Professional Documents
Culture Documents
Astm Bronsic Diagnostic Si Management PDF
Uploaded by
Alina GheOriginal Description:
Original Title
Copyright
Available Formats
Share this document
Did you find this document useful?
Is this content inappropriate?
Report this DocumentCopyright:
Available Formats
Astm Bronsic Diagnostic Si Management PDF
Uploaded by
Alina GheCopyright:
Available Formats
The information contained in this ICSI Health Care Guideline is intended primarily for health profes-
sionals and the following expert audiences:
physicians, nurses, and other health care professional and provider organizations;
health plans, health systems, health care organizations, hospitals and integrated health care
delivery systems;
medical specialty and professional societies;
researchers;
federal, state and local government health care policy makers and specialists; and
employee benefit managers.
This ICSI Health Care Guideline should not be construed as medical advice or medical opinion
related to any specific facts or circumstances. If you are not one of the expert audiences listed
above you are urged to consult a health care professional regarding your own situation and any
specific medical questions you may have. In addition, you should seek assistance from a health
care professional in interpreting this ICSI Health Care Guideline and applying it in your individual
case.
This ICSI Health Care Guideline is designed to assist clinicians by providing an analytical framework
for the evaluation and treatment of patients, and is not intended either to replace a clinicians
judgment or to establish a protocol for all patients with a particular condition. An ICSI Health Care
Guideline rarely will establish the only approach to a problem.
Copies of this ICSI Health Care Guideline may be distributed by any organization to the
organizations employees but, except as provided below, may not be distributed outside of the
organization without the prior written consent of the Institute for Clinical Systems Improvement,
Inc. If the organization is a legally constituted medical group, the ICSI Health Care Guideline may
be used by the medical group in any of the following ways:
copies may be provided to anyone involved in the medical groups process for developing and
implementing clinical guidelines;
the ICSI Health Care Guideline may be adopted or adapted for use within the medical group
only, provided that ICSI receives appropriate attribution on all written or electronic documents;
and
copies may be provided to patients and the clinicians who manage their care, if the ICSI Health
Care Guideline is incorporated into the medical groups clinical guideline program.
All other copyright rights in this ICSI Health Care Guideline are reserved by the Institute for Clinical
Systems Improvement. The Institute for Clinical Systems Improvement assumes no liability for
any adaptations or revisions or modifications made to this ICSI Health Care Guideline .
Health Care Guideline
I
CS
I
I NSTITUTE FOR CLINICAL
SYSTEMS I MPROVEMENT
Executive Summary March 2005
Diagnosis and Management of Asthma
Scope and Target Population:
This guideline addresses the diagnosis and outpatient management of acute and chronic asthma
in all patients over five years of age who present with asthma-like symptoms or have been
diagnosed with asthma.
Clinical Highlights for Individual Clinicians:
1. Conduct interval evaluations of asthma including medical history and physical
examination, assessment of asthma triggers and allergens, measurement of pulmonary
function, and consideration of consultation and/or allergy testing.
2. Regularly assess asthma control.
3. Match medical intervention with asthma severity and adjust to correspond with change
over time.
4. Achieve effective control of chronic persistent asthma through use of inhaled corticosteroid
therapy
5. Provide asthma education to patients and parents of pediatric patients. Education should
include basic facts about asthma, how medications work, inhaler technique, a written action
plan including home peak flow rate monitoring or a symptom diary, environmental control
measures, and emphasis on the need for regular follow-up visits.
Priority Aims:
1. Promote the accurate assessment of asthma severity through the use of objective measures
of lung function.
2. Promote long-term control of persistent asthma through the use of inhaled corticosteroid
drug therapy.
3. Promote the partnership of patients with asthma and/or their parents with health care
professionals through education and the use of written action plans.
Additional Background:
This guideline closely follows the recommendations of the: National Asthma Education Program
Expert Panel Report 2, Guidelines for the Diagnosis and Management of Asthma. NIH
Publication No. 97-4051. U.S. Department of Health and Human Services, Public Health
Service/National Institutes of Health/National Heart, Lung and Blood Institute.
Health Care Guideline:
Diagnosis and Outpatient Management of Asthma
These clinical guidelines are
designed to assist clinicians
by providing an analytical
framework for the evaluation
and treatment of patients, and
are not intended either to
replace a clinician's judgment
or to establish a protocol for
all patients with a particular
condition. A guideline will
rarel y establ i sh the onl y
approach to a problem.
Seventh Edition
March 2005
Work Group Leader
Richard Sveum, MD
Allergy, Park Nicollet Health
Services
Work Group Members
Allergy
Mary Keating, MD
CentraCare
Family Medicine
Michael Rethwill, MD
HealthPartners Medical Group
Pediatrics
Kent duRivage, MD
HealthPartners Medical Group
Pulmonary Medicine
Keith Harmon, MD
Park Nicollet Health Services
Certied Physician
Assistant
Eunice Weslander, PA-C
HealthPartners Central MN
Clinics
Nursing
Shirley Nordahl, CPNP
Allina Medical Clinic
Health Education
Janet Malkiewicz, RN AE-C
HealthPartners Medical Group
Respiratory Therapist/
Asthma Educator
Marlis O'Brien, RRT, CPFT,
AE-C
Mayo Health System -
Franciscan Skemp
Pharmacist/Asthma Educator
Brian Bach, RPh, AE-C
Mayo Health System -
Franciscan Skemp
Measurement Advisor
Beth Green, MBA, RRT
ICSI
Facilitator
Linda Setterlund, MA
ICSI
www.icsi.org
I I
CS
INSTITUTE FOR CLINICAL
SYSTEMS IMPROVEMENT
Copyright 2005 by Institute for Clinical Systems Improvement 1
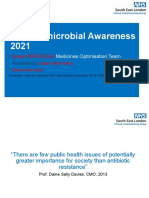
A = Annotation
Definitions and
symptoms of asthma
1
A
no
Previous
diagnosis of
asthma?
2
A
Establish
diagnosis of
asthma
3
A
Acute
asthma?
4
A
no
Interval evaluation:
Medical history
Assess asthma
triggers/allergens
Physical examination
Measure pulmonary
function
- spirometry
- PEFR
Consider consultation
and/or allergy testing
6
A
Assess asthma severity
7
A
Step care of pharmacologic
treatment:
mild intermittent
mild persistent
moderate persistent
severe persistent
8
A
Asthma education:
basic facts about asthma
how medications work
inhaler technique
written action plan based on
home peak flow rate monitoring
or symptom diary
environmental control measures
emphasize need for regular
follow-up visits
9
A
Schedule regular
follow-up visits
10
A
Management of acute
asthma:
2 agonists
Corticosteroids
Action plan
Follow-up for
chronic management
5
A
yes
yes
Institute for Clinical Systems Improvement
www.icsi.org
2
Algorithms and Annotations ................................................................................................................1-26
Algorithm ..............................................................................................................................................1
Foreword
Scope and Target Population ..........................................................................................................3
Clinical Highlights and Recommendations ....................................................................................3
Priority Aims ..................................................................................................................................3
Related ICSI Scientic Documents ................................................................................................3
Brief Description of Evidence Grading ..........................................................................................4
Disclosure of Potential Conict of Interest ....................................................................................4
Annotations ...........................................................................................................................................5-24
Appendices ............................................................................................................................................25-26
Annotation Appendix A Asthma Action Plan ..............................................................................25-26
Supporting Evidence ..............................................................................................................................27-38
Evidence Grading System .....................................................................................................................28-29
References .............................................................................................................................................30-31
Conclusion Grading Worksheets ...........................................................................................................32-38
Conclusion Grading Worksheet Appendix A Annotation #8
(Leukotriene Receptor Antagonists [LTRAs]) ..........................................................................32-35
Conclusion Grading Worksheet Appendix B Annotation #9
(Asthma Education) ...................................................................................................................36-38
Support for Implementation ................................................................................................................39-47
Priority Aims and Suggested Measures ................................................................................................40
Measurement Specications ...........................................................................................................41-44
Key Implementation Recommendations ...............................................................................................45
Knowledge Products .............................................................................................................................45
Recommended Resources .....................................................................................................................46-47
Table of Contents
Diagnosis and Outpatient Management of Asthma
Seventh Edition/March 2005
Institute for Clinical Systems Improvement
www.icsi.org
3
Foreword
Scope and Target Population
This guideline addresses the diagnosis and outpatient management of acute and chronic asthma in all patients
over ve years of age who present with asthma-like symptoms or have been diagnosed with asthma.
