharme FM, Lasserson TJ, Cates CJ. Long-acting beta2-agonists versus anti-
leukotrienes as add-on therapy to inhaled corticosteroids for chronic asthma.
Cochrane Database Syst Rev 2006;(4):Art. No.: CD003137. DOI:10.1002/
14651858.CD003137.pub3.
80. Stelmach I, Grzelewski T, Bobrowska-Korzeniowska M, et al. A randomized,
double-blind trial of the effect of anti-asthma treatment on lung function in chil-
dren with asthma. Pulm Pharmacol Ther 2007;20:691700.
81. Morrow T. Implications of pharmacogenomics in the current and future treatment
of asthma. J Manag Care Pharm. 2007;13:497505.
82. Razi C, Bakirtas A, Harmanci K, et al. Effect of montelukast on symptoms and
exhaled nitric oxide levels in 7- to 14-year-old children with seasonal allergic rhi-
nitis. Ann Allergy Asthma Immunol 2006;97:76774.
83. Chen ST, Lu KH, Sun HL, et al. Randomized placebo-controlled trial comparing
montelukast and cetirizine for treating perennial allergic rhinitis in children aged
2-6 yr. Pediatr Allergy Immunol 2006;17:4954.
84. Nayak A, Langdon RB. Montelukast in the treatment of allergic rhinitis: an
evidence-based review. Drugs 2007;67:887901.
85. Taramarcaz P, Gibson PG. Intranasal corticosteroids for asthma control in peo-
ple with coexisting asthma and rhinitis. Cochrane Database Syst Rev
2003;(3):Art. No.: CD003570. DOI:10.1002/14651858.CD003570.
86. Price DB, Swern A, Tozzi CA, et al. Effect of montelukast on lung function in
asthma patients with allergic rhinitis: analysis from the COMPACT trial. Allergy
2006;61:73742.
Asthma in Childhood 219
87. Calpin C, Macarthur C, Stephens D, et al. Effectiveness of prophylactic inhaled
steroids in childhood asthma: a systemic review of the literature. J Allergy Clin
Immunol 1997;100:4527.
88. Adams NP, Bestall JB, Malouf R, et al. Beclomethasone versus placebo for
chronic asthma. Cochrane Database Syst Rev 2005;(1):Art. No.: CD002738.
DOI:10.1002/14651858.CD002738.pub2.
89. Adams N, Bestall J, Jones P. Beclomethasone at different doses for chronic
asthma. Cochrane Database Syst Rev 1999;(4):Art. No.: CD002879.
DOI:10.1002/14651858.CD002879.
90. Verberne AA, Frost C, Duiverman EJ, et al. Addition of salmeterol versus dou-
bling the dose of beclomethasone in children with asthma. The Dutch Asthma
Study Group. Am J Respir Crit Care Med 1998;158:2139.
91. Adams N, Bestall J, Jones PW. Budesonide versus placebo for chronic asthma
in children and adults. Cochrane Database Syst Rev 1999;(4):Art. No.:
CD003274. DOI:10.1002/14651858.CD003274.
92. Adams N, Bestall J, Jones P. Budesonide at different doses for chronic asthma.
Cochrane Database Syst Rev 2000;(2):Art. No.: CD003271. DOI:10.1002/
14651858.CD003271.
93. Shapiro G, Bronsky EA, LaForce CF, et al. Dose-related efficacy of budesonide
administered via a dry powder inhaler in the treatment of children with moderate
to severe persistent asthma. J Pediatr 1998;132:97682.
94. Adams N, Bestall JM, Jones PW. Beclomethasone versus budesonide for
chronic asthma. Cochrane Database Syst Rev 2000;(1):Art. No.: CD003530.
DOI:10.1002/14651858.CD003530.
95. Adams NP, Bestall JC, Lasserson TJ, et al. Fluticasone versus placebo for
chronic asthma in adults and children. Cochrane Database Syst Rev
2005;(4):Art. No.: CD003135. DOI:10.1002/14651858.CD003135.pub3.
96. Adams NP, Bestall JC, Jones PW, et al. Fluticasone at different doses for chronic
asthma in adults and children. Cochrane Database Syst Rev 2005;(3):Art. No.:
CD003534. DOI:10.1002/14651858.CD003534.pub2.
97. Adams N, Lasserson TJ, Cates CJ, et al. Fluticasone versus beclomethasone or
budesonide for chronic asthma in adults and children. Cochrane Database Syst
Rev 2007;(4):Art. No.: CD002310. DOI:10.1002/14651858.CD002310.pub4.
98. Lasserson TJ, Cates CJ, Jones A-B, et al. Fluticasone versus HFA-
beclomethasone dipropionate for chronic asthma in adults and children.
Cochrane Database Syst Rev 2006;(2):Art. No.: CD005309. DOI:10.1002/
14651858.CD005309.pub3.
99. van Aalderen WM, Price D, De Baets FM, et al. Beclomethasone dipropionate
extrafine aerosol versus fluticasone propionate in children with asthma. Respir
Med 2007;101:158593.
100. OConnor B, Bonnaud G, Haahtela T, et al. Dose-ranging study of mometasone
furoate dry powder inhaler in the treatment of moderate persistent asthma using
fluticasone propionate as an active comparator. Ann Allergy Asthma Immunol
2001;86:397404.
101. Bernstein DI, Berkowitz RB, Chervinsky P, et al. Dose-ranging study of a new
steroid for asthma: mometasone furoate dry powder inhaler. Respir Med 1999;
93:60312.
102. Fish JE, Karpel JP, Craig TJ, et al. Inhaled mometasone furoate reduces oral
prednisone requirements while improving respiratory function and health-
related quality of life in patients with severe persistent asthma. J Allergy Clin
Immunol 2000;106:85260.
Robinson & Van Asperen 220
103. Berger WE, Milgrom H, Chervinsky P, et al. Effects of treatment with mometa-
sone furoate dry powder inhaler in children with persistent asthma. Ann Allergy
Asthma Immunol 2006;97:67280.
104. Richter K, Kanniess F, Biberger C, et al. Comparison of the oropharyngeal de-
position of inhaled ciclesonide and fluticasone propionate in patients with
asthma. J Clin Pharmacol 2005;45:14652.
105. von Berg A, Engelstatter R, Minic P, et al. Comparison of the efficacy and
safety of ciclesonide 160 microg once daily vs. budesonide 400 microg
once daily in children with asthma. Pediatr Allergy Immunol 2007;18:
391400.
106. Vermeulen JH, Gyurkovits K, Rauer H, et al. Randomized comparison of the
efficacy and safety of ciclesonide and budesonide in adolescents with severe
asthma. Respir Med 2007;101:218291.
107. Pedersen S, Garcia Garcia ML, Manjra A, et al. A comparative study of inhaled
ciclesonide 160 microg/day and fluticasone propionate 176 microg/day in chil-
dren with asthma. Pediatr Pulmonol 2006;41:95461.
108. Gelfand EW, Georgitis JW, Noonan M, et al. Once-daily ciclesonide in children:
efficacy and safety in asthma. J Pediatr 2006;148:37783.
109. Sharek PJ, Bergman DA, Ducharme F. Beclomethasone for asthma in children:
effects on linear growth. Cochrane Database Syst Rev 1999;(3):Art. No.:
CD001282. DOI:10.1002/14651858.CD001282.
110. Long-term effects of budesonide or nedocromil in children with asthma. The
Childhood Asthma Management Program Research Group. N Engl J Med
2000;343:105463.
111. Anthracopoulos MB, Papadimitriou A, Panagiotakos DB, et al. Growth deceler-
ation of children on inhaled corticosteroids is compensated for after the first
12 months of treatment. Pediatr Pulmonol 2007;42:46570.
112. Agertoft L, Pedersen S. Effect of long-term treatment with inhaled budeso-
nide on adult height in children with asthma. N Engl J Med 2000;343:
10649.
113. Todd GR, Acerini CL, Ross-Russell R, et al. Survey of adrenal crisis associated
with inhaled corticosteroids in the United Kingdom. Arch Dis Child 2002;87:
45761.
114. Gulliver T, Morton R, Eid N. Inhaled corticosteroids in children with asthma: phar-
macologic determinants of safety and efficacy and other clinical considerations.
Paediatr Drugs 2007;9:18594.
115. Rohatagi S, Luo Y, Shen L, et al. Protein binding and its potential for eliciting
minimal systemic side effects with a novel inhaled corticosteroid, ciclesonide.
Am J Ther. 2005;12:2019.
116. Abdullah AK, Khan S. Evidence-based selection of inhaled corticosteroid for
treatment of chronic asthma. J Asthma 2007;44:112.
117. Powell H, Gibson PG. High dose versus low dose inhaled corticosteroid as initial
starting dose for asthma in adults and children. Cochrane Database Syst Rev
2003;(4):Art. No.: CD004109. DOI:10.1002/14651858.CD004109.pub2.
118. Verberne AA, Frost C, Roorda RJ, et al. One year treatment with salmeterol com-
pared with beclomethasone in children with asthma. The Dutch Paediatric
Asthma Study Group. Am J Respir Crit Care Med 1997;156:68895.
119. Bisgaard H. Effect of long-acting beta2 agonists on exacerbation rates of
asthma in children. Pediatr Pulmonol 2003;36:3918.
120. Bisgaard H, Szefler S. Long-acting beta2 agonists and paediatric asthma. Lan-
cet 2006;367:2868.
Asthma in Childhood 221
121. Ni Chroinin M, Greenstone IR, Danish A, et al. Long-acting beta2-agonists ver-
sus placebo in addition to inhaled corticosteroids in children and adults with
chronic asthma. Cochrane Database Syst Rev 2005;(4):Art. No.: CD005535.
DOI:10.1002/14651858.CD005535.
122. Ni Chroinin M, Greenstone IR, Ducharme FM. Addition of inhaled long-acting
beta2-agonists to inhaled steroids as first line therapy for persistent asthma in
steroid-naive adults. Cochrane Database Syst Rev 2004;(4):Art. No.:
CD005307. DOI:10.1002/14651858.CD005307.
123. Walters EH, Gibson PG, Lasserson TJ, et al. Long-acting beta2-agonists for
chronic asthma in adults and children where background therapy contains var-
ied or no inhaled corticosteroid. Cochrane Database Syst Rev 2007;(1):Art. No.:
CD001385. DOI:10.1002/14651858.CD001385.pub2.
124. Salpeter SR, Buckley NS, Ormiston TM, et al. Meta-analysis: effect of long-
acting beta-agonists on severe asthma exacerbations and asthma-related
deaths. Ann Intern Med 2006;144:90412.
125. Chowdhury BA. Division Director Memorandum: overview of the FDA back-
ground materials prepared for the meeting to discuss the implications of
the available data related to the safety of long acting beta-agonist broncho-
dilators. 2005. Available at: http://www.fda.gov/ohrms/dockets/ac/05/briefing/
2005-414881_03_01-FDA-Div-Dir-Memo.pdf. Accessed April 2008.
126. OByrne PM, Bisgaard H, Godard PP, et al. Budesonide/formoterol combination
therapy as both maintenance and reliever medication in asthma. Am J Respir
Crit Care Med 2005;171:12936.
127. Bisgaard H, Le Roux P, Bjamer D, et al. Budesonide/formoterol maintenance plus
reliever therapy: a new strategy in pediatric asthma. Chest 2006;130:173343.
128. Robinson DS, Campbell DA, Durham SR, et al. Systematic assessment of diffi-
cult-to-treat asthma. Eur Respir J 2003;22:47883.
129. Mash B, Bheekie A, Jones PW. Inhaled versus oral steroids for adults with
chronic asthma. Cochrane Database Syst Rev 2001;(1):Art. No.: CD002160.
DOI:10.1002/14651858.CD002160.
130. Dean T, Dewey A, Bara A, et al. Azathioprine as an oral corticosteroid sparing
agent for asthma. Cochrane Database Syst Rev 2003;(4):Art. No.: CD003270.
DOI:10.1002/14651858.CD003270.pub2.
131. Dewey A, Dean T, Bara A, et al. Chloroquine as a steroid sparing agent for
asthma. Cochrane Database Syst Rev 2003;(4):Art. No.: CD003275.
DOI:10.1002/14651858.CD003275.
132. Dewey A, Dean T, Bara A, et al. Colchicine as an oral corticosteroid sparing
agent for asthma. Cochrane Database Syst Rev 2003;(3):. DOI:10.1002/
14651858.CD003273.
133. Evans DJ, Cullinan P, Geddes DM, et al. Cyclosporin as an oral corticosteroid
sparing agent in stable asthma. Cochrane Database Syst Rev 2000;(4):Art.
No.: CD002993. DOI:10.1002/14651858.CD002993.
134. Dewey A, Bara A, Dean T, et al. Dapsone as an oral corticosteroid sparing agent
for asthma. Cochrane Database Syst Rev 2002;(4):Art. No.: CD003268.
DOI:10.1002/14651858.CD003268.
135. Davies H, Olson L, Gibson P. Methotrexate as a steroid sparing agent for asthma
in adults. Cochrane Database Syst Rev 1998;(3):Art. No.: CD000391.
DOI:10.1002/14651858.CD000391.
136. Evans DJ, Cullinan P, Geddes DM, et al. Gold as an oral corticosteroid sparing
agent in stable asthma. Cochrane Database Syst Rev 2000;(4):Art. No.:
CD002985. DOI:10.1002/14651858.CD002985.
Robinson & Van Asperen 222
137. Comet R, Domingo C, Larrosa M, et al. Benefits of low weekly doses of metho-
trexate in steroid-dependent asthmatic patients. A double-blind, randomized,
placebo-controlled study. Respir Med 2006;100:4119.
138. Niggemann B, Leupold W, Schuster A, et al. Prospective, double-blind,
placebo-controlled, multicentre study on the effect of high-dose, intravenous im-
munoglobulin in children and adolescents with severe bronchial asthma. Clin
Exp Allergy 1998;28:20510.
139. Kishiyama JL, Valacer D, Cunningham-Rundles C, et al. A multicenter, random-
ized, double-blind, placebo-controlled trial of high-dose intravenous immuno-
globulin for oral corticosteroid-dependent asthma. Clin Immunol 1999;91:12633.
140. Schwartz HJ, Hostoffer RW, McFadden ER Jr, et al. The response to intravenous
immunoglobulin replacement therapy in patients with asthma with specific anti-
body deficiency. Allergy Asthma Proc 2006;27:538.
141. Walker S, Monteil M, Phelan K, et al. Anti-IgE for chronic asthma in adults and
children. Cochrane Database Syst Rev 2006;(2):Art. No.: CD003559.
DOI:10.1002/14651858.CD003559.pub3.
142. Milgrom H, Berger W, Nayak A, et al. Treatment of childhood asthma with anti-
immunoglobulin E antibody (omalizumab). Pediatrics 2001;108:E36.
143. Wu AC, Paltiel AD, Kuntz KM, et al. Cost-effectiveness of omalizumab in adults
with severe asthma: results from the Asthma Policy Model. J Allergy Clin Immu-
nol 2007;120:114652.
144. Brown R, Turk F, Dale P, et al. Cost-effectiveness of omalizumab in patients with
severe persistent allergic asthma. Allergy 2007;62:14953.
145. Abramson MJ, Puy RM, Weiner JM. Allergen immunotherapy for asthma. Co-
chrane Database Syst Rev 2003;(4):Art. No.: CD001186. DOI:10.1002/
14651858.CD001186.
146. Shaikh WA. Immunotherapy vs inhaled budesonide in bronchial asthma: an
open, parallel, comparative trial. Clin Exp Allergy 1997;27:127984.
147. Penagos M, Passalacqua G, Compalati E, et al. Metaanalysis of the efficacy of
sublingual immunotherapy in the treatment of allergic asthma in pediatric
patients, 3 to 18 years of age. Chest 2008;133:599609.
148. Nelson HS. Allergen immunotherapy: where is it now? J Allergy Clin Immunol
2007;119:76979.
149. Kamada AK, Hill MR, Ikle DN, et al. Efficacy and safety of low-dose troleando-
mycin therapy in children with severe, steroid-requiring asthma. J Allergy Clin
Immunol 1993;91:87382.
150. Sharma S, Jaffe A, Dixon G. Immunomodulatory effects of macrolide antibiotics
in respiratory disease: therapeutic implications for asthma and cystic fibrosis.
Paediatr Drugs 2007;9:10718.
151. Seddon P, Bara A, Ducharme FM, et al. Oral xanthines as maintenance treat-
ment for asthma in children. Cochrane Database Syst Rev 2006;(1):Art. No.:
CD002885. DOI:10.1002/14651858.CD002885.pub2.
152. Bassler D, MitraA, DucharmeFM, et al. Ketotifenaloneor as additional medication
for long-term control of asthma and wheeze in children. Cochrane Database Syst
Rev 2004;(1):Art. No.: CD001384. DOI:10.1002/14651858.CD001384.pub2.
153. Andze GO, Luks FI, Bensoussan AL, et al [Role of surgical treatment of gastro-
esophageal reflux in children with severe asthma]. Pediatrie 1991;46:4514
[in French].
154. Tucci F, Resti M, Fontana R, et al. Gastroesophageal reflux and bronchial
asthma: prevalence and effect of cisapride therapy. J Pediatr Gastroenterol
Nutr 1993;17:26570.
Asthma in Childhood 223
155. Gustafsson PM, Kjellman NI, Tibbling L. A trial of ranitidine in asthmatic children
and adolescents with or without pathological gastro-oesophageal reflux. Eur
Respir J 1992;5:2016.
156. Shapiro GG, Kemp JP, DeJong R, et al. Effects of albuterol and procaterol on
exercise-induced asthma. Ann Allergy 1990;65:2736.
157. Koh MS, Tee A, Lasserson TJ, et al. Inhaled corticosteroids compared to placebo
for prevention of exercise induced bronchoconstriction. Cochrane Database Syst
Rev 2007;(3):Art. No.: CD002739. DOI:10.1002/14651858.CD002739.pub3.
158. Pedersen S, Hansen OR. Budesonide treatment of moderate and severe asthma
in children: a dose-response study. J Allergy Clin Immunol 1995;95:2933.
159. Spooner CH, Saunders LD, Rowe BH. Nedocromil sodium for preventing exer-
cise-induced bronchoconstriction. Cochrane Database Syst Rev 2002;(1):Art.
No.: CD001183. DOI:10.1002/14651858.CD001183.
160. Pearlman DS, Ostrom NK, Bronsky EA, et al. The leukotriene D4-receptor antag-
onist zafirlukast attenuates exercise-induced bronchoconstriction in children.
J Pediatr 1999;134:2739.
161. Melo RE, Sole D, Naspitz CK. Exercise-induced bronchoconstriction in children:
montelukast attenuates the immediate-phase and late-phase responses.
J Allergy Clin Immunol 2003;111:3017.
162. Kemp JP, Dockhorn RJ, Shapiro GG, et al. Montelukast once daily inhibits exer-
cise-induced bronchoconstriction in 6- to 14-year-old children with asthma.
J Pediatr 1998;133:4248.
163. KimJH, LeeSY, KimHB, et al. Prolongedeffect of montelukast inasthmaticchildren
with exercise-induced bronchoconstriction. Pediatr Pulmonol 2005;39:1626.
164. Stelmach I, Grzelewski T, Majak P, et al. Effect of different antiasthmatic treatments
on exercise-induced bronchoconstriction in children with asthma. J Allergy Clin
Immunol 2008;121:3839.
165. Cheng J, Tao Pan, Ye GH, et al. Calorie controlled diet for chronic asthma.
Cochrane Database Syst Rev 2003;(2):Art. No.: CD004674. DOI:10.1002/
14651858.CD004674.pub2.
166. AllamMF, LucenaRA. Seleniumsupplementationfor asthma. CochraneDatabase
Syst Rev 2004;(2):Art. No.: CD003538. DOI:10.1002/14651858.CD003538.pub2.
167. Thien FCK, De Luca S, Woods R, et al. Dietary marine fatty acids (fish oil) for
asthma in adults and children. Cochrane Database Syst Rev 2002;(2):Art.
No.: CD001283. DOI:10.1002/14651858.CD001283.
168. Ram FSF, Ardern KD. Dietary salt reduction or exclusion for allergic asthma.
Cochrane Database Syst Rev 2004;(2):Art. No.: CD000436. DOI:10.1002/
14651858.CD000436.pub2.
169. RamFS, Ardern KD. Tartrazine exclusion for allergic asthma. Cochrane Database
Syst Rev 2001;(4):Art. No.: CD000460. DOI:10.1002/14651858.CD000460.
170. Ram FSF, Rowe BH, Kaur B. Vitamin C supplementation for asthma.
Cochrane Database Syst Rev 2004;(3):Art. No.: CD000993. DOI:10.1002/
14651858.CD000993.pub2.
171. Shenfield G, Lim E, Allen H. Survey of the use of complementary medicines and
therapies in children with asthma. J Paediatr Child Health 2002;38:2527.
172. McCarney RW, Brinkhaus B, Lasserson TJ, et al. Acupuncture for chronic
asthma. Cochrane Database Syst Rev 2003;(3):Art. No.: CD000008.
DOI:10.1002/14651858.CD000008.pub2.
173. McCarney RW, Linde K, Lasserson TJ. Homeopathy for chronic asthma.
Cochrane Database Syst Rev 2004;(1):Art. No.: CD000353. DOI:10.1002/
14651858.CD000353.pub2.
Robinson & Van Asperen 224
174. Hondras MA, Linde K, Jones AP. Manual therapy for asthma. Cochrane Database
Syst Rev 2005;(2):Art. No.: CD001002. DOI:10.1002/14651858.CD001002.pub2.
175. Holloway E, Ram FSF. Breathing exercises for asthma. Cochrane Database Syst
Rev 2004;(1):Art. No.: CD001277. DOI:10.1002/14651858.CD001277.pub2.
176. Dennis J, Cates CJ. Alexander technique for chronic asthma. Cochrane Database
Syst Rev 2000;(2):Art.No.:CD000995. DOI:10.1002/14651858.CD000995.
177. Slader CA, Reddel HK, Spencer LM, et al. Double blind randomised controlled
trial of two different breathing techniques in the management of asthma. Thorax
2006;61:6516.
178. Ram FSF, Wellington SR, Barnes NC. Inspiratory muscle training for asthma.
Cochrane Database Syst Rev 2003;(3):Art. No.: CD003792. DOI:10.1002/
14651858.CD003792.
179. Ram FSF, Robinson SM, Black PN, et al. Physical training for asthma. Cochrane
Database Syst Rev 2005;(4):Art. No.: CD001116. DOI:10.1002/
14651858.CD001116.pub2.
180. Gtzsche PC, Johansen HK, Schmidt LM, et al. House dust mite control mea-
sures for asthma. Cochrane Database Syst Rev 2004;(4):Art. No.: CD001187.
DOI:10.1002/14651858.CD001187.pub2.
181. Singh M, Bara A, Gibson P. Humidity control for chronic asthma. Cochrane Database
Syst Rev 2002;(1):Art. No.: CD003563. DOI:10.1002/14651858.CD003563.
182. Blackhall K, Appleton S, Cates CJ. Ionisers for chronic asthma. Cochrane Database
Syst Rev 2003;(2):Art. No.: CD002986. DOI:10.1002/14651858.CD002986.
183. Kilburn S, Lasserson TJ, McKean M. Pet allergen control measures for allergic
asthma in children and adults. Cochrane Database Syst Rev 2001;(1):Art.
No.: CD002989. DOI:10.1002/14651858.CD002989.
184. Campbell F, Gibson P. Feather versus non-feather bedding for asthma. Cochrane
Database Syst Rev 2000;(4):Art. No.: CD002154. DOI:10.1002/14651858.
CD002154.
185. Beamon S, Falkenbach A, Fainburg G, et al. Speleotherapy for asthma. Cochrane
Database Syst Rev 2001;(2):Art. No.: CD001741. DOI:10.1002/14651858.
CD001741.
186. Arshad SH, Bateman B, Sadeghnejad A, et al. Prevention of allergic disease
during childhood by allergen avoidance: the Isle of Wight prevention study.
J Allergy Clin Immunol 2007;119:30713.
187. Chan-Yeung M, Ferguson A, Watson W, et al. The Canadian childhood asthma
primary prevention study: outcomes at 7 years of age. J Allergy Clin Immunol
2005;116:4955.
188. Marks GB, Mihrshahi S, Kemp AS, et al. Prevention of asthma during the first 5
years of life: a randomized controlled trial. J Allergy Clin Immunol 2006;118:
5361.
189. Kramer MS, Matush L, Vanilovich I, et al. Effect of prolonged and exclusive
breast feeding on risk of allergy and asthma: cluster randomised trial. BMJ
2007;335:815.
190. DiFranza JR, Aligne CA, Weitzman M. Prenatal and postnatal environmental
tobacco smoke exposure and childrens health. Pediatrics 2004;113:100715.
191. Warner JO. A double-blinded, randomized, placebo-controlled trial of cetirizine in
preventingtheonset of asthmainchildrenwithatopicdermatitis: 18months treatment
and 18 months posttreatment follow-up. J Allergy Clin Immunol 2001;108:92937.
192. Yunginger JW, Reed CE, OConnell EJ, et al. A community-based study of the
epidemiology of asthma. Incidence rates, 19641983. Am Rev Respir Dis
1992;146:88894.
Asthma in Childhood 225
193. Bisgaard H, Hermansen MN, Loland L, et al. Intermittent inhaled corticosteroids
in infants with episodic wheezing. N Engl J Med 2006;354:19982005.
194. Murray CS, Woodcock A, Langley SJ, et al. Secondary prevention of asthma by
the use of Inhaled Fluticasone propionate in Wheezy infants (IFWIN): double-
blind, randomised, controlled study. Lancet 2006;368:75462.
195. Cates CJ, Jefferson TO, Bara AI, et al. Vaccines for preventing influenza in peo-
ple with asthma. Cochrane Database Syst Rev 2003;(4):Art. No.: CD000364.
DOI:10.1002/14651858.CD000364.pub2.
196. Carroll W, Burkimsher R. Is there any evidence for influenza vaccination in
children with asthma? Arch Dis Child 2007;92:6445.
197. Influenza vaccination coverage among children with asthmaUnited States
200405 influenza season. MMWR Morb Mortal Wkly Rep 2007;56:1936.
198. Sheikh A, Alves B, Dhami S. Pneumococcal vaccinefor asthma. CochraneDatabase
Syst Rev 2002;(1):Art. No.: CD002165. DOI:10.1002/14651858.CD002165.
199. Wolf FM, Guevara JP, Grum CM, et al. Educational interventions for asthma in
children. Cochrane Database Syst Rev 2002;(4):Art. No.: CD000326.
DOI:10.1002/14651858.CD000326.
200. Cano-Garcinuno A, Diaz-Vazquez C, Carvajal-Uruena I, et al. Group education on
asthmafor childrenandcaregivers: arandomized, controlledtrial addressingeffects
on morbidity and quality of life. J Investig Allergol Clin Immunol 2007;17:21626.
201. Bhogal S, Zemek R, Ducharme FM. Written action plans for asthma in children.
Cochrane Database Syst Rev 2006;(3):Art. No.: CD005306. DOI:10.1002/
14651858.CD005306.pub2.
202. Wensley D, Silverman M. Peak flow monitoring for guided self-management in
childhood asthma: a randomized controlled trial. Am J Respir Crit Care Med
2004;170:60612.
203. Chang AB, Taylor B, Masters IB, et al. Indigenous healthcare worker involve-
ment for indigenous adults and children with asthma. Cochrane Database
Syst Rev 2007;(4):Art.No.: CD006344. DOI:10.1002/14651858.CD006344.pub2.
204. Yorke J, Fleming S, Shuldham C. Psychological interventions for children with
asthma. Cochrane Database Syst Rev 2005;(4):Art. No.: CD003272.
DOI:10.1002/14651858.CD003272.pub2.
205. Yorke J, Shuldham C. Family therapy for asthma in children. Cochrane Database
Syst Rev 2005;(2):Art.No.:CD000089. DOI:10.1002/14651858.CD000089.pub2.
206. PetskyHL, KynastonJA, Turner C, et al. Tailoredinterventionsbasedonsputumeosin-
ophils versus clinical symptoms for asthma in children and adults. Cochrane Data-
base Syst Rev 2007;(2):. DOI:10.1002/14651858.CD005603.pub2.
207. Zacharasiewicz A, Erin EM, Bush A. Noninvasive monitoring of airway inflamma-
tion and steroid reduction in children with asthma. Curr Opin Allergy Clin Immu-
nol 2006;6:15560.
Robinson & Van Asperen 226
Congeni tal Ai rway
Lesi ons and Lung
Di sease
Ian Brent Masters, MBBS, FRACP, PhD
THE RELEVANCE OF CONGENITAL AIRWAYAND LUNG LESIONS FOR PEDIATRICIANS
Congenital airway and cystic lung lesions are not common in pediatrics.
13
Despite the
low incidence of these lesions, pediatricians are likely to encounter this type of disor-
der through common respiratory symptoms and signs (respiratory noises, tachypnea,
and cough). For pediatricians, pediatric pulmonologists, radiologists, otolaryngolo-
gists, thoracic surgeons, and intensive care staff, the management and care of
children who have these lesions can require considerable expenditures of time and
other resources within a tertiary care center.
4,5
Specifically, most children who have
suspected airway lesions require a laryngoscopy and bronchoscopy and detailed
radiologic assessments, and some need intensive care and/or operative manage-
ment.
6,7
Even though there are no published health economics data for this level of
care, the health care costs for the diagnostic and long-term management of these
disorders are likely to be large.
Congenital lesions related to the lung can be classified as (1) parenchymal, (2) air-
way, (3) vascular (arterial/venous), and (4) lymphatic lesions. Upper airway structural
disorders are the most common disorders encountered, with laryngomalacia being
the most common; subglottic stenosis, subglottic hemangiomas, subglottic cystic
lesions, vocal cord paralysis, and webs are less common. The lower airway disorders
are the malacia disorders, airway stenoses, hypoplastic disorders or small airways,
ectopic and accessory bronchi, bronchial atresia, and diverticulum and airway distor-
tion disorders.
13
Finally, parenchymal lung lesions such as cystic adenomatoid
malformation, sequestrations, foregut malformations, and congenital lobar emphy-
sema also can be seen as structural lesions of the distal airways and parenchyma.
8
Queensland Childrens Respiratory Centre, Royal Children Hospital, Herston, 4029, Brisbane,
Queensland, Australia
E-mail address: brent_masters@health.qld.gov.au
KEYWORDS
Laryngomalacia
Tracheobronchomalacia
Cystic adenomatoid malformation
Pediatr Clin N Am 56 (2009) 227242
doi:10.1016/j.pcl.2008.10.006 pediatric.theclinics.com
0031-3955/08/$ see front matter 2009 Elsevier Inc. All rights reserved.
Pulmonary vascular and lymphatic anomalies include pulmonary arteriovenous
malformations
9
and primary and secondary lymphangiectasia disorders.
1012
This article describes some of the many diagnostic and management issues that sur-
round the most common of these disorders: laryngomalacia, tracheobronchomalacia
disorders, andthecysticlesions, particularlycysticadenomatoidmalformation. Manage-
ment of these conditions generally is not evidenced based, but most of the current
approaches to care have stood the test of time and have very good outcomes.