Clinical Highlights and Recommendations
1. Conduct interval evaluations of asthma including medical history and physical examination, assessment
of asthma triggers and allergens, measurement of pulmonary function, and consideration of consultation
and/or allergy testing. (Annotation #6)
2. Regularly assess asthma control. (Annotation #7)
3. Match medical intervention with asthma severity and adjust to correspond with change over time.
(Annotation #8 and Table 8A)
4. Achieve effective control of chronic persistent asthma through use of inhaled corticosteroid therapy.
(Table #8A)
5. Provide asthma education to patients and parents of pediatric patients. Education should include basic
facts about asthma, how medications work, inhaler technique, a written action plan including home peak
ow rate monitoring or a symptom diary, environmental control measures, and emphasis on the need
for regular follow-up visits. (Annotation #9)
Priority Aims
1. Promote the accurate assessment of asthma severity through the use of objective measures of lung func-
tion.
2. Promote long-term control of persistent asthma through the use of inhaled corticosteroid drug
therapy.
3. Promote the partnership of patients with asthma and/or their parents with health care professionals
through education and the use of written action plans.
Related ICSI Scientic Documents
Other ICSI guidelines whose scope and/or recommendations are closely related to the content of this guide-
line are:
1. Emergency and Inpatient Management of Asthma
2. Chronic Obstructive Pulmonary Disease
3. Rhinitis
Diagnosis and Outpatient Management of Asthma
Seventh Edition/March 2005
Institute for Clinical Systems Improvement
www.icsi.org
4
Evidence Grading
Individual research reports are assigned a letter indicating the class of report based on design type: A, B,
C, D, M, R, X.
Key conclusions are assigned a conclusion grade: I, II, III, or Grade Not Assignable.
A full explanation of these designators is found in the Supporting Evidence section of the guideline.
Disclosure of Potential Conict of Interest
In the interest of full disclosure, ICSI has adopted the policy of revealing relationships work group members
have with companies that sell products or services that are relevant to this guideline topic. The reader should
not assume that these nancial interests will have an adverse impact on the content of the guideline, but they
are noted here to fully inform readers. Readers of the guideline may assume that only work group members
listed below have potential conicts of interest to disclose.
No work group members have potential conicts of interest to disclose.
ICSI's conflict of interest policy and procedures are available for review on ICSI's website at
http://www.icsi.org.
Diagnosis and Outpatient Management of Asthma
Foreword Seventh Edition/March 2005
Institute for Clinical Systems Improvement
www.icsi.org
5
Algorithm Annotations
1. Denition and Symptoms of Asthma
Denition of asthma
Asthma is a chronic inammatory disorder of the airways. It is characterized by:
1. Airway inammatory cells, including eosinophils, macrophages, mast cells, epithelial cells and
activated lymphocytes that release various cytokines, adhesion molecules and other mediators.
2. Inammation resulting in an acute, subacute or chronic process that alters airway tone, modulates
vascular permeability, activates neurons, increases secretion of mucus, and alters airway structure
reversibly or permanently.
3. Airway hyperresponsiveness in response to allergens, environmental irritants, viral infections and
exercise.
4. Airow obstruction caused by acute bronchial constriction, edema, mucus plugs, and frequently
permanent remodeling.
A. Symptoms
1. Wheezing
2. Breathlessness
3. Cough, productive or dry
4. Chest discomfort
B. Pattern of symptoms
1. Perennial/seasonal
2. Episodic/continual
3. Diurnal
C. Severity of symptom classication
1. Number of symptom episodes per week
2. Number of nocturnal symptoms per month
3. Objective measures of lung function (FEV
1
, PEF, PEF variability)
Symptoms of asthma
Symptoms suggestive of asthma include episodic wheezing and cough with nocturnal, seasonal or exertional
characteristics. Infants and children with frequent episodes of "bronchitis" are likely to have asthma. Atopic
and positive family histories for asthma, particularly when associated with previously mentioned symptoms,
should encourage one to consider a diagnosis of asthma.
Eliciting symptoms should emphasize characterizing the current classication scheme that describes frequency
per week, changes in physical activity, diurnal variation, and seasonal variation. It is important to recognize
that patients with asthma are heterogeneous, falling into every age group, from infancy to older age, and
presenting a spectrum of signs and symptoms that vary in degree and severity from patient to patient as well
Diagnosis and Outpatient Management of Asthma
Seventh Edition/March 2005
Institute for Clinical Systems Improvement
www.icsi.org
6
as within an individual patient over time (National Asthma Education and Prevention Program [NAEPP],
1997; National Asthma Education and Prevention Program [NAEPP], 2002).
Supporting evidence is of classes: M, R
2. Previous Diagnosis of Asthma?
Key Points:
At each evaluation, it is important to consider whether or not a previous diag-
nosis was correct.
History and physical consistent with diagnosis.
Diagnosis conrmed by spirometry.
Response to therapy consistent with symptoms.
Diagnostic spirometry and a methacholine challenge test, if necessary, are important to clinching the diag-
nosis. The patient's history and response to therapy should guide other diagnostic tests when considering
alternative diagnoses. Follow-up pulmonary function tests every one to two years in mild asthmatics will
reconrm the diagnosis and objectify serial change and level of control. More frequent monitoring should
be considered for the moderate and severe persistent categories.
Spirometry is the cornerstone of the laboratory evaluation that enables the clinician to demonstrate airow
obstruction and establish a diagnosis of asthma with certainty. Spirometry is essential for assessing the
severity of asthma in order to make appropriate therapeutic recommendations. The use of objective measures
of lung function is recommended because patient-reported symptoms often do not correlate with the vari-
ability and severity of airow obstruction. Testing should be performed in compliance with the American
Thoracic Society standards. Obstructive and restrictive ventilatory defects can generally be determined
using FEV
1
/FVC ratio (American Thoracic Society, 1991).
Supporting evidence is of class: R
3. Establish Diagnosis of Asthma
Key Points:
The diagnosis of asthma is based on the patient's medical history, physical
examination, pulmonary function tests and laboratory test results.
Spirometry is recommended for the diagnosis of asthma.
A. Asthma triggers
1. Viral respiratory infections
2. Environmental allergens
3. Exercise, temperature, humidity
4. Occupational and recreational allergens or irritants
5. Environmental irritants (perfume, tobacco smoke, wood-burning stoves)
6. Drugs (aspirin, NSAID, beta blocker) and food (sultes)
Diagnosis and Outpatient Management of Asthma
Algorithm Annotations Seventh Edition/March 2005
Institute for Clinical Systems Improvement
www.icsi.org
7
B. Other historical components
1. Emergency room visits and hospitalization
2. Medication use (especially oral steroids)
3. Lung function, PEFR variability
4. Associated symptoms, e.g., rhinitis, sinusitis, gastroesophageal reux (GERD)
C. Clinical testing
1. Accurate spirometry is recommended in every patient 5 years of age or older at the time of diag-
nosis.
2. Additional studies done, tailored to the specic patient.
allergy testing (skin testing, in vitro specic IgE antibody testing)
chest radiography, to exclude alternative diagnosis
bronchial provocation testing if spirometry is normal or near normal
sinus x-rays or CT scan
GERD evaluation
CBC with eosinophils, total IgE, sputum exam
Spirometry is generally valuable in children 5 years of age or older, however some children cannot conduct
the maneuver depending on developmental ability. Spirometry measurements (FEV
1
, FVC, FEV
1
/FVC)
before and after the patient inhales a short-acting bronchodilator should be undertaken for patients in whom
the diagnosis of asthma is being considered. Airow obstruction is indicated by reduced FEV
1
and FEV
1
/
FVC values relative to reference or predicted values. Signicant reversibility is indicated by an increase of
12 percent or greater and 200 mL in FEV
1
, after inhaling a short-acting bronchodilator.
Methacholine challenge testing may provide a useful conrmatory diagnostic test in patients with normal
or near-normal spirometry. Investigation into the role of allergy, at least with a complete history, should
be done in every patient, given high prevalence of positive skin tests among individuals with asthma and
the benets of limiting exposure to known allergens. Eosinophil count and IgE may be elevated in asthma,
however, neither test has sufcient specicity or sensitivity to be used alone in a diagnosis. The chest x-ray
and electrocardiogram are usually normal in asthma but may be useful to exclude other pulmonary or cardiac
conditions. Sputum examination may be helpful if sputum eosinophilia or infection are suspected.
There are several clinical scenarios in children that have a frequent association with asthma and should
strongly suggest asthma as a possible diagnosis. These include recurrent pulmonary inltrates (especially
right middle lobe inltrates) that clear radiologically within two to three days, and the diagnosis of pneu-
monia without fever. Asthma may cause some radiologic uncertainty since mucus plugging and atelectasis
may be interpreted as inltrates.
Differential Diagnostic Possibilities for Asthma
1. Upper airway disease
allergic rhinitis and sinusitis
2. Obstruction involving large airways
foreign body in trachea or bronchus
Diagnosis and Outpatient Management of Asthma
Algorithm Annotations Seventh Edition/March 2005
Institute for Clinical Systems Improvement
www.icsi.org
8
vocal cord dysfunction
vascular rings or laryngeal webs
laryngotracheomalacia, tracheal stenosis or bronchostenosis
enlarged lymph nodes or tumor (benign or malignant)
bronchiectasis of various causes, including cystic brosis
3. Obstruction of small airways
viral bronchiolitis or obliterative bronchiolitis
cystic brosis
bronchopulmonary dysplasia
pulmonary inltrates with eosinophilia
chronic obstructive pulmonary disease (chronic bronchitis or emphysema)
4. Other causes
pulmonary embolism
congestive heart failure
cough secondary to drugs (angio-tension-converting enzyme [ACE] inhibitors)
aspiration from swallowing mechanism dysfunction or gastroesophageal reux
recurrent cough not due to asthma
It is important to identify infant or early childhood diseases that might supercially resemble asthma but
in reality are not asthmatic in pathophysiology. These symptoms should stimulate investigation of clinical
etiologies other than asthma (failure to thrive, vomiting/choking, chronic bacterial infections, cardiovascular
and pulmonary abnormalities).
An important under-recognized alternative diagnosis is vocal cord dysfunction. Patients have recurrent
breathlessness and wheezing, usually inspiratory, but they can also have expiratory wheezing. It is often
monophasic and loud over the glottis. Respiratory failure can occur with alveolar hypoventilation, requiring
emergent intubation. It also coexists in patients who have asthma. The ow-volume loop and video image
can help make the diagnosis.
4. Acute Asthma?
Symptoms of an acute asthma episode include progressive breathlessness, cough, wheezing or chest tight-
ness. An acute asthma episode is characterized by a decrease in expiratory airow that can be documented
and quantied by measurement of lung function (spirometry or PEFR). The algorithm is intended for treat-
ment of outpatients. Critically ill patients are beyond the scope of this guideline. See ICSI's Emergency
and Inpatient Management of Asthma.
Indications for emergency care include:
Peak ow less than 50% predicted normal
Failure to respond to a beta agonist
Severe wheezing or coughing
Diagnosis and Outpatient Management of Asthma
Algorithm Annotations Seventh Edition/March 2005
Institute for Clinical Systems Improvement
www.icsi.org
9
Extreme anxiety due to breathlessness
Gasping for air, sweaty, or cyanotic
Rapid deterioration over a few hours
Severe retractions and nasal aring
Hunched forward
5. Management of Acute Asthma
Key Points:
Patients experiencing an acute asthma exacerbation need a focused history
and physical examination and measurement of airow.
Treatment is begun with inhaled short-acting
2
-agonists administered by
meter dose inhaler (MDI)/spacer or nebulizer.
Further intensication of therapy is based on severity, response, and prior
history, but typically includes a short course of oral corticosteroids.
Decision to hospitalize must be individualized.
All patients should receive follow-up and short-term education.
The following is an outline of management:
Review history and physical exam which may include:
History
- Severity of symptoms, limitations, and sleep disturbance
- Duration of symptoms
- Current medical treatment plan
- Adherence to medical treatment plan
- Rescue medication use:
recent use of short-acting
2
-agonists
number of bursts of oral steroids in past year
- Review asthma action plan and daily charting of peak ows
- Previous ER visits or hospitalization
- Record triggers:
URI
Bronchitis, pneumonia
Exposure to allergens or irritants
Exercise
Diagnosis and Outpatient Management of Asthma
Algorithm Annotations Seventh Edition/March 2005
Institute for Clinical Systems Improvement
www.icsi.org
10
Physical exam
- Vital signs
- Auscultation of chest
- FEV
1
or
peak ow rate
- O
2
saturation (pulse oximetry)
- Use of accessory muscles
- Alertness
- Color
Laboratory studies
Treatment with bronchodilators should not be delayed for laboratory studies. Tests which may be
useful include:
- Arterial Blood Gases (ABG's)
- Chest X-Ray (CXR)
- Complete Blood Count (CBC)
- Electrocardiogram (EKG)
- Electrolytes
- Theophylline concentration
Assess severity
Assessment is based on history and physical exam.
Treatment
Usual initial treatment is with short-acting
2
-agonist (albuterol) administered by nebulizer or MDI/
spacer.
Alternatives:
Epinephrine: (1:1000)
Adult: 0.3-0.5 mg subq or IM q 20 min up to 3 doses
Pediatrics: 0.01 mg/kg up to 0.3-0.5 mg subq or IM every 20 min up to 3 doses
Ipratropium added to nebulized
2
-agonist (albuterol)
Nebulized dose for adults and those over 12 years of age is 0.5 mg every 4 hr. Not FDA approved
for any indication in those under 12 years of age.
Ipratropium is not currently FDA-approved for use in asthma.
Levalbuterol
Dose for adolescents 12 years of age and over and adults is 0.63 mg (via nebulizer) TID (every
6-8 hr); may increase to 1.25 mg via neb TID (every 6-8 hr) if patient does not exhibit adequate
response.
Diagnosis and Outpatient Management of Asthma
Algorithm Annotations Seventh Edition/March 2005
Institute for Clinical Systems Improvement
www.icsi.org
11
Dose for children 6-11 years of age is 0.31 mg (via nebulizer) TID. Routine dosing should not
exceed 0.63 mg TID.
Assess Response
Good response:
peak ow or FEV
1
greater than 70% predicted normal
no wheezing on auscultation
Incomplete response:
peak ow or FEV
1
50-70% predicted normal
mild wheezing
Consider hospitalization, particularly for high-risk patients:
past history of sudden severe exacerbation
prior intubation for asthma
two or more hospitalizations for asthma in the past year
three or more emergency care visits for asthma within the past year
hospitalization or an emergency care visit for asthma within the past month
use of more than 2 canisters per month of inhaled short-acting
2
-agonists
current use of systemic corticosteroids or recent withdrawal from systemic corticoste-
roids
difculty perceiving airow obstruction or its severity
comorbidity, as from cardiovascular disease or chronic obstructive pulmonary
disease
serious psychiatric disease or psychosocial problems
low socioeconomic status and urban residence
illicit drug use
sensitivity to Alternaria
Poor response:
peak ow or FEV
1
less than 50% predicted
no improvement in respiratory distress
strongly consider hospitalization
continue inhaled
2
-agonist every 60 minutes
start oral prednisone unless contraindicated
Adult: short course "burst" 40-60 mg/day as single or 2 divided doses for 3 to 10 days
Pediatric: short course "burst" 1-2 mg/kg day in 2 divided doses, maximum 60 mg/day for 3
to 10 days
Diagnosis and Outpatient Management of Asthma
Algorithm Annotations Seventh Edition/March 2005
Institute for Clinical Systems Improvement
www.icsi.org
12
Home treatment and revised asthma action plan
Medications
Inhaled
2
-agonist every 2-6 hours
Initiate or increase anti-inammatory medication:
inhaled corticosteroids
cromolyn/nedocromil
consider leukotriene modiers
Strongly consider systemic corticosteroids in patients with acute asthma exacerbation. Corti-
costeroids aid symptom resolution and prevent asthma relapse (Chapman, 1991; Fanta, 1983;
Harris, 1987; Scarfone, 1993).
Antibiotics are not recommended for the treatment of acute asthma except for those patients
with signs of acute bacterial infection, fever and purulent sputum.