LARYNGOMALACIA
Incidence
The incidence of laryngomalacia is not known, but it has long been recognized as the
most common cause of chronic or persistent stridor in infants. Laryngomalacia also
may occur in late-onset forms in the child and adult populations with various levels
of associated feeding difficulties, disordered breathing during sleep, and exercise-
induced laryngeal obstruction.
1315
Pathogenesis
The pathogenesis of laryngomalacia is not known, but familial cases and cases asso-
ciated with a variety of syndromes have been described,
1620
thus suggesting
a potential genetic basis.
The morphologic descriptions of laryngomalacia consist of an omega-shaped
epiglottis, short aryepiglottic folds, and varying degrees of arytenoid and arytenoid
mucosal prolapse and of posterior displacement of the epiglottis. Laryngomalacia
has been classified as type 1, 2, and 3, depending the involvement of the three
components.
21,22
The functional elements of these changes have resulted in many
theories about the cause of laryngomalacia, but it is possible that both the anatomic
appearances and functional elements result fromgenetic factors producing abnormal-
ities and maturational delays in the sensorineural function of the larynx, because
symptoms resolve in most children by 2 years of age.
23
Classification of Laryngomalacia
Laryngomalacia generally is classified by its laryngoscopic appearance. In the most
commonly used classification, prolapse of the mucosa overlying the arytenoid carti-
lages is designated type 1; foreshortened aryepiglottic folds are designated type 2;
and posterior displacement of the epiglottis is designated type 3. Various combina-
tions of these types may be seen,
21
and concomitant pharyngeal collapse also may
occur.
24
In addition to this classification, clinical classifications have been used to
help direct therapy. In neonates and infants these classifications have centered on
stridor, the severity of airway obstruction, and the impact on respiratory function
and general well being, development, and growth.
25
In late-onset groups, from child-
hood to adulthood, laryngomalacia has been described by its association with feeding
disorders (feeding-disordered laryngomalacia), sleep-disordered breathing (sleep-
disordered laryngomalacia), and exercise (exercise-induced laryngomalacia).
15
Evidence-based management of laryngomalacia
Evidence-based management recommendations using integrated and validated
algorithms for diagnosis and management are lacking for almost all aspects of care
of laryngomalacia. Despite these apparent deficits, current management of laryngo-
malacia depends on an accurate diagnosis and an assessment of the clinical impact
on respiratory function and general features of growth and neurodevelopmental
Masters 228
status. In addition, concomitant management of reflux-related diseases is helpful in
some patients.
26
The following general approach to the assessment and management
of stridor and laryngomalacia is suggested:
1. Define the timing of the stridor (eg, inspiratory, expiratory, biphasic)
2. Classify the severity of obstruction
3. Assess for concomitant factors
Syndromes
Chronic cough
Swallowing difficulties, general growth such as weight gain
Cutaneous disorders
Neurodevelopmental status of the infants
When stridor is inspiratory, the degree of obstruction is minimal, and there are no
concomitant factors, management should be expectant observation over time.
If other factors are found, referral to a pediatric pulmonologist or otolaryngologist is
recommended. The ongoing management for the different severities of laryngomala-
cia is described in the following sections.
Mild laryngomalacia Mild laryngomalacia is characterized by isolated, intermittent,
cogwheel inspiratory stridor with minimal work of breathing (recession/retractions)
and normal growth and development. Symptoms and signs such as concomitant
coughing, wheezing, vocal changes, swallowing or feeding difficulties, skin lesions,
and cardiovascular or constitutional symptoms invariably denote other disorders. In
most infants signs resolve progressively over the first 2 years of life. Parental reassur-
ance and regular follow-up assessments should be performed to support the parent
and to ensure appropriate resolution of the childs problems.
Moderate laryngomalacia Moderate laryngomalacia is characterized by continual
stridor and significant work of breathing (recession/retractions) without other consti-
tutional symptoms and signs. Children should have a chest radiograph and an airway
assessment with laryngoscopy and bronchoscopy. Radiographic investigations in
the form of airway fluoroscopy screening are of limited specific diagnostic value
(evidence grade 5 very low). A barium-swallow esophagogram may provide impor-
tant specific diagnostic information concerning the swallow mechanisms, particu-
larly when vascular rings and slings are suspected (evidence grade 5 very low).
Laryngoscopy and bronchoscopy provide the specifics of diagnosis that surround
the differential diagnoses of lingual cysts, vocal cord disorders, hemangiomas and
cysts, and tracheobronchial abnormalities. In most children, symptoms resolve by
2 years of age. Once the diagnosis has been affirmed by the diagnostic procedures,
parental reassurance and regular follow-up assessments should be performed to
support the parents and ensure appropriate progress and resolution of the childs
problems.
Severelaryngomalacia Severe laryngomalacia is characterized by continuous inspiratory
stridor, increased work or breathing, varying degrees of respiratory failure (severe ob-
struction) requiring oxygen therapy and/or airway support, and constitutional symptoms
such as failure to thrive or developmental delay. Surgical interventions are likely to be
required. The surgical interventions are predominantly aryepiglottoplasties (supraglotto-
plasty) performed by a variety of techniques including laser (evidence grade 5
low).
15,21,23,27
Tracheostomy is rarely required. Once the diagnosis has been affirmed
by the diagnostic procedures and interventions have taken place, regular follow-up
Congenital Airway Lesions and Lung Disease 229
assessments should be performed to support the parents and ensure appropriate prog-
ress and resolution of the childs problems. Supraglottoplasty does not necessarily re-
sult in a total and sustained loss of stridor, but it usually reduces the work of breathing
appreciably. Successful feeding may be slower to recover (Table 1).
21,27
TRACHEOBRONCHOMALACIA DISORDERS
Incidence
The incidence of tracheobronchomalacia disorders is thought to range between
1:1500 and 1:2500 children.
29,30
Despite this relatively low incidence, these lesions
are encountered commonly in pediatric bronchoscopic practices, particularly when
investigating stridulous, recurrent, or persistent wheezy and rattly conditions and
chronic cough, especially in association with congenital heart disease and syndromic
conditions.
20,31,32
Marchant and colleagues
33
have shown that a significant number of
children who have isolated chronic cough also have malacia disorders. In addition
Chang and colleagues
34
have shown that an unusual quality of cough, such as a vibra-
tory or brassy cough, has high levels of association with bronchoscopically proven
malacia. Despite these advances in knowledge, incorrect diagnoses brought about
by attributing these disorders to asthma are common in both pediatric
35,36
and adult
practice.
37
Therefore it is likely that the estimated incidence of malacia of 1:1500 to
1:2500 significantly underestimates the true incidence. Consequently, pediatricians
need to remain vigilant and cognizant of this diagnosis.
Pathogenesis
The pathogenesis of tracheobronchomalacia disorders is not known, but indirect
associative evidence indicates that it is likely that these disorders develop during fetal
life around 5 to 8 weeks after conception.
3841
Molecular genetic studies of fetal lung and airway development indicate signaling
pathway abnormalities involving a variety of genes
42
including the Hox, Shh, and Gli
genes.
4349
The Sox9 gene is essential to the formation of cartilage both spatially
and temporally,
5
and Shh (sonic hedgehog) expression is important to the formation
of cartilage rings.
40
In addition, alterations in the timing of expression or in the compounds that form the
structural support of the airway cartilagethe collagens and aggrecanscould alter
the mechanical properties of tracheal cartilage.
5054
Type II collagen has the dominant
role in tensile properties of cartilage, whereas type I collagen seems to be more impor-
tant in shaping the airway.
51,5355
The aggrecans, which offer the airway cartilage
compressive resilience, are vulnerable to proteases, including the metalloproteases
that abound during fetal lung growth and development.
50,52,56
Lysyl oxidases,
Table1
Outline of the evidence for management of laryngomalacia
Medication/Intervention Recommendation
Grading of
Recommendation
(Based on Evidence
of Benefit)
Quality of
Supporting
Evidence
Airway fluoroscopy screen
28
Not recommended Low Low
Supraglottoplasty
27
Recommended in
severe cases only
Moderate Low
Investigation for GOR
26
Recommended in
symptomatic patients
Moderate Low
Masters 230
a copper-dependent extracellular enzyme group, are important to the tensile proper-
ties of collagen because they catalyze the formation of lysine and hydroxy-lysine
cross-links in collagen.
57
Bone morphogenetic protein expression also is important
for lysyl oxidase gene expression and activation, and it currently is thought to be im-
portant in tracheoesophageal fistula and malacia.
42,5863
The anatomic distribution of different collagen types within the large airways com-
plicates the issues further, because collagen type I, II, and III patterns of distribution do
change temporarily and regionally from the neonatal period to childhood.
64
Just how
gene expression controls these transitions is not known, but, again, alterations to
these processes could render the airway vulnerable, both temporally and spatially,
to the formation of malacia lesions.
Classification of Malacia Lesions
The term malacia is derived from Greek word malakia, meaning soft. In the
respiratory context it infers a sustained softening of the airway cartilage that results
in a dynamic change in the appearance of the airway during the respiratory cycle or
during forced breathing maneuvers.
4
Malacia has been classified in a variety of
ways, but none has been accepted universally. These classifications include major
airway collapse,
4
excessive dynamic airway collapse,
37,65
and tracheal dyskine-
sia;
6668
where a 50% reduction in cross-sectional area is considered significant.
69
Qualified descriptions (eg, consistent with innominate artery compression or Eiffel
Tower appearance consistent with double aortic arch)
7072
and the designations pri-
mary malacia and secondary malacia also are used.
73,74
The degree of malacia is measured best with bronchoscopy assessment at the end-
expiratory point when the lumen is at its narrowest.
4,7579
Tracheomalacia can be
defined and measured using CT,
8086
but this approach has a number of limitations
in pediatrics, and publications are limited to anecdotal case reports.
8791
Bronchoma-
lacia (lobar and segmental) is not well defined by CT.
Evidence-based management of tracheobronchomalacia
Diagnosis Essentially, the management of tracheobronchomalacia disorders is based
on expert opinion derived from anecdotal experiences using the levels of severity of
the symptoms and signs, the bronchoscopic appearance of the lesions across the re-
spiratory cycle, and other investigations to define the spectrum of illness from mild to
severe. Currently, diagnostic and management algorithms are being developed, but
none has been tested rigorously (evidence grade 5 very low).
65,92
These approaches
Fig.1. Bronchoscopic images of malacia (tracheomalacia) taken with the bronchoscope held
10 mm from the anterior aspect of the lesion in low-light conditions to enhance the visual
definition of the lesion. (A) Anterior flattening of the trachea at the junction of the middle
and lower third of the trachea. (B) Anterior flattening with anterior slope from left to right.
(C) Tracheomalacia: saber or triangular shape.
Congenital Airway Lesions and Lung Disease 231
are necessary, because the loss of cross-sectional area in the lesions does not seem
to correlate well with symptoms and signs (evidence grade 5 moderate).
79,93
The diagnosis should be considered in children who have persistent or protracted
recurrent airway symptoms (persistent or recurrent wet cough, unusual cough, ex-
piratory stridor, wheeze, rattliness or rattly respirations, dyspnea/respiratory distress),
recurrent protracted bacterial bronchitis, pneumonia (particularly with atypical radio-
graphic features such as persistent or recurrent collapse), localized gas trapping,
and unusual radiographic densities. Suspicion of this diagnosis also should be
increased in children who have syndromes involving cardiac disorders, non-cystic
fibrosis bronchiectatic states, and asthmalike states in which there has not been
an adequate response to medications (evidence grade 5 moderate).
33,9497
All
children in whom the diagnosis is suspected should have simple radiographic assess-
ments, and some will require bronchoscopic assessments and more invasive and
detailed radiographic assessments such as a contrast swallow, CT with contrast, or
MRI (evidence grade 5 very low).
Mild tracheobronchomalacia The mild end of the tracheobronchomalacia spectrum
usually ranges from trivial rattly respirations and intermittent illnesses to more trouble-
some recurrent bronchitic illnesses, recurrent croup, recurrent cough, and wheezy ill-
nesses.
33,6668,94,95
Even in this group of children, unpredictable and severe
obstructive episodes may require intensive care management. The management of
patients who have recurrent bronchitis or protracted bronchitis has not been studied
in any formal sense,
98
but there is little doubt that these illnesses have a significant
Fig. 3. (A) The pars is bulging into the lumen of right and left main stem bronchi with exces-
sive dynamic collapse or tracheal dyskinesia. (B) Crescent-shaped tracheomalacia with exten-
sion to and complete occlusion of the right main stem bronchi. (C) H-shaped
tracheoesophageal fistula with a catheter and posterior malacia. The catheter was passed
through the working channel of the bronchoscope and placed into and through the fistula.
In this case the pars was heaped up in the extrathoracic trachea before the passage of the
catheter.
Fig. 2. Tracheomalacia. (A) Note localized anterior flattening at the junction of the mid and
lower thirds of the trachea with maintenance of the posterior shape. (B) Note the anterior
flattening at the carina and lateral to medial apposition of the origin of left main stem
bronchus. (C) Note anterior flattening and some bulging of the pars with anterior-to-poste-
rior apposition of surfaces on the right side.
Masters 232
effect on the psychologic functioning of both the child and families involved
99
(evidence grade 5 high). Antibiotics and chest physiotherapy along with conventional
asthma medications, particularly bronchodilators and oral steroids, are the commonly
used modes of treatment
36
(evidence grade 5 very low). Evidence-based information
is lacking for these modes of treatment except salbutamol
100
(evidence grade 5 low),
for which the benefits of outcome are inconclusive. Because children treated with oral
steroids may experience significant side effects, this practice, in particular, should be
evaluated thoroughly by evidence-based methodologies.
Moderatetracheobronchomalacia For children who have intermittent severe obstruction
or moderate sustained obstruction, management usually involves supportive thera-
pies such as subnasal oxygen and continuous positive airway pressure (CPAP) or
bi-level positive airway pressure (BiPAP) during sleep and with intercurrent illness
(evidence grade 5 very low).
101104
Severe tracheobronchomalacia At the severe end of the spectrum, with sustained and
life-threatening airway obstruction that necessitates intensive care management
with intubation, surgery has been the most common approach because of its potential
to be curative without the need for ongoing supportive care.
105
The surgical ap-
proaches include aortopexy,
105107
tracheopexy, stent placement,
7
correction of vas-
cular deformities, and correction of existing cardiac defects, when possible.
108112
The outcome of these approaches has been defined by case series; these approaches
generally result in functional improvement even though the anatomic repair sometimes
is incomplete or nonsustained. Many difficulties have been reported with stent
Fig. 5. Bronchomalacia: left main stem malacia. (A) Proximal. Note a rotated view and com-
plete closure of the medial aspect of the left main stem (anterior/posterior surface apposi-
tion). (B) Midpoint. Note incomplete closure of the left main stem (superior/inferior surface
apposition) forming a crescent appearance. (C) Distal. Note incomplete closure of the left
main stem (superior/inferior surface apposition) forming a triangular appearance with the
left upper lobe visible at 12 oclock.
Fig. 4. Tracheomalacia. (A) Note the anterior flattening forming a triangular appearance
from left to right. (B) Eiffel tower or equilateral triangular appearance consistent with dou-
ble aortic arch. (C) Note the anterior flattening forming a triangular appearance from right
to left.
Congenital Airway Lesions and Lung Disease 233
placement, and benefits do not necessarily justify the potential problems in mainte-
nance and removal.
7
Not all reports of surgery have included ventilated patients,
and none of the surgical series has reported any detailed clinical assessments of se-
verity or quantified measurements of the malacia. It is difficult to attribute the entire
outcome of the operations to the reduction in airway resistance, particularly because
the cross-sectional area of lesions does not correlate well with measured illness
profiles,
79,93
and in infants who have malacia a complex interrelationship exists
between lung volumes and flow and resistance measurements (evidence grade 5
moderate).
103
Despite these operative approaches, some children require long-term
tracheostomy and pressure support in the form of CPAP or BiPAP. Deaths also
have been recorded within this group of severely ill patients.
113
Advice to parents and caregivers The advice provided to parents and other health
workers is important for the ongoing management of children who have malacia
disorders. Parents often seem to have little or no understanding of the condition,
especially when a child has a long-standing diagnosis of asthma. Therefore this author
bases the general advice to parents and children around improving understanding of
the disorder through visual imagery by using bronchoscopic images such as those in
Figs. 1 through 8. In addition, the association between the dynamics of the lesions and
symptoms and signs of the illness is explained. Furthermore, the natural history is
explained. In particular, the caregivers are informed that the lesions tend to improve
with increasing age and that only a small percentage of lesions remain the same or
deteriorate over time, but the characteristics of the lesions that improve are not known
(evidence grade 5 very low).
79
Generally children who have malacia have higher rela-
tive risks of respiratory illness, greater symptom levels, and a tendency to more
protracted recovery than normal controls during infancy and early childhood (evidence
Fig. 7. Bronchomalacia. (A) Right main stem is flattened in the anterior/posterior aspects to
produce a key-hole appearance. (B) Right upper lobe is crescent shaped with complete clo-
sure. (C) Right middle lobe has a slitlike appearance with the airway almost completely
closed.
Fig. 6. Bronchomalacia. (A) Left upper lobe is flattened to produce a slit like appearance. (B)
The left lower lobe has a circumferential appearance, while the left upper lobe appears
normal but small. (C) Crescent-like appearance of left lower lobe orifice.
Masters 234
grade 5 moderate).
93
Treatment options and their limitations also are explained and
reiterated during reviews (evidence grade 5 very low). Regular patient reviews also
may have an important role in reducing anxieties, in reducing ad hoc medical visits
and hospitalizations, and in regulating or removing unnecessary therapies (evidence
grade 5 very low) (Table 2).
99
CYSTIC LUNG DISORDERS
Cystic lung disorders include cystic adenomatoid malformation, extra lobar seques-
tration, bronchopulmonary foregut malformations, bronchial atresia, and lobar emphy-
sema. There is considerable overlap among these conditions.
116,117
Fig. 8. Secondary tracheomalacia. Anterior cartilages are depressed to the posterior trachea
by the angle of the tracheostomy tube.
Table 2
Outline of the evidence for management of tracheobronchomalacia disorders
Medication/Intervention Recommendation
Grading of
Recommendation
(Based on Evidence
of Benefit)
Quality of Supporting
Evidence
Inhaled beta-2 agonists
100
Not routinely
recommended
Moderate Low
Inhaled or oral
corticosteroids
36
Not routinely
recommended
Low Low
Antibiotics
114
Recommended for
protracted bronchitis
Low Low
Physiotherapy Recommended Low Low
Surgery
105,106,115
Recommended in
severe cases
Low Low
Congenital Airway Lesions and Lung Disease 235
Incidence
The incidence of cystic lesions of the lung is not known, and the lesions may be
subclinical across life, but they generally are regarded as rare.
8,118120
Pathogenesis
Molecular genetic evidence indicates congenital cyst adenomatoid malformation
(c-CAM) and other cystic disorders are associated with aberrations in signaling path-
way genes, in particular Hoxb-5, which is important for the proliferation and patterning
of the last seven subdivisions of the smaller airways,
121
fibroblast growth factor,
122
and fatty acid binding protein.
123
Classification
c-CAM is classified pathologically by the diameter of the cystic lesions. Type 1 cysts
are 2 to 10 mm in diameter, type 2 cysts are 0.5 to 2 mm, and type 3 cysts are micro-
scopic glandlike and bronchiole-like structures.
118
These cystic structures may be liq-
uid or gas filled. There is no specific clinical classification, but they may be identified as
a result of antenatal ultrasound assessments, in utero problems such a hydrops and
pleural effusions, respiratory distress in the neonatal period with either radiodensities
or gas-trapping radiologic appearances, atypical or recurrent pneumonia/abscess,
gas-leak disorders, or as incidental or unsuspected radiologic findings in children
and adults.
8,120
Evidence-based management of congenital cystic lung disorders
Management depends on the timing of diagnosis, the severity of respiratory illness, or
the likelihood of respiratory illnesses. Surgical removal of the lesions or lobe involved
by open or thoracoscopic techniques is the general approach.
124126
Controversy
exists about the conservative management of asymptomatic postnatal diagnoses of
c-CAM and extra lobar sequestration; however, congenital lobar emphysema may re-
solve spontaneously, so an observant approach is justified (evidence grade 5 very
low).
119
Longitudinal research is required for these disorders.
REFERENCES
1. Landing BH, Dixon LG. Congenital malformations and genetic disorders of the
respiratory tract (larynx, trachea, bronchi, and lungs). Am Rev Respir Dis
1979;120(1):15185.
2. Chen JC, Holinger LD. Congenital tracheal anomalies: pathology study using se-
rial macrosections and review of the literature. Pediatr Pathol 1994;14(3):51337.
3. Chen JC, Holinger LD. Congenital laryngeal lesions: pathology study using serial
macrosections and review of the literature. Pediatr Pathol 1994;14(2):30125.
4. Mair EA, Parsons DS. Pediatric tracheobronchomalacia and major airway col-
lapse. Ann Otol Rhinol Laryngol 1992;101(4):3009.
5. Elluru RG, Whitsett JA. Potential role of Sox9 in patterning tracheal cartilage ring
formation in an embryonic mouse model. Arch Otolaryngol Head Neck Surg
2004;130(6):7326.
6. Altman KW, Wetmore RF, Marsh RR. Congenital airway abnormalities in patients
requiring hospitalization. Arch Otolaryngol Head Neck Surg 1999;125(5):5258.
7. Pillai JB, Smith J, Hasan A, et al. Review of pediatric airway malacia and its man-
agement, with emphasis on stenting. Eur J Cardiothorac Surg 2005;27(1):3544.
Masters 236
8. Berrocal T, Madrid C, Novo S, et al. Congenital anomalies of the tracheobron-
chial tree, lung, and mediastinum: embryology, radiology, and pathology. Radio-
graphics 2004;24(1):e17.
9. Liechty KW, Flake AW. Pulmonary vascular malformations. Semin Pediatr Surg
2008;17(1):916.
10. Barker PM, Esther CR Jr, Fordham LA, et al. Primary pulmonary lymphangiecta-
sia in infancy and childhood. Eur Respir J 2004;24(3):4139.
11. Esther CR Jr, Barker PM. Pulmonary lymphangiectasia: diagnosis and clinical
course. Pediatr Pulmonol 2004;38(4):30813.
12. Bellini C, Boccardo F, Campisi C, et al. Congenital pulmonary lymphangiectasia.
Orphanet J Rare Dis 2006;1:43.
13. Smith GJ, Cooper DM. Laryngomalacia and inspiratory obstruction in later child-
hood. Arch Dis Child 1981;56(5):3459.
14. Hoeve LJ, Rombout J. Pediatric laryngobronchoscopy. 1332 procedures stored
in a data base. Int J Pediatr Otorhinolaryngol 1992;24(1):7382.
15. Richter GT, Rutter MJ, deAlarcon A, et al. Late-onset laryngomalacia: a variant of
disease. Arch Otolaryngol Head Neck Surg 2008;134(1):7580.
16. Amin MR, Isaacson G. State-dependent laryngomalacia. Ann Otol Rhinol Lar-
yngol 2007;106(11):88790.
17. Bent J. Pediatric laryngotracheal obstruction: current perspectives on stridor.
Laryngoscope 2006;116(7):105970.
18. Jacobs IN, Gray RF, Todd NW. Upper airway obstruction in children with Down
syndrome. Arch Otolaryngol Head Neck Surg 1996;122(9):94550.
19. Markert ML, Majure M, Harville TO, et al. Severe laryngomalacia and broncho-
malacia in DiGeorge syndrome and CHARGE association. Pediatr Pulmonol
1997;24(5):3649.
20. Masters IB, Chang AB, Patterson L, et al. Series of laryngomalacia, tracheoma-
lacia, and bronchomalacia disorders and their associations with other conditions
in children. Pediatr Pulmonol 2002;34(3):18995.
21. Olney DR, Greinwald JH Jr, Smith RJ, et al. Laryngomalacia and its treatment.
Laryngoscope 1999;109(11):17705.
22. Cicekcibasi AE, Keles B, Uyar M. The morphometric development of the fetal lar-
ynx during the fetal period. Int J Pediatr Otorhinolaryngol 2008;72(5):68391.
23. Thompson DM. Abnormal sensorimotor integrative function of the larynx in con-
genital laryngomalacia: a new theory of etiology. Laryngoscope 2007;117(6 Pt 2
Suppl 114):133.
24. Shatz A, Goldberg S, Picard E, et al. Pharyngeal wall collapse and multiple syn-
chronous airway lesions. Ann Otol Rhinol Laryngol 2004;113(6):4837.
25. Shah UK, Wetmore RF. Laryngomalacia: a proposed classification form. Int J Pe-
diatr Otorhinolaryngol 1998;46(12):216.
26. Giannoni C, Sulek M, Friedman EM, et al. Gastroesophageal reflux association
with laryngomalacia: a prospective study. Int J Pediatr Otorhinolaryngol 1998;
43(1):1120.
27. ODonnell S, Murphy J, Bew S, et al. Aryepiglottoplasty for laryngomalacia:
results and recommendations following a case series of 84. Int J Pediatr Otorhi-
nolaryngol 2007;71(8):12715.
28. Rudman DT, Elmaraghy CA, Shiels WE, et al. The role of airway fluoroscopy in
the evaluation of stridor in children. Arch Otolaryngol Head Neck Surg 2003;
129(3):3059.
29. Carden KA, Boiselle PM, Waltz DA, et al. Tracheomalacia andtracheobronchoma-
lacia in children and adults: an in-depth review. Chest 2005;127(3):9841005.
Congenital Airway Lesions and Lung Disease 237
30. BoogaardR, HuijsmansSH, PijnenburgMW, et al. Tracheomalaciaandbronchoma-
lacia in children: incidence and patient characteristics. Chest 2005;128(5):33917.
31. Chen SJ, Lee WJ, Wang JK, et al. Usefulness of three-dimensional electron
beam computed tomography for evaluating tracheobronchial anomalies in chil-
dren with congenital heart disease. Am J Cardiol 2003;92(4):4836.
32. Lee SL, Cheung YF, Leung MP, et al. Airway obstruction in children with congen-
ital heart disease: assessment by flexible bronchoscopy. Pediatr Pulmonol 2002;
34(4):30411.
33. Marchant JM, Masters IB, Taylor SM, et al. Evaluation and outcome of young
children with chronic cough. Chest 2006;129(5):113241.
34. Chang AB, Gaffney JT, Eastburn MM, et al. Cough quality in children: a compar-
ison of subjective vs. bronchoscopic findings. Respir Res 2005;6(1):3.
35. Wood RE. Localized tracheomalacia or bronchomalacia in children with intracta-
ble cough. J Pediatr 1990;116(3):4046.
36. Thomson F, Masters IB, Chang AB. Persistent cough in children and the overuse
of medications. J Paediatr Child Health 2002;38(6):57881.
37. Murgu SD, Colt HG. Tracheobronchomalacia and excessive dynamic airway
collapse. Respirology 2006;11(4):388406.
38. Perl AK, Whitsett JA. Molecular mechanisms controlling lung morphogenesis.
Clin Genet 1999;56(1):1427.
39. Roth-Kleiner M, Post M. Genetic control of lung development. Biol Neonate
2003;84(1):838.
40. Miller LA, Wert SE, Clark JC, et al. Role of Sonic hedgehog in patterning of tra-
cheal-bronchial cartilage and the peripheral lung. Dev Dyn 2004;231(1):5771.
41. Shannon JM, Hyatt BA. Epithelial-mesenchymal interactions in the developing
lung. Annu Rev Physiol 2004;66:62545.
42. Warburton D, Bellusci S, De Langhe S, et al. Molecular mechanisms of early lung
specification and branching morphogenesis. Pediatr Res 2005;57(5 Pt 2):
26R37R.
43. Qi BQ, Merei J, Farmer P, et al. Tracheomalacia with esophageal atresia and
tracheoesophageal fistula in fetal rats. J Pediatr Surg 1997;32(11):15759.
44. Merei J, Hasthorpe S, Farmer P, et al. Relationship between esophageal atresia
with tracheoesophageal fistula and vertebral anomalies in mammalian embryos.
J Pediatr Surg 1998;33(1):5863.
45. Possoegel AK, Diez-Pardo JA, Morales C, et al. Notochord involvement in exper-
imental esophageal atresia. Pediatr Surg Int 1999;15(34):2015.
46. Xia H, Migliazza L, Diez-Pardo JA, et al. The tracheobronchial tree is abnormal in
experimental congenital diaphragmatic hernia. Pediatr Surg Int 1999;15(34):
1847.
47. Xia H, Otten C, Migliazza L, et al. Tracheobronchial malformations in experimen-
tal esophageal atresia. J Pediatr Surg 1999;34(4):5369.
48. Beasley SW, Diez Pardo J, Qi BQ, et al. The contribution of the adriamycin-in-
duced rat model of the VATER association to our understanding of congenital
abnormalities and their embryogenesis. Pediatr Surg Int 2000;16(7):46572.
49. Williams AK, Qi BQ, Beasley SW. Demonstration of abnormal notochord devel-
opment by three-dimensional reconstructive imaging in the rat model of esoph-
ageal atresia. Pediatr Surg Int 2001;17(1):214.
50. Roberts CR, Rains JK, Pare PD, et al. Ultrastructure and tensile properties of
human tracheal cartilage. J Biomech 1998;31(1):816.
51. Mankarious LA, Goetinck PF. Growth and development of the human cricoid
cartilage: an immunohistochemical analysis of the maturation sequence of the
Masters 238
chondrocytes and surrounding cartilage matrix. Otolaryngol Head Neck Surg
2000;123(3):1748.
52. Chen Q, Johnson DM, Haudenschild DR, et al. Progression and recapitulation of
the chondrocyte differentiation program: cartilage matrix protein is a marker for
cartilage maturation. Dev Biol 1995;172(1):293306.
53. Mankarious LA, Adams AB, Pires VL. Patterns of cartilage structural protein loss
in human tracheal stenosis. Laryngoscope 2002;112(6):102530.
54. Cherukupally SR, Adams AB, Mankarious LA. Age-related mechanisms of
cricoid cartilage response to injury in the developing rabbit. Laryngoscope
2003;113(7):11458.
55. Kim JC, Mankarious LA. Novel cell proliferation marker for identification of
a growth center in the developing human cricoid. Arch Otolaryngol Head
Neck Surg 2000;126(2):197202.
56. Roberts CR, Pare PD. Composition changes in human tracheal cartilage in
growth and aging, including changes in proteoglycan structure. Am J Physiol
1991;261(2 Pt 1):L92101.
57. Maki JM, Sormunen R, Lippo S, et al. Lysyl oxidase is essential for normal
development and function of the respiratory system and for the integrity of elas-
tic and collagen fibers in various tissues. Am J Pathol 2005;167(4):92736.
58. Lu MM, Yang H, Zhang L, et al. The bone morphogenic protein antagonist grem-
lin regulates proximal-distal patterning of the lung. Dev Dyn 2001;222(4):
66780.
59. Okamoto T, Yamamoto Y, Gotoh M, et al. Cartilage regeneration using slow re-
lease of bone morphogenetic protein-2 from a gelatin sponge to treat experi-
mental canine tracheomalacia: a preliminary report. ASAIO J 2003;49(1):639.
60. Warburton D, Bellusci S, Del Moral PM, et al. Growth factor signaling in lung
morphogenetic centers: automaticity, stereotypy and symmetry. Respir Res
2003;4:5.