Education
Teach or check inhaler technique/teach nebulizer use
Explain medications
Review action plan
Monitor peak ow
Reinforce trigger control
Follow-up
All patients need return appointment for management of asthma
Review and discuss signs and symptoms requiring emergent care
(National Asthma Education and Prevention Program Expert Panel, 1997; National Asthma Education
and Prevention Program Expert Panel Report: Guidelines for the Diagnosis and Outpatient Management
of Asthma, 2002)
Supporting evidence is of classes: A, M, R
6. Interval Evaluation
Interval evaluation of asthma should include the following:
- Medical history
- Assess asthma triggers/allergens
- Physical examination
- Measure pulmonary function
- Consider specialty consultation
Diagnosis and Outpatient Management of Asthma
Algorithm Annotations Seventh Edition/March 2005
Institute for Clinical Systems Improvement
www.icsi.org
13
Medical History
Disruption of usual activities (work, school, home)
Sleep disturbance
Level of usage of short-acting
2
-agonist
Adherence to medical treatment plan
Interval exacerbation of symptoms (either treated by self or a health care provider)
Symptoms suggesting comorbid conditions or alternative diagnosis
Side effects of medications
Reassessment of medical history can elicit factors that effect overall asthma control and sense of well-being
(Juniper, 1993). The key symptoms that should alert the clinician include disruptive daytime symptoms
and disturbances of sleep. It is also the consensus of the Expert Panel that symptoms early in the morning
that do not improve fteen minutes after short-acting
2
-agonist are a predictor of poor control. The quan-
tity of short-acting
2
-agonist that is being used should be discussed since overuse can be a marker of the
potentially fatality-prone asthmatic (Spitzer, 1992). The use of a quality of life tool or questionnaire can
assist to elicit history (Juniper, 1992).
Supporting evidence is of classes: C, D
Assess asthma triggers/allergens
Inquire about exposure to triggers and allergens (e.g., occupational, pets, smoke)
Allergy testing is recommended for patients with persistent asthma who are exposed to perennial
indoor allergens
Studies of emergency room visits and near death show allergens as a factor in asthma exacerbation. Asthma
triggers in the workplace also need to be considered. About 15 percent of asthma in adults is work related
(Blanc, 1987; Malo, 1992; O'Hollaren, 1991; Pollart, 1988).
The differential diagnosis, as previously discussed, can range from common to rare. The most common
contributing disorders that exacerbate asthma are allergic rhinitis and sinusitis (Corren, 1992; Rachelefsky,
1984). Another common condition to consider is gastroesophageal reux disease (GERD). Reux is three
times more common in asthmatics, and treating GERD leads to improved asthma control (Harper, 1987).
Supporting evidence is of classes: A, C, D
Physical Examination
Assess signs associated with asthma, concurrent illness or medication side effects
Height in children
Head, eyes, ears, nose, throat, lungs, heart, skin
It is important to discuss any potential medication side effects as this often has a direct relationship to compli-
ance. Common side effects from inhaled steroids include oral candidiasis and dysphonia.
2
-agonists may
cause tachycardia, tremor or nervousness. Individuals on long-term oral corticosteroids or frequent bursts
of steroids need to be monitored for complications of corticosteroids use such as osteoporosis, hypertension,
diabetes and Cushing's syndrome.
Diagnosis and Outpatient Management of Asthma
Algorithm Annotations Seventh Edition/March 2005
Institute for Clinical Systems Improvement
www.icsi.org
14
The height of individuals on corticosteroids should be monitored over time. The potential effect on linear
growth in children is important because these drugs tend to be used over long periods of time. Cumulative
data in children suggest that low-to-medium doses of inhaled corticosteroids may have the potential of
decreasing growth velocity, but this effect is not sustained in subsequent years of treatment, is not progres-
sive, and may be reversible (Childhood Asthma Management Program Research Group, The, 2000; NAEPP
Update, 2002).
Inhaled glucocorticoids used to treat asthma have been shown to have deleterious effects on bone mineral
density and markers of bone mineral metabolism. The risk of fracture attributable to inhaled or nasal gluco-
corticoids is uncertain (Lung Health Study Research Group, The, 2000).
The remainder of the physical exam either supports or refutes conditions and comorbidities discussed above
(see history).
Supporting evidence is of classes: A, M
Measure Pulmonary Function
It is important to measure pulmonary function at each follow-up visit. The two main methods are spirometry
and peak expiratory ow rate (PEFR). Spirometry is more precise and yields more information than PEFR.
It is helpful to verify the accuracy of the peak ow meter. It is useful when certain physical limitations
affect accuracy of PEFR (example: very young or elderly, neuromuscular or orthopedic problems) (Miles,
1995; Enright, 1994).
Spirometry recommended:
for initial diagnosis or to reassess or conrm diagnosis
after treatment is initiated or changed, and once symptoms and PEFR have stabilized, to docu-
ment attainment of "near normal pulmonary function"
at least every 1 to 2 years to assess maintenance of airway function; more often as severity
indicates
Regular monitoring of pulmonary function is particularly important for asthma patients who do not perceive
their symptoms until obstruction is severe (Kikuchi, 1994; Connolly, 1992).
PEFR
Used for follow-up, not for diagnosis
PEFR provides a simple, quantitative and reproductive measure of severity of airow obstruction. The
results are more reliable if the same type, and preferably the patient's own meter are used.
During interval assessment the clinician should question the patient and review records to evaluate the
frequency, severity and causes of exacerbation. Triggers that may contribute should be reviewed. All patients
on chronic maintenance medication should be questioned about exposure to inhalant allergens.
Supporting evidence is of classes: C, R
Consider Specialty Consultation
Adults with severe persistent asthma, consider for moderate persistent asthma
Children with moderate to severe persistent asthma, consider for mild persistent asthma
Diagnosis and Outpatient Management of Asthma
Algorithm Annotations Seventh Edition/March 2005
Institute for Clinical Systems Improvement
www.icsi.org
15
Poorly controlled or complex asthma including previous life-threatening asthma exacerbation,
or asthma exacerbations requiring more than 2 bursts of oral corticosteroids in 1 year, or asthma
complicated by other medical or psychosocial conditions
Additional diagnostic evaluations and/or testing, e.g., allergy skin testing, bronchoprovocation
Allergy testing is recommended for patients with persistent asthma who are exposed to perennial
indoor allergens
Evaluation and treatment of allergy, e.g., address occupation-related asthma, environmental coun-
seling, immunotherapy
Patients who require additional or intensive asthma education not otherwise available
For patients with moderate to severe persistent asthma, who are exposed to perennial indoor aller-
gens, Omalizumab is available. They should be managed by an allergy specialist.
Referral to an asthma specialist should be considered when a patient's symptoms are severe or are not
responding to standard care. Referral is also necessary when specialized testing, such as allergy testing
or bronchoprovocation are needed. There is evidence that referral to an asthma specialist can reduce
repeat visit to the emergency room (Zieger, 1991).
Supporting evidence is of class: C
7. Assess Asthma Severity
The classication of asthma as mild intermittent, mild persistent, moderate persistent or severe persistent
is based on the clinical characteristics as well as objective assessment of lung function through FEV
1
or
peak ow monitoring. The presence of one of the features of severity is sufcient to place a patient in
that category and an individual's classication may change over time. Patients at any level of severity can
have mild, moderate or severe exacerbations. Some patients with intermittent asthma experience severe
and life-threatening exacerbations separated by long periods of normal lung function and no symptoms
(National Asthma Education and Prevention Program, 1997; National Asthma Education and Prevention
Program, 2002).
Step 1: Mild Intermittent
symptoms twice a week or less
asymptomatic and normal PEF between exacerbations
exacerbations are brief (few hours to a few days)
nighttime symptoms twice a month or less
FEV
1
or PEF 80% predicted or greater and PEF variability 20% predicted or less
Step 2: Mild Persistent
symptoms twice a week or more but once a day or less
exacerbations may affect activity
nighttime symptoms twice a month or more
FEV
1
or PEF 80% predicted or greater and PEF variability 20-30% predicted
Diagnosis and Outpatient Management of Asthma
Algorithm Annotations Seventh Edition/March 2005
Institute for Clinical Systems Improvement
www.icsi.org
16
Step 3: Moderate Persistent
daily symptoms
daily use of inhaled short-acting beta
2
-agonists
exacerbations affect activity
exacerbations twice a week or more; may last days
nighttime symptoms once a week or more or 4 times per month
FEV
1
or PEF between 60-80% predicted
PEF variability 30% or greater
Step 4: Severe Persistent
continual symptoms
limited physical activity
frequent exacerbations
frequent nighttime symptoms
FEV
1
or PEF 60% predicted or less and PEF variability 30% predicted or greater
Supporting evidence is of classes: M, R
8. Step Care of Pharmacologic Treatment
Key Points:
Achieve effective control of chronic persistent asthma through use of inhaled
corticosteroid therapy.
The aim of asthma therapy is to maintain control of asthma with the least amount of medication and hence
minimize the risk for adverse effects. The stepwise approach to therapy in which the dose and number of
medications and frequency of administration are increased as necessary and decreased when possible is
used to achieve this control. Since asthma is a chronic inammatory disorder of the airways with recurrent
exacerbations, therapy for persistent asthma emphasizes efforts to suppress inammation over the long-term
and prevent exacerbations. See tables 8A, 8B, 8C, and 8D.
Based on data comparing LTRAs to inhaled corticosteroids, inhaled corticosteroids are the preferred treat-
ment option for mild persistent asthma in adults, and by extrapolation until published data become available,
for children. LTRAs are an alternative, although not preferred, treatment.
(Bleecker, 2000; Ducharme, 2002; National Asthma Education and Prevention Program, 1997; Szeer,
2005)
[Conclusion Grade I: See Conclusion Grading Worksheet Appendix A Annotation #8 (Leukotriene
Receptor Antagonists [LTRAs])]
Managing asthma during pregnancy is the same treatment used for non-pregnant asthma patients (NAEPP
Update, 2005).
NOTE: Annual inuenza vaccinations are recommended for patients with persistent asthma (National
Asthma Education and Prevention Program, 1997).
Supporting evidence is of classes: A, M, R
Diagnosis and Outpatient Management of Asthma
Algorithm Annotations Seventh Edition/March 2005
Institute for Clinical Systems Improvement
www.icsi.org
17
Table 8A.
Stepwise Approach for Managing Asthma in Adults and Children Older than 5 Years of Age
Step Long-Term Control
Step 1 - Mild Intermittent
symptoms 2 times a week
asymptomatic and normal PEF between exacerbations
exacerbations are brief (few hours to a few days)
nighttime symptoms 2 times a month
FEV
1
or PEF 80% predicted and PEF variability
20%
No daily medications needed
Step 2 - Mild Persistent
symptoms 2 times a week but 1 time a day
exacerbations may affect activity
nighttime symptoms 2 times a month
FEV
1
or PEF 80 percent predicted and PEF
variability 20-30%
Daily medication:
Inhaled corticosteroids (low dose) (preferred)
OR
Leukotriene modifiers, theophylline, nedocromil or cromolyn
Step 3 - Moderate Persistent
daily symptoms
daily use of inhaled short-acting
2
-agonists
exacerbation affects activity
exacerbations >2 week, may last days
nighttime symptoms >1 time a week
FEV
1
or PEF 60% - 80% predicted
PEF variability 30%
Daily medications:
Inhaled corticosteroid (low or medium dose) plus inhaled long-acting
2
agonist (preferred)
OR
Inhaled corticosteroid (medium dose) plus leukotriene modifier,
theophyline, or oral long-acting
2
Step 4 - Severe Persistent
continual symptoms
limited physical activity
frequent exacerbations
frequent nighttime symptoms
FEV
1
or PEF 60 % and PEF variability
30 %
Daily medications:
Inhaled corticosteroid
(medium dose or high dose)
PLUS: Long-acting
2
agonist (preferred)
and/OR Leukotriene modifier
and/OR Theophylline
Recommended for uncontrolled asthma:
Oral corticosteroids
(See Table 8D)
Step down:
Review treatment every 1-6 months; a gradual stepwise
reduction in treatment may be possible.
Step up:
If control not maintained, consider step up. First review patient
medication technique, adherence and environmental control (avoidance of
allergens or other factors that contribute to asthma severity)
Quick relief:
Short-acting bronchodilator: inhaled
2
-agonists as needed for symptoms with MDI spacer/holding chamber
Intensity of treatment will depend on severity of exacerbation.
Use of short-acting inhaled
2
-agonists on a daily basis, or increasing use, indicates the need for additional long-term control
therapy.
Education:
Step 1:
Teach basic facts about asthma
Teach inhaler/spacer/holding chamber technique
Discuss role of medications
Develop self-management plan
Develop action plan for when and how to take rescue actions, especially for patients with a history of severe exacerbations
Discuss appropriate environmental control measures to avoid exposure to known allergens and irritants
Step 2:
Teach self-monitoring
Refer to group education if available
Review and update self-management plan
Step 3:
Refer to individual education/counseling
Diagnosis and Outpatient Management of Asthma
Algorithm Annotations Seventh Edition/March 2005
Institute for Clinical Systems Improvement
www.icsi.org
18
Table 8B.
Usual Dosages for Long-Term Medications
Medication Dosage Form Adult Dose Child Dose Comments
Inhaled Corticosteroids (refer to Table 8C)
Systemic
Corticosteroids
Methylprednisolone
Prednisolone
Prednisone
2, 4, 8, 16, 32 mg
tablets
5 mg tablets,
5 mg/5 cc,
15 mg/5 cc
1, 2.5, 5, 10, 20, 50 mg
tablets
5 mg/5 cc
Divided 7.5-60
mg daily in a
single dose or
divided qid as
needed for control
Short-course
"burst" 40-60 mg
per day as single
or 2 divided doses
for 3-10 days
0.25-2 mg/kg
daily in single
dose or qid as
needed for control
Single course:
"burst" 1-2
mg/kg/day,
maximum 60
mg/day, for 3-10
days
(Applies to all three systemic
corticosteroids)
For long-term treatment of
severe persistent asthma,
administer single dose in
a.m. either daily or on
alternate days (alternate-
day therapy may produce
less adrenal suppression).
If daily doses are required,
one study suggests
improved efficacy and no
increase in adrenal
suppression when
administered at 3:00 p.m.
(Beam et al. 1992)
Short courses or "bursts
are effective for
establishing control when
initiating therapy or
during a period of gradual
deterioration.
The burst should be
continued until patient
achieves 80% PEF
personal best or symptoms
resolve. This usually
requires 3-10 days but may
require longer. There is no
evidence that tapering the
dose following
improvement prevents
relapse if sufficient doses
of inhaled corticosteroids
are used simultaneously.
Cromolyn and Nedocromil
Cromolyn
Nedocromil
MDI 800 g/puff
Nebulizer solution -
20 mg/ampule
MDI 1.75 mg/puff
2-4 puffs tid-qid
1 ampule tid-qid
2-4 puffs bid-qid
1-2 puffs tid-qid
1 ampule tid-qid
1-2 puffs bid-qid
One dose prior to exercise
or allergen exposure
provides effective
prophylaxis for 1-2 hours.
See cromolyn above.
Diagnosis and Outpatient Management of Asthma
Algorithm Annotations Seventh Edition/March 2005
Institute for Clinical Systems Improvement
www.icsi.org
19
Table 8B. (cont)
Usual Dosages for Long-Term Medications (continued)
Medication Dosage Form Adult Dose Child Dose Comments
Long-Acting
2
-Agonists
Salmeterol
Formoterol Fumarate DPI
Fluticasone propionate/
salmeterol DPI
Sustained-Release
Albuterol
Inhaled
DPI 50 g/inhalation
12 g/dose
(single use capsule by
inhalation)
Dosage strengths and
adult dose (one
inhalation) q 12 hr for
all three strengths) with
the strengths:
100 g fluticasone/50g
salmeterol
250 g fluticasone/50g
salmeterol
500 g fluticasone/50g
salmeterol
Tablet
4 mg tablet
1 inhalation q 12 hours
1 capsule by inhalation
BID
1 inhalation BID
4 mg q 12 hours
1 inhalation q 12 hours
1 capsule by inhalation
BID
1 inhalation BID
0.3-0.6 mg/kg/day, not
to exceed 8 mg/day
May use one dose nightly for
symptoms.
Should not be used for
symptom relief or for
exacerbations.
FDA approved for children 5
years of age and older.
FDA approved for children 4
years of age and older.
Methylxanthines
Theophylline Liquids, sustained-
release tablets, and
capsules
Starting dose 10
mg/kg/day up to 300
mg/day max
Starting dose 10
mg/kg/day; usual max:
<1 year of age: 0.2
(age in weeks) + 5 =
mg/kg/day
>1 year of age: 16
mg/kg/day
Adjust dosage to achieve serum
concentration of 5-15 g/mL
at a steady-state (at least 48
hours on same dosage).
Due to wide interpatient
variability in theophylline
metabolic clearance, routine
serum theophyline level
monitoring is important.
Average adult dose 600-900
mg/day
Leukotriene Modifiers
Montelukast 4 mg granules
4 mg tablet**
5 mg tablet**
10 mg tablet
10 mg/qhs 4 mg/qd evening or qhs
(2-5 years of age)
5 mg/qd evening or qhs
(6-14 years of age)
10 mg/qd evening or qhs
(15 years of age and
older)
Zafirlukast 10 mg tablet
20 mg tablet
40 mg daily
(20 mg bid)
( 12 years of age)
10 mg bid
(7-11 years of age)
For zafirlukast,
administration with meals
decreases bioavailability; take
at least 1 hour before or 2
hours after meals.
Zileuton 600 mg tablet 2,400 mg daily (one 600
mg tablet, qid)
600 mg tablet QID
(12 years of age and
older)
For zileuton, monitor hepatic
enzymes (ALT).