61. Yamamoto Y, Okamoto T, Goto M, et al. Experimental study of bone morphoge-
netic proteins-2 slow release from an artificial trachea made of biodegradable
materials: evaluation of stenting time. ASAIO J 2003;49(5):5336.
62. Okamoto T, Yamamoto Y, Gotoh M, et al. Slow release of bone morphogenetic
protein 2 from a gelatin sponge to promote regeneration of tracheal cartilage
in a canine model. J Thorac Cardiovasc Surg 2004;127(2):32934.
63. Crowley AR, Mehta SS, Hembree MJ, et al. Faulty bone morphogenetic protein
signaling in esophageal atresia with tracheoesophageal fistula. J Pediatr Surg
2006;41(7):120813.
64. Cohen SR, Perelman N, Mahnovski V, et al. Whole organ evaluation of collagen in
the developing human larynx and adjoining anatomic structures (hyoid and
trachea). Ann Otol Rhinol Laryngol 1993;102(9):6559.
65. Murgu S, Colt H. Tracheobronchomalacia untangling the Gordian knot. Journal
of Bronchology 2005;12(4):23944.
66. Couvreur J, Grimfeld A, Tournier G, et al [Tracheal dyskinesia (tracheomalacia)
in children. Reflections apropos of 127 cases diagnosed by endoscopy]. Ann
Pediatr (Paris) 1980;27(9):56170 [in French].
67. Loundon N, Brugel L, Roger C, et al. Current approach of primary tracheal
dyskinesia. Pediatr Pulmonol Suppl 1999;18:6770.
68. Corre A, Chaudre F, Roger G, et al. Tracheal dyskinesia associated with midline
abnormality: embryological hypotheses and therapeutic implications. Pediatr
Pulmonol 2001;(Suppl 23):102.
Congenital Airway Lesions and Lung Disease 239
69. Campbell AH. Definition and causes of the tracheobronchial collapse syndrome.
Br J Dis Chest 1967;61(1):111.
70. Fletcher BD, Cohn RC. Tracheal compression and the innominate artery: MR
evaluation in infants. Radiology 1989;170(1 Pt 1):1037.
71. Mahboubi S, Harty MP, Hubbard AM, et al. Innominate artery compression of the
trachea in infants. Int J Pediatr Otorhinolaryngol 1996;35(3):197205.
72. Weber TR, Keller MS, Fiore A. Aortic suspension (aortopexy) for severe trache-
omalacia in infants and children. Am J Surg 2002;184(6):5737 [discussion
577].
73. Benjamin B. Tracheomalacia in infants and children. Ann Otol Rhinol Laryngol
1984;93(5 Pt 1):43842.
74. Beasley SW, Qi BQ. Understanding tracheomalacia. J Paediatr Child Health
1998;34(3):20910.
75. Shaffer TH, Wolfson MR, Panitch HB. Airway structure, function and develop-
ment in health and disease. Paediatr Anaesth 2004;14(1):314.
76. Masters IB, Eastburn M, Francis PW, et al. Quantification of the magnification
and distortion effects of a pediatric flexible video-bronchoscope. Respir Res
2005;6(1):16.
77. Masters IB, Eastburn MM, Wootton R, et al. A new method for objective identifi-
cation and measurement of airway lumen in paediatric flexible videobroncho-
scopy. Thorax 2005;60(8):6528.
78. Masters IB, Ware RS, Zimmerman PV, et al. Airway sizes and proportions in
children quantified by a video-bronchoscopic technique. BMC Pulm Med
2006;6(1):5.
79. Masters IB, Zimmerman PV, Chang AB. Longitudinal quantification of growth
and changes in primary tracheobronchomalacia sites in children. Pediatr Pulmo-
nol 2007;42(10):90613.
80. Aquino SL, Shepard JA, Ginns LC, et al. Acquired tracheomalacia: detection by
expiratory CT scan. J Comput Assist Tomogr 2001;25(3):3949.
81. Boiselle PM, Ernst A. Recent advances in central airway imaging. Chest 2002;
121(5):165160.
82. Boiselle PM. Multislice helical CT of the central airways. Radiol Clin North Am
2003;41(3):56174.
83. Boiselle PM, Feller-Kopman D, Ashiku S, et al. Tracheobronchomalacia: evolving
role of dynamic multislice helical CT. Radiol Clin North Am 2003;41(3):62736.
84. Boiselle PM, Lee KS, Ernst A. Multidetector CT of the central airways. J Thorac
Imaging 2005;20(3):18695.
85. Boiselle PM, Ernst A. Tracheal morphology in patients with tracheomalacia: prev-
alence of inspiratory lunate and expiratory frown shapes. J Thorac Imaging
2006;21(3):1906.
86. Boiselle PM, Lee KS, Lin S, et al. Cine CT during coughing for assessment of
tracheomalacia: preliminary experience with 64-MDCT. AJR Am J Roentgenol
2006;187(2):W1757.
87. Faust RA, Remley KB, Rimell FL. Real-time, cine magnetic resonance imaging
for evaluation of the pediatric airway. Laryngoscope 2001;111(12):218790.
88. Long FR, Castile RG. Technique and clinical applications of full-inflation and
end-exhalation controlled-ventilation chest CT in infants and young children.
Pediatr Radiol 2001;31(6):41322.
89. Faust RA, Rimell FL, Remley KB. Cine magnetic resonance imaging for evalua-
tion of focal tracheomalacia: innominate artery compression syndrome. Int J
Pediatr Otorhinolaryngol 2002;65(1):2733.
Masters 240
90. Briganti V, Oriolo L, Buffa V, et al. Tracheomalacia in oesophageal atresia: mor-
phological considerations by endoscopic and CTstudy. Eur J Cardiothorac Surg
2005;28(1):115.
91. Briganti V, Oriolo L, Mangia G, et al. Tracheomalacia in esophageal atresia. Use-
fulness of preoperative imaging evaluation for tailored surgical correction.
J Pediatr Surg 2006;41(9):16248.
92. Murgu SD, Colt HG. Treatment of adult tracheobronchomalacia and excessive
dynamic airway collapse: an update. Treat Respir Med 2006;5(2):10315.
93. Masters IB, Zimmerman PV, Pandeya N, et al. Quantified tracheobronchoma-
lacia disorders and their clinical profiles in children. Chest 2008;133(2):
4617.
94. Chang AB, Landau LI, Van Asperen PP, et al. Cough in children: definitions and
clinical evaluation. Med J Aust 2006;184(8):398403.
95. Marchant JM, Masters IB, Chang AB. Defining paediatric chronic bronchitis.
Respirology 2004;9(Suppl):A61.
96. Marchant JM, Masters IB, Chang AB. Chronic cough in children. Eur Respir J
2003;22(Suppl 45):176S.
97. Marchant JM, Masters IB, Taylor SM, et al. Utility of signs and symptoms of
chronic cough in predicting specific cause in children. Thorax 2006;61(8):
6948.
98. Masters IB, Chang AB. Interventions for primary (intrinsic) tracheomalacia in
children. Cochrane Database Syst Rev 2005;(4):CD005304.
99. Newcombe PA, Sheffield JK, Juniper EF, et al. Development of a parent-proxy
quality-of-life chronic cough-specific questionnaire: clinical impact vs psycho-
metric evaluations. Chest 2008;133(2):38695.
100. Hofhuis W, van der Wiel EC, Tiddens HA, et al. Bronchodilation in infants with
malacia or recurrent wheeze. Arch Dis Child 2003;88(3):2469.
101. Miller RW, Pollack MM, Murphy TM, et al. Effectiveness of continuous positive
airway pressure in the treatment of bronchomalacia in infants: a bronchoscopic
documentation. Crit Care Med 1986;14(2):1257.
102. Ferguson GT, Benoist J. Nasal continuous positive airway pressure in the treat-
ment of tracheobronchomalacia. Am Rev Respir Dis 1993;147(2):45761.
103. Panitch HB, Allen JL, Alpert BE, et al. Effects of CPAP on lung mechanics in in-
fants with acquired tracheobronchomalacia. Am J Respir Crit Care Med 1994;
150(5 Pt 1):13416.
104. Essouri S, Nicot F, Clement A, et al. Noninvasive positive pressure ventilation in
infants with upper airway obstruction: comparison of continuous and bilevel
positive pressure. Intensive Care Med 2005;31(4):57480.
105. Dave S, Currie BG. The role of aortopexy in severe tracheomalacia. J Pediatr
Surg 2006;41(3):5337.
106. Ahel V, Banac S, Rozmanic V, et al. Aortopexy and bronchopexy for the manage-
ment of severe tracheomalacia and bronchomalacia. Pediatr Int 2003;45(1):
1046.
107. van der Zee DC, Bax NM. Thoracoscopic tracheoaortopexia for the treatment of
life-threatening events in tracheomalacia. Surg Endosc 2007;21(11):20245.
108. Roberts CS, Othersen HB Jr, Sade RM, et al. Tracheoesophageal compression
from aortic arch anomalies: analysis of 30 operatively treated children. J Pediatr
Surg 1994;29(2):3347 [discussion 3378].
109. Kazim R, Berdon WE, Montoya CH, et al. Tracheobronchial anomalies in chil-
dren with congenital cardiac disease. J Cardiothorac Vasc Anesth 1998;
12(5):5535.
Congenital Airway Lesions and Lung Disease 241
110. Fiore AC, Brown JW, Weber TR, et al. Surgical treatment of pulmonary artery
sling and tracheal stenosis. Ann Thorac Surg 2005;79(1):3846 [discussion 38].
111. Alsenaidi K, Gurofsky R, Karamlou T, et al. Management and outcomes of dou-
ble aortic arch in 81 patients. Pediatrics 2006;118(5):e133641.
112. Brown JW, Ruzmetov M, Vijay P, et al. Surgical treatment of absent pulmonary
valve syndrome associated with bronchial obstruction. Ann Thorac Surg 2006;
82(6):22216.
113. Burden RJ, Shann F, Butt W, et al. Tracheobronchial malacia and stenosis in chil-
dren in intensive care: bronchograms help to predict outcome. Thorax 1999;
54(6):5117.
114. Chang AB, Glomb WB. Guidelines for evaluating chronic cough in pediatrics:
ACCP evidence-based clinical practice guidelines. Chest 2006;129(1 Suppl):
260S83S.
115. Abdel-Rahman U, Ahrens P, Fieguth HG, et al. Surgical treatment of tracheoma-
lacia by bronchoscopic monitored aortopexy in infants and children. Ann Thorac
Surg 2002;74(2):3159.
116. Imai Y, Mark EJ. Cystic adenomatoid change is common to various forms of cys-
tic lung diseases of children: a clinicopathologic analysis of 10 cases with em-
phasis on tracing the bronchial tree. Arch Pathol Lab Med 2002;126(8):93440.
117. Morikawa N, Kuroda T, Honna T, et al. Congenital bronchial atresia in infants and
children. J Pediatr Surg 2005;40(12):18226.
118. Kim WS, Lee KS, Kim IO, et al. Congenital cystic adenomatoid malformation of
the lung: CT-pathologic correlation. AJR Am J Roentgenol 1997;168(1):4753.
119. Eber E. Antenatal diagnosis of congenital thoracic malformations: early surgery,
late surgery, or no surgery? Semin Respir Crit Care Med 2007;28(3):35566.
120. Azizkhan RG, Crombleholme TM. Congenital cystic lung disease: contemporary
antenatal and postnatal management. Pediatr Surg Int 2008;24(6):64357.
121. Volpe MV, Pham L, Lessin M, et al. Expression of Hoxb-5 during human lung de-
velopment and in congenital lung malformations. Birth Defects Res A Clin Mol
Teratol 2003;67(8):5506.
122. Gonzaga S, Henriques-Coelho T, Davey M, et al. Cystic adenomatoid malforma-
tions are induced by localized FGF10 overexpression in fetal rat lung. Am
J Respir Cell Mol Biol 2008;39:34655.
123. Wagner AJ, Stumbaugh A, Tigue Z, et al. Genetic analysis of congenital cystic
adenomatoid malformation reveals a novel pulmonary gene: fatty acid binding
protein-7 (brain type). Pediatr Res 2008;64(1):116.
124. Tsai AY, Liechty KW, Hedrick HL, et al. Outcomes after postnatal resection of
prenatally diagnosed asymptomatic cystic lung lesions. J Pediatr Surg 2008;
43(3):5137.
125. Rothenberg SS. First decades experience with thoracoscopic lobectomy in
infants and children. J Pediatr Surg 2008;43(1):404 [discussion 45].
126. Vu LT, Farmer DL, Nobuhara KK, et al. Thoracoscopic versus open resection for
congenital cystic adenomatoid malformations of the lung. J Pediatr Surg 2008;
43(1):359.
Masters 242
Obstructi ve Sl eep
Breathi ng Di sorders
ChunTing Au, MPhil, RPSGT, Albert Martin Li, MD*
Sleep-disordered breathing (SDB) refers to a group of respiratory conditions that are
exacerbated during sleep. SDB is increasingly being recognized as an important
disease entity, and if the condition is left untreated, significant morbidity and even
mortality can result.
1
The most prominent SDB condition in children is obstructive
sleep apnea (OSA), which belongs to the severe end of a spectrum, ranging in severity
from primary or simple snoring through upper airway resistance syndrome, obstruc-
tive hypopnea syndrome, to its most severe form, OSA (Box 1). The American Tho-
racic Society defines childhood OSA as a disorder that is characterized by repeated
episodes of partial or complete upper airway obstruction during sleep that result in
disruption of normal ventilation and sleep patterns.
2
EPIDEMIOLOGY
The accurate identification of the prevalence of childhood OSA should allow better
resource allocation and clinicians to performmore targeted screening. In relation to re-
search, recognizing differences in the prevalence of the condition among races may
allowa better understanding of its etiology. A recent reviewstressed that published lit-
eratureonthe prevalence of childhoodOSAis fraught withdifficulty becauseof avariety
of methodologic issues.
3
Within these limitations, reviewof relevant literature suggests
a prevalence of OSA from 0.1% to 13%, but most studies report a figure between 1%
and 4%. There are accumulating data to suggest that OSA is more common among
overweight or obese boys. This condition peaks between the ages of 2 and 8 years, co-
inciding with the peak age of lymphoid hyperplasia. Some data do suggest a higher
prevalence among African Americans in the United States, but whether such a racial
Department of Pediatrics, Prince of Wales Hospital, The Chinese University of Hong Kong,
Shatin, Hong Kong
* Corresponding author.
E-mail address: albertmli@cuhk.edu.hk (A. Li).
KEYWORDS
Sleep-disordered breathing
Obstructive sleep apnea
Child
Snoring
Sleep disturbance
Pediatr Clin N Am 56 (2009) 243259
doi:10.1016/j.pcl.2008.10.012 pediatric.theclinics.com
0031-3955/08/$ see front matter 2009 Elsevier Inc. All rights reserved.
difference also holds true for other population remains to be examined. Table 1 shows
the prevalence of OSA reported after diagnostic testing in 13 studies.
ETIOLOGY
The most common cause for childhood OSA is adenotonsillar hypertrophy, but the
large tonsils and adenoids alone cannot account for the entire pathophysiologic pro-
cess. There is accumulating evidence to suggest that OSA is related to an interaction
of structural and neuromuscular variables within the upper airway. Although several
studies showed that children with OSA have larger tonsils and adenoids when com-
pared with age-matched controls, a linear relation between the size of lymphoid
tissues and severity of OSA has never been documented.
1719
Some patients with
no other known risk factors have persistent OSA despite having their tonsils and ad-
enoids removed. A recent study revealed that childhood OSA was related to impaired
response of the central nervous system to mechanical stimulation of the respiratory
system.
20
Thus, structural factors alone cannot be fully responsible for this condition.
Upper airway resistance increases during sleep even in normal humans because of
the reduction in muscle tone of the pharyngeal dilator muscles.
21,22
When the upper
airway resistance is further increased because of other factors, such as adenotonsillar
hypertrophy or neuromotor function abnormalities, however, the upper airway col-
lapses at a lower threshold.
23,24
In more general terms, the mechanism underlying
this condition is related to some combination of three processes: (1) decreased upper
airway patency (adenotonsillar hypertrophy, allergies associated with chronic rhinitis
or nasal obstruction), (2) reduced capacity to maintain airway patency related to neu-
romuscular tone (obesity, neuromuscular disorder), and (3) decreased drive to breathe
(brain stem injury).
There are a variety of medical conditions that are associated with an increased risk
for OSA (Table 2). Since its first description in 1976, childhood OSA has been recog-
nized as a different disease entity from adult OSA with respect to etiology, clinical
manifestations, and management (Table 3).
CLINICAL FEATURES
The most common presenting complaint of childhood OSA is snoring, and the condi-
tion is unlikely in the absence of habitual snoring (snoring for most nights of the week),
although many children with snoring do not have OSA. Nocturnal and daytime
symptoms associated with the condition are shown in Table 4.
No combination of symptoms and physical findings has been found to distinguish
OSA reliably from primary snoring.
25
In most cases, children have enlarged tonsils
or adenoids and do not demonstrate breathing difficulties during clinical examination.
There is no reliable relation between the size of the tonsils on direct inspection and the
presence of OSA.
26
Box1
Continuumof obstructive sleep-disordered breathing
Primary snoring: increased airway resistance without other symptoms
Upper airway resistance syndrome: sleep disturbance with normal blood gas profile
Obstructive hypopnea syndrome: hypopnea, sleep disturbance without desaturation
OSA: apnea, hypopnea, sleep disturbance with desaturation
Au & Li 244
Table1
Prevalence of childhood obstructive sleep apnea
Author No. Subjects Country Age (Years)
Diagnostic
Technique
Prevalence of
Obstructive Sleep
Apnea Symptoms
Ali et al, 1993
4
782 screened
132 monitored
United
Kingdom
45 Pulse oximetry, video 0.7%
Gislason et al, 1995
5
454 Iceland 0.56 PSG (AHI >3) 2.9%
Redline et al, 1999
6
126 United States 218 PSG 1.6% (AHI >10)
10.3% (AHI >5)
Brunetti et al, 2001
7
895 screened
12 monitored
Italy 311 PSG (AHI >3) 1.0%1.8%
Anuntaseree et al, 2001
8
1008 screened 8
monitored
Thailand 613 PSG (AHI >1) 0.69%
S anchez-Armengol
et al, 2001
9
100 Spain 1216 PSG (RDI >10) 2.0%
Ng et al, 2002
10
200 Hong Kong 6.4 4 PSG (AHI >1) 0.1%
Castronovo et al,
2003
11
595 screened
265 monitored
Italy 36 Pulse oximetry 13%
Rosen CL, 2003
12
243 United States 811 PSG (OAI >1) 1.9%
OBrien et al, 2003
13
5728 United States 57 PSG (AHI >5) 5.7%
Kaditis et al, 2004
14
3680 Greece 118 PSG (AHI >5) 4.3%
Sogut et al, 2005
15
1198 Turkey 311 PSG (AHI >3) 0.9%
Anuntaseree
et al, 2005
16
755 Thailand 910 PSG (AHI >1) 1.3%
Abbreviations: AHI, apnea hypopnea index; PSG, polysomnography; RDI, respiratory disturbance index.
O
b
s
t
r
u
c
t
i
v
e
S
l
e
e
p
B
r
e
a
t
h
i
n
g
D
i
s
o
r
d
e
r
s
2
4
5
COMPLICATIONS ASSOCIATED WITHOBSTRUCTIVE SLEEPAPNEA
Neurocognitive Abnormalities
In contrast to adult patients, affected children tend to have preserved sleep architec-
ture;
27
therefore, excessive daytime sleepiness (EDS) is not a predominant feature.
Despite the relative absence of EDS, childhood OSA and even nonapneic snoring
Table 2
Medical conditions associated with childhood obstructive sleep apnea
Craniofacial syndromes Crouzon syndrome
Apert syndrome
Treacher-Collins syndrome
Goldenhar syndrome
Pierre Robin syndrome
Neurologic diseases Arnold-Chiari malformation
Meningomyelocele
Cerebral palsy
Duchenne muscular dystrophy
Conditions with abnormal muscle tone Down syndrome
Prader-Willi syndrome
Hypothyroidism
Conditions with reduced upper airway patency Adenotonsillar hypertrophy
Obesity
Allergic rhinitis
Macroglossia
Laryngomalacia
Subglottic stenosis
Mucopolysaccharidoses/metabolic
storage diseases
Table 3
Comparison of obstructive sleep apnea in children and adults
Children Adults
Estimated prevalence 1%4% 2%4%
Peak age 28 years 3060 years
Gender (male/female) 1:1 3:1
Weight Normal, decreased, increased Overweight
Major cause Adenotonsillar hypertrophy Obesity
Gas exchange abnormalities Always Always
Duration of obstructive apneas Any >10 seconds
Abnormal AI (per hour) >1 >5
Abnormal AHI (per hour) >1 >10
Sleep architecture Preserved Always altered
Arousals Occasional Always
Daytime sleepiness 30% >90%
Neurocognitive problems Common Less common
Common treatment Adenotonsillectomy CPAP
Abbreviations: AHI, apnea-hypopnea index; AI, apnea index; CPAP, continuous positive airway
pressure.
Au & Li 246
seem to be associated with significant neurocognitive sequelae, for example, behav-
ioral and learning problems, poor attention span, hyperactivity, and even lower than av-
erage intelligent quotient.
28
Indeed, one clinical study showed an alarmingly high
prevalence of snoring and gas exchange abnormalities in children who were academ-
ically poor achievers, and significant improvement in school performance was seen af-
ter adenotonsillectomy.
29
This finding has subsequently been substantiated in other
clinical studies,
3032
establishing a causal relation between OSA and neurocognitive
deficit.
It has been estimated that up to 30% of children with habitual snoring or OSA have
inattention and hyperactivity.
30
The attention deficit hyperactivity disorder (ADHD)
symptoms that these children exhibit may not be true ADHD but rather a lack of
behavioral inhibition secondary to repeated sleep arousals and intermittent hypoxic
episodes that affects working memory, motor control, and self-regulation of motiva-
tion.
33
These attention and behavioral problems have also been shown to have an ad-
verse effect on cognition and school performance.
34
There is, however, recent
evidence to suggest reversibility of such neurocognitive dysfunction after treatment.
31
A more recent study indicated that the behavioral problems in children with SDB were
not only attributable to SDB-related impairments but to being overweight, to insuffi-
cient sleep, and to comorbid sleep disorders, especially insomnia.
35
Therefore, clini-
cians should consider the relative contributions of all these factors when assessing
behavior in children with SDB.
Cardiovascular Consequences
Hypertension has long been recognized as one of the complications in adult OSA.
From the Wisconsin Sleep Cohort, it was found that adults with an apnea hypopnea
index (AHI) of 15 or greater had a three times higher chance of developing hyperten-
sion.
36
Corresponding data are scarce for the pediatric population, however, and the
few published studies have provided conflicting results.
3742
Marcus and colleagues
37
Table 4
Symptoms of childhood obstructive sleep apnea
Nocturnal symptoms Loud habitual snoring
Difficulty breathing when asleep
Apneic pauses
Restless sleep
Sweating
Dry mouth
Abnormal sleeping position
Enuresis
Night terrors/sleep walking
Bruxism/teeth grinding
Daytime symptoms Mouth breathing
Morning headache
Difficulty in waking up
Mood changes
Poor attention span/academic problems
Increased nap/daytime sleepiness
Chronic nasal congestion/rhinorrhea
Frequent upper respiratory tract infections
Difficulty in swallowing/poor appetite
Hearing problems
Obstructive Sleep Breathing Disorders 247
suggested that children with OSA had higher diastolic blood pressure (BP) during
wakefulness and sleep compared with primary snorers. Amin and colleagues,
38
con-
versely, found lower diastolic BP among children with OSA during wakefulness. Guil-
leminault and colleagues
39
demonstrated that a subgroup of children with OSA were
hypotensive rather than hypertensive. The mechanism behind this low BP group is not
known; it was suggested to be attributable to dominant vagal discharge as a result of
increased work of breathing. Kohyama and colleagues
40
showed that children with
OSA had higher diastolic BP; furthermore, the diastolic BP was significantly correlated
with the AHI. The group also found that 29% of patients in the group with an AHI
greater than 10 lacked a sleep-related decrease in BP versus 19% of patients in the
lower AHI group (AHI <10). Similarly, Enright and colleagues
41
found that obesity,
sleep efficiency, and respiratory disturbance index (RDI) were associated with an in-
crease in BP in preadolescent children. A recent study by Leung and collegues,
42
however, failed to confirm such a positive association between BP and severity of
OSA. These inconsistent findings in BP measurements in children with OSA might
have been related to the small sample sizes and the lack of normal healthy subjects
for comparison. A meta-analysis concluded that there was inadequate evidence for
an increased risk for elevated BP in children with SDB. Zintzaras and Kaditis
43
also
found marked heterogeneity among published series and emphasized the need for
further studies to clarify this important issue in childhood OSA. The authors group
has recently completed a large-scale community-based study further confirming the
positive association between childhood OSA and elevated daytime and nighttime
BP and has demonstrated that OSA is an independent predictor of nocturnal hyper-
tension.
44
Another clinical study revealed that increases in ambulatory BP in children
with OSA could predict changes in left ventricular relative wall thickness.
45
These find-
ings consolidate the linkage between SDB and BP elevation in children, and future re-
search should concentrate on BP changes after treatment for OSA.
Changes in ventricular geometry have also been reported in children with OSA.
Amin and colleagues
46
investigated the heart size of 28 and 19 patients who had
OSA and primary snoring, respectively, and found that the left ventricular mass in-
dex and wall thickness were greater in children with OSA. Those with an AHI of 10
or more had a right and left ventricular mass greater than the ninety-fifth percentile.
The same group later showed that there was a dose-dependent decrease in left
ventricular diastolic function with increased severity of OSA.
47
S
anchez-Armengol
and colleagues
48
studied a group of adolescents (mean age: 13.7 1.6 years)
and found that the posterior ventricular wall thickness could be predicted from de-
saturation events and RDI. The intermittent hypoxia that occurs in children with
OSA may induce elevations of pulmonary artery pressure, and such events may
lead to right ventricular dysfunction,
49,50
but the exact pathophysiologic mechanism
leading to ventricular dysfunction and morphologic changes and the effects of treat-
ment need to be further examined.
Arterial distensibility assessed in vivo by measurement of pulse wave velocity (PWV)
is an important predictor of cardiovascular risk in adults.
51
The PWV and BP were
examined in a group of children with primary snoring, and these children were docu-
mented to have higher systolic, diastolic, and mean BP in comparison to the control
group. Furthermore, the PWV was increased in children with primary snoring, which
signified decreased arterial distensibility.
52
A recent study has also provided evidence
of endothelial dysfunction in children with OSA. Postocclusive hyperemia, a marker of
endothelial function, was blunted in 26 children with OSA, and such altered endothelial
function was reversible at 4 to 6 months after treatment, particularly in those without
a family history of cardiovascular disease.
53
Au & Li 248
Insulin Resistance
There has been an alarming increase in the prevalence of type 2 diabetes mellitus (DM)
in children, and in recent years, type 2 DM has become the most frequent endocrine
disorder affecting glucose metabolism in children.
54
Insulin resistance is considered
an important risk factor for the development of type 2 DM, and therefore provides
an early intervention parameter for prevention of the disease and its significant
long-term consequences.
55
The term metabolic syndrome, a well-established risk factor for cardiovascular
disease in adults, refers to clustering of insulin resistance, an abnormal lipid profile,
hypertension, and obesity. Up to the time of writing, there is no clear-cut agreed-on
definition of the metabolic syndrome for children.
56
Using adult criteria, the overall
prevalence of metabolic syndrome among 12- to 19-year-old adolescents in the
United States was found to be 4.2%.
57
Weiss and colleagues
58
found that the
risk for metabolic syndrome was nearly 50% in severely obese adolescents and
that the risk increased with every 0.5-unit increment in body mass index (BMI).
Raised fasting insulin levels and increased BMI during childhood are strong predic-
tors for the development of metabolic syndrome in adulthood.
59
Furthermore, insulin
resistance in childhood is associated with an increased risk for later cardiovascular-
related morbidity and mortality.
60
Similar to obesity, there is accumulating evidence to suggest OSA as an important
risk factor for insulin resistance in adults.
61,62
There are, however, limited data in the
literature on the same subject in pediatrics. Previous pediatric studies that examined
the relation between OSA, obesity, and insulin resistance
6368
have reported conflict-
ing results. In a large cohort of nonobese and obese snoring children, Tauman and col-
leagues
63
showed that insulin resistance (assessed by insulin/glucose ratio and
homeostatic model assessment) and lipid dysregulation (evidence of increased
plasma triglyceride and decreased plasma high-density lipoprotein concentration)
were primarily determined by the degree of adiposity and that OSA played a minimal,
if any, role in the occurrence of insulin resistance. These findings have been confirmed
in a study involving Greek nonobese children.
64
In other studies conducted in obese
children with OSA, however, insulin resistance was found to correlate with the severity
of the respiratory disease independent of the degree of obesity.
6567
More recently,
Gozal and colleagues
68
further confirmed that OSA seemed to induce insulin resis-
tance in obese but not nonobese children. Moreover, follow-up study demonstrated
significant improvements in lipid profiles and apolipoprotein B levels after adenoton-
sillectomy. This finding suggested a causal role for OSA in lipid homeostasis indepen-
dent of the degree of adiposity, but the complex interaction between insulin, obesity,
OSA, and metabolic dysfunction needs further investigation.
Growth Failure
The pathogenesis associated with failure to thrive in children with OSA is likely to be an
interplay among various mechanisms that include increased resting energy expendi-
ture, difficulty with swallowing secondary to enlarged tonsils, and abnormal release of
growth-related hormones.
69
Caloric intake and sleeping energy expenditure, in addi-
tion to anthropomorphic measurements, were taken before and after adenotonsillec-
tomy in 14 children confirmed to have OSA. Average sleeping energy expenditure
decreased and the mean weight z-score increased after surgery without any change
in caloric intake.
70
The presence of poor appetite, difficulty in swallowing, and nausea
with vomiting was reported more frequently in children with OSA compared with con-
trols.
71
Statistically significant increases in weight and insulin-like growth factor-I
Obstructive Sleep Breathing Disorders 249
levels were found in a group of children with OSA after adenotonsillectomy.
72
Fortu-
nately, we are seeing less of this complication as parents are becoming more aware
of this condition and seeking medical intervention early.
ROLE OF INFLAMMATION IN CHILDHOOD OBSTRUCTIVE SLEEPAPNEA
Inflammation is a mechanism that may link OSA and cardiovascular disease.
73,74
Adults with OSA have higher levels of proinflammatory cytokines, tumor necrosis
factor (TNF)-a, and interleukin-6,
75,76
which decrease after treatment for OSA.
7779
C-reactive protein (CRP) is the most widely studied marker of systemic inflammation
in children. Published studies have reported conflicting results, however.
8083
In
a study of 81 children with a mean age of 9.3 years, Tauman and colleagues
80
found
raised levels of CRP, a strong marker of cardiovascular risk, in children with OSA com-
pared with controls, with levels correlating with disease severity. A similar correlation
between CRP and sleep apnea severity was also documented in a study involving
older children with a mean age of 13.7 years.
81
These positive results were not
confirmed by two other studies, however.
82,83
Adipose tissue is an important source
of inflammatory cytokines, which are essential inducers for CRP production.
84
Obesity
is therefore a confounding factor in the correlation between CRP and OSA, and that
can partly explain discrepancies among results of published studies. Two recent stud-
ies have provided further support for the presence of systemic inflammation in children
with OSA.
85,86
In both studies, these investigators (from the same research institute)
demonstrated a significant reduction in CRP after treatment for OSA. The same re-
search group also examined another marker of systemic inflammation, TNFa, and
demonstrated that its serum levels were elevated in children with polysomnography
(PSG) proved OSA and that the magnitude of the TNFa level was primarily correlated
with the degree of respiratory eventinduced sleep fragmentation.
87
Children with OSA have also been documented to have elevated plasma levels of
P-selectin, a marker of platelet activation, lending support to the premise that inflam-
matory processes are elicited by OSA in children and may contribute to an accelerated
risk for cardiovascular morbidity.
88
Further large-scale controlled studies are needed
to delineate the role of systemic inflammation in childhood OSA clearly; particularly im-
portant is the implication of such inflammation in future cardiovascular risk.
DIAGNOSIS OF OBSTRUCTIVE SLEEPAPNEA
Many methods have been studied to diagnose OSA, starting with a history and phys-
ical examination; proceeding to audiotaping or videotaping; and ending with pulse
oximetry, abbreviated PSG, and full PSG. Although PSG is the current gold standard
for the diagnosis of OSA, many authorities have questioned its usefulness and feasi-
bility in routine clinical practice. Arguments, such as cost and lack of consensus on the
interpretation of PSG findings, are enough for many physicians to consider PSG not
necessary for diagnosis. Conversely, a history and physical examination alone are
poor at predicting OSA,
25
and abbreviated studies tend to be helpful if results are
positive but have a poor predictive value if the results are negative.
1
PSG is a cumbersome examination and may not accurately reflect the childs sleep
in his or her habitual environment. The parameters originally used to evaluate child-
hood PSG were based on adult values. PSG has not been well standardized in its per-
formance or interpretation, especially within the pediatric population. Normative
standards for PSGdetermination have been chosen on the basis of statistical distribu-
tion of data, and it has not been established that those standards have any validity as
predictors of long-term outcome. Most pediatric respiratory clinicians consider an
Au & Li 250
obstructive apnea index greater than 1 to be abnormal.
89
This criterion does not take
into account episodes of hypopnea, however, and, recently, an obstructive apnea-
hypopnea index greater than 1 has been proposed as diagnostic for OSA.
90
TREATMENT OF OBSTRUCTIVE SLEEPAPNEA
Medical Treatment
Broad-spectrum antibiotics may offer temporary improvement, particularly if snoring
and obstruction occur intermittently and are associated with recurrent tonsillitis or ad-
enoiditis.
91
The use of antibiotics does not seem to obviate the need for surgery in
most cases with adenotonsillar hypertrophy, however.
92
Nasal corticosteroids have
been examined as an alternative to adenotonsillectomy in otherwise healthy children
with OSA.
93,94
In a prospective, randomized, double-blind study, children with mild to
moderate OSA were treated with a 6-week course of nasal corticosteroids or placebo.
The researchers were able to demonstrate a moderate improvement in cases treated
with nasal corticosteroids. This was associated with concomitant decreases of
approximately 50%in the desaturation index and the movement arousal index. In con-
trast, the placebo group did not show any improvement.
93
Nasal corticosteroids work
by exerting lympholytic action and effects on inflammation and upper airway edema.
95
In an open-labeled study, the leukotriene receptor antagonist montelukast was found
to be clinically effective in reducing disease severity in children with mild OSA.
96
In
a subsequent study, a combination of intranasal steroids and leukotriene modifier
was found to be useful in children with residual OSA after adenotonsillectomy.
97
Surgical Treatment
Treating children with OSA depends on the childs underlying abnormalities, the site of
obstruction, and the presence or absence of contributing neurologic or functional
abnormalities. Adenotonsillectomy is considered the cardinal treatment of childhood
OSA, and the procedure is superior to adenoidectomy or tonsillectomy alone.
98
Nev-
ertheless, a recent study reported that complete surgical cure of OSA occurred in only
25% of children, with another 50% showing significant improvements in their OSA
parameters. The following groups of patients have been identified to be at a higher
risk for persistent OSA despite surgery: initial severe OSA, obesity, and those with
a positive family history of OSA.
99
Another recent study showed that initial BMI,
gain velocity of BMI, and African-American race confer an independent increased
risk for recurrence of SDB after adenotonsillectomy.
100
This implied that good weight
control is important after surgical treatment. Other surgical procedures, such as nasal
septoplasty, epiglottoplasty, uvulopharyngopalatoplasty, and maxillofacial surgery,
are seldom performed in children but may be indicated in selected cases.
101
Mechanical Treatment
Nasal continuous positive airway pressure (CPAP) provides positive pressure to the
lumen of the airway and decreases airway collapsibility. It is of utmost importance
that the initial approach to the family and childbe performed correctly andsuccessfully.
CPAPtherapy should be titrated during PSGto determine effective pressures, and chil-
dren on CPAPtherapy should be followed regularly to ensure compliance and proper fit
of the mask interface. CPAP may be indicated in the following clinical situations:
Adenotonsillectomy not indicated or contraindicated
Adenotonsillectomy fails to resolve symptoms completely, usually in children
with additional risk factors, such as obesity
Before surgery in children with severe OAS
98
Obstructive Sleep Breathing Disorders 251
Bilevel positive airway pressure (BiPAP) also allows setting of a backup rate and pro-
vides some ventilatory assistance. This is especially important for patients with sleep-
related hypoventilation caused by muscle weakness, neurologic disease, or obesity.
CPAP and BiPAP are highly efficacious in pediatric obstructive apnea, but treatment
is associated with a high dropout rate, and even in those adherent children, nighttime
use is still suboptimal considering the long sleep hours in children.
102
One potential
Fig. 1. Diagnosis and treatment of childhood OSA.
Au & Li 252
complication of long-term nasal mask CPAP or BiPAP is midface hypoplasia. In chil-
dren on long-term nasal positive-pressure therapy, maxillomandibular growth should
be monitored carefully and regularly.
Oral appliances, such as mandibular advancing devices and tongue retainers, are
rarely used in children with OSA. Supplemental oxygen therapy abolishes desaturation
episodes associated with OSA, but it does not treat the underlying obstruction and
may worsen hypoventilation.
WHAT DO I DO WHEN ACHILD WITHSNORING OR SLEEP DISTURBANCE PRESENTS?
Fig. 1 is a proposed algorithm describing how children with snoring or sleep distur-
bance can be dealt with in clinical practice. The following is a summary of the
algorithm:
1. Features suggestive of OSA should be sought during history taking.
2. Patients who have certain medical conditions (see diagram) are at higher risk for
developing OSA, and their further management is best managed by a specialist.
3. Clinical symptoms alone are not able to discriminate between simple snoring and
OSA. The gold standard for the diagnosis of childhood OSA is overnight PSG.
Because of its high running cost, however, the service is not widely available. Other
Table 5
Recommendations of treatment for childhood obstructive sleep apnea
Medication or Intervention Recommendation
Grading of
Eecommendation
(Based on Evidence
of Benefit)
Quality of
Supporting
Evidence
Adenotonsillectomy Recommended as first-line
therapy for children
with OSA secondary
to adenotonsillar
hypertrophy
Strong High
Weight loss Recommended as
supplementary
therapy for obese patients
Strong High
Nasal steroids with
or without
leukotriene
receptor
antagonist
An option for children
with mild OSA related
to nasal obstruction
caused by allergic
rhinitis
Weak Low
Noninvasive
positive-pressure
ventilation
Recommended for
children who are
not candidates for
surgery or whose
symptoms are not completely
resolved after surgery
Strong High
Oral appliances Rarely used in
childhood OSA
Weak Low
Oxygen
supplementation
Not suitable as
monotherapy
because it can
aggravate carbon
dioxide retention
Weak Low
Obstructive Sleep Breathing Disorders 253
abbreviated studies, such as nocturnal pulse oximetry, daytime nap studies, and
unattended home PSG, may also be considered. These studies have high rates
of false-negative results, however.
4. Children with normal PSG should also be followed up to determine if symptoms of
OSA appear and if any possible complications of snoring, such as hypertension
and neurocognitive behavioral problems, emerge.
5. Children with positive overnight PSG or other abbreviated studies should be
treated according to the underlying causes. One should take note that an individual
patient can have multiple causes of OSA (Table 5).
6. Overnight PSG should be repeated after treatment to determine whether additional
therapy is required.
Even though our understanding and knowledge of childhood OSA have expanded
exponentially over the past few years, there are still many unanswered diagnostic
and mechanistic questions on the condition. Recent evidence indicates that childhood
OSA cannot be easily classified into simple clinical entities. The associated symptoms
in children may vary and, many times, are difficult to detect. The diagnosis of the con-
dition in children is far from being straightforward, with the use of PSG in separating
snoring children into categories being a gross simplification. Further advancement in
this important field of pediatric medicine can only be made with international collabo-
rative research using evidence-based definitions, standardized techniques, and diag-
nostic criteria. Further research work should give a better insight of the origins of adult
morbidity resulting from childhood sleep-related breathing problems and how they
can be prevented.
REFERENCES
1. American Academy of Pediatrics. Clinical practice guideline: diagnosis and
management of childhood obstructive sleep apnea syndrome. Pediatrics
2002;109(4):70412.
2. American Thoracic Society. Standards and indications for cardiopulmonary
sleep studies in children. Am J Respir Crit Care Med 1996;153(2):86678.
3. Lumeng JC, Chervin RD. Epidemiology of pediatric obstructive sleep apnea.
Proc Am Thorac Soc 2008;5(2):24252.
4. Ali NJ, Pitson DJ, Stradling JR. Snoring, sleep disturbance, and behaviour in
45 year olds. Arch Dis Child 1993;68(3):3606.
5. Gislason T, Benediktsd
ottir B. Snoring, apneic episodes, and nocturnal hypox-
emia among children 6 months to 6 years old. An epidemiologic study of lower
limit of prevalence. Chest 1995;107(4):9636.
6. Redline S, Tishler PV, Schluchter M, et al. Risk factors for sleep-disordered
breathing in children. Associations with obesity, race, and respiratory problems.
Am J Respir Crit Care Med 1999;159(5 Pt 1):152732.
7. Brunetti L, Rana S, Lospalluti ML, et al. Prevalence of obstructive sleep apnea
syndrome in a cohort of 1,207 children of southern Italy. Chest 2001;120(6):
19305.
8. Anuntaseree W, Rookkapan K, Kuasirikul S, et al. Snoring and obstructive sleep
apnea in Thai school-age children: prevalence and predisposing factors. Pediatr
Pulmonol 2001;32(3):2227.
9. S
anchez-Armengol A, Fuentes-Pradera MA, Capote-Gil F, et al. Sleep-related
breathing disorders in adolescents aged 12 to 16 years: clinical and polygraphic
findings. Chest 2001;119(5):1393400.
Au & Li 254
10. Ng DK, Kwok KL, Poon G, et al. Habitual snoring and sleep bruxism in
a paediatric outpatient population in Hong Kong. Singapore Med J 2002;
43(11):5546.
11. Castronovo V, Zucconi M, Nosetti L, et al. Prevalence of habitual snoring and
sleep-disordered breathing in preschool-aged children in an Italian community.
J Pediatr 2003;142(4):37782.
12. Rosen CL, Larkin EK, Kirchner HL, et al. Prevalence and risk factors for sleep-
disordered breathing in 8- to 11-year-old children: association with race and
prematurity. J Pediatr 2003;142(4):3839.
13. OBrien LM, Holbrook CR, Mervis CB, et al. Sleep and neurobehavioral charac-
teristics of 5- to 7-year-old children with parentally reported symptoms of
attention-deficit/hyperactivity disorder. Pediatrics 2003;111(3):55463.
14. Kaditis AG, Finder J, Alexopoulos EI, et al. Sleep-disordered breathing in 3,680
Greek children. Pediatr Pulmonol 2004;37(6):499509.
15. Sogut A, Altin R, Uzun L, et al. Prevalence of obstructive sleep apnea syndrome
and associated symptoms in 311-year-old Turkish children. Pediatr Pulmonol
2005;39(3):2516.
16. Anuntaseree W, Kuasirikul S, Suntornlohanakul S. Natural history of snoring and
obstructive sleep apnea in Thai school-age children. Pediatr Pulmonol 2005;
39(5):41520.
17. Brooks LJ, Stephens BM, Bacevice AM. Adenoid size is related to severity but
not the number of episodes of obstructive apnea in children. J Pediatr 1998;
132(4):6826.
18. Fernbach SK, Brouillette RT, Riggs TW, et al. Radiologic evaluation of adenoids
and tonsils in children with obstructive sleep apnea: plain films and fluoroscopy.
Pediatr Radiol 1983;13(5):25865.
19. Laurikainen E, Erkinjuntti M, Alihanka J, et al. Radiological parameters of the
bony nasopharynx and the adenotonsillar size compared with sleep apnea
episodes in children. Int J Pediatr Otorhinolaryngol 1987;12(3):30310.
20. Huang J, Colrain IM, Melendres MC, et al. Cortical processing of respiratory
afferent stimuli during sleep in children with the obstructive sleep apnea
syndrome. Sleep 2008;31(3):40310.
21. Tangel DJ, Mezzanotte WS, White DP. Influence of sleep on tensor palatini EMG
and upper airway resistance in normal men. J Appl Phys 1991;70(6):257481.
22. Wiegand DA, Latz B, Zwillich CW, et al. Upper airway resistance and geniohyoid
muscle activity in normal men during wakefulness and sleep. J Appl Phys 1990;
69(4):125261.
23. Marcus CL, McColley SA, Carroll JL, et al. Upper airway collapsibility in chil-
dren with obstructive sleep apnea syndrome. J Appl Phys 1994;77(2):
91824.
24. Marcus CL. Pathophysiology of childhood obstructive sleep apnea: current
concepts. Respir Physiol 2000;119(23):14354.
25. Carroll JL, McColley SA, Marcus CL, et al. Inability of clinical history to distin-
guish primary snoring from obstructive sleep apnea syndrome in children. Chest
1995;108(3):6108.
26. Li AM, Hui S, Wong E, et al. Obstructive sleep apnoea in children with ad-
enotonsillar hypertrophy: prospective study. Hong Kong Med J 2001;7(3):
23640.
27. Goh DY, Galster P, Marcus CL. Sleep architecture and respiratory disturbances
in children with obstructive sleep apnea. Am J Respir Crit Care Med 2000;
162(2 Pt 1):6826.
Obstructive Sleep Breathing Disorders 255
28. Beebe DW. Neurobehavioral morbidity associated with disordered breathing
during sleep in children: a comprehensive review. Sleep 2006;29(9):111534.
29. Gozal D. Sleep-disordered breathing and school performance in children.
Pediatrics 1998;102(3 Pt 1):61620.
30. Chervin RD, Archbold KH, Dillon JE, et al. Inattention, hyperactivity, and
symptoms of sleep-disordered breathing. Pediatrics 2002;109(3):44956.
31. Chervin RD, Ruzicka DL, Giordani BJ, et al. Sleep-disordered breathing, behav-
ior, and cognition in children before and after adenotonsillectomy. Pediatrics
2006;117(4):e76978.
32. Gozal D, Pope DW Jr. Snoring during early childhood and academic
performance at ages thirteen to fourteen years. Pediatrics 2001;107(6):
13949.
33. Chervin RD, Dillon JE, Bassetti C, et al. Symptoms of sleep disorders,
inattention, and hyperactivity in children. Sleep 1997;20(12):118592.
34. Hiscock H, Canterford L, Ukoumunne OC, et al. Adverse associations of sleep
problems in Australian preschoolers: national population study. Pediatrics
2007;119(1):8693.
35. Owens JA, Mehlenbeck R, Lee J, et al. Effect of weight, sleep duration, and
comorbid sleep disorders on behavioral outcomes in children with sleep-disor-
dered breathing. Arch Pediatr Adolesc Med 2008;162(4):31321.
36. Peppard PE, Young T, Palta M, et al. Prospective study of the association
between sleep-disordered breathing and hypertension. N Engl J Med 2000;
342(19):137884.
37. Marcus CL, Greene MG, Carroll JL. Blood pressure in children with obstructive
sleep apnea. Am J Respir Crit Care Med 1998;157(4 Pt 1):1098103.
38. Amin RS, Carroll JL, Jeffries JL, et al. Twenty-four-hour ambulatory blood pres-
sure in children with sleep-disordered breathing. Am J Respir Crit Care Med
2004;169(8):9506.
39. Guilleminault C, Khramsov A, Stoohs RA, et al. Abnormal blood pressure in
prepubertal children with sleep-disordered breathing. Pediatr Res 2004;55(1):
7684.
40. Kohyama J, Ohinata JS, Hasegawa T. Blood pressure in sleep disordered
breathing. Arch Dis Child 2003;88(2):13942.
41. Enright PL, Goodwin JL, Sherrill DL, et al. Tucson childrens assessment of sleep
apnea study. Blood pressure elevation associated with sleep-related breathing
disorder in a community sample of white and Hispanic children: the Tucson chil-
drens assessment of sleep apnea study. Arch Pediatr Adolesc Med 2003;
157(9):9014.
42. Leung LC, Ng DK, Lau MW, et al. Twenty-four-hour ambulatory BP in snor-
ing children with obstructive sleep apnea syndrome. Chest 2006;130(4):
100917.
43. Zintzaras E, Kaditis AG. Sleep-disordered breathing and blood pressure in
children: a meta-analysis. Arch Pediatr Adolesc Med 2007;161(2):1728.
44. Li AM, Au CT, Sung RY, et al. Ambulatory blood pressure in children with
obstructive sleep apnoeaa community based study. Thorax 2008;63(9):8039.
45. Amin R, Somers VK, McConnell K, et al. Activity-adjusted 24-hour ambulatory
blood pressure and cardiac remodeling in children with sleep disordered
breathing. Hypertension 2008;51(1):8491.
46. Amin RS, Kimball TR, Bean JA, et al. Left ventricular hypertrophy and abnormal
ventricular geometry in children and adolescents with obstructive sleep apnea.
Am J Respir Crit Care Med 2002;165(10):13959.
Au & Li 256
47. Amin RS, Kimball TR, Kalra M, et al. Left ventricular function in children with
sleep-disordered breathing. Am J Cardiol 2005;95(6):8014.
48. S
anchez-Armengol A, Rodrguez-Puras MJ, Fuentes-Pradera MA, et al.
Echocardiographic parameters in adolescents with sleep-related breathing
disorders. Pediatr Pulmonol 2003;36(1):2733.
49. Tal A, Leiberman A, Margulis G, et al. Ventricular dysfunction in children with
obstructive sleep apnea: radionuclide assessment. Pediatr Pulmonol 1988;
4(3):13943.
50. Shiomi T, Guilleminault C, Stoohs R, et al. Obstructed breathing in children
during sleep monitored by echocardiography. Acta Paediatr 1993;82(10):
86371.
51. Blacher J, Asmar R, Djane S, et al. Aortic pulse wave velocity as a marker of
cardiovascular risk in hypertensive patients. Hypertension 1999;33(5):11117.
52. Kwok KL, Ng DK, Cheung YF. BP and arterial distensibility in children with
primary snoring. Chest 2003;123(5):15616.
53. Gozal D, Kheirandish-Gozal L, Serpero LD, et al. Obstructive sleep apnea and
endothelial function in school-aged nonobese children: effect of adenotonsillec-
tomy. Circulation 2007;116(20):230714.
54. Vivian EM. Type 2 diabetes in children and adolescentsthe next epidemic?
Curr Med Res Opin 2006;22(2):297306.
55. Gahagan S, Silverstein J. American Academy of Pediatrics Committee on Native
American Child Health; American Academy of Pediatrics Section on Endocrinol-
ogy. Prevention and treatment of type 2 diabetes mellitus in children, with
special emphasis on American Indian and Alaska Native children. American
Academy of Pediatrics Committee on Native American Child Health. Pediatrics
2003;112(4):e32847.
56. Tresaco B, Bueno G, Pineda I, et al. Homeostatic model assessment (HOMA)
index cut-off values to identify the metabolic syndrome in children. J Physiol
Biochem 2005;61(2):3818.
57. Cook S, Weitzman M, Auinger P, et al. Prevalence of a metabolic syndrome
phenotype in adolescents: findings from the Third National Health and Nutrition
Examination Survey, 19881994. Arch Pediatr Adolesc Med 2003;157(8):
8217.
58. Weiss R, Dziura J, Burgert TS, et al. Obesity and the metabolic syndrome in
children and adolescents. N Engl J Med 2004;350(23):236274.
59. Srinivasan SR, Myers L, Berenson GS. Predictability of childhood adiposity and
insulin for developing insulin resistance syndrome (syndrome X) in young adult-
hood: the Bogalusa Heart Study. Diabetes 2002;51(1):2049.
60. Cruz ML, Huang TT, Johnson MS, et al. Insulin sensitivity and blood pressure in
black and white children. Hypertension 2002;40(1):1822.
61. Punjabi NM, Sorkin JD, Katzel LI, et al. Sleep-disordered breathing and insulin
resistance in middle-aged and overweight men. Am J Respir Crit Care Med
2002;165(5):67782.
62. Ip MS, Lam B, Ng MM, et al. Obstructive sleep apnea is independently associ-
ated with insulin resistance. Am J Respir Crit Care Med 2002;165(5):6706.
63. Tauman R, OBrien LM, Ivanenko A, et al. Obesity rather than severity of sleep-
disordered breathing as the major determinant of insulin resistance and altered
lipidemia in snoring children. Pediatrics 2005;116(1):e6673.
64. Kaditis AG, Alexopoulos EI, Damani E, et al. Obstructive sleep-disordered
breathing and fasting insulin levels in nonobese children. Pediatr Pulmonol
2005;40(6):51523.
Obstructive Sleep Breathing Disorders 257
65. de la Eva RC, Baur LA, Donaghue KC, et al. Metabolic correlates with obstruc-
tive sleep apnea in obese subjects. J Pediatr 2002;140(6):6549.
66. Li AM, Chan MH, Chan DF, et al. Insulin and obstructive sleep apnea in obese
Chinese children. Pediatr Pulmonol 2006;41(12):117581.
67. Verhulst SL, Schrauwen N, Haentjens D, et al. Sleep-disordered breathing and
the metabolic syndrome in overweight and obese children and adolescents.
J Pediatr 2007;150(6):60812.
68. Gozal D, Sans Capdevila O, Kheirandish-Gozal L. Metabolic alterations in
obstructive sleep apnea among non-obese and obese prepubertal children.
Am J Respir Crit Care Med 2008;117(10):11429.
69. Li AM, Yin J, Chan D, et al. Sleeping energy expenditure in paediatric
patients with obstructive sleep apnoea syndrome. Hong Kong Med J 2003;
9(5):3536.
70. Marcus CL, Carroll JL, Koerner CB, et al. Determinants of growth in children with
the obstructive sleep apnea syndrome. J Pediatr 1994;125(4):55662.
71. Bland RM, Bulgarelli S, Ventham JC, et al. Total energy expenditure in children
with obstructive sleep apnoea syndrome. Eur Respir J 2001;18(1):1649.
72. Bar A, Tarasiuk A, Segev Y, et al. The effect of adenotonsillectomy on serum
insulin-like growth factor-I and growth in children with obstructive sleep apnea
syndrome. J Pediatr 1999;135(1):7680.
73. Parish JM, Somers VK. Obstructive sleep apnea and cardiovascular disease.
Mayo Clin Proc 2004;79(8):103646.
74. Ryan S, Taylor CT, McNicholas WT. Selective activation of inflammatory path-
ways by intermittent hypoxia in obstructive sleep apnea syndrome. Circulation
2005;112(17):26607.
75. Alberti A, Sarchielli P, Gallinella E, et al. Plasma cytokine levels in patients with
obstructive sleep apnea syndrome: a preliminary study. J Sleep Res 2003;
12(4):30511.
76. Vgontzas AN, Papanicolaou DA, Bixler EO, et al. Elevation of plasma cytokines
in disorders of excessive daytime sleepiness: role of sleep disturbance and
obesity. J Clin Endocrinol Metab 1997;82(5):13136.
77. Kataoka T, Enomoto F, Kim R, et al. The effect of surgical treatment of obstructive
sleep apnea syndrome on the plasma TNF-alpha levels. Tohoku J Exp Med
2004;204(4):26772.
78. Ohga E, Tomita T, Wada H, et al. Effects of obstructive sleep apnea on circulat-
ing ICAM-1, IL-8, and MCP-1. J Appl Phys 2003;94(1):17984.
79. Yokoe T, Minoguchi K, Matsuo H, et al. Elevated levels of C-reactive protein
and interleukin-6 in patients with obstructive sleep apnea syndrome are de-
creased by nasal continuous positive airway pressure. Circulation 2003;
107(8):112934.
80. Tauman R, Ivanenko A, OBrien LM, et al. Plasma C-reactive protein levels
among children with sleep-disordered breathing. Pediatrics 2004;113(6):
e5649.
81. Larkin EK, Rosen CL, Kirchner HL, et al. Variation of C-reactive protein levels in
adolescents: association with sleep-disordered breathing and sleep duration.
Circulation 2005;111(15):197884.
82. Tam CS, Wong M, McBain R, et al. Inflammatory measures in children with
obstructive sleep apnoea. J Paediatr Child Health 2006;42(5):27782.
83. Kaditis AG, Alexopoulos EI, Kalampouka E, et al. Morning levels of C-reactive
protein in children with obstructive sleep-disordered breathing. Am J Respir
Crit Care Med 2005;171(3):2826.
Au & Li 258
84. Juge-Aubry CE, Henrichot E, Meier CA. Adipose tissue: a regulator of inflamma-
tion. Best Pract Res Clin Endocrinol Metab 2005;19(4):54766.
85. Kheirandish-Gozal L, Capdevila OS, Tauman R, et al. Plasma C-reactive protein
in nonobese children with obstructive sleep apnea before and after adenotonsil-
lectomy. J Clin Sleep Med 2006;2(3):3014.
86. Gozal D, Serpero LD, Sans Capdevila O, et al. Systemic inflammation in non-
obese children with obstructive sleep apnea. Sleep Med 2008;9(3):2549.
87. Tauman R, Serpero LD, Capdevila OS, et al. Adipokines in children with sleep
disordered breathing. Sleep 2007;30(4):4439.
88. OBrien LM, Serpero LD, Tauman R, et al. Plasma adhesion molecules in children
with sleep-disordered breathing. Chest 2006;129(4):94753.
89. Marcus CL, Omlin KJ, Basinki DJ, et al. Normal polysomnographic values for
children and adolescents. Am Rev Respir Dis 1992;146(5 Pt 1):12359.
90. American Academy of Sleep Medicine. The international classification of sleep dis-
orders, diagnostic and coding manual. 2nd edition. Westchester (IL): American
Academy of Sleep Medicine; 2005. p. 58.
91. Sclafani AP, Ginsburg J, Shah MK, et al. Treatment of symptomatic chronic
adenotonsillar hypertrophy with amoxicillin/clavulanate potassium: short- and
long-term results. Pediatrics 1998;101(4 Pt 1):67581.
92. Don DM, Goldstein NA, Crockett DM, et al. Antimicrobial therapy for children
with adenotonsillar hypertrophy and obstructive sleep apnea: a prospective ran-
domized trial comparing azithromycin vs placebo. Otolaryngol Head Neck Surg
2005;133(4):5628.
93. Brouillette RT, Manoukian JJ, Ducharme FM, et al. Efficacy of fluticasone nasal
spray for pediatric obstructive sleep apnea. J Pediatr 2001;138(6):83844.
94. Demain JG, Goetz DW. Pediatric adenoidal hypertrophy and nasal airway
obstruction: reduction with aqueous nasal beclomethasone. Pediatrics 1995;
95(3):35564.
95. Kiely JL, Nolan P, McNicholas WT. Intranasal corticosteroid therapy for obstruc-
tive sleep apnoea in patients with co-existing rhinitis. Thorax 2004;59(1):505.
96. Goldbart AD, Goldman JL, Veling MC, et al. Leukotriene modifier therapy for
mild sleep-disordered breathing in children. Am J Respir Crit Care Med 2005;
172(3):36470.
97. Kheirandish L, Goldbart AD, Gozal D. Intranasal steroids and oral leukotriene
modifier therapy in residual sleep-disordered breathing after tonsillectomy and
adenoidectomy in children. Pediatrics 2006;117(1):e616.
98. Kirk V, Kahn A, Brouillette RT. Diagnostic approach to obstructive sleep apnea in
children. Sleep Med Rev 1998;2(4):25569.
99. Tauman R, Gulliver TE, Krishna J, et al. Persistence of obstructive sleep apnea
syndrome in children after adenotonsillectomy. J Pediatr 2006;149(6):8038.
100. Amin R, Anthony L, Somers V, et al. Growth velocity predicts recurrence of
sleep-disordered breathing 1 year after adenotonsillectomy. Am J Respir Crit
Care Med 2008;177(6):6549.
101. Shine NP, Coates HL, Lannigan FJ. Obstructive sleep apnea, morbid obesity,
and adenotonsillar surgery: a review of the literature. Int J Pediatr Otorhinolar-
yngol 2005;69(11):147582.
102. Marcus CL, Rosen G, Ward SL, et al. Adherence to and effectiveness of positive
airway pressure therapy in children with obstructive sleep apnea. Pediatrics
2006;117(3):e44251.
Obstructive Sleep Breathing Disorders 259
Chroni c Respi ratory
Fai l ure and
Neuromuscul ar Di sease
J. Declan Kennedy, MD, FRCP, FRACP
a,b,
*,
A. James Martin, MRCP, FRACP
b
Over the past 2 decades, there have been significant developments in the understand-
ing of the pathophysiology and management of respiratory complications of neuro-
muscular disorders (NMDs) in children, resulting in an increase in life expectancy,
reduction in hospital admissions, and increase in the quality of life for the patient
and his or her caregivers. A major driver of these changes has been the availability
of sophisticated technology to investigate and treat affected children. Other important
factors include recognition that affected children require close monitoring by a well-
coordinated multidisciplinary team, timely use of airway clearance techniques,
improved recognition of those at risk for respiratory failure, and the provision of
noninvasive ventilation (NIV) for those in respiratory failure. Expert assessment and
management of orthopedic, nutritional, and cardiac complications of NMDs have
also added to improved prognosis (Table 1).
Despite advances in clinical practice and undoubtedly improved prognosis, the
evidence on which some management principles are based is relatively sparse, with
the number of consensus statements on the use of NIV in children exceeding that
of randomized trials of its use. There is, however, no doubt that the outlook for a child
with significant respiratory muscle weakness in this decade is markedly improved,
with the mean age of survival in Duchenne muscular dystrophy (DMD) increasing by
30% from 19 to 25 years.
1
Even for those with the most severe disorder, type 1 spinal
muscular atrophy (SMA-1), the prognosis for those treated in some specialized
a
Discipline of Paediatrics, Faculty of Health Sciences, Medical School, University of Adelaide,
South Australia 5005, Australia
b
Department of Pulmonary Medicine, University of Adelaide, Womens and Childrens Hospi-
tal, 72 King William Road, North Adelaide, South Australia 5006, Australia
* Corresponding author. Department of Pulmonary Medicine, University of Adelaide, Womens
and Childrens Hospital, 72 King William Road, North Adelaide, South Australia, 5006,
Australia.