* This list is not all-inclusive; for discussion of other factors, see package inserts.
** Childrens dose chewable tablets.
Diagnosis and Outpatient Management of Asthma
Algorithm Annotations Seventh Edition/March 2005
Institute for Clinical Systems Improvement
www.icsi.org
20
Table 8C.
Estimated Comparative Daily Dosage for Inhaled Corticosteroids
ADULTS
Drug Low Dose Medium Dose High Dose
Beclomethasone
dipropionate HFA
(Hydrofluoroalkane)
formulation with
strengths of 40 g/puff
and 80 g/puff)
80 mg-240 mg
(2-6 puffs - 40 g)
(1-3 puffs - 80 g)
240 g- 480 g
(6-12 puffs - 40 g)
(3-6 puffs - 80 g)
> 480 g
(> 12 puffs - 40 g)
(> 6 puffs - 80 g)
Budesonide DPI
200 g/dose
200-600 g
(1-3 inhalations)
600-1200 g
(3-6 inhalations)
> 1200 g
(> 6 inhalations)
Flunisolide
250 g/puff
500-1,000 g
(2-4 puffs)
1,000-2,000 g
(4-8 puffs)
>2,000 g
(>8 puffs)
Fluticasone
MDI: 44, 110, 220
g/puff
88-264 g
(2-6 puffs - 44 g) OR
(2 puffs - 110 g)
264-660 g
(2-6 puffs - 110 g)
>660 g
(>6 puffs - 110 g) OR
(>3 puffs - 220 g)
Combination Product
fluticasone
propionate/salmeterol
DPI
100 g fluticasone/50 g
salmeterol one
inhalation q 12 hr
250 g fluticasone/50 g
salmeterol one
inhalation q 12 hr
500 g fluticasone/50 g
salmeterol one inhalation
q 12 hr
Triamcinolone acetonide
100 g/puff
400-1,000 g
(4-10 puffs)
1,000-2,000 g
(10-20 puffs)
>2,000 g
(>20 puffs)
NOTES:
The most important determinant of appropriate dosing is the clinician's judgment of the patient's response to
therapy. The clinician must monitor the patient's response on several clinical parameters and adjust the dose
accordingly. The stepwise approach to therapy emphasizes that once control of asthma is achieved, the dose of
medication should be carefully titrated to the minimum dose required to maintain control, thus reducing the
potential for adverse effect.
Some dosages may be outside package labeling.
MDI dosages are expressed as the actuater dose (the amount of drug leaving the actuater and delivered to the
patient), which is the labeling required in the United States. This is different from the dosage expressed as the
valve dose (the amount of drug leaving the valve, all of which is not available to the patient), which is used in
many European countries and in some of the scientific literature. DPI doses are expressed as the amount of drug in
the inhaler following activation.
Budesonide is the preferred inhaled for pregnant women corticosteroid because more data are available on using
budesonide in pregnancy than are available on other inhaled corticosteroids, and the data are reassuring. It is
important to note that there are no data indicating that the other inhaled corticosteroid preparations are unsafe
during pregnancy.
Diagnosis and Outpatient Management of Asthma
Algorithm Annotations Seventh Edition/March 2005
Institute for Clinical Systems Improvement
www.icsi.org
21
Table 8C. (cont)
Estimated Comparative Daily Dosage for Inhaled Corticosteroids
CHILDREN
Drug Low Dose Medium Dose High Dose
Beclomethasone
dipropionate HFA
40 g/puff
80 g/puff
84-336 g
80-160 g
(2-4 puffs - 40 g)
(1-2 puffs- 80 g)
336-672 g
160-320 g
(4-8 puffs - 40 g)
(2-4 puffs - 80 g)
> 672 g
> 320 g
(> 8 puffs - 40 g)
(> 4 puffs - 80 g)
Budesonide DPI
200 g/dose
For nebulization:
strengths 0.25 mg/2 mL
and 0.5 mg/2 mL
200-400 g
(1-2 inhalations)
0.5 mg
400-800 g
(2-4 inhalations - 200 g)
1.0 mg/day
> 800 g
(> 4 inhalations - 200 g)
2.0 mg/day
Flunisolide
250 g/puff
500-750 g
(2-3 puffs)
1,000-1,250 g
(4-5 puffs)
>1,250 g
(> 5 puffs)
Fluticasone
MDI: 44, 110, 220
g/puff
88-176 g
(2-4 puffs - 44 g)
176-440 g
(4-10 puffs - 44 g) OR
(2-4 puffs - 110 g)
> 440 g
(> 4 puffs - 110 g) OR
(> 2 puffs - 220 g)
Triamcinolone acetonide
100 g/puff
400-800 g
(4-8 puffs)
800-1,200 g
(8-12 puffs)
> 1,200 g
(> 12 puffs)
NOTES:
The most important determinant of appropriate dosing is the clinician's judgement of the patient's response to
therapy. The clinician must monitor the patient's response on several clinical parameters and adjust the dose
accordingly. The stepwise approach to therapy emphasizes that once control of asthma is achieved, the dose of
medication should be carefully titrated to the minimum dose required to maintain control, thus reducing the
potential for adverse effect.
The reference point for the range in the dosages for children is data on the safety of inhaled corticosteroids in
children, which, in general, suggest that the dose ranges are equivalent to beclomethasone dipropionate 200-400
g/day (low dose), 400-800 g/day (medium dose), and > 800 g/day (high dose).
Some dosages may be outside package labeling.
MDI dosages are expressed as the actuater dose (the amount of drug leaving the actuater and delivered to the
patient), which is the labeling required in the United States. This is different from the dosage expressed as the
valve dose (the amount of drug leaving the valve, all of which is not available to the patient), which is used in
many European countries and in some of the scientific literature. DPI doses are expressed as the amount of drug in
the inhaler following activation.
Diagnosis and Outpatient Management of Asthma
Algorithm Annotations Seventh Edition/March 2005
Institute for Clinical Systems Improvement
www.icsi.org
22
Table 8D.
Usual Dosages for Quick-Relief Medications
Medication Dosage Form Adult Dose Child Dose Comments
Short-Acting Inhaled Beta
2
-Agonists
Albuterol
Albuterol HFA
Pirbuterol
MDIs
90 g/puff, 200
puffs
90 g /puff, 200
puffs
200 g /puff, 400
puffs
2 puffs 5
minutes prior to
exercise
2 puffs tid-qid
prn
1-2 puffs 5
minutes prior to
exercise
2 puffs tid-qid
prn
An increasing use or lack of expected effect
indicates diminished control of asthma.
Not generally recommended for long-term
treatment. Regular use on a daily basis
indicates the need for additional long-term
controller therapy.
Differences in potency exist so that all
products are essentially equal in efficacy on
a per puff basis.
May double usual dose for mild
exacerbations.
Nonselective agents (i.e., epinephrine,
isoproterenol, metaproterenol) are not
recommended due to their potential for
excessive cardiac stimulation, especially in
high doses.
Spacer/holding chambers are
recommended with MDI
Albuterol
Levalbuterol
nebulization
DPI
Nebulizer solution
5 mg/mL (0.5%)
Premixed Vials
2.5 mg/3 mL
(0.088%)
1.25 mg/3mL
(0.042%)
0.63 mg/3 mL and
1.25 mg/3 mL
1.25-5 mg (.25-1 cc)
in 2-3 cc of saline q
4-8 hours
12 yrs and older is
0.63 mg to 1.25 mg
TID
0.05 mg/kg (min
1.25 mg, max 2.5
mg) in 2-3 cc of
saline q 4-6 hours
6-11 years is 0.31
mg to 0.63 mg TID
May mix with cromolyn or ipratropium
nebulizer solutions. May double dose for
mild exacerbations.
Routine dosing should not exceed 0.63 mg
TID in children
Anticholinergics
Ipratropium
MDIs
18 g/puff, 200
puffs
Nebulizer/solution
.25 mg/mL
(0.025%)
2-6 puffs q 6 hours
0.25-0.5 mg q 6
hours
1-2 puffs q 6 hours
0.25 mg q 6 hours
Evidence is lacking for anticholinergice
producing added benefit to
2
-agonists in
long-term asthma therapy.
Systemic Corticosteroids (Applies to all three systemic corticosteroids)
Methylprednisolone
Prednisolone
Prednisone
2, 4, 8, 16, 32 mg
tablets
5 mg tabs, 5 mg/5
cc, 15 mg/5 cc
1, 2.5, 5, 10, 20 25
mg tabs; 5 mg/cc;
5 mg/5 cc
short course
"burst": 40-60
mg/day as
single or 2
divided doses
for 3-10 days
Short course
"burst": 1-2
mg/kg/day,
maximum 60
mg/day, for
3-10 days
Short courses or "bursts" are effective for
establishing control when initiating therapy
or during a period of gradual deterioration.