E-mail address: declan.kennedy@adelaide.edu.au (J.D. Kennedy).
KEYWORDS
Noninvasive ventilation
Neuromuscular disease
Respiratory failure
Child health
Pathophysiology
Pediatr Clin N Am 56 (2009) 261273
doi:10.1016/j.pcl.2008.10.011 pediatric.theclinics.com
0031-3955/08/$ seefront matter. CrownCopyright 2009PublishedbyElsevier Inc. All rights reserved.
centers has improved from 9.6 4.0 months of age to 65.2 45.8 months of age
(range: 11153 months).
2
The increase in longevity has and is bringing its own
challenges to patients, caregivers, and the health system.
3
The picture is further
complicated by variation in service provision between and within countries based
on available resources and different ethical views.
The primary purpose of this article is to review the principles of pathophysiology, in-
vestigation, and management of the respiratory complications of children with NMDs.
The management of orthopedic, nutritional, and cardiac complications is not within
the remit of this review. NMDs of childhood can be broadly classified into muscular
dystrophies, metabolic and congenital myopathies, anterior horn cell disorders, pe-
ripheral neuropathies, and diseases affecting the neuromuscular junction. The two dis-
orders that are the most common and exemplify the important principles of
assessment, investigation, and management that apply to all these disorders are
DMD and SMA. This review concentrates on these two conditions.
Table1
Grading of evidence of interventions in respiratory care of children who have neuromuscular
disorders
Assessment/Intervention Recommendation
Grading of
Recommendation
Quality of
Supporting Evidence
Symptoms or signs of
respiratory failure
Close clinical
monitoring of patient
Strong Strong
FVC <1 L Urgent respiratory
review because
survival risk is poor,
NIV if not previously
started
Strong Moderate
FVC <40% indicative
of nocturnal
hypoventilation
Refer for sleep study
or polysomnogram
Strong Weak
Maximal inspiratory
pressure <40 cm H
2
O
Polysomnogram with
evaluation of
day/night CO
2
levels
Moderate Weak
Peak cough flows
(PCFs) <270 L/min in
older children
Monitor patient closely
because there is a
risk for respiratory
failure with LRTI
Strong Strong
When wheelchair
bound
Overnight sleep
monitoring
Moderate Weak
Intervention:
supplemental oxygen
Not recommended Strong Moderate
If upper airway
obstruction but not
significant respiratory
muscle weakness
Adenotonsillectomy (or
CPAP if no
adenotonsillar
hypertrophy)
Moderate Weak
If acute respiratory
failure or chronic or
nocturnal and diurnal
hypercarbia
NIV Strong Moderate
Abbreviations: CO
2
, carbon dioxide; CPAP, continuous positive airway pressure; FVC, forced vital
capacity; LRTI, lower respiratory tract infection; PCF, peak cough flow.
Kennedy & Martin 262
PHYSIOLOGIC EFFECTS OF RESPIRATORY MUSCLE WEAKNESS
Understanding the physiologic sequelae of evolving respiratory muscle weakness is
important because it facilitates the prediction and early recognition of symptoms
and physical signs, which are often subtle in slowly evolving neuromuscular condi-
tions.
4
The normal infant and young child are at a physiologic disadvantage compared
with older children and adults, and this is further compounded when respiratory mus-
cle weakness is superimposed. The lung is relatively stiff compared with the highly
compliant chest wall in infants and young children,
5
impeding the generation of ade-
quate tidal volumes.
6
In those with significant muscular weakness, however, func-
tional residual capacity (FRC) is not maintained because of an even more compliant
chest wall and failure to maintain inspiratory muscle tone, predisposing to airway clo-
sure and microatelectasis. Upper and lower airways are of smaller caliber in younger
children, with a greater amount of intrathoracic airway resistance occurring in the
smaller airways.
7
In addition, the large central airways are more collapsible because
of increased compliance.
7
The respiratory pump power is further challenged by the
younger childs horizontal ribs and reduced zone of apposition of the diaphragm.
8
Thus, any disease of the lower airways in a young child quickly brings added stress
to an already stressed system. If challenged, therefore, the infant with severe neuro-
muscular weakness cannot easily increase minute ventilation and respiratory failure
quickly follows. The infant also has poorer collateral ventilation. The pores of Kohn
and the other interalveolar pathways are not well developed; therefore any lower respi-
ratory disease adds further to compromise because the collateral channels are less
available for compensation.
9
Add to this the fact that infants have fewer alveoli in total
and reduced elastic recoil; thus, it is surprising that the infant with significant neuro-
muscular disease can breathe at all.
With the ongoing development of neuromuscular weakness, chest wall compliance
decreases because of the gradual stiffening of costosternal and costovertebral articula-
tions, which become ankylosed with lack of use.
10
In SMA-1, pectus excavatum de-
velops with concomitant paradoxical respiration because as the diaphragm contracts,
the abdomen expands and the anterior chest wall sinks in.
11
As patients who have
SMA-1 slowly get older, although still in infancy, respiratory muscles that are not func-
tioningat their optimal length tension relations because of weakness undergo significant
changes, with resultant loss of normal elasticity and plasticity.
11
When scoliosis de-
velops, lung volumes are further reduced, whereas the intercostal muscles are placed
at further mechanical disadvantage. The consensus view is that control of breathing is
normal in NMD, but in chronic respiratory failure a blunting of central chemoreceptors
is thought to occur as a result of chronic carbon dioxide (CO
2
) retention.
12
AIRWAY-PROTECTIVE MECHANISMS IN NEUROMUSCULAR WEAKNESS
With loss of expiratory muscle strength, cough power is reduced and is further com-
promised by inspiratory muscle weakness, because a precough inspiration in excess
of 60% of total lung capacity is optimally required.
13
Transmural airway pressures de-
crease, thereby reducing the cough flow transients that aid mucus clearance from the
airway, and bulbar weakness impairs glottis closure, thereby further impairing cough
strength.
13
If a lower respiratory tract infection is imposed on the vulnerable respiratory phys-
iology of a child with NMD, a marked increase in respiratory work occurs at a time
when the pump muscles are further weakened by the viral infection itself.
14,15
Airway
resistance increases as a result of increased airway secretions that cannot be effec-
tively cleared by an impaired cough. Lung compliance decreases as a result of
Chronic Respiratory Failure 263
increasing mucus plugging and atelectasis. Acute respiratory failure ensues, and the
child may succumb if not mechanically ventilated by NIV or an endotracheal tube. A
presentation that is an all too common scenario in childhood NMD is rushing the child
in acute respiratory failure attributable to a lower respiratory tract infection or pneumo-
nia to the emergency department. Incidences of 0.8 to 1 per year have been reported
in NMDs.
16
A similar presentation can also be the result of aspiration secondary to
swallowing dysfunction.
17
SLEEPAND RESPIRATORY FAILURE
It is during sleep that physiologic changes are magnified, thereby increasing the likeli-
hood of respiratory compromise. In normal children, while sleeping, the respiratory
pattern of wakefulness changes in a characteristic wayventilatory control inputs
from higher centers are lost; chemoreceptor, medullary, and cortical arousal center
sensitivity decreases; respiratory muscle power diminishes; and upper airway muscle
tone decreases. As a result, tidal volume decreases and there is a mild decrease in
oxygen saturation and increase in CO
2
.
18
During rapid eye movement (REM) sleep,
respiratory control is at its nadir, skeletal muscle atonia is maximal with loss of acces-
sory muscle power, and diaphragmatic function is maintained. Depending on the
severity and distribution of respiratory muscle weakness in a child with NMD, the
sleep-induced effects on muscle power are heightened as NMD-induced diaphrag-
matic weakness accentuates the normal muscle atonia of REM. Thus, in a child with
NMD, sleep does not knit up the ravelld sleeve of care but may, in a true sense, be
the death of each days life.
19
The net result of the physiologic changes outlined previously is the development in
NMD of hypoventilation, first during rapid eye movement sleep, then during no rapid
eye movement, and, subsequently, during wakefulness. Depending on the distribution
of respiratory muscle weakness, however, the pattern may vary. For example, if dia-
phragmatic function is not significantly impaired while upper airway musculature is
weak and tonsils and adenoids are enlarged, upper airway obstruction may predom-
inate during sleep.
18
SYMPTOMS AND SIGNS OF RESPIRATORYCOMPROMISE IN NEUROMUSCULAR DISORDERS
In severe early-onset respiratory muscle weakness, as encountered in SMA-1, phys-
ical examination may reveal a bell-shaped chest with tachypnea, paradoxical breath-
ing, and head bobbing in the context of severe generalized hypotonia. In more slowly
evolving respiratory failure, such as that of DMD, the development of symptoms may
be insidious and often missed. Those symptoms that should be specifically sought
relate to the effects of nocturnal hypoventilation with resultant hypoxia and sleep frag-
mentation, including daytime behavioral and neurocognitive problems, hyperactivity
or tiredness, morning headaches, nocturnal arousals and frequent repositioning,
and daytime sleepiness.
6,20
Anorexia at breakfast and cyanosis during meals and
on transfer from a wheelchair may also occur.
21
Symptoms may be poorly predictive
of sleep breathing difficulties, however.
22,23
Mellies and colleagues
4
recently reported
that a structured symptom questionnaire was poorly predictive of sleep-disordered
breathing (SDB) or nocturnal hypercapnic ventilation in a group of 49 children with
NMDs of varying etiologies. The deficit in general intellectual functioning in boys
with DMD further complicates ascertainment of significant symptoms, and in the clin-
ical setting of a pediatric outpatient visit, these boys often sit quietly with their parents
saying little about their concerns. Thus, in summary, symptoms of respiratory failure
are often not reported or are subtle and overlooked.
Kennedy & Martin 264
RESPIRATORY MONITORING IN CHILDHOOD NEUROMUSCULAR DISORDERS
Role of Lung Function Testing in Predicting Respiratory Failure
Serial monitoring of lung function is mandated for all children with NMD when it is able
to be performedusually after the age of 5 years.
24,25
The rate of decline in forced vital
capacity (FVC) in DMD is variable (2%39% per year), with a median of 8%, whereas
a FVC of less than 1 L in DMD is associated with a median survival of 3.1 years and
a 5-year survival rate of only 8%.
26
Bourke and Gibson
27
suggest that FVC may
be a better measure of overall survival in DMD than nocturnal hypoxia. A recent report
suggested that a FVC of greater than 60% represented a low risk for nocturnal
hypoventilation, whereas a FVC less than 40% was a good predictor of nocturnal
hypoventilation in children with NMDs of varying etiologies.
25
Daytime PaCO
2
levels
greater than 45 mm Hg, in combination with spirometry, have also been used to pre-
dict SDB,
28
whereas Mellies and colleagues
4
asserted that SDB with nocturnal hyper-
capnic hypoventilation could be predicted by a PaCO
2
greater than 40 mm Hg (92%
sensitivity, 72%specificity) and inspiratory vital capacity less than 40%(96% sensitiv-
ity, 88% specificity) in a group of 49 children and adolescents who had NMD of mixed
etiology (aged 11.3 4.4 years). These researchers also reported that a maximum
peak inspiratory pressure less than 4 kPa and less than 2.5 kPa predicted SDB onset
and nocturnal hypercapnia, respectively.
4
Similarly maximum expiratory mouth pres-
sure (MEP) has been used to measure effective cough capacity (MEP >60 cm H
2
O is
adequate, and MEP <45 cm H
2
O is insufficient),
29
whereas a maximum inspiratory
mouth pressure (MIP) less than 60 cm has been suggested as indicative of the need
to consider NIV.
30
Peak cough flows (PCFs) are now recognized as important mea-
sures of the capacity for mucociliary clearance. Consensus documents have accepted
270 L/min as the acceptable level of flow;
24,25
at greater than that level, there is a re-
duced risk for developing respiratory failure during upper respiratory tract infections,
whereas a level lower than that target value identifies patients who would benefit from
manually assisted cough techniques.
31
In adult patients who have NMD, however,
with PCF values of 270 L/min while well, these values often decrease to less than
160 L/min during acute viral infections,
31
a level insufficient to clear airway secretions.
The target PCF value of 270 L/min may not be appropriate for children because those
younger than 13 years of age are often not able to generate values of 270 L/min.
13
PCFs less than 270 L/min are more likely when FVC is <2.1 L in children who have
DMD.
32
It is worth noting that PCF can be increased by breath stacking.
In those with the most severe form of NMD, SMA-1, infant lung function testing is
technically demanding and untested in this clinical setting, but monitoring with poly-
somnography (PSG), or with oximetry if the former is not available, particularly during
sleep, is extremely helpful in assessing evolving respiratory muscle weakness and re-
sultant hypoventilation.
17
There is a clear consensus in the literature
24,25,30
that serial
monitoring of lung function is mandated for all children who are old enough to perform
it. For spirometric evaluation, MIP, MEP, and PCF, this is usually after the age of
5 years.
When to Refer for Specialized Respiratory Review
Although a recent American Thoracic Society consensus statement
24
recommended
that those who have DMD be reviewed by a pediatric respiratory physician twice
yearly after FVC has decreased to less than 80% of that predicted, or if aged 12 years
or when confined to a wheel chair, many respiratory pediatricians believe that they
should review all children with NMD after the diagnosis has been confirmed. This
allows the pediatric respiratory physician and respiratory team to meet with the family
Chronic Respiratory Failure 265
before respiratory complications have developed to discuss their potential evolution
and the methods of assessing and treating them. This is important to facilitate before
the family undertakes Internet surfing, wherein management techniques with
varying levels of scientific support may be promulgated. The frequency of specialized
respiratory assessment depends on clinical progress.
25
In children whose respiratory
muscle weakness is evolving more slowly, annual monitoring with spirometry and
overnight PSG is reasonable initially. The timing of further overnight studies may be
varied depending on the PSG results. The more difficult question to answer is when
to begin overnight monitoring, although guidelines are outlined elsewhere in this
article.
Timing of Polysomnography
In children who have DMD, consensus guidelines
24
suggest that overnight monitoring
should be considered fromthe time the child becomes a wheelchair user or when clin-
ically indicated. As outlined previously, symptoms of nocturnal hypoxemia and sleep
fragmentation may often be subtle. PSG should be considered annually when FVC is
less than 60% and more often if it is less than 40%. A MIP less than 60%
30
and
daytime PaCO
2
greater than 40 mm Hg
4
are also helpful in prompting a referral for
PSG evaluation. These target values are general guidelines only, because not infre-
quently in clinical practice, one sees children whose FVC is greater than 70% of
that predicted but whose PSGs demonstrate significant alveolar hypoventilation.
TREATMENT OF RESPIRATORY FAILURE IN NEUROMUSCULAR DISORDERS
Although one of the major changes in the treatment of respiratory failure in NMDs has
been the introduction of NIV, the literature evidence on which its effectiveness is
based is not clear-cut. In a recent Cochrane review, the conclusions of Annane and
colleagues
33
were that current evidence about the therapeutic benefit of mechanical
ventilation (in NMD) is weak, but directionally consistent suggesting alleviation of the
symptoms of chronic hypoventilation in the short term. They suggested that large
randomized trials were needed to confirmlong-termbeneficial effects of NIV on symp-
toms, quality of life, unplanned hospital admissions, and mortality and, finally, to eval-
uate its cost-effectiveness. For this review, only eight trials in the literature were
deemed eligible for evaluation because entry criteria dictated that they had to be qua-
sirandomized or randomized controlled studies and most patients studied were
adults. It is against this backdrop that one needs to consider the pros and cons of
NIV treatment in pediatric patients who have NMD.
Although noninvasive positive-pressure ventilation was first used in the 1960s,
34,35
it
was not until the 1980s, after the development of the continuous positive airway pres-
sure mask,
36
that Rideau and colleagues
37
in Europe and Bach and colleagues
35
in the
United States suggested that noninvasive positive-pressure ventilation (NIV) be used
to treat respiratory failure in NMD. With the subsequent development of suitable child-
rens masks, NIV gained acceptance in pediatric practice during the 1990s. In a recent
review of NIV in children, Norregaard
6
noted that knowledge of NIV application in chil-
dren depended in the main on reports of case series, with little firm evidence of when
to initiate NIV in this age group. It is also salutary to note howfar pediatric clinical prac-
tice has come since the findings of a consensus conference,
38
which reported that
nasal mask ventilation in young children must be considered an investigational tech-
nique for research and/or use only by experienced centers. Notwithstanding the con-
clusions of the Cochrane report outlined previously, NIV is now accepted as one of the
major strategies in the treatment of respiratory failure in children who have NMD and is
Kennedy & Martin 266
strongly supported by several consensus statements.
17,24,25
There is not a clear con-
sensus in the literature as to when one should initiate NIV, however.
EVIDENCE THAT NONINVASIVE VENTILATION IS EFFECTIVE IN RESPIRATORY
FAILURE IN NEUROMUSCULAR DISORDERS
The evidence for NIVs effectiveness in NMD is based mainly on case series, non-
randomized trials, and comparisons with historical controls. Despite this, the weight
of evidence is persuasive. Eagle and colleagues
1
reported that the mean age of death
in patients who had DMD and were treated with NIV had increased from19 to 25 years
when compared with historical controls who did not receive this treatment, whereas
Simonds and colleagues
39
found a one year and five year survival rate of 85% and
73%, respectively, in DMD patients treated with NIV. There are now a series of studies
that report improvements not only in survival but in symptoms of nocturnal hypoven-
tilation, gas exchange during the day and night, preservation of lung function, quality
of life, and frequency of hospital admissions.
21,31,3946
John Bach has been a tireless
advocate over many years of NIV in the treatment of respiratory failure in NMD, and his
results even in severe muscle weakness, such as SMA-1,
2,47
are impressive. He re-
ported that as a result of noninvasive management in his clinic (which included mon-
itoring of oximetry, mechanical-assisted coughing techniques, and short-term
intubations for acute respiratory infections), 80 of 115 patients who had SMA-1
were still alive without tracheostomy at 4 years, with 8 children older than 8 years of
age and 2 older than 10 years of age.
48
The management of children who have
SMA-1 is a highly controversial area, however, and as outlined by Bush and col-
leagues,
49
individual physicians may discourage long-term daytime NIV but many
will disagree with this approach in good faith. What Bachs approach may be dem-
onstrating is that with aggressive management of respiratory failure with NIV, close
monitoring of ventilation with oximetry, and the early introduction of mechanical-assis-
ted coughing in acute respiratory infections, the long-term outlook for many children
with neuromuscular weakness of varying etiologies may be enhanced.
WHEN TO START NONINVASIVE VENTILATION
There is little consensus in the literature regarding when to start NIV, with some
advocating its introduction if the patient is hypercapnic or hypoxic during sleep or
wakefulness (in DMD).
50
Others (in congenital muscular dystrophies, SMA-2, and
congenital myopathies) advocate its initiation in those with acute respiratory failure,
symptomatic diurnal hypercapnia or symptomatic nocturnal hypoventilation in the ab-
sence of daytime hypercapnia, failure to thrive, or more than three chest infections per
year, with its use in nonsymptomatic nocturnal hypercapnia or hypopnea being con-
sidered on an individual basis.
25
As outlined previously, symptoms are often subtle.
Mallory
51
suggests that its use should commence early, that is, before the onset of
respiratory failure. The American Thoracic Society consensus statement
24
suggests
that NIV be used to treat sleep-related upper airway obstruction and chronic respira-
tory insufficiency in DMD, although no definitive guidelines are given as to levels of
severity that would mandate NIV. A second consensus statement
30
suggests NIV
use in NMD if the patient has symptoms, such as fatigue, morning headache, and
one of the following: (1) PaCO
2
of 45 mm Hg or greater, (2) nocturnal oxygen saturation
of 88% or less for 5 consecutive minutes, or (3) maximal inspiratory pressures less
than 60 cm H
2
O or FVC less than 50% of that predicted. Ward and colleagues
44
make the point that these recommendations are not based on controlled studies
and that the oxygen saturation guidelines were not based on evidence but partly on
Chronic Respiratory Failure 267
Medicare guidelines for oxygen therapy in chronic obstructive pulmonary disease.
52
These researchers performed one of the few randomized controlled trials of NIV in
a group of patients who had NMD (of mixed etiology).
44
They randomized 26 subjects,
aged 7 to 51 years, with an FVC less than 50% of that predicted with nocturnal hyper-
capnia (peak TcCO
2
>6.5 kPa) but normal daytime CO
2
levels to nocturnal NIV or to
a control group without NIV. Nocturnal ventilation improved in the treated group, but 9
of 10 controls needed NIV after a mean of 8.3 months (SD 5 7.3). These findings sup-
port the conclusion that once nocturnal hypoventilation is present, NIV treatment
should be considered.
40
A recent index, the Breathing Intolerance Index, was devel-
oped by Koga and colleagues
53
calculated from the formula of inspiratory time (T
i
) di-
vided by total respiratory time (T
tot
), multiplied by the result of tidal volume (V
t
) divided
by vital capacity (VC) [ie, (T
i
/T
tot
) (V
t
/VC)]. These investigators found that a value
greater than 0.15 was noted for all subjects on NIV.
One of the studies often quoted in the literature as demonstrating the possible haz-
ard of initiating NIV early is that of Raphael and colleagues.
54
Its importance lies in its
being one of the few randomized trials of NIV use in children. These researchers aim
was to evaluate the use of prophylactic NIV in a group of 70 teenaged patients who
had DMD with a FVC from 20% to 50% of that predicted and who had not developed
diurnal hypercapnia by randomizing them to NIV or standard treatment. The worrying
result was a fourfold increase in mortality in the NIV group, with most resulting from
respiratory infections. These investigators thought that the putative reason for the
increase in mortality was the false sense of security in patients using NIV, thereby re-
sulting in a delay in seeking medical help during a significant respiratory infection. The
study has subsequently been criticized by many investigators for limitations in design
and analysis, including failure to document patient compliance with NIV or to use as-
sisted cough techniques, a higher proportion of patients with cardiac dysfunction in
the NIV group,
52
and the absence of PSG data before and after NIV initiation.
55
The initiation of NIV should optimally be electively planned after discussions with
family and patients. Unfortunately, in practice, this is not always what happens. Sritip-
payawan and colleagues
56
reported that of 73 children who had NMD of mixed etiol-
ogies, only 21% had NIV commenced electively. Some authorities have suggested
that the reticence to discuss long-term ventilatory support with patients might be
because of health providers assessments of the patients poor quality of life.
57,58
As outlined by Kohler and colleagues,
59
however, even patients who have DMD
with advanced muscle weakness report a high quality of life despite their illness, which
was not correlated with physical limitation or need for NIV.
The long-term positive effects of NIV in children who have NMD have been demon-
strated in two recent studies. Mellies and colleagues
43
reported that in 30 patients who
had NMD of varying etiologies, NIV normalized nocturnal and daytime gas exchange
and sleep and that the effects persisted over 25.3 12.7 months. In 15 children who
had varying types of NMD, Katz and colleagues
45
found that over at least a 1-year
period, NIV resulted in an 85% reduction in days in the hospital and a 68% reduction
in days in intensive care. The physiologic reasons for this improvement in respiratory
failure parameters have been recently explored by Nickol and colleagues,
60
who found
that increased ventilatory response to CO
2
was the main contributor. An intriguing as-
pect of NIV use is its possible positive effects on lung and chest wall growth. Bach and
Bianchi
11
have advocated its use for this purpose, suggesting high span positive in-
spiratory pressure plus positive end-expiratory pressure to improve lung compliance
and prevent pectus excavatum in SMA-1. The effectiveness of NIV in promoting lung
and chest wall growth awaits further elucidation. The long-term potential effect of NIV
on facial development also needs to be remembered because a recent study of
Kennedy & Martin 268
40 children using NIV (cystic fibrosis [n 5 10], obstructive sleep apnea [n 5 16], and
NMD [n 5 14]) found a prevalence of global facial flattening in 68%. No correlation
was found with age or daily or cumulative use of NIV.
61
The increasing use of NIV in neuromuscular disease in children must be seen
against the background of other developments that have, in concert, improved the
quality and quantity of life for affected children. The importance of airway clearance
methods using manual-assisted techniques (manual-assisted coughing with
increased inspiratory capacity facilitated by glossopharyngeal breathing, breath
stacking, or self-inflating bag and mask) has been highlighted in recent studies and
consensus statements.
24,25,31
In addition, mechanical insufflator-exsufflators play an
important role in mobilizing airway secretions, especially in those whose PCFs are in-
effective, and their efficacy in NMD has been highlighted in several recent stud-
ies.
31,6264
Chatwin and colleagues
65
demonstrated in 22 patients with NMD, 8 of
whom were children, that the insufflator-exsufflator produced a greater increase in
PCFs than voluntary unassisted cough or cough assisted by physiotherapy or nonin-
vasive positive-pressure ventilation. Two newer mucus clearance devices whose
benefit awaits clarification include high-frequency chest wall oscillation and intrapul-
monary percussive ventilation.
66,67
The continued improvement in outlook from a respiratory point of view for children
who have NMD has also been aided by the early use of antibiotics in acute respiratory
infections, influenza, and pneumococcal vaccinations; improved intensive care tech-
niques; and specialized regional care centers. Nonrespiratory interventions, such as
the use of oral steroids in DMD to improve muscle strength and respiratory function
68
(although not uniformly accepted),
24
surgical correction of scoliosis,
69
early interven-
tion and treatment of cardiac dysfunction,
70,71
recognition and treatment of gastro-
esophageal reflux and aspiration,
17
close monitoring of nutritional status, and
intervention with gastrostomy in those failing to thrive
24
are all integral to optimal
management of these complex patients.
In summary, the management of respiratory complications of children who have
neuromuscular disease has markedly improved in the past 15 years. The reasons
for this are many and include a better appreciation of the symptoms of hypoventilation
during sleep, which are often subtle; a greater understanding of the importance of
close monitoring by a respiratory pediatrician with serial lung function testing and
overnight monitoring; the acceptance of the importance of NIV in treating acute and
chronic hypoventilation; and improved airway clearance techniques, including assis-
ted coughing and insufflator-exsufflators. The role of the respiratory pediatrician is
vital in coordinating all these aspects of care.
Further improvements in the quality and quantity of life for children who have
NMD are likely in the years ahead with gene- and cell-based treatments. This
should also have a significant impact on patients families and health systems.
Governments need to be made aware of the demands that are likely to be
made on the health systems as a result. There is an urgent need for improvement
in the home care and respite opportunities provided in addition to education and
skills training for young adults. We have come some way, but there is much to be
done.
ACKNOWLEDGMENTS
The authors gratefully acknowledge the assistance of Dr. Cameron van den Heuvel
at the University of Adelaide in formatting and proofreading this manuscript.
Chronic Respiratory Failure 269
REFERENCES
1. Eagle M, Baudouin SV, Chandler C, et al. Survival in Duchenne muscular dystro-
phy: improvements in life expectancy since 1967 and the impact of home noctur-
nal ventilation. Neuromuscul Disord 2002;12(10):9269.
2. Bach JR, Saltstein K, Sinquee D, et al. Long-term survival in Werdnig-Hoffmann
disease. Am J Phys Med Rehabil 2007;86(5):33945.
3. Birnkrant D. New challenges in the management of prolonged survivors of pedi-
atric neuromuscular diseases: a pulmonologists perspective. Pediatr Pulmonol
2006;41:11137.
4. Mellies U, Ragette R, Schwake C, et al. Daytime predictors of sleep disordered
breathing in children and adolescents with neuromuscular disorders. Neuromus-
cul Disord 2003;13(2):1238.
5. Papastamelos C, Panitch HB, Allen JL. Chest wall compliance in infants and chil-
dren with neuromuscular disease. Am J Respir Crit Care Med 1996;154(4 Pt 1):
10458.
6. Norregaard O. Noninvasive ventilation in children. Eur Respir J 2002;20(5):
133242.
7. Gaultier C. Developmental anatomy and physiology of the respiratory system. In:
Taussig LM, Landau L, Le Souef PN, et al, editors. Pediatric respiratory medicine.
St. Louis (MO): Mosby; 1999. p. 1837.
8. Devlieger H, Daniels H, Marchal G, et al. The diaphragm of the newborn infant:
anatomical and ultrasonographic studies. J Dev Physiol 1991;16(6):3219.
9. Rosenberg DE, Lyons HA. Collateral ventilation in excised human lungs. Respira-
tion 1979;37(3):12534.
10. Estenne M, Heilporn A, Delhez L, et al. Chest wall stiffness in patients with chronic
respiratory muscle weakness. Am Rev Respir Dis 1983;128(6):10027.
11. Bach JR, Bianchi C. Prevention of pectus excavatum for children with spinal
muscular atrophy type 1. Am J Phys Med Rehabil 2003;82(10):8159.
12. Perrin C, Unterborn JN, D Ambrosio CD, et al. Pulmonary complications of
chronic neuromuscular diseases and their management. Muscle Nerve 2004;
29(1):527.
13. Panitch HB. Respiratory issues in the management of children with neuromuscu-
lar disease. Respir Care 2006;51(8):88593.
14. Mier-Jedrzejowicz A, Brophy C, Green M. Respiratory muscle weakness during
upper respiratory tract infections. Am Rev Respir Dis 1988;138(1):57.
15. Poponick JM, Jacobs I, Supinski G, et al. Effect of upper respiratory tract infec-
tion in patients with neuromuscular disease. Am J Respir Crit Care Med 1997;
156(2 Pt 1):65964.
16. Bach JR, Rajaraman R, Ballanger F, et al. Neuromuscular ventilatory insufficiency:
effect of home mechanical ventilator use v oxygen therapy on pneumonia and
hospitalization rates. Am J Phys Med Rehabil 1998;77(1):819.
17. Wang CH, Finkel RS, Bertini ES, et al. Consensus statement for standard of care
in spinal muscular atrophy. J Child Neurol 2007;22(8):102749.
18. Givan D. Sleep and breathing in children with neuromuscular disease. In:
LoughlinGM, Carroll JL, Marcus CL, editors. Sleepandbreathinginchildrenade-
velopmental approach, vol. 147. New York: Marcel Dekker AG; 2000. p. 691735.
19. Macbeth, II, ii. Jaggard and Blount, First Folio. 1623.
20. Mellies U, Dohna-Schwake C, Ragette R, et al. [Nocturnal noninvasive ventilation
of children and adolescents with neuromuscular diseases: effect on sleep and
symptoms]. Wien Klin Wochenschr 2003;115(24):8559 [in German].
Kennedy & Martin 270
21. Simonds AK, Ward S, Heather S, et al. Outcome of paediatric domiciliary mask
ventilation in neuromuscular and skeletal disease. Eur Respir J 2000;16(3):
47681.
22. Young HK, Lowe A, Fitzgerald DA, et al. Outcome of noninvasive ventilation in
children with neuromuscular disease. Neurology 2007;68(3):198201.
23. Suresh S, Wales P, Dakin C, et al. Sleep related breathing disorder in Duchenne
muscular dystrophy: disease spectrum in the pediatric population. J Paediatr
Child Health 2005;41:5003.
24. Finder JD, Birnkrant D, Carl J, et al. Respiratory care of the patient with Duchenne
muscular dystrophy: ATS consensus statement. Am J Respir Crit Care Med 2004;
170(4):45665.
25. Wallgren-Pettersson C, Bushby K, Mellies U, et al. 117th ENMC workshop: venti-
latory support in congenital neuromuscular disorderscongenital myopathies,
congenital muscular dystrophies, congenital myotonic dystrophy and SMA (II).
46 April 2003, Naarden, The Netherlands. Neuromuscul Disord 2004;14(1):
5669.
26. Phillips MF, Quinlivan RC, Edwards RH, et al. Changes in spirometry over time as
a prognostic marker in patients with Duchenne muscular dystrophy. Am J Respir
Crit Care Med 2001;164(12):21914.
27. Bourke SC, Gibson GJ. Sleep and breathing in neuromuscular disease. Eur
Respir J 2002;19(6):1194201.
28. Hukins CA, Hillman DR. Daytime predictors of sleep hypoventilation in Duchenne
muscular dystrophy. Am J Respir Crit Care Med 2000;161(1):16670.
29. Szeinberg A, Tabachnik E, Rashed N, et al. Cough capacity in patients with mus-
cular dystrophy. Chest 1988;94(6):12325.
30. Consensus Conference. Clinical indications for noninvasive positive pressure
ventilation in chronic respiratory failurre due to restrictive lung disease, COPD,
and nocturnal hypoventilation. A consensus conference report. Chest 1999;
116:52134.
31. Tzeng AC, Bach JR. Prevention of pulmonary morbidity for patients with neuro-
muscular disease. Chest 2000;118(5):13906.
32. Gauld LM, Boynton A. Relationship between peak cough flow and spirometry in
Duchenne muscular dystrophy. Pediatr Pulmonol 2005;39(5):45760.
33. Annane D, Orlikowski D, Chevret S. Nocturnal mechanical ventilation for chronic
hypoventilation in patients with neuromuscular and chest wall disorders.
Cochrane Database Syst Rev 2007;(4):128.
34. Alba A, Khan A, Lee M. Mouth IPPV for sleep. Rehabilitation Gazette 1981;24:
479.
35. Bach JR, Alba A, Mosher R, et al. Intermittent positive pressure ventilation via na-
sal access in the management of respiratory insufficiency. Chest 1987;92(1):
16870.
36. Sullivan CE, Issa FG, Berthon-Jones M, et al. Reversal of obstructive sleep
apnoea by continuous positive airway pressure applied through the nares. Lan-
cet 1981;1(8225):8625.
37. Rideau Y, Gatin G, Bach J, et al. Prolongation of life in Duchennes muscular
dystrophy. Acta Neurol (Napoli) 1983;5(2):11824.
38. Make BJ, Hill NS, Goldberg AI, et al. Mechanical ventilation beyond the intensive
care unit. Report of a consensus conference of the American College of Chest
Physicians. Chest 1998;113(Suppl 5):289S344S.
39. Simonds AK, Muntoni F, Heather S, et al. Impact of nasal ventilation on survival in
hypercapnic Duchenne muscular dystrophy. Thorax 1998;53(11):94952.
Chronic Respiratory Failure 271
40. Simonds AK. Recent advances in respiratory care for neuromuscular disease.
Chest 2006;130(6):187986.
41. Vianello A, Bevilacqua M, Salvador V, et al. Long-term nasal intermittent positive
pressure ventilation in advanced Duchennes muscular dystrophy. Chest 1994;
105(2):4458.
42. Bach JR, Ishikawa Y, Kim H. Prevention of pulmonary morbidity for patients with
Duchenne muscular dystrophy. Chest 1997;112(4):10248.
43. Mellies U, Ragette R, Dohna Schwake C, et al. Long-term noninvasive ventilation
in children and adolescents with neuromuscular disorders. Eur Respir J 2003;
22(4):6316.
44. Ward S, Chatwin M, Heather S, et al. Randomised controlled trial of non-invasive
ventilation (NIV) for nocturnal hypoventilation in neuromuscular and chest wall
disease patients with daytime normocapnia. Thorax 2005;60(12):101924.
45. Katz S, Selvadurai H, Keilty K, et al. Outcome of non-invasive positive pressure ven-
tilation in paediatric neuromuscular disease. Arch Dis Child 2004;89(2):1214.
46. Dohna-Schwake C, Podlewski P, Voit T, et al. Non-invasive ventilation reduces
respiratory tract infections in children with neuromuscular disorders. Pediatr
Pulmonol 2008;43(1):6771.
47. Bach JR, Baird JS, Plosky D, et al. Spinal muscular atrophy type 1: management
and outcomes. Pediatr Pulmonol 2002;34(1):1622.
48. Bach JR. There are other ways to manage spinal muscular atrophy type 1. Chest
2005;127(4):1463.
49. Bush A, Fraser J, Jardine E, et al. Respiratory management of the infant with type
1 spinal muscular atrophy. Arch Dis Child 2005;90(7):70911.
50. Wagner KR, Lechtzin N, Judge DP. Current treatment of adult Duchenne muscu-
lar dystrophy. Biochim Biophys Acta 2007;1772(2):22937.
51. Mallory GB. Pulmonary complications of neuromuscular disease. Pediatr
Pulmonol Suppl 2004;26:13840.
52. Mehta S, Hill NS. Noninvasive ventilation. Am J Respir Crit Care Med 2001;163(2):
54077.
53. Koga T, Watanabe K, Sano M, et al. Breathing intolerance index. Am J Phys Med
Rehabil 2005;85:2430.
54. Raphael JC, Chevret S, Chastang C, et al. Randomised trial of preventive nasal
ventilation in Duchenne muscular dystrophy. French Multicentre Cooperative
Group on Home Mechanical Ventilation Assistance in Duchenne de Boulogne
Muscular Dystrophy. Lancet 1994;343(8913):16004.
55. Fauroux B, Lofaso F. Non-invasive mechanical ventilation: when to start for what
benefit? Thorax 2005;60(12):97980.
56. Sritippayawan S, Kun SS, Keens TG, et al. Initiation of home mechanical ventila-
tion in children with neuromuscular diseases. J Pediatr 2003;142(5):4815.
57. Bach JR, Campagnolo DI, Hoeman S. Life satisfaction of individuals with
Duchenne muscular dystrophy using long-term mechanical ventilatory support.
Am J Phys Med Rehabil 1991;70(3):12935.
58. Gibson B. Long-term ventilation for patients with Duchenne muscular dystrophy:
physicians beliefs and practices. Chest 2001;119(3):9406.
59. Kohler M, Clarenbach CF, Boni L, et al. Quality of life, physical disability, and re-
spiratory impairment in Duchenne muscular dystrophy. Am J Respir Crit Care
Med 2005;172(8):10326.
60. Nickol AH, Hart N, Hopkinson NS, et al. Mechanisms of improvement of respira-
tory failure in patients with restrictive thoracic disease treated with non-invasive
ventilation. Thorax 2005;60(9):75460.
Kennedy & Martin 272
61. Fauroux B, Lavis JF, Nicot F, et al. Facial side effects during noninvasive positive
pressure ventilation in children. Intensive Care Med 2005;31(7):9659.
62. Winck JC, Goncalves MR, Lourenco C, et al. Effects of mechanical insufflation-ex-
sufflation on respiratory parameters for patients with chronic airway secretion
encumbrance. Chest 2004;126(3):77480.
63. Bach JR, Niranjan V, Weaver B. Spinal muscular atrophy type 1: a noninvasive
respiratory management approach. Chest 2000;117(4):11005.
64. Miske LJ, Hickey EM, Kolb SM, et al. Use of the mechanical in-exsufflator in
pediatric patients with neuromuscular disease and impaired cough. Chest
2004;125(4):140612.
65. Chatwin M, Ross E, Hart N, et al. Cough augmentation with mechanical insuffla-
tion/exsufflation in patients with neuromuscular weakness. Eur Respir J 2003;
21(3):5028.
66. Plioplys AV, Lewis S, Kasnicka I. Pulmonary vest therapy in pediatric long-term
care. J Am Med Dir Assoc 2002;3(5):31821.
67. Toussaint M, De Win H, Steens M, et al. Effect of intrapulmonary percussive
ventilation on mucus clearance in Duchenne muscular dystrophy patients: a pre-
liminary report. Respir Care 2003;48(10):9407.
68. Biggar WD, Harris VA, Eliasoph L, et al. Long-term benefits of deflazacort
treatment for boys with Duchenne muscular dystrophy in their second decade.
Neuromuscul Disord 2006;16(4):24955.
69. Eagle M, Bourke J, Bullock R, et al. Managing Duchenne muscular dystrophy
the additive effect of spinal surgery and home nocturnal ventilation in improving
survival. Neuromuscul Disord 2007;17(6):4705.
70. Bushby K, Muntoni F, Bourke JP. 107th ENMC international workshop: the man-
agement of cardiac involvement in muscular dystrophy and myotonic dystrophy.
7th-9th June 2002, Naarden, The Netherlands. Neuromuscul Disord 2003;13(2):
16672.
71. Cardiovascular health supervision for individuals affected by Duchenne or
Becker muscular dystrophy. Pediatrics 2005;116(6):156973.
Chronic Respiratory Failure 273
Domi ci l i ary Oxygen
for Chi l dren
Ian M. Balfour-Lynn, MBBS, MD, FRCP, FRCPCH, FRCS(Ed), DHMSA
The pediatric use of domiciliary oxygen (supplemental oxygen delivered in the home)
has been steadily increasing since its first reported use in children in the 1970s.
1
Like
much pediatric practice, because of a scarcity of good evidence to inform clinicians,
there is a lack of consensus over many issues. Most available evidence relates to
infants discharged home with chronic neonatal lung disease (CNLD), which is easily
the largest patient group receiving domiciliary oxygen. Because this article is part of
a series on evidence-based management, much of it relates to CNLD; however,
other conditions are also covered, remembering the adage lack of evidence of benefit
is not the same as evidence for lack of benefit (Box 1). Nevertheless, whenever pos-
sible, recommendations are accompanied by a grade indicating quality of evidence
and strength of the recommendation using the GRADE system.
2
DEFINITIONS
Although domiciliary refers to the home, in the context of oxygen therapy, it refers to de-
livery of supplemental oxygen outside the hospital because it may also be used outside
the home, especially by children. Modes of delivery fall intothree categories. Long-term
oxygen therapy (LTOT) is definedas the provision of oxygen for continuous use at home
for patients who have chronic hypoxemia (attributable to any cause) to maintain oxygen
saturation (SaO
2
) at or greater than 92% (depending on the type of oximeter) or PaO
2
greater than 8 kPa.
3
It may be required 24 hours per day or during periods of sleep
only; thus, the adult definition that includes a requirement for more than 15 hours per
day is not relevant. Ambulatory oxygen therapy (AOT) refers to the provision of portable
oxygen that can be used outside the home. In adult patients, this is not always neces-
sary because many are house-bound (although they may still need to attend hospital
appointments). All children on LTOT require facilities for portable AOT unless they
only use nighttime oxygen. This particularly applies to the infant age group (who spend
periods during the day sleeping) because parents need to be able to take the baby out-
side the home to lead as normal a life as possible. Short burst oxygen therapy (SBOT)
Department of Paediatric Respiratory Medicine, Royal Brompton Hospital, Sydney Street,
London SW3 6NP, UK
E-mail address: i.balfourlynn@ic.ac.uk
KEYWORDS
Oxygen
Domiciliary
Home
Neonatal lung disease
Pediatr Clin N Am 56 (2009) 275296
doi:10.1016/j.pcl.2008.10.010 pediatric.theclinics.com
0031-3955/08/$ see front matter 2009 Elsevier Inc. All rights reserved.
refers to acute use of short-term oxygen, and there are few indications specific to chil-
dren, although it is undoubtedly used that way in many families (eg, during seizures).
NORMAL OXYGEN LEVELS
Painful arterial stabs result in a crying (and sometimes hypoxic) child, which gives
unreliable results; thus, studies of oxygen levels in children are invariably performed
using pulse oximetry. The issue here, however, is that pulse oximeters do not all give
equivalent readings of SaO
2
; thus, it is necessary to know which oximeter was used
when comparing studies. A group of investigators have studied children at varying
ages using the same equipment (Table 1). Their study of healthy term infants in
the first month of life measured by pulse oximetry found in the first week of life
that the baseline SaO
2
ranged from 92% to 100% (median of 97.6%), whereas in
weeks 2 through 4, it ranged from 87% to 100% (median of 98.0%).
4
Episodes of
desaturation (SaO
2
%80% for R4 seconds) occurred in 35% of recordings in
week 1 and in 60% in weeks 2 through 4. These investigators also studied 67 older
healthy full-term infants aged 4 to 8 weeks and found that their baseline SaO
2
, mea-
sured by pulse oximetry, ranged from 97% to 100% (median of 99.8%).
5
Short
Box1
Principal pediatric conditions that may require long-term oxygen therapy
CNLD (bronchopulmonary dysplasia)
Other neonatal lung conditions (eg, pulmonary hypoplasia)
Congenital heart disease with pulmonary hypertension
Pulmonary hypertension secondary to pulmonary disease
Interstitial lung disease
Obliterative bronchiolitis
Cystic fibrosis and non-cystic fibrosis bronchiectasis
Obstructive sleep apnea syndrome and other sleep-related disorders
Neuromuscular conditions requiring noninvasive ventilation
Disorders of the chest wall (eg, thoracic dystrophy, severe kyphoscoliosis)
Sickle cell disease
End-of-life palliative care
Table1
Normal oxygen saturation levels in healthy children, measured by the same group of investigators
using pulse oximetry
Age n Median Range Reference
Ex-preterm babies at term 66 99.4 89100 6
1 week 50 97.6 92100 4
24 weeks 50 98.0 87100 4
48 weeks 67 99.8 97100 5
216 (mean 8) years 70 99.5 96100 8
Balfour-Lynn 276
episodes of desaturation to 80% or less were found in 81% of infants, occurring at
a median of 0.9 per hour, with a median duration of 1.2 seconds (97% were for less
than 4 seconds). They studied 66 preterm infants born at a gestational age of 25 to
36 weeks (median of 34 weeks) when they had reached term.
6
Their baseline SaO
2
ranged from 89% to 100% (median of 99.4%). Desaturations were more frequent
(median of 5.4 per hour) and longer (median of 1.5 seconds) than in the term infants,
however.
5
High altitude affects SaO
2
and may need to be taken into account when
interpreting normal values (and publications).
7
Finally, they studied 70 healthy older
children with a mean age of 8 years (range: 216 years) using a pulse oximeter.
8
Baseline SaO
2
was a median of 99.5% (range: 95.8%100%, fifth centile
5 96.6%). The number of desaturations of 90% or less decreased with age, with
episodic decreases seen in 47% of 2- to 6-year-olds and in 13% of 13- to 16-
year-olds. A more recent study in 100 third-grade primary school children (mean
age 5 9.3 years) recorded overnight SaO
2
measured by pulse oximetry.
9
The me-
dian SaO
2
was 97% (range: 94%100%), and a baseline SaO
2
less than 97%
was uncommon. Furthermore, although intermittent desaturations by 4% or more
were frequent, the SaO
2
rarely decreased to 90% or less.
WHATARE THE ADVERSE EFFECTS OF CHRONIC LOWOXYGEN SATURATION?
This, of course, depends on the degree and duration of the low SaO
2
levels, and it is
likely that mild hypoxemia has no adverse effects. Newborns and infants younger than
1 year of age, however, have an increased tendency to ventilation-perfusion mis-
match, making them particularly susceptible to hypoxemic episodes, especially if
they are ill or in the presence of airway hypoxia.
7
There are several factors that con-
tribute to this greater risk for developing hypoxemia: the presence of fetal hemoglobin
(with the oxygen dissociation curve shifted to the left), tendency to pulmonary vaso-
constriction in the presence of airway hypoxia, tendency to bronchoconstriction in
the presence of airway hypoxia, relatively fewer alveoli, compliant rib cage, and small-
er airway diameter.
7
In addition, in the first 2 months of life, infants may show a para-
doxical inhibition of the respiratory drive causing apnea or hypoventilation in response
to hypoxia or infection.
7
Some of the more recognized adverse effects are outlined in
this article.
Pulmonary Arterial Hypertension
Chronic alveolar hypoxia leads to an increase in systolic pulmonary artery pressure
resulting from pulmonary vasoconstriction and increased pulmonary vascular resis-
tance. There is adaptation of the pulmonary endothelium with pulmonary artery re-
modeling.
10
This can lead to right ventricular hypertrophy and dysfunction, and
eventually to right heart failure.
Acute Life-Threatening Events and Sudden Infant Death
It is known that hypoxia can cause apnea and hypoventilation; thus, the greatest con-
cern is that a period of hypoxia may lead to an acute life-threatening event or actual
sudden infant death (SID).
Neurodevelopmental Problems
Intermittent oxygen desaturations are associated with significant learning difficulties in
animal studies.
11
Chronic or intermittent hypoxia has been shown to affect cognitive
and behavioral outcomes adversely, particularly in some children with congenital
cyanotic heart disease and sleep-disordered breathing.
12
Domiciliary Oxygen for Children 277
Suboptimal growth
In infants with chronic hypoxemia, this is best demonstrated by the fact that
growth velocities improve when the babies are given supplemental oxygen.
This may relate to the effects of hypoxemia on nutrient absorption from the
gastrointestinal tract
13
or may be attributable to changes in growth hormone
secretion.
14
Increased airway resistance
This may result from hypoxia in infants with CNLD, a finding that was not seen in
healthy infants.
15
Increased airway inflammation
This can result from hypoxia attributable to up-regulated cytokine expression
and neutrophil inflammation in CF.
16
WHATARE THE ADVERSE EFFECTS OF CHRONIC HIGH OXYGEN SATURATION?
Theeffect of toomuchoxygenonthedevelopingretina is well established, althoughless
relevant at the stage at which the baby is being considered for hospital discharge. Ox-
ygen toxicity, particularly in premature infants, can inhibit lung healing and contribute to
ongoing lung injury through the formation of reactive oxygen intermediates and perox-
idation of membrane lipids.
17
The Benefits of Oxygen Saturation Targeting (BOOST)
study showed a nonsignificant excess) of deaths from pulmonary causes in the babies
kept at a higher SaO
2
.
18
The Supplemental Therapeutic Oxygen for Prethreshold Reti-
nopathy of Prematurity (STOP-ROP) study found an increased rate of adverse pulmo-
nary sequelae (pneumonia and exacerbations of CNLD), although not deaths, in the
high-saturation group; this group also had more infants still requiring supplemental ox-
ygen at 3 months.
19
Oxidative stress from a high oxygen concentration may also be
a contributing factor to the development of bronchopulmonary dysplasia (BPD),
20
and
it is suggested that a fraction of inspired oxygen (FIO
2
) of 0.8 to 1.0 for 24 hours is asso-
ciated (but not necessarily causative) with the occurrence of BPD.
1
In addition, animal
work has shown a possible permanent blunting of the ventilatory response to hypoxia
after exposure to high oxygen concentrations during a critical developmental period.
11
This could lead to an increase in sleep-disordered breathing and even sudden death.
WHAT IS THE EVIDENCE THAT SUPPLEMENTAL OXYGEN IS BENEFICIALTO PATIENTS
AND THAT DOMICILIARYOXYGEN IS PREFERABLE TOHOSPITAL BASED OXYGEN?
These questions are answered for a variety of conditions outlined in this article,
accepting that evidence is often lacking. Benefit is considered in terms of symptoms
(eg, breathlessness, respiratory distress, exercise tolerance), growth and neurodevel-
opment, school attendance and hospitalization rates, quality of life, psychologic im-
pact, and survival. Obviously, these parameters are not applicable to all patient groups.
This section deals with the issues of LTOT and AOT because almost all children
receiving LTOT should not be confined to their home; thus, equipment for AOT
must be provided (unless LTOT is used at nighttime only). The indications for LTOT
are therefore identical to those for AOT.
Chronic Neonatal Lung Disease
The definitions of CNLD and BPD keep evolving. CNLD is said to be present in babies
born before term who require continuous oxygen at 36 weeks of gestational age, or if
they are born at greater than 32 weeks of gestational age, they still require supplemen-
tal oxygen at 28 days of age. BPD is defined as the need for supplemental oxygen for
at least 28 days after birth, and it is graded according to the oxygen flow rate required
Balfour-Lynn 278
near to term.
21
CNLD is the main indication for LTOT in children; data from the Child-
rens Home Oxygen Record database for England and Wales indicate that CNLDis the
underlying cause in 57%of cases. Data fromsurviving babies (born between 1997 and
2002) weighing less than 1500 g showed that 22% developed BPD.
22
They often
require a prolonged period of mechanical ventilation and continued to need supple-
mental oxygen once extubated. With increased survival of extremely low birth weight
premature infants, the incidence of CNLD is also likely to increase,
23
as is the need for
LTOT.
There have been no controlled studies on the effects of mild hypoxemia on mortality
in infants who have CNLD. It has been suggested that the use of supplementary oxy-
gen may reduce mortality from SID, however.
24
This may be because oxygen therapy
reduces the number of apneic and cyanotic episodes, in addition to the frequency of
intermittent desaturations.
24
Certainly, supplemental oxygen significantly reduces pul-
monary arterial hypertension in infants who have CNLD, and this effect is achieved at
an oxygen concentration that is deliverable at home (23 L/min by nasal cannulae).
25
Measurement of infant lung function has shown that supplemental oxygen reduced
total pulmonary resistance and increased compliance in babies who had severe
BPD and reversible obstructive lung disease.
26
The effect of oxygen on sleep quality
is difficult to interpret, but it seems that although desaturations are reduced, this is at
the cost of sleep disruption.
2729
Home oxygen has been shown to improve growth to the level of healthy term
infants, and premature discontinuation of the supplementation (against medical ad-
vice) caused a significant deceleration in weight gain.
3032
The effect of supplemental
oxygen on neurodevelopment is difficult to assess, but it is likely to be beneficial.
33
Further, it reduces the risk for nosocomial infection and it is believed to be good for
parent-child bonding.
33
Although there have been no randomized trials of babies on
LTOT, it is suggested that caring for babies on supplementary oxygen at home is pref-
erable to a prolonged hospital stay.
34
Finally, it is beneficial in terms of freed resources
for neonatal units and reduces the total cost of care for an infant.
3437
Recommendation: Domiciliary LTOT should be considered for infants who have
CNLD and are otherwise ready for hospital discharge. Recommendation B, quality
of evidence: moderate.
Other (Oxygen-Dependent) Neonatal Lung Conditions
Other relevant neonatal lung conditions include pulmonary hypoplasia, congenital
pneumonia, and meconium aspiration syndrome; however, compared with CNLD,
these cases are rare. Survivors of congenital diaphragmatic hernia repair not uncom-
monly develop chronic lung disease, mainly attributable to pulmonary hypoplasia or
lung damage resulting from mechanical ventilation. Some require domiciliary oxygen,
but this is unusual beyond 2 years of age.
38
Randomized controlled trials have not
been (nor could they be) conducted; hence, the low-level recommendation, Neverthe-
less, it is likely that outcomes from receiving LTOT at home would be no different from
those in babies with CNLD.
Recommendation: Domiciliary LTOT should be considered for infants with other
oxygen-dependent neonatal lung conditions who are otherwise ready for hospital
discharge. Recommendation I, quality of evidence: poor.
Congenital Heart Disease: Acyanotic and Cyanotic
It is likely that only those with pulmonary hypertension (without Eisenmenger syn-
drome) need to be at home on long-termoxygen. In cyanotic congenital heart disease,
oxygen has little effect in raising SaO
2
and is not indicated, although the degree of
Domiciliary Oxygen for Children 279
polycythemia may be reduced.
39
In some cases with chronic left-to-right shunting,
however, irreversible pulmonary vascular disease can develop and cause right-to-
left shunting (Eisenmenger syndrome). The resulting pulmonary hypertension is not
responsive to oxygen. However, in a small but important controlled study, 100%
oxygen given for a minimum of 12 hours per day for up to 5 years significantly im-
proved survival in children with pulmonary vascular disease too severe to have correc-
tive surgery.
40
This was not the case in a recent 2-year study of adults with advanced
Eisenmenger syndrome, however, in which nocturnal oxygen had no impact on sur-
vival, exercise capacity, or quality of life.
41
Some children with congenital heart dis-
ease who are awaiting corrective surgery (without Eisenmenger syndrome), and
who have raised pulmonary artery pressure that is oxygen responsive, may benefit
fromLTOT, as can some children after surgery.
42
In addition, children with severe right
ventricular failure and resting hypoxemia need long-termoxygen, but are unlikely to be
at home.
39
Decisions in these cases should be made by a specialist pediatric
cardiologist.
Recommendation: Domiciliary LTOT should be considered for children with pulmo-
nary hypertension accompanying Eisenmenger syndrome (if they have symptomatic
relief) and in children who have pulmonary vascular disease too severe for corrective
surgery, who are otherwise ready for hospital discharge. Recommendation B, quality
of evidence: low.
Pulmonary Hypertension (Secondary and Primary)
Pulmonary hypertension resulting from pulmonary disease (secondary) is caused by
chronic hypoxia and considerably worsens the overall prognosis of the underlying dis-
ease.
10
There are several associated pulmonary disorders (reviewed by Roy and Cour-
iel).
43
Acute hypoxia causes smooth muscle contraction in pulmonary arteries, and
chronic hypoxia leads to pulmonary vasoconstriction and endothelial dysfunction.
Children have a more reactive pulmonary circulation in response to hypoxemia than
adults, and oxygen is the most important vasodilator for maintenance of pulmonary
vascular tone.
43
LTOT reverses or at least slows the progress of the hypoxic-induced
changes to the pulmonary vascular bed and can contribute to improved survival.
10
Primary pulmonary hypertension has a poor prognosis in children (median survival
<1 year). Some of the children desaturate during sleep (especially during the early
morning hours) because of mild hypoventilation, which may lead to severe dyspnea,
and the resulting hypoxemia can be eliminated by supplemental oxygen.
39
These chil-
dren also need oxygen available at home for emergency use (eg, when they have viral
upper respiratory tract infections) because some tend to desaturate.
Recommendation: Domiciliary LTOT should be considered for children with pulmo-
nary hypertension who are otherwise ready for hospital discharge. Recommendation
B, quality of evidence: low.
Interstitial Lung Disease
Interstitial lung disease represents a spectrum of rare conditions with a variable but
often poor outlook (eg, chronic pneumonitis of infancy, nonspecific interstitial pneu-
monitis, desquamative interstitial pneumonitis, immunodeficiency) in which oxygen
exchange is impaired. Drug therapy (usually systemic corticosteroids or hydroxychlor-
oquine) is sometimes beneficial. Many of the children are hypoxic and require LTOT.
The European Respiratory Society Task Force on Chronic Interstitial Lung Disease re-
ported that 26% of all children with interstitial lung disease were on long-term oxygen,
including 55% of those younger than 2 years of age.
44
There has been a single unpub-
lished adult study (reported in a Cochrane review) with the finding that domiciliary
Balfour-Lynn 280
oxygen had no effect on mortality after 3 years.
45
A randomized controlled trial of do-
miciliary oxygen can never be conducted; hence, the low level of the evidence-based
recommendation. Nevertheless, in reality, the recommendation is to offer it.
Recommendation: Domiciliary LTOT should be considered for hypoxic children who
have interstitial lung disease and are otherwise ready for hospital discharge. Recom-
mendation I, quality of evidence: poor.
Obliterative Bronchiolitis
Obliterative bronchiolitis leads to severe obstructive lung disease, and although it may
occur after a viral infection (eg, adenovirus), the cause is often unknown. There is no
specific therapy, and, again, the outlook is variable. Many of the children are hypoxic
and require LTOT, although, again, there is no evidence base to back this up. In
a recent large review, there is no mention of oxygen in the section on treatment.
46
In one study of 18 children in Chile who had postadenoviral bronchiolitis obliterans,
28% children required home oxygen but it could be discontinued after 1 year in all
the children.
47
A smaller study from Malaysia of children on home oxygen found
that those with bronchiolitis obliterans required a longer duration, with a median of
28 months (interquartile range: 1466 months).
48
Recommendation: Domiciliary LTOT should be considered for hypoxic children who
have obliterative bronchiolitis and are otherwise ready for hospital discharge. Recom-
mendation I, quality of evidence: poor.
Cystic Fibrosis and Non-Cystic Fibrosis Bronchiectasis
As therapy improves, there are fewer children with cystic fibrosis (CF) who are hypoxic
and require supplemental oxygen, and pulmonary hypertension is uncommon in chil-
dren who have CF. Hypoxemia may be associated with infective chest exacerbations
when ventilation-perfusion mismatch is worsened. It is estimated that 1% to 2% of
children who have CF receive LTOT.
3
There is, however, no clear-cut definition of hyp-
oxia in CF, and little evidence to guide when supplemental oxygen is indicated.
16
Oxygenation problems are not limited to those who have severe disease; a study of
24 children (median age of 9.5 years) showed that 96% of children with normal lung
function or mild to moderate lung disease (defined as forced expiratory volume in
1 second, percentage predicted of 40%60%and 60%80%, respectively) had desa-
turation events during sleep, although they would not be classified as having nocturnal
hypoxia (SaO
2
<90% for >5% of the time).
49
There was a degree of correlation of noc-
turnal oxygenation with clinical, radiographic, and growth parameters. Although the
proportion of children who had CF and had desaturations was similar to that in a study
of normal children,
9
the children who had CF had a lower mean and minimum SaO
2
and more desaturation events.
There is surprisingly little evidence for the benefit of LTOT in CF, and although it led
to an improvement in school or work attendance, there was no effect on mortality, fre-
quency of hospitalization, or disease progression in a small study (n 5 28).
50
A prob-
lemwith that study was that nocturnal oxygen was titrated to normalize daytime SaO
2
,
which is not necessarily predictive of nocturnal hypoxemia; thus, some of the patients
may have been undertreated. It is not clear how many of the subjects were children,
although all were older than 12 years of age; two of four of the recruiting hospitals
were childrens CF units. It is recommended that LTOT be reserved for those patients
who have CF who obtain symptomatic relief,
51
particularly because adherence to
treatment is usually poor if the child feels no benefit. The potential adverse psycho-
logic effect of starting oxygen at home must be also considered. It is often taken as
an indicator of a serious deterioration in the childs condition and has rightly been
Domiciliary Oxygen for Children 281
described as an emotional life event for a patient who has CF.
52
It is yet another bur-
den of treatment; thus, the patient and family must be motivated and convinced of the
need.
In two small adult studies comparing noninvasive ventilation (NIV) with supplemental
oxygen, it was noted that in those receiving supplemental oxygen alone, the improve-
ment in oxygenation was accompanied by an increase in transcutaneous carbon di-
oxide (CO
2
), which caused morning headaches in a few patients.
53,54
Studies have
not been performed in children, but there is no reason to suggest that this would be
different in adolescents having severe lung disease, who are the ones likely to be re-
ceiving home oxygen. It is therefore recommended that monitoring of transcutaneous
CO
2
levels be performed when oxygen therapy is initiated.
A Cochrane systematic review has summarized the effects of supplemental oxygen
on exercise from three studies (which included a few children only); there was an im-
provement in exercise duration and peak performance.
55
In reality, use of supplemen-
tal oxygen for exercise would not be an indication for domiciliary oxygen in children.
There are other causes of bronchiectasis in children (although in approximately
50% cases, no underlying cause is found), and LTOT is occasionally necessary for
those with severe disease.
Recommendation: Domiciliary LTOT should be considered for hypoxic children who
have CF as a means to improve school attendance and for those who obtain symp-
tomatic relief. Monitoring of transcutaneous CO
2
levels should be performed when
oxygen therapy is initiated. Recommendation B, quality of evidence: low.