The burst should be continued until patient
achieves 80% PEF personal best or
symptoms resolve. This usually requires 3-
10 days but may require longer. There is no
evidence that tapering the dose following
improvement prevents relapse if sufficient
doses of inhaled corticosteroids are used
simultaneously.
Diagnosis and Outpatient Management of Asthma
Algorithm Annotations Seventh Edition/March 2005
Institute for Clinical Systems Improvement
www.icsi.org
23
9. Asthma Education
Key Points:
Patient education is essential for successful management of asthma. It should
begin at the time of diagnosis and be ongoing.
The following patient education is recommended:
Basic facts about asthma
- The contrast between asthmatic and normal airways
- What happens to the airways in an asthma attack
How medications work and the need for adherence
- Long-term control: medications that prevent symptoms, often by reducing inammation
- Quick relief: short-acting bronchodilator relaxes muscles around airways
- Stress the importance of long-term control medications and not to expect quick relief from
them
Inhaler technique
- Metered dose inhaler (MDI) or nebulizer use (patient should repeat demonstration)
- Spacer/holding chamber use with MDI
- Dry powder inhaler
Written action plan including home peak ow monitoring
When and how to take actions
- Symptom monitoring and recognizing early signs of deterioration.
- Responding to changes in asthma severity. A written Asthma Action
Plan including daily medications and instructions should be offered to
all patients with asthma.
Review and rene the plan at follow-up visits.
- Home peak ow monitoring is recommended for patients with moderate to
severe persistent asthma, or anyone with a history of severe exacerbations.
- Discuss plan for children at school including management of exercise-
induced bronchospasm.
- Assess adherence to pharmacotherapy and environmental control
measures.
Data are insufcient to support or refute the benets of using written asthma action plans compared to
medical management alone. However, a Cochrane review of 25 studies compared self-management
interventions by adults with acute asthma episodes. Some had written action plans, others did not. The
self-management interventions with written action plans had the greatest benets, including reduced
emergency department visits and hospitalizations and improved lung function (NAEPP update 2002).
Diagnosis and Outpatient Management of Asthma
Algorithm Annotations Seventh Edition/March 2005
Institute for Clinical Systems Improvement
www.icsi.org
24
The NAEPP EPR-2 continues to recommend the use of written action plans as part of an overall effort
to educate patients in self-management is benecial especially for patients with moderate or severe
persistent asthma and patients with a history of severe exacerbations.
Environmental control measures
- Identifying and avoiding exposure to allergens or other environmental triggers
Emphasize need for regular follow-up visits and asthma treatment adherence
Supervised self-management (using patient education and adjustments of anti-inammatory medica-
tion based on PEF or symptoms coupled with regular medical review, utilization and adherence to
medication) reduces asthma morbidity. This reduction includes lost work days, unscheduled ofce
visits, and ER and hospital admissions (Gibson, 2000; Ignatio-Garcia, 1995; Lahdensuo, 1996).
[Conclusion Grade I: See Conclusion Grading Worksheet Appendix B Annotation #9 (Asthma Educa-
tion)]
A sample Asthma Action Plan is attached in Annotation Appendix A, "Asthma Action Plan."
See Minnesota Department of Health Action Plan at http://www.mnasthma.org/AAP/
Supporting evidence is of classes: A, M, R
10. Schedule Regular Follow-Up Visits
Asthma is a chronic inammatory lung disease and all chronic diseases need regular follow-up visits. Prac-
titioners need to assess whether or not control of asthma has been maintained and if a step down in therapy is
appropriate. Further, practitioners need to monitor and review the daily self-management and action plans,
the medications, and the patient's inhaler and peak ow monitoring techniques.
The exact frequency of clinician visits is a matter of clinical judgement
Severity Regular follow-up visit
Mild Intermittent 6-12 months
Mild Persistent 6 months
Moderate Persistent 3 months
Severe Persistent 1 to 2 months and as often as needed to establish control
Diagnosis and Outpatient Management of Asthma
Algorithm Annotations Seventh Edition/March 2005
Institute for Clinical Systems Improvement
www.icsi.org
25
H
o
w
t
o
u
s
e
t
h
e
p
e
a
k
f
l
o
w
m
e
t
e
r
1
.
P
l
a
c
e
i
n
d
i
c
a
t
o
r
a
t
b
a
s
e
o
f
t
h
e
s
c
a
l
e
.
2
.
S
t
a
n
d
u
p
.
3
.
T
a
k
e
a
d
e
e
p
b
r
e
a
t
h
.
4
.
P
l
a
c
e
t
h
e
m
e
t
e
r
i
n
m
o
u
t
h
a
n
d
c
l
o
s
e
l
i
p
s
a
r
o
u
n
d
t
h
e
m
o
u
t
h
p
i
e
c
e
.
5
.
B
l
o
w
o
u
t
a
s
h
a
r
d
a
n
d
f
a
s
t
a
s
p
o
s
s
i
b
l
e
.
6
.
R
e
p
e
a
t
t
h
e
p
r
o
c
e
s
s
t
w
o
m
o
r
e
t
i
m
e
s
.
7
.
R
e
c
o
r
d
t
h
e
h
i
g
h
e
s
t
o
f
t
h
e
t
h
r
e
e
n
u
m
b
e
r
s
.
H
o
w
t
o
u
s
e
t
h
e
i
n
h
a
l
e
r
1
.
S
h
a
k
e
t
h
e
i
n
h
a
l
e
r
a
n
d
a
t
t
a
c
h
s
p
a
c
e
r
i
f
n
e
e
d
e
d
.
2
.
S
t
a
n
d
u
p
.
3
.
B
r
e
a
t
h
e
i
n
m
e
d
i
c
a
t
i
o
n
s
l
o
w
l
y
t
h
r
o
u
g
h
s
p
a
c
e
r
.
4
.
H
o
l
d
b
r
e
a
t
h
f
o
r
1
0
s
e
c
o
n
d
s
.
5
.
B
r
e
a
t
h
e
o
u
t
s
l
o
w
l
y
.
6
.
R
e
p
e
a
t
p
u
f
f
s
a
s
d
i
r
e
c
t
e
d
a
n
d
w
a
i
t
t
w
o
t
o
f
i
v
e
m
i
n
u
t
e
s
b
e
t
w
e
e
n
p
u
f
f
s
.
7
.
R
i
n
s
e
m
o
u
t
h
w
i
t
h
w
a
t
e
r
a
f
t
e
r
i
n
h
a
l
i
n
g
s
t
e
r
o
i
d
s
t
o
p
r
e
v
e
n
t
t
h
r
u
s
h
.
C
o
m
m
u
n
i
t
y
A
s
t
h
m
a
E
d
u
c
a
t
i
o
n
S
u
p
e
r
A
s
t
h
m
a
S
a
t
u
r
d
a
y
A
s
t
h
m
a
C
a
m
p
s
O
p
e
n
A
i
r
w
a
y
f
o
r
S
c
h
o
o
l
s
A
s
t
h
m
a
S
u
p
p
o
r
t
G
r
o
u
p
s
A
s
t
h
m
a
U
p
d
a
t
e
N
e
w
s
l
e
t
t
e
r
F
o
r
i
n
f
o
r
m
a
t
i
o
n
,
c
a
l
l
:
A
m
e
r
i
c
a
n
L
u
n
g
A
s
s
o
c
i
a
t
i
o
n
o
f
M
i
n
n
e
s
o
t
a
a
t
(
6
1
2
)
2
2
7
-
8
0
1
4
o
r
1
-
8
0
0
-
6
4
2
-
L
U
N
G
A
m
e
r
i
c
a
n
L
u
n
g
A
s
s
o
c
i
a
t
i
o
n
o
f
H
e
n
n
e
p
i
n
C
o
u
n
t
y
a
t
(
6
1
2
)
8
7
1
-
7
3
3
2
A
d
d
i
t
i
o
n
a
l
I
n
f
o
r
m
a
t
i
o
n
W
r
i
t
e
o
r
c
a
l
l
:
A
l
l
e
r
g
y
a
n
d
A
s
t
h
m
a
N
e
t
w
o
r
k
/
M
o
t
h
e
r
s
o
f
A
s
t
h
m
a
t
i
c
s
,
I
n
c
.