Obstructive Sleep Apnea Syndrome
In cases in which the obstruction can be relieved, any pulmonary hypertension that
may have developed is usually reversible and resolves rapidly.
43
Obstructive sleep ap-
nea syndrome may require NIV if the obstruction cannot be relieved. Occasionally,
supplemental oxygen alone is used if the child does not tolerate face mask ventilation
(eg, some children with Downs syndrome). As a temporary treatment, it seems to be
safe and has a beneficial effect on oxygenation and sleep quality.
56
Oxygen does not
suppress the ventilatory drive in most children who have obstructive sleep apnea
syndrome, but PaCO
2
levels should still be monitored.
57
Recommendation: Domiciliary LTOT can be considered for children who have
obstructive sleep apnea syndrome and do not tolerate NIV as long as PaCO
2
levels
are monitored. Recommendation B, quality of evidence: low.
Chronic Hypoventilation: Central, Neuromuscular Weakness, Chest Wall Disorders
There are some patients who require long-term NIV because of chronic hypoventila-
tion (to control hypercapnia and hypoxemia). Oxygen alone is inadequate for most
children with chronic hypoventilation. A UK survey in 1997 estimated the number of
children receiving NIV to be 141, of whom 93 (65%) were at home.
58
The incidence
was shown to have increased over the previous decade, and this figure is likely to con-
tinue to increase in the future. The children had a variety of conditions, principally neu-
romuscular disorders (46%), congenital central hypoventilation syndrome (13%),
spinal injury (12%), craniofacial syndromes (7%), and BPD (4%). There was a variety
of other less frequent causes (18%). In 35% of cases, they had access to supplemen-
tal oxygen at home as well (E. Jardine, personal communication, 2004). It is likely that
these children have other problems affecting the lungs (eg, recurrent infection attribut-
able to aspiration fromswallowing difficulties and gastroesophageal reflux) that lead to
the oxygen requirement. In one UK series of children with neuromuscular and skeletal
disease requiring NIV, 5 of 40 children required supplemental oxygen at night (to
Balfour-Lynn 282
maintain SaO
2
>90%), and 2 of the children stopped the oxygen after 6 months of
NIV.
59
Core guidelines have suggested that children on home ventilation should
have a stable oxygen requirement with an FIO
2
requirement of less than 40%.
60
Recommendation: Domiciliary LTOT can be considered for children with chronic
hypoventilation who remain hypoxic despite NIV with optimal CO
2
control. Recom-
mendation I, quality of evidence: low.
Sickle Cell Disease
It is important that children who have sickle cell disease and upper airway obstruction
do not become hypoxemic during sleep because it can lead to debilitating episodes of
sickling.
61
Low overnight SaO
2
has been linked to cerebrovascular disease and fre-
quent episodes of acute pain.
62
In addition, in a recent study of 75 children aged older
than 6 years, the prevalence of elevated pulmonary artery pressure was 30%, which
was similar to that in adults.
63
This was significantly associated with a low SaO
2
docu-
mented in the clinic. Because pulmonary hypertension confers a high risk for death in
sickle cell disease (at least in adults),
64
it is obvious that chronic hypoxemia must be
prevented. For this reason, domiciliary oxygen should be provided for children with
persistent nocturnal hypoxia after other causes (eg, adenotonsillar hypertrophy)
have been treated. It is recommended in the UK guideline for sickle cell disease in
childhood that overnight SaO
2
should be measured if there is a history of snoring,
or nocturnal enuresis after the age of 6 years.
62
The UK guideline also recommends
an annual measurement of SaO
2
when the child is well and is in outpatient treatment;
if it is less than 95%, overnight monitoring should be undertaken.
62
Furthermore, home
oxygen is suggested as one of the therapies for chronic sickle lung, although the UK
guideline gives no evidence to back up this recommendation.
Recommendation: Domiciliary LTOT should be considered for children who have
sickle cell disease and nocturnal hypoxia. Recommendation I, quality of evidence: low.
Palliative Care and End-of-Life Care
There are no data on the management of terminal dyspnea in patients who have neu-
romuscular disorders and CF.
65
Most published data are on adult patients who have
terminal cancer; a double-blind crossover trial in 14 adults showed that oxygen at
a rate of 5 L/min delivered by mask improved the subjective sensation of dyspnea.
66
A recent meta-analysis, however, found that oxygen did not provide symptomatic
benefit for patients who had cancer with refractory dyspnea and were mildly or
nonhypoxemic.
67
It has been suggested that supplemental oxygen may be effective
in relieving dyspnea in children who cannot tolerate NIV (especially when they are
not hypercapnic).
68
With chronic hypercapnia, the hypercarbic drive to breathe may
be blunted, and in these circumstances, when the primary drive to breathe is hypox-
emia, this may be removed by supplemental oxygen. Although this may lead to hypo-
pnea or even apnea, this is less of a concern in an end-of-life situation.
68
It may also be
important for the family to have a full view of their childs face; thus, nasal cannulae
may be preferable to a NIV face mask.
68
Clinical experience shows that some children
do get a degree of symptomatic relief from supplemental oxygen, although, of course,
it does not affect the final outcome. In addition, reversing hypoxemia can cause pul-
monary vasodilation and prevent the intracranial vasodilation that can be a cause of
headaches.
68
For these reasons, oxygen can be offered, but children are likely to
continue with it only if they find it helpful.
Recommendation: Domiciliary LTOT can be considered for children undergoing
palliative care who obtain symptomatic relief from supplemental oxygen. Recommen-
dation I, quality of evidence: low.
Domiciliary Oxygen for Children 283
INDICATIONS FOR ACUTE USE OF DOMICILIARYOXYGEN
Neurodisability: Recurrent Seizures
It is apparent that some children with seizures are receiving home oxygen, which is
administered at the time of the seizure. There has been a study of respiratory function
observed during 101 seizures in 37 children.
69
An increase in respiratory rate was
noted in 66% of the 21 generalized seizures, but this was not associated with apnea
or hypoxemia (measured by pulse oximetry). No respiratory abnormalities were seen
during the 40 absence seizures. Nevertheless, the 40 focal seizures were often asso-
ciated with respiratory abnormalities, 70%by frequent respiratory pauses and 30%by
apnea, and significant hypoxemia (defined as SaO
2
<85%) was observed in 40% of
seizures. Supplemental oxygen is unlikely to be beneficial because the brief period
of hypoxia does not respond to oxygen while the child is not breathing, and the hyp-
oxia is self-limited and brief anyway. The UK guideline referred to on the National In-
stitute for Clinical Excellence Web site does, however, suggest that oxygen be
administered to patients in the hospital having generalized tonic-clonic status
epilepticus.
70
Recommendation: domiciliary acute oxygen therapy is not recommended for chil-
dren with neurodisability who have recurrent seizures. Recommendation I, quality of
evidence: low.
Acute Asthma
Any child with an acute asthma episode severe enough to require oxygen should be in
the hospital and not at home. There are, however, a few children who have such se-
vere asthma that they need supplemental oxygen while waiting for an ambulance to
take themto the hospital; thus, it must be available at home. In addition, these severely
asthmatic children may need an oxygen supply to drive their nebulizer while waiting for
the ambulance. Generally, spacer devices are preferred for administering bronchodi-
lators,
71
but there are occasions when the child is only able to use a nebulizer. Home
nebulizers are usually driven by roomair, but nebulized salbutamol can cause an initial
decrease in SaO
2
in asthmatic children and wheezy infants, more commonly with air-
than with oxygen-driven nebulization.
72,73
This may be clinically significant if the child
is already hypoxemic and on the steep part of the oxygen dissociation curve from the
acute bronchoconstriction. For those children with recurrent severe life-threatening
episodes, it is better to have oxygen available in the home for use with their nebulizer
before transfer to the hospital.
Recommendation: domiciliary acute oxygen therapy is recommended for children
with recurrent episodes of severe acute asthma as a temporary therapy before ambu-
lance transfer to the hospital. Recommendation B, quality of evidence: moderate.
Acute Bronchiolitis
The need for supplemental oxygen in an infant with acute bronchiolitis has generally
been regarded as an indication for hospital admission. The recommendation in the
Scottish Intercollegiate Guideline Network (SIGN) guideline is that infants with an
SaO
2
of 92% or less require inpatient care, and they can be considered for discharge
when their SaO
2
is greater than 94%.
74
Nevertheless, there has since been a random-
ized trial of 92 infants aged 2 to 24 months presenting with acute bronchiolitis and hyp-
oxia, defined as an SaO
2
of 87% or less.
75
After an 8-hour observation period, 70% of
those randomized for discharge with home oxygen could be discharged (some no lon-
ger required oxygen, and some failed to meet the discharge criteria). Of those sent
home, 97% were treated successfully with oxygen at a rate of 1 L/min by means of
Balfour-Lynn 284
nasal cannulae as outpatients; 1 infant, however, had to be admitted after a cyanotic
spell that occurred after 24 hours at home. This certainly opens up a potential alterna-
tive to hospital admission, but if financial considerations were excluded, the authors
suspicion is that most parents would opt for a short hospital stay. It must also be re-
membered that these patients presumably had the US definition of bronchiolitis (it is
not defined in the paper) and that some of them would have been diagnosed outside
the United States as having acute viral wheeze or infantile asthma.
Recommendation: domiciliary acute oxygen therapy can be considered for children
who have acute bronchiolitis after a period of hospital observation. Recommendation
B, quality of evidence: moderate.
ASSESSMENT OF INITIATION OF LONG-TERM OXYGEN THERAPY (WHEN TOSTART)
The following sections on assessment and follow-up are mainly concerned with in-
fants who have CNLD. This is the largest patient group and is distinguished by having
a good prognosis; there are fewother patients who can be weaned off the oxygen over
time.
Assessment in Infancy
Suitability for domiciliary oxygen therapy should be assessed by a specialist with ap-
propriate experience in the care of the relevant condition; this is usually a respiratory
pediatrician or neonatologist (but may be a pediatric cardiologist, general pediatrician,
or palliative care specialist). The family must also be assessed as competent to man-
age home oxygen therapy and be able to cope with all aspects of the babys care. In
adults, measurement of arterial PaO
2
is considered critical, but this is neither possible
nor practical in infants. In pediatric practice, SaO
2
measured by pulse oximetry re-
mains the main formof assessment, because an arterial stab in a crying (hypoxic) child
is unreliable, whereas capillary PaO
2
does not correlate well with arterial PaO
2
.
76
Sin-
gle measurements are insufficient, and before discharge, SaO
2
must be measured
continuously for at least 6 to 12 hours, including periods of sleep, wakefulness, and
activity or feeding (watching for the effects of movement artifact). It is important to in-
clude all levels of activity because infants have an increased oxygen requirement when
active and infants who have CNLD may develop feeding-related hypoxemia.
77
In ad-
dition, some children may only be hypoxemic at night, without daytime hypoxemia. An
instrument should be used that has been validated in infants, and although it has been
suggested that pulse oximeter readings should be verified by an arterial gas measure-
ment at the start of the study, this is impractical and is not essential. It is important to
remember that correlation between SaO
2
and arterial PaO
2
is such that at 94% satu-
ration, the PaO
2
may vary from 9 to 17 kPa.
78
Although correlation is particularly poor
in the saturation range of 85%to 90%,
79
this should not matter because all infants with
SaO
2
less than 90% should receive LTOT anyway.
Most of the work in infancy relates to CNLD, and there is only limited evidence to
recommend a minimally acceptable level of oxygenation; hence, the lack of consen-
sus on who requires home oxygen.
80
Normal SaO
2
is around 96%, and supplemental
oxygen is usually considered for infants who cannot maintain SaO
2
at 93% or greater
when asleep or quietly awake; oxygen therapy is then given to achieve SaO
2
greater
than 92%.
3
Previously, some researchers have recommended keeping SaO
2
at 95%
or greater,
24
but there is a trend toward lower levels now. This resulted from concerns
over oxygen lung toxicity after two important trials. The first was the BOOST trial of 358
premature infants who still required oxygen at 32 weeks of postmenstrual age.
18
This
showed that maintaining SaO
2
at 95% to 98% had no advantage over 91% to 94% in
Domiciliary Oxygen for Children 285
terms of growth and neurodevelopment at 1 year of age (using oximeters). The study
also found that the group with the higher target oxygen level had an excess of deaths
from pulmonary causes, albeit not statistically significant. This was in keeping with the
second study, the STOP-ROP trial on retinopathy of prematurity.
19
Here, 649 preterm
infants were randomly assigned to different target oxygen levels (89%94% vs. 96%
99%) for at least 2 weeks, using oximeters that are calibrated to display SaO
2
that is
1.6%saturation points lower than other commercial oximeters. The study found an in-
creased rate of adverse pulmonary sequelae (pneumonia and exacerbations of
CNLD), although not deaths, in the high-saturation group when assessed at 3 months
after the due date of the infant (13.2% versus 8.5%). The high-saturation group also
had more infants still requiring supplemental oxygen at 3 months (47% versus
37%). Further studies are underway using lower target saturations (85%89%), and
results of these trials are to be combined in a meta-analysis.
81
It must be remembered
that the correct target saturation for a preterm baby who has not yet reached term is
likely to differ from that of an infant who is old enough to be at home, albeit with
supplemental oxygen.
Recommendation: Oxygen therapy should aim to keep SaO
2
at 92% to 94% in in-
fants, particularly during the preterm period, with no more than 5% of time spent at
lower than 90% saturation. Assessment of SaO
2
must be for at least 6 to 12 hours
and include periods of sleep, wakefulness, and activity or feeding. Recommendation
B, quality of evidence: moderate.
Assessment in Older Children
For older children, adult criteria for oxygen prescription may be acceptable, although
specific studies on upper and lower limits of PaO
2
for LTOT are lacking. It is important
to include an entire night (with at least 4 hours of uninterrupted sleep) in case the child
only develops nocturnal hypoxemia, such as in CF, in which nocturnal hypoxemia usu-
ally precedes daytime desaturation. In children with hypoventilation, such as in neuro-
muscular disease, it is important to check the CO
2
status because in the presence of
hypercapnia, NIV is necessary rather than LTOT alone. Measurement of overnight
transcutaneous or end-tidal CO
2
is ideal, although capillary CO
2
taken just as the child
wakes up may be useful if either of the former is not available. Full polysomnography is
not usually required.
DISCHARGE CRITERIA
A multidisciplinary meeting should ensure that discharge planning is achieved prop-
erly because extensive collaboration is required between the parents and multidisci-
plinary team. The goal is to select the infants and families most likely to cope at
home and to get the timing of discharge right.
82
Each neonatal unit has its own criteria,
but some general principles follow:
3
The oxygen requirement must be stable with mean SaO
2
of 93% or greater, with-
out frequent episodes of desaturation. SaO
2
should not drop lower than 90% for
more than 5% of the artifact-free recording period.
No other clinical conditions should preclude discharge, and the child must be
medically stable with satisfactory growth. There should be no apneic episodes
for at least 2 weeks.
Immunizations should be up to date. Palivizumab may be considered at the
appropriate time of year for infants who have CNLD requiring home oxygen.
Parents are willing and believed to be capable of taking the baby home while still
on oxygen.
Balfour-Lynn 286
Home conditions must be satisfactory, and, preferably, a landline telephone is in-
stalled (in addition to a mobile phone). A visit from a member of the home care
team is required before discharge.
Parents are trained and have written information on the use of home oxygen and
also cardiopulmonary resuscitation in the case of infants. Vigilance for an empty
oxygen supply, dislodged cannulae, or blocked valve is critical. A structured
education program can be useful.
83
Advice is given about no smoking in the home. It needs to be strongly discour-
aged, but help to do so must be offered. In a study of burns affecting 27 adults
on home oxygen, 89% were smoking at the time; thus, parents must be aware of
the danger.
84
Advice must also be given about open flames (eg, birthday cake
candles).
85
Notification to local fire services is recommended.
Older children also need to have training on how to use their oxygen equipment.
Parents must be advised about travel with cylinders and inform their home and
car insurers.
Appropriate support must be in place (eg, community nursing, nurse specialists,
health visitor, social worker).
Communication with a general practitioner has taken place, and roles are
clarified for delivering clinical care.
Parents must have a list of telephone numbers for advice and emergency help,
including a telephone number for repair of equipment breakdown.
Arrangements are in place for open access to the local pediatric unit.
Recommendation: Children can be discharged fromthe neonatal unit when their ox-
ygen requirement is stable with a mean SaO
2
of 93% or greater and without frequent
episodes of desaturation. The SaO
2
should not drop to lower than 90% for more than
5% of the artifact-free recording period. There should be no other clinical conditions
precluding discharge, and the child must be medically stable with satisfactory growth.
Recommendation B, quality of evidence: low.
FOLLOW-UP OF INFANTS ON DOMICILIARYOXYGEN
Arrangements for follow-up after discharge should be coordinated by the hospital
specialist who has initiated domiciliary oxygen. Liaison must take place between
the specialist, local or community pediatrician, general practitioner, nurse specialists,
community pediatric nursing service, occupational therapist, and health visitor. The
oxygen requirement is likely to change over time; it should be reduced in infants
with CNLD but is likely to increase in most other conditions. Regular home monitoring
with pulse oximetry is necessary and should be set up by community or specialist
nurses. A visit within the first 24 hours is important to reassure parents. The first formal
SaO
2
monitoring should take place within a week; subsequent recordings should oc-
cur as clinically indicated but rarely less often than every 3 to 4 weeks.
86
Recorded
data can then be discussed with the supervising consultant, although protocols can
be in place for experienced nursing teams to initiate changes.
These infants require a lot of input from health care professionals. Emotional sup-
port is necessary because parents display marked pre- and postdischarge anxiety,
which decreases as they see their babys oxygen dependency resolving.
87
Mothers
have also been reported to show low self-esteem, self-blame, and elements of grief
and isolation
88
in addition to less vitality and more mental health problems.
89
A study
in Oxford, United Kingdom, on 55 babies with CNLD at home with LTOT looked at
health care use in 31 of the babies.
34
It was found that these families received a median
Domiciliary Oxygen for Children 287
of 43 visits per baby (range: 8173 visits) from a pediatric community nurse and that
these lasted a median of 45 minutes; 83% of families saw a health visitor, with a me-
dian of 12 visits (range: 282 visits), and the visits were for a median of 30 minutes;
83% of families saw a general practitioner, with a median of 6 visits (range: 1140
visits), and the visits were for a median of 10 minutes. A lesser proportion of families
also saw a hospital consultant (they almost all had hospital clinic visits, however, on
a median of four occasions), social worker, physiotherapist, and speech therapist.
In addition, infants with CNLD who require home oxygen have more frequent and
longer hospital admissions, and more clinic attendances, than those sent home with-
out oxygen; this means that their total cost of care was 40% greater.
90
This is partic-
ularly the case if they had been hospitalized in the first 2 years of life with respiratory
syncytial virus infection, which had a significant impact on the cost of care.
91
In the
Oxford study, 41% of the babies required readmission, on a median of 1 occasion
(range: 010 occasions), staying for a median 9 days (range: 164 days).
34
The children should be seen regularly by the hospital specialist in the clinic to mon-
itor the underlying condition in addition to growth and neurodevelopment. There must
be direct access for the child to be admitted to the hospital in the case of any emer-
gency or acute deterioration in his or her condition, and the parents must have the tele-
phone numbers of the team. Even a simple viral upper respiratory tract infection in
a young infant on LTOT may necessitate admission, and winter (particularly the first)
can be an anxious time for parents. If the caregivers believe the child requires an
increase in oxygen, they can turn up the flow rate but must then seek advice from
the home care team. Even when the child comes off oxygen, support must continue
because the children may sometimes relapse and require further periods of oxygen
therapy after an apparently complete recovery. This is usually related to intercurrent
infection.
Recommendation: Regular home monitoring with pulse oximetry is necessary. After
an initial visit within the first 24 hours, the first formal SaO
2
monitoring should take
place within 1 week; subsequent recordings are done as clinically indicated but usu-
ally not less often than every 3 to 4 weeks. Recommendation B, quality of evidence:
low.
WEANING INFANTS OFF LONG-TERMOXYGEN THERAPY (WHEN TOSTOP)
The issue of weaning off oxygen principally applies to infants with CNLD and some
other neonatal lung conditions. In children with congenital heart disease, only those
having successful corrective surgery or transplantation no longer require LTOT.
Some young children with interstitial lung disease or obliterative bronchiolitis may im-
prove sufficiently to lose their oxygen dependency. The older children with progressive
lung disease, such as CF or neuromuscular conditions, usually continue to require ox-
ygen for the remainder of their lives. It is not easy to counsel the parents of children
who have CNLD as to how long LTOT is needed. Although group data showed that
capillary blood PaCO
2
measured near term correlates with length of oxygen depen-
dency in CNLD, oxygen dependency is impossible to predict for an individual.
92
In
general, however, those with a higher PaCO
2
are more likely to require oxygen for lon-
ger. The length of time that infants with CNLD remain on LTOT varies, but it is usually
less than 12 months, although some require it for several years.
35,93,94
Persisting
symptoms or failure to progress warrants review to rule out such conditions as trache-
obronchomalacia, large airway stenosis or granuloma formation, gastroesophageal
reflux, recurrent aspiration, or unsuspected congenital cardiac disease.
Balfour-Lynn 288
There is enormous variety of practice with regard to criteria used by pediatricians
about when to discontinue LTOT in children with CNLD, which reflects a lack of
evidence on which to base guidelines.
95
During periods of weaning or withdrawal of
oxygen, more frequent monitoring is needed. It is not normally necessary for the child
to have a SaO
2
monitor kept in the home because one can be provided for intermittent
monitoring. Recording should include monitoring during daytime activity, feeding, and
sleep. Short-term awake SaO
2
measurements do not predict prolonged sleeping
SaO
2
.
32
The same target saturations used to decide on initiation of supplementation
are used for weaning purposes (92%94%). Saturation targets in the physiologic
range (95%98%) may be thought to be desirable in infants with pulmonary hyperten-
sion. In a study using 2-hour room air challenges, most infants reached their lowest
saturations within 40 minutes of discontinuing oxygen and a level of 92% or greater
best predicted readiness for weaning judged by 6 months of follow-up.
96
Furthermore,
infants requiring an oxygen flow rate of 0.02 L/min per kilogram of body weight were
most likely to be successfully weaned.
96
Some units wean infants from continuous low-flow oxygen to nighttime and naps
only, whereas others maintain continuous oxygen until the child has no requirement
at all; there is no evidence to recommend which approach is best. When the oxygen
requirement is minimal, the children should have supervised weaning into air with con-
tinuous monitoring (including active periods and sleep). The babies tend to be weaned
down to an oxygen flow rate of 0.1 L/min using a low-flow meter, and from that level,
they can usually be weaned straight to air. Although extremely low (or ultralow) flow
meters exist (range: 0.0250.2 L/min), allowing the flow to be reduced even further
before weaning to air, this is usually unnecessary. There is also concern that some
caregivers may become confused by the decimal points. Weaning is preferably
done at home because this minimizes the chances of nosocomial infection, although
a child may sometimes need a brief hospital admission. It is usually prudent to ensure
that the child has coped with at least one viral upper respiratory tract infection without
problems before the equipment is removed from the home, and it should be left there
for a few months, especially in the winter.
Recommendation: The same target saturations used to decide on initiation of
supplementation should be used for weaning purposes (92%94%). Higher saturation
targets (95%98%) may be used in infants with pulmonary hypertension. Recommen-
dation B, quality of evidence: low.
Infants can be weaned from continuous low-flow oxygen to provision of oxygen
during nighttime and naps only or remain in continuous oxygen on a 24-hour basis until
the child has no requirement at all. Recommendation I, quality of evidence: poor.
EQUIPMENT
Provision of equipment depends on local arrangements and availability, but there are
some general principles.
3
Oxygen concentrators are usually the preferred devices with large back-up
cylinders for breakdown (which must be secured to a wall). They work by filtering
room air and removing the nitrogen to increase the oxygen concentration.
Oxygen concentrators need two outlets, one in the childs bedroom and one in
the main living room area.
Portable cylinders are required for ambulatory use. Although many find
lightweight cylinders easier to handle, the standard-weight cylinders last longer
outside the home.
Domiciliary Oxygen for Children 289
Oxygen cylinders may be more appropriate if initial flow rates are lower than
0.3 L/min and the anticipated duration of oxygen therapy is less than 3 months.
A back-up cylinder must be available for those on continuous oxygen. Particular
attention must be paid to safety and securing of cylinders in the presence of
young children.
Low-flow meter (0.11 L/min) must be available for infants and extremely young
children.
A humidification system is often required for those on flow rates greater than
1 L/min for nasal comfort. Cold bubble humidifiers may be used for this purpose,
but they only achieve 40% relative humidity and are inadequate for direct airway
humidification (eg, by means of a tracheostomy). Heated humidification is less
convenient for domestic use and is only effective at flowrates of 4 L/min or higher
delivered by a concentrator because water can block the tubing at lower flow
rates.
Appropriately sized soft twin-prong nasal cannulae (small children rarely tolerate
>2 L/min by nasal cannulae), a face mask, and nonkinking extension tubing must
be provided. Stomahesive (or equivalent) should also be provided to protect the
skin in those using nasal cannulae.
An oxygen conserver is a device to ensure that oxygen is delivered from the cyl-
inder only during inspiration, which prolongs the cylinder life up to threefold. They
are said to be usable in older children (>8 years of age) but are generally not used
in pediatric practice because of the often irregular and shallowbreathing patterns
of children.
Ambulatory equipment must be available as part of the oxygen delivery systems
unless oxygen is only required at night. This must be lightweight so that older
children can handle it themselves, and for infants, it must fit on to a pram or
push chair. Parents need advice on the type of pram to buy (ie, one with a metal
basket underneath that is safe and strong enough to hold the cylinder).
Children in wheelchairs need to have cylinder fitting provided by their wheelchair
service to maintain safety.
Oxygen Saturation Monitor (Pulse Oximeter)
The issue of whether parents should be provided with their own saturation monitor has
been an area of debate in the United Kingdom. If a child requires continuous monitor-
ing, it is unlikely that he or she is ready for hospital discharge. There is no evidence that
provision of oximeters improves the outcome of babies on home oxygen (or that it
does not); however, in practice, they may lead to excessive adjustments of the flow
rate by the caregivers.
86
They may also give false reassurance, and SaO
2
is only
one aspect of the babys respiratory status. Some parents, however, request one
for spot measurements as a guide to when oxygen needs increasing, during, for exam-
ple, a viral cold. In fact, the baby should be seen in these circumstances, usually by the
home care nurse, who can then make a proper assessment. In addition, the use as an
overnight alarm is often unsatisfactory because of the number of false alarms,
mostly frommovement artifact. Nevertheless, the American Thoracic Society has sup-
ported the provision of oximeters to parents, but their rationale seems to be mostly
cost based in terms of reducing hospital and office visits.
97
OXYGEN OUTSIDE THE HOME
School
There is a small but important demand for oxygen therapy to be available in schools.
Liaison is required between the specialist pediatric respiratory team and education
Balfour-Lynn 290
health services, and this is usually coordinated by community pediatric services. The
following need particular consideration:
Oxygen delivery equipment must be lightweight and easy for the child to handle
and adjust.
Safety devices must be in place for stabilizing oxygen cylinders or other
equipment.
Insurance coverage must be obtained by the school for the staff and premises.
Adequate technical back-up must be available.
School staff must be trained in the use of oxygen therapy.
School staff must have easily identified health care contacts.
Provision must be made for ambulatory oxygen for the journey to and from
school.
Holidays and Airplanes
Arrangements can and should be made for oxygen concentrators and cylinders to be
in place so that families can go away on holiday. Oxygen-dependent children need an
increased flow rate during air flight because of the drop in air pressure, and hence
equivalent FIO
2
to 0.15 at cruising altitude; the issue of preflight testing has been re-
viewed recently.
98
SUMMARY
The use of domiciliary oxygen is significant, with approximately 3500 children receiv-
ing it in England and Wales. The evidence base behind this is poor, although evidence
for its use in CNLD (the most common indication) is reasonable. Lack of evidence
should not mean, however, that it is wrong to prescribe domiciliary oxygen, and com-
mon sense and clinical experience must prevail. Studies are urgently needed because,
currently, we are not even sure of the ideal target SaO
2
.
REFERENCES
1. MacLean JE, Fitzgerald DA. A rational approach to home oxygen use in infants
and children. Paediatr Respir Rev 2006;7:21522.
2. Atkins D, Best D, Briss PA, et al. GRADE Working Group. Grading quality of
evidence and strength of recommendations. BMJ 2004;328:1490.
3. Balfour-Lynn IM, Primhak RA, Shaw BN. Home oxygen for children: who, how and
when? Thorax 2005;60:7681.
4. Poets CF, Stebbens VA, Lang JA, et al. Arterial oxygen saturation in healthy term
neonates. Eur J Pediatr 1996;155:21923.
5. Stebbens VA, Poets CF, Alexander JR, et al. Oxygen saturation and breathing
patterns in infancy. 1: full term infants in the second month of life. Arch Dis Child
1991;66:56973.
6. Poets CF, Stebbens VA, Alexander JR, et al. Oxygen saturation and breathing
patterns in infancy. 2: preterm infants at discharge from special care. Arch Dis
Child 1991;66:5748.
7. Samuels MP. The effects of flight and altitude. Arch Dis Child 2004;89:44855.
8. Poets CF, Stebbens VA, Samuels MP, et al. Oxygen saturation and breathing
patterns in children. Pediatrics 1993;92:68690.
9. Urschitz MS, Wolff J, Von Einem V, et al. Reference values for nocturnal home
pulse oximetry during sleep in primary school children. Chest 2003;123:96101.
Domiciliary Oxygen for Children 291
10. Higenbottam T, Cremona G. Acute and chronic hypoxic pulmonary hypertension.
Eur Respir J 1993;6:120712.
11. Halbower AC, McGrath SA. Home oxygen therapy: the jury is still in session.
J Perinatol 2004;24:5961.
12. Bass JL, Corwin M, Gozal D, et al. The effect of chronic or intermittent hypoxia on
cognition in childhood: a review of the evidence. Pediatr 2004;114:80516.
13. Bernstein D, Bell JG, Kwong L, et al. Alterations in postnatal intestinal function
during chronic hypoxemia. Pediatr Res 1992;31:2348.
14. Fitzgerald D, Van Asperen P, OLeary P, et al. Sleep, respiratory rate, and growth
hormone in chronic neonatal lung disease. Pediatr Pulmonol 1998;26:2419.
15. Teague WG, Pian MS, Heldt GP, et al. An acute reduction in the fraction of
inspired oxygen increases airway constriction in infants with chronic lung dis-
ease. Am Rev Respir Dis 1988;137:8615.
16. Urquhart DS, Montgomery H, Jaff
e A. Assessment of hypoxia in children with cys-
tic fibrosis. Arch Dis Child 2005;90:113843.
17. Weinberger B, Laskin DL, Heck DE, et al. Oxygen toxicity in premature infants.
Toxicol Appl Pharmacol 2002;181:607.
18. Askie LM, Henderson-Smart DJ, Irwig L, et al. Oxygen-saturation targets and
outcomes in extremely preterm infants. N Engl J Med 2003;349:95967.
19. Supplemental Therapeutic Oxygen for Prethreshold Retinopathy of Prematurity
(STOP-ROP), a randomized, controlled trial. I: primary outcomes. Pediatrics
2000;105:295310.
20. Saugstad OD. Chronic lung disease: oxygen dogma revisited. Acta Paediatr
2001;90:1135.
21. Baraldi E, Filippone M. Chronic lung disease after premature birth. N Engl J Med
2007;357:194655.
22. Fanaroff AA, Stoll BJ, Wright LL, et al. NICHD Neonatal Research Network. Trends
in neonatal morbidity and mortality for very low birthweight infants. Am J Obstet
Gynecol 2007;196:147e18.
23. Hack M, Fanaroff AA. Outcomes of children of extremely low birthweight and
gestational age in the 1990s. Semin Neonatol 2000;5:89106.
24. Poets CF. When do infants need additional inspired oxygen? A review of the
current literature. Pediatr Pulmonol 1998;26:4248.
25. Abman SH, Wolfe RR, Accurso FJ, et al. Pulmonary vascular response to oxygen
in infants with severe bronchopulmonary dysplasia. Pediatrics 1985;75:804.
26. Tay-Uyboco JS, Kwiatkowski K, Cates DB, et al. Hypoxic airway constriction in
infants of very low birth weight recovering from moderate to severe bronchopul-
monary dysplasia. J Pediatr 1989;115:4569.
27. Harris MA, Sullivan CE. Sleep pattern and supplementary oxygen requirements in
infants with chronic neonatal lung disease. Lancet 1995;345:8312.
28. Fitzgerald D, Van Asperen P, Leslie G, et al. Higher SaO
2
in chronic neonatal lung
disease: does it improve sleep? Pediatr Pulmonol 1998;26:23540.
29. Simakajornboon N, Beckerman RC, Mack C, et al. Effect of supplemental oxygen
on sleep architecture and cardiorespiratory events in preterm infants. Pediatrics
2002;110:8848.
30. Groothuis JR, Rosenberg AA. Home oxygen promotes weight gain in infants with
bronchopulmonary dysplasia. Am J Dis Child 1987;141:9925.
31. Hudak BB, Allen MC, Hudak ML, et al. Home oxygen therapy for chronic lung
disease in extremely low-birth-weight infants. Am J Dis Child 1989;143:35760.
Balfour-Lynn 292
32. Moyer-Mileur LJ, Nielson DW, Pfeffer KD, et al. Eliminating sleep-associated hyp-
oxemia improves growth in infants with bronchopulmonary dysplasia. Pediatrics
1996;98:77983.
33. Kotecha S, Allen J. Oxygen therapy for infants with chronic lung disease. Arch
Dis Child Fetal Neonatal Ed 2002;87:F114.
34. Hallam L, Rudbeck B, Bradley M. Resource use and costs of caring for oxygen-
dependent children: a comparison of hospital and home-based care. J Neonatal
Nursing 1996;2:2530.
35. Baraldi E, Carra S, Vencato F, et al. Home oxygen therapy in infants with broncho-
pulmonary dysplasia: a prospective study. Eur J Pediatr 1997;156:87882.
36. Spinner SS, Girifalco RB, Gibson E, et al. Earlier discharge of infants from neona-
tal intensive care units: a pilot program of specialized case management and
home care. Delaware Valley Child Health Alliance. Clin Pediatr (Phila) 1998;37:
3537.
37. Greenough A, Alexander J, Burgess S, et al. High versus restricted use of home
oxygen therapy, health care utilisation and the cost of care in chronic lung
disease. Eur J Ped 2004;163:2926.
38. Jaillard SM, Pierrat V, Dubois A, et al. Outcome at 2 years of infants with congen-
ital diaphragmatic hernia: a population-based study. Ann Thorac Surg 2003;75:
2506.
39. Widlitz A, Barst RJ. Pulmonary arterial hypertension in children. Eur Respir J
2003;21:15576.
40. Bowyer JJ, Busst CM, Denison DM, et al. Effect of long term oxygen treatment
at home in children with pulmonary vascular disease. Br Heart J 1986;55:
38590.
41. Sandoval J, Aguirre JS, Pulido T, et al. Nocturnal oxygen therapy in patients with
Eisenmenger syndrome. Am J Crit Care Med 2001;164:16827.
42. Ohashi N, Matsushima M, Maeda M, et al. Advantages of oxygen inhalation ther-
apy for postoperative pulmonary hypertension. Pediatr Cardiol 2005;26:902.
43. Roy R, Couriel JM. Secondary pulmonary hypertension. Paediatr Respir Rev
2006;7:3644.
44. Clement A, Ers Task Force. Task force on chronic interstitial lung disease in immu-
nocompetent children. Eur Respir J 2004;24:68697.
45. Crockett AJ, Cranston JM, Antic N, Domiciliary oxygen for interstitial lung
disease. Cochrane Database Syst Rev 2001;(3):CD002883.
46. Kurland G, Michelson P. Bronchiolitis obliterans in children. Pediatr Pulmonol
2005;39:193208.
47. Castro-Rodriguez JA, Daszenies C, Garcia M, et al. Adenovirus pneumonia in
infants and factors for developing bronchiolitis obliterans: a 5-year follow-up.
Pediatr Pulmonol 2006;41:94753.
48. Norzila MZ, Azizi BH, Norrashidah AW, et al. Home oxygen therapy for children
with chronic lung diseases. Med J Malaysia 2001;56:1517.
49. Uyan ZS, Ozdemir N, Ersu R, et al. Factors that correlate with sleep oxygenation
in children with cystic fibrosis. Pediatr Pulmonol 2007;42:71622.
50. Zinman R, Corey M, Coates AL, et al. Nocturnal home oxygen in the treatment of
hypoxemic cystic fibrosis patients. J Pediatr 1989;114:36877.
51. Schidlow DV, Taussig LM, Knowles MR. Cystic Fibrosis Foundation consensus
conference report on pulmonary complications of cystic fibrosis. Pediatr Pulmo-
nol 1993;15:18798.
Domiciliary Oxygen for Children 293
52. Tiddens HAWM, Devadason SG, et al. Delivery of therapy to the cystic fibrosis
lung. In: Hodson ME, Geddes D, Bush A, et al, editors. Cystic fibrosis. 3rd edition.
London: Hodder Arnold; 2007. p. 18498.
53. Gozal D. Nocturnal ventilatory support in patients with cystic fibrosis: comparison
with supplemental oxygen. Eur Respir J 1997;10:19992003.
54. Young AC, Wilson JW, Kotsimbos TC, et al. Randomised placebo controlled trial
of non-invasive ventilation for hypercapnia in cystic fibrosis. Thorax 2008;63:
727.
55. Mallory GB, Fullmer JJ, Vaughan DJ, Oxygen therapy for cystic fibrosis.
Cochrane Database Syst Rev 2005;(4):CD003884.
56. Aljadeff G, Gozal D, Bailey-Wahl SL, et al. Effects of overnight supplemental ox-
ygen in obstructive sleep apnea in children. Am J Respir Crit Care Med 1996;153:
515.
57. Marcus CL, Carroll JL, Bamford O, et al. Supplemental oxygen during sleep in
children with sleep-disordered breathing. Am J Respir Crit Care Med 1995;152:
1297301.
58. Jardine E, OToole M, Paton JY, et al. Current status of long term ventilation in
children in the United Kingdom: questionnaire survey. BMJ 1999;318:2959.
59. Simonds AK, Ward S, Heather S, et al. Outcome of paediatric domiciliary mask
ventilation in neuromuscular and skeletal disease. Eur Respir J 2000;16:47681.
60. Jardine E, Wallis C. Core guidelines for the discharge home of the child on long
term assisted ventilation in children in the United Kingdom. Thorax 1998;53:
7627.
61. Blaisdell CJ. Sickle cell disease and breathing during sleep. Lung Biol Health Dis
2000;147:75563.
62. NHS Sickle Cell and Thalassaemia Screening Programme in partnership with the
Sickle Cell Society. Sickle cell disease in childhood. Detailed guidance standards
and guidelines for clinical care. Available at: http://www.sickleandthal.org.uk/
Documents/DETAILED_CLIN_Oct19.pdf. Accessed 2008.
63. Pashankar FD, Carbonella J, Bazzy-Asaad A, et al. Prevalence and risk factors of
elevated pulmonary artery pressures in children with sickle cell disease. Pediat-
rics 2008;121:77782.
64. Gladwin MT, Sachdev V, Jison ML, et al. Pulmonary hypertension as a risk factor
for death in patients with sickle cell disease. N Engl J Med 2004;350:88695.
65. Collins JJ, Fitzgerald DA. Palliative care and paediatric respiratory medicine.
Paediatr Respir Rev 2006;7:2817.
66. Bruera E, de Stoutz N, Velasco-Leiva A, et al. Effects of oxygen on dyspnoea in
hypoxaemic terminal-cancer patients. Lancet 1993;342:134.
67. Uronis HE, Currow DC, McCrory DC, et al. Oxygen for relief of dyspnoea in mildly-
or non-hypoxaemic patients with cancer: a systematic review and meta-analysis.
Br J Cancer 2008;98:2949.
68. Ullrich CK, Mayer OH. Assessment and management of fatigue and dyspnea in
pediatric palliative care. Pediatr Clin North Am 2007;54:73556.
69. ORegan ME, Brown JK. Abnormalities in cardiac and respiratory function
observed during seizures in childhood. Dev Med Child Neurol 2005;47:49.
70. Stokes T, Shaw EJ, Juarez-Garcia A, et al. Clinical guidelines and evidence re-
view for the epilepsies: diagnosis and management in adults and children in pri-
mary and secondary care. 2004 London: Royal College of General Practitioners.
Available at: http://www.nice.org.uk/nicemedia/pdf/CG020fullguideline.pdf. Ac-
cessed 2008.
Balfour-Lynn 294
71. Cates CJ, Crilly JA, Rowe BH. Holding chambers (spacers) versus nebulisers for
beta-agonist treatment of acute asthma. Cochrane Database Syst Rev 2006;(2):
CD000052.
72. Gleeson JG, Green S, Price JF. Air or oxygen as driving gas for nebulised
salbutamol. Arch Dis Child 1988;63:9004.
73. Prendiville A, Rose A, Maxwell DL, et al. Hypoxaemia in wheezy infants after
bronchodilator treatment. Arch Dis Child 1987;62:9971000.
74. Scottish Intercollegiate Guidelines Network. Bronchiolitis in children. A national
clinical guideline. 2006. Available at: http://www.sign.ac.uk/pdf/sign91.pdf. Ac-
cessed 2008.
75. Bajaj L, Turner CG, Bothner J. A randomized trial of home oxygen therapy from
the emergency department for acute bronchiolitis. Pediatrics 2006;117:63340.
76. Yildizdasx D, Yapiciog lu H, Yilmaz HL, et al. Correlation of simultaneously obtained
capillary, venous, and arterial blood gases of patients in a paediatric intensive
care unit. Arch Dis Child 2004;89:17680.
77. Singer L, Martin RJ, Hawkins SW, et al. Oxygen desaturation complicates feeding
in infants with bronchopulmonary dysplasia after discharge. Pediatrics 1992;90:
3804.
78. Wasunna A, Whitelaw AG. Pulse oximetry in preterm infants. Arch Dis Child 1987;
62:9578.
79. Roberts CM, Bugler JR, Melchor R, et al. Value of pulse oximetry in screening for
long-term oxygen therapy requirement. Eur Respir J 1993;6:55962.
80. Ellsbury DL, Acarregui MJ, McGuinness GA, et al. Controversy surrounding the
use of home oxygen for premature infants with bronchopulmonary dysplasia.
J Perinatol 2004;24:3640.
81. Higgins RD, Bancalari E, Willinger M, et al. Executive summary of the workshop
on oxygen in neonatal therapies: controversies and opportunities for research.
Pediatrics 2007;119:7906.
82. Gracey K, Talbot D, Lankford R, et al. The changing face of bronchopulmonary
dysplasia: part 2. Discharging an infant home on oxygen. Adv Neonatal Care
2003;3:8898.
83. Laubscher B. Home oxygen therapy: beware of birthday cakes. Arch Dis Child
2003;88:1125.
84. Robb BW, Hungness ES, Hershko DD, et al. Home oxygen therapy: adjunct or
risk factor? J Burn Care Rehabil 2003;24:4036.
85. Brown KA, Sauve RS. Evaluation of a caregiver education program: home oxygen
therapy for infants. J Obstet Gynecol Neonatal Nurs 1994;23:42935.
86. Primhak RA. Discharge and aftercare in chronic lung disease of the newborn.
Semin Neonatol 2003;8:11726.
87. Zanardo V, Freato F. Home oxygen therapy in infants with bronchopulmonary
dysplasia: assessment of parental anxiety. Early Hum Dev 2001;65:3946.
88. Manns SV. Life after the NNU: the long term effects on mothers lives, managing
a child at home with broncho-pulmonary dysplasia and on home oxygen. Neuro
Endocrinol Lett 2004;25(Suppl 1):12732.
89. McLean A, Townsend A, Clark J, et al. Quality of life of mothers and families car-
ing for preterm infants requiring home oxygen therapy: a brief report. J Paediatr
Child Health 2000;36:4404.
90. Greenough A, Alexander J, Burgess S, et al. Home oxygen status and rehospital-
isation and primary care requirements of infants with chronic lung disease. Arch
Dis Child 2002;86:403.
Domiciliary Oxygen for Children 295
91. Greenough A, Alexander J, Burgess S, et al. Health care utilisation of prematurely
born, preschool children related to hospitalisation for RSV infection. Arch Dis
Child 2004;89:6738.
92. Victor S, Shaw B. Carbon dioxide levels do not predict duration of home oxygen
requirement: a retrospective study. J Perinat Med 2002;30:3335.
93. Sauve RS, McMillan DD, Mitchell I, et al. Home oxygen therapy. Outcome of
infants discharged from NICU on continuous treatment. Clin Pediatr 1989;28:
1138.
94. Abman SH, Davis JM, et al. Bronchopulmonary dysplasia. In: Chernick V, Boat TF,
Wilmott RW, et al, editors. Kendigs disorders of the respiratory tract in children.
7th edition. Philadelphia: WB Saunders; 2006. p. 34258.
95. Solis A, Harrison G, Shaw BN. Assessing oxygen requirement after discharge in
chronic lung disease: a survey of current practice. Eur J Pediatr 2002;161:
42830.
96. Simoes EA, Rosenberg AA, King SJ, et al. Room air challenge: prediction for
successful weaning of oxygen-dependent infants. J Perinatol 1997;17:1259.
97. American Thoracic Society. Statement on the care of the child with chronic lung
disease of infancy and childhood. Am J Respir Crit Care Med 2003;168:35696.
98. Bossley C, Balfour-Lynn IM. Taking young children on aeroplanes: what are the
risks? Arch Dis Child 2008;93:52833.
Balfour-Lynn 296
You might also like
- Respiratorynoises: Howusefularethey Clinic Ally?: Craig MellisDocument17 pagesRespiratorynoises: Howusefularethey Clinic Ally?: Craig Mellisskargirl07No ratings yet
- 01 Pediatric Clinics - February2009Document291 pages01 Pediatric Clinics - February2009Tessa CruzNo ratings yet
- Childhood Asthma Research PaperDocument4 pagesChildhood Asthma Research Paperaflbtjglu100% (1)
- Jurnal AsmaDocument11 pagesJurnal AsmaAi Siti Rika FauziahNo ratings yet
- An Update On The Perioperative Management of Children With Upper Respiratory InfectionsDocument18 pagesAn Update On The Perioperative Management of Children With Upper Respiratory InfectionsAditya ManjunathNo ratings yet
- Resp Emer in ChildrenDocument35 pagesResp Emer in ChildrenvgmanjunathNo ratings yet
- Treating The Wheezing Infant: Ronina A. Covar, MD, Joseph D. Spahn, MDDocument24 pagesTreating The Wheezing Infant: Ronina A. Covar, MD, Joseph D. Spahn, MDSophia RoseNo ratings yet
- Research Paper On Childhood AsthmaDocument5 pagesResearch Paper On Childhood Asthmaiakoasulg100% (1)
- Asthma Risk in Children Born After Infertility TreatmentDocument9 pagesAsthma Risk in Children Born After Infertility TreatmentKinjal ShahNo ratings yet
- Vestibular DisorderDocument417 pagesVestibular DisorderDEEKSHA ABROLNo ratings yet
- Hearing Screening Pediatrics 2009Document14 pagesHearing Screening Pediatrics 2009Francisco ValleNo ratings yet
- Ear Discharge in Children Presenting With Acute Otitis MediaDocument5 pagesEar Discharge in Children Presenting With Acute Otitis MediaghostmanzNo ratings yet
- Rds CBL CombinedDocument37 pagesRds CBL CombinedMagdalene ChooNo ratings yet
- Special Issue ARTICLE Less Is More: Evidence-Based Management of BronchiolitisDocument11 pagesSpecial Issue ARTICLE Less Is More: Evidence-Based Management of BronchiolitisyundaNo ratings yet
- JPCC 2380 0534 01 0002 PDFDocument4 pagesJPCC 2380 0534 01 0002 PDFLuiggi D. Chambi MaidaNo ratings yet
- Thorax 2008 Shields Iii1 Iii15Document16 pagesThorax 2008 Shields Iii1 Iii15diapalupiNo ratings yet
- Severity Scoring Systems: Are They Internally Valid, Reliable and Predictive of Oxygen Use in Children With Acute Bronchiolitis?Document7 pagesSeverity Scoring Systems: Are They Internally Valid, Reliable and Predictive of Oxygen Use in Children With Acute Bronchiolitis?Ivan VeriswanNo ratings yet
- Acute Upper Airway Obstruction in Children: Paediatric Anaesthesia Tutorial 368Document9 pagesAcute Upper Airway Obstruction in Children: Paediatric Anaesthesia Tutorial 368Fireka JuniantikaNo ratings yet
- Guidelines For Evaluating Chronic Cough in Pediatrics: ACCP Evidence-Based Clinical Practice GuidelinesDocument24 pagesGuidelines For Evaluating Chronic Cough in Pediatrics: ACCP Evidence-Based Clinical Practice GuidelinescynnttNo ratings yet
- 06-Seminars in Fetal DevelopmentDocument75 pages06-Seminars in Fetal DevelopmentGanesh Subramanian MohanNo ratings yet
- Accuracy of The Interpretation of Chest Radiographs For The Diagnosis of Paediatric PneumoniaDocument5 pagesAccuracy of The Interpretation of Chest Radiographs For The Diagnosis of Paediatric Pneumoniania gusnawatiNo ratings yet
- Ni Hms 545265Document21 pagesNi Hms 545265Resti Zulvanita DeviNo ratings yet
- Tosse Cronica em CriançasDocument17 pagesTosse Cronica em CriançasEdvaldo Pereira da Silva JúniorNo ratings yet
- Dissertation On Bronchial AsthmaDocument7 pagesDissertation On Bronchial AsthmaInstantPaperWriterSpringfield100% (1)
- Wheezing Phenotypes in PreschoolersDocument4 pagesWheezing Phenotypes in PreschoolersRannyNo ratings yet
- Asthma Thesis PDFDocument5 pagesAsthma Thesis PDFmichellejohnsoncharleston100% (2)
- Diagnosis of Asthma in Children: ReferencesDocument6 pagesDiagnosis of Asthma in Children: Referencesdante_chungaNo ratings yet
- MainDocument6 pagesMainDiana Catalina Avila BareñoNo ratings yet
- Pediatrics 2003 Cunningham 436 40Document7 pagesPediatrics 2003 Cunningham 436 40Putu Agus GrantikaNo ratings yet
- Clinical Controversies in Aerosol Therapy For Infants and ChildrenDocument23 pagesClinical Controversies in Aerosol Therapy For Infants and Childrencelma44No ratings yet
- AOM CPG RevisedDocument26 pagesAOM CPG Revisedmefav7778520No ratings yet
- Asthma Research Paper ExampleDocument4 pagesAsthma Research Paper Exampleorlfgcvkg100% (1)
- Follow-Up Shows No Adverse Outcomes of CNEP in Neonates: LancetDocument1 pageFollow-Up Shows No Adverse Outcomes of CNEP in Neonates: LancetajuliocNo ratings yet
- A.Hislop ERS Course April 07Document93 pagesA.Hislop ERS Course April 07minerva_stanciuNo ratings yet
- Craniofacial and Upper Airway Morphology inDocument14 pagesCraniofacial and Upper Airway Morphology inkerminkNo ratings yet
- A Framework For The Management of The Pediatric AirwayDocument23 pagesA Framework For The Management of The Pediatric AirwayDaniel GallegoNo ratings yet
- As Ma Pediatric ADocument6 pagesAs Ma Pediatric APatricia GuíoNo ratings yet
- Research Paper Topics On AsthmaDocument6 pagesResearch Paper Topics On Asthmadldtcbulg100% (1)
- Prediction of Pneumonia in A Pediatric Emergency Department: PediatricsDocument10 pagesPrediction of Pneumonia in A Pediatric Emergency Department: PediatricsLeslie Lindsay AlvarezNo ratings yet
- Evidence-Based LaryngologyFrom EverandEvidence-Based LaryngologyDavid E. RosowNo ratings yet
- CPG Management of Childhood Asthma (2014)Document20 pagesCPG Management of Childhood Asthma (2014)Haz100% (1)
- Screening For Good Health: The Australian Guide To Health Screening And ImmunisationFrom EverandScreening For Good Health: The Australian Guide To Health Screening And ImmunisationNo ratings yet
- Diagnosis and Treatment of Chronic CoughFrom EverandDiagnosis and Treatment of Chronic CoughSang Heon ChoNo ratings yet
- Diffi Cult To Treat Asthma: Sandhya Khurana Fernando Holguin EditorsDocument339 pagesDiffi Cult To Treat Asthma: Sandhya Khurana Fernando Holguin Editorsneumologia.intervencionNo ratings yet
- 32-Acute Otitis MediaDocument11 pages32-Acute Otitis MediasasNo ratings yet
- Diagnostic Tests in Pediatric Pulmonology: Applications and InterpretationFrom EverandDiagnostic Tests in Pediatric Pulmonology: Applications and InterpretationStephanie D. DavisNo ratings yet
- N N N N: Outcomes in Children Treated For Persistent Bacterial BronchitisDocument3 pagesN N N N: Outcomes in Children Treated For Persistent Bacterial BronchitisJohalyn Esther AlvarezNo ratings yet
- Bronchiolitis High Risk ApneaDocument7 pagesBronchiolitis High Risk ApneaclikgoNo ratings yet
- Protracted Bacterial Bronchitis The Last DecadeDocument18 pagesProtracted Bacterial Bronchitis The Last DecadeyuniNo ratings yet
- Bronchial Asthma Research PaperDocument6 pagesBronchial Asthma Research Paperniisexgkf100% (1)
- Asthma DissertationDocument7 pagesAsthma DissertationBuyCollegePaperOnlineUK100% (1)
- The Impact of A Dedicated Physiotherapist Clinic For Children With Dysfunctional BreathingDocument6 pagesThe Impact of A Dedicated Physiotherapist Clinic For Children With Dysfunctional BreathingKuro ShibaNo ratings yet
- Pediatrics StridorDocument13 pagesPediatrics StridorEmaNo ratings yet
- Prevalence of Asthma in Australian ChildrenDocument4 pagesPrevalence of Asthma in Australian Childrenoktha_pohanNo ratings yet
- Copia de Otolaryngology Clinic of North America Evidence-Based Practice Management of Hoarseness-DysphoniaDocument18 pagesCopia de Otolaryngology Clinic of North America Evidence-Based Practice Management of Hoarseness-DysphoniaEdna R. Alvarez PaezNo ratings yet
- A Proposal For A'new Method of Evaluation - of The Newborn Infant PDFDocument8 pagesA Proposal For A'new Method of Evaluation - of The Newborn Infant PDFcbac1990No ratings yet
- Paediatric Dysphagia: How I Inform My Decisions (1) - Penetrating QuestionsDocument3 pagesPaediatric Dysphagia: How I Inform My Decisions (1) - Penetrating QuestionsSpeech & Language Therapy in PracticeNo ratings yet
- Case Study PN Pcap C FinalDocument50 pagesCase Study PN Pcap C FinalKimberly Milaran0% (1)
- 30 Scientific Studies Link Vaccines to AutismDocument23 pages30 Scientific Studies Link Vaccines to Autismazrulelias100% (5)
- Alergia AlimentariaDocument16 pagesAlergia AlimentariaUri MoraNo ratings yet
- Prevención NAC y EDA NiñosDocument13 pagesPrevención NAC y EDA NiñosUri MoraNo ratings yet
- Clinical Predictors of PneumoniaDocument10 pagesClinical Predictors of PneumoniaUri MoraNo ratings yet
- (Lung Biology in Health and Disease, V. 137) Richard D Bland - Jacqueline J Coalson-Chronic Lung Disease in Early Infancy-Marcel Dekker (2000)Document1,080 pages(Lung Biology in Health and Disease, V. 137) Richard D Bland - Jacqueline J Coalson-Chronic Lung Disease in Early Infancy-Marcel Dekker (2000)Uri MoraNo ratings yet
- Recommendation WHODocument176 pagesRecommendation WHODananjaya JuniorNo ratings yet
- Pulmonary Venoocclusive Disease in ChildhoodDocument8 pagesPulmonary Venoocclusive Disease in ChildhoodUri MoraNo ratings yet
- (European Respiratory Monograph) A. Bush, K-H. Carlsen, M.S. Zach-Growing Up With Lung Disease - The Lung in Transition To Adult Life-European Respiratory Society Journals Ltd. (2002)Document111 pages(European Respiratory Monograph) A. Bush, K-H. Carlsen, M.S. Zach-Growing Up With Lung Disease - The Lung in Transition To Adult Life-European Respiratory Society Journals Ltd. (2002)Uri MoraNo ratings yet
- Empiema en PediatriaDocument7 pagesEmpiema en PediatriaUri MoraNo ratings yet
- Oxygen Therapy CBPGDocument44 pagesOxygen Therapy CBPGUri Mora100% (2)
- Asthma and Respiratory Physiology Putting Lung Function Into PerspectiveDocument10 pagesAsthma and Respiratory Physiology Putting Lung Function Into PerspectiveUri MoraNo ratings yet
- Pulmonary Alveolar MicrolithiasisDocument9 pagesPulmonary Alveolar MicrolithiasisUri MoraNo ratings yet
- Acute Respiratory Distress Syndrome The Berlin DefinitionDocument8 pagesAcute Respiratory Distress Syndrome The Berlin DefinitionUri MoraNo ratings yet
- Measurement of FEF and FEF Does Not Contribute To Clinical Decision MakingDocument8 pagesMeasurement of FEF and FEF Does Not Contribute To Clinical Decision MakingUri MoraNo ratings yet
- LungFunction Ninos Menores 6 Anos 2013Document11 pagesLungFunction Ninos Menores 6 Anos 2013Uri MoraNo ratings yet
- Acute Kidney Injury - Final Version (08 March 2011)Document59 pagesAcute Kidney Injury - Final Version (08 March 2011)Abdel-hafiz MamounNo ratings yet
- Neonates Chest RXDocument9 pagesNeonates Chest RXUri MoraNo ratings yet
- Thorax and Lungs SGDocument2 pagesThorax and Lungs SGDestinee Caple100% (1)
- Ventilator LectureDocument57 pagesVentilator LecturemonishaNo ratings yet
- Right-sided heart failure secondary to cor pulmonaleDocument1 pageRight-sided heart failure secondary to cor pulmonaleAlyssa Mae Radam100% (1)
- BronchitisDocument2 pagesBronchitisАнастасия ПащенкоNo ratings yet
- Chest RetractionDocument11 pagesChest RetractionJURY LEIGH SALUQUENNo ratings yet
- Chest TubeDocument13 pagesChest TubeDanus RamadanusNo ratings yet
- 12 RLDDocument43 pages12 RLDNur akilaNo ratings yet
- Marik Covid Protocol Summary PDFDocument1 pageMarik Covid Protocol Summary PDFCiuvat Dumitru ValentinNo ratings yet
- Puritan Bennett Bi Level Breath Mode White PaperDocument12 pagesPuritan Bennett Bi Level Breath Mode White PaperEndar SulistyoNo ratings yet
- Suppurative Lung DiseasesDocument39 pagesSuppurative Lung Diseasesmatchees-gone rogueNo ratings yet
- Roleplay AsthmaDocument5 pagesRoleplay AsthmaDian WalineloNo ratings yet
- Ventilators, Intensive CareDocument48 pagesVentilators, Intensive CarealetripoleNo ratings yet
- Reflection Respiratory SystemDocument4 pagesReflection Respiratory SystemAin Sufiza0% (1)
- Types of Nebulizers - Ultrasonic, Vibrating Mesh, & Jet Nebulizers - NebologyDocument7 pagesTypes of Nebulizers - Ultrasonic, Vibrating Mesh, & Jet Nebulizers - NebologyUriel ChavarriaNo ratings yet
- Lesson Plan VentilatorDocument25 pagesLesson Plan VentilatorLoma Waghmare (Jadhav)No ratings yet
- Spirometry Testing - What Is A SpirometerDocument11 pagesSpirometry Testing - What Is A SpirometerFatima Sherrisa SaliNo ratings yet
- Vyntus-Family BR EN PDFDocument7 pagesVyntus-Family BR EN PDFLajoskaNo ratings yet
- Dr. Rowshne Jahan Spirometry Presentation-1Document40 pagesDr. Rowshne Jahan Spirometry Presentation-1Shahadat Hossain BabuNo ratings yet
- Pulmonary Function TestDocument39 pagesPulmonary Function TestLuqman AlwiNo ratings yet
- Postural Drainage Techniques for Mucus ClearanceDocument22 pagesPostural Drainage Techniques for Mucus ClearanceGhia_Angeles_8457No ratings yet
- Raus Respiratory Care Pharmacology 8th Edition Gardenhire Test BankDocument8 pagesRaus Respiratory Care Pharmacology 8th Edition Gardenhire Test Bankxuyenkeva3fon8100% (31)
- Client with Difficulty BreathingDocument6 pagesClient with Difficulty BreathingJoji BaitNo ratings yet
- BronchiectasisDocument40 pagesBronchiectasisyana jaeNo ratings yet
- Mechanical Ventilation - Lessons From The ARDSNet TrialDocument5 pagesMechanical Ventilation - Lessons From The ARDSNet TrialRDG20202No ratings yet
- Drugs Acting On The Respiratory SystemDocument13 pagesDrugs Acting On The Respiratory SystemAlloiBialbaNo ratings yet
- Health Teaching Plan For Cough and ColdDocument10 pagesHealth Teaching Plan For Cough and ColdMae VisperasNo ratings yet
- Chronic Obstructive Pulmonary DiseaseDocument2 pagesChronic Obstructive Pulmonary DiseaseAdam HuntNo ratings yet
- PhysioEx Exercise 7 Activity 2Document8 pagesPhysioEx Exercise 7 Activity 2villanuevaparedesaracely4No ratings yet
- Ventilator Associated PneumoniaDocument2 pagesVentilator Associated PneumoniaMuzana DariseNo ratings yet
- Chronic Obstructive Pulmonary Disease (COPD) Is A Condition ofDocument12 pagesChronic Obstructive Pulmonary Disease (COPD) Is A Condition ofDiana Jalaynie S. SambolawanNo ratings yet