3
5
5
4
C
h
a
i
n
B
r
i
d
g
e
R
o
a
d
,
S
u
i
t
e
2
0
0
F
a
i
r
f
a
x
,
V
A
2
2
0
3
0
-
2
7
0
9
(
7
0
3
)
3
8
5
-
4
4
0
3
A
d
d
i
t
i
o
n
a
l
R
e
a
d
i
n
g
C
h
i
l
d
r
e
n
W
i
t
h
A
s
t
h
m
a
b
y
T
h
o
m
a
s
F
.
P
l
a
u
t
,
M
D
T
h
e
A
s
t
h
m
a
H
a
n
d
b
o
o
k
a
n
d
T
h
e
B
e
s
t
o
f
S
u
p
e
r
S
t
u
f
f
b
y
t
h
e
A
m
e
r
i
c
a
n
L
u
n
g
A
s
s
o
c
i
a
t
i
o
n
W
h
a
t
E
v
e
r
y
o
n
e
N
e
e
d
s
t
o
K
n
o
w
A
b
o
u
t
A
s
t
h
m
a
b
y
t
h
e
A
l
l
e
r
g
y
a
n
d
A
s
t
h
m
a
N
e
t
w
o
r
k
W
i
n
n
i
n
g
O
v
e
r
A
s
t
h
m
a
b
y
E
i
l
e
e
n
D
o
l
a
n
S
a
v
a
g
e
A
s
t
h
m
a
A
c
t
i
o
n
P
l
a
n
P
a
t
i
e
n
t
N
a
m
e
D
a
t
e
o
f
B
i
r
t
h
C
h
a
r
t
N
u
m
b
e
r
P
r
o
v
i
d
e
r
(
s
)
C
l
i
n
i
c
P
h
o
n
e
N
u
m
b
e
r
T
o
b
e
s
t
m
a
n
a
g
e
y
o
u
r
a
s
t
h
m
a
,
y
o
u
w
i
l
l
n
e
e
d
t
o
f
o
l
l
o
w
t
h
e
i
n
s
t
r
u
c
t
i
o
n
s
i
n
t
h
i
s
a
s
t
h
m
a
a
c
t
i
o
n
p
l
a
n
e
s
p
e
c
i
a
l
l
y
d
e
s
i
g
n
e
d
f
o
r
y
o
u
.
Annotation Appendix A Asthma Action Plan
Diagnosis and Outpatient Management of Asthma
Seventh Edition/March 2005
Institute for Clinical Systems Improvement
www.icsi.org
26
Diagnosis and Outpatient Management of Asthma
Annotation Appendix A Asthma Action Plan Seventh Edition/March 2005
G
r
e
e
n
Z
o
n
e
:
A
l
l
C
l
e
a
r
P
e
r
s
o
n
a
l
b
e
s
t
p
e
a
k
f
l
o
w
P
e
a
k
f
l
o
w
(
8
0
-
1
0
0
%
o
f
p
e
r
s
o
n
a
l
b
e
s
t
)
S
y
m
p
t
o
m
s
:
N
o
s
y
m
p
t
o
m
s
o
f
a
s
t
h
m
a
A
b
l
e
t
o
p
a
r
t
i
c
i
p
a
t
e
i
n
u
s
u
a
l
a
c
t
i
v
i
t
i
e
s
N
o
s
l
e
e
p
d
i
s
t
u
r
b
a
n
c
e
b
y
a
s
t
h
m
a
s
u
c
h
a
s
c
o
u
g
h
i
n
g
,
w
h
e
e
z
i
n
g
,
s
h
o
r
t
n
e
s
s
o
f
b
r
e
a
t
h
o
r
c
h
e
s
t
t
i
g
h
t
n
e
s
s
M
e
d
i
c
a
t
i
o
n
s
:
N
a
m
e
D
o
s
e
T
i
m
e
M
e
d
i
c
a
t
i
o
n
s
i
d
e
e
f
f
e
c
t
s
:
I
n
h
a
l
e
r
,
s
p
a
c
e
r
,
n
e
b
u
l
i
z
e
r
o
r
r
o
t
o
c
a
p
s
P
a
r
t
i
c
i
p
a
t
i
o
n
i
n
r
u
n
n
i
n
g
,
p
l
a
y
i
n
g
a
n
d
s
p
o
r
t
s
;
t
a
k
e
b
e
f
o
r
e
e
x
e
r
c
i
s
e
D
i
a
r
y
c
a
n
b
e
u
s
e
d
w
i
t
h
p
e
a
k
f
l
o
w
m
e
t
e
r
a
n
d
/
o
r
s
y
m
p
t
o
m
s
E
n
v
i
r
o
n
m
e
n
t
a
l
c
o
n
t
r
o
l
o
f
a
s
t
h
m
a
t
r
i
g
g
e
r
s
,
e
.
g
.
,
c
i
g
a
r
e
t
t
e
s
m
o
k
e
,
e
x
e
r
c
i
s
e
,
i
l
l
n
e
s
s
,
c
o
l
d
a
i
r
,
a
n
i
m
a
l
s
,
e
t
c
.
Y
e
l
l
o
w
Z
o
n
e
:
C
a
u
t
i
o
n
P
e
a
k
f
l
o
w
(
5
0
-
8
0
%
o
f
p
e
r
s
o
n
a
l
b
e
s
t
)
E
a
r
l
y
w
a
r
n
i
n
g
s
i
g
n
s
o
f
a
c
u
t
e
a
s
t
h
m
a
e
p
i
s
o
d
e
:
C
o
u
g
h
i
n
g
R
u
n
n
y
,
s
t
u
f
f
y
o
r
c
o
n
g
e
s
t
e
d
n
o
s
e
S
n
e
e
z
i
n
g
N
o
t
s
l
e
e
p
i
n
g
o
r
e
a
t
i
n
g
w
e
l
l
T
i
r
e
d
,
w
e
a
k
o
r
l
o
w
e
n
e
r
g
y
I
t
c
h
y
o
r
w
a
t
e
r
y
e
y
e
s
D
r
o
p
i
n
p
e
a
k
f
l
o
w
m
e
t
e
r
r
e
a
d
i
n
g
S
y
m
p
t
o
m
s
o
f
a
c
u
t
e
a
s
t
h
m
a
e
p
i
s
o
d
e
:
R
a
p
i
d
b
r
e
a
t
h
i
n
g
W
h
e
e
z
i
n
g
F
r
e
q
u
e
n
t
,
t
i
g
h
t
c
o
u
g
h
D
i
f
f
i
c
u
l
t
y
b
r
e
a
t
h
i
n
g
o
u
t
S
u
c
k
i
n
g
i
n
t
h
e
c
h
e
s
t
s
k
i
n
b
e
t
w
e
e
n
t
h
e
r
i
b
s
B
e
g
i
n
o
r
i
n
c
r
e
a
s
e
m
e
d
i
c
a
t
i
o
n
s
i
f
w
a
r
n
i
n
g
s
i
g
n
s
o
r
s
y
m
p
t
o
m
s
b
e
c
o
m
e
w
o
r
s
e
o
r
l
a
s
t
m
o
r
e
t
h
a
n
1
2
h
o
u
r
s
.
I
f
u
n
s
u
r
e
,
c
a
l
l
y
o
u
r
c
l
i
n
i
c
.
M
e
d
i
c
a
t
i
o
n
s
:
N
a
m
e
D
o
s
e
T
i
m
e
M
e
d
i
c
a
t
i
o
n
s
i
d
e
e
f
f
e
c
t
s
:
I
f
n
o
s
y
m
p
t
o
m
r
e
l
i
e
f
w
i
t
h
i
n
3
0
m
i
n
u
t
e
s
o
f
g
i
v
i
n
g
m
e
d
i
c
a
t
i
o
n
a
n
d
p
e
a
k
f
l
o
w
i
s
%
,
a
d
d
o
r
a
l
s
t
e
r
o
i
d
R
e
d
Z
o
n
e
:
M
e
d
i
c
a
l
A
l
e
r
t
P
e
a
k
f
l
o
w
:
(
l
e
s
s
t
h
a
n
5
0
%
o
f
p
e
r
s
o
n
a
l
b
e
s
t
)
S
e
v
e
r
e
s
y
m
p
t
o
m
s
r
e
q
u
i
r
i
n
g
i
m
m
e
d
i
a
t
e
m
e
d
i
c
a
l
c
a
r
e
:
F
l
a
r
e
d
n
o
s
t
r
i
l
s
H
u
n
c
h
e
d
b
o
d
y
P
r
o
l
o
n
g
e
d
s
h
o
r
t
n
e
s
s
o
f
b
r
e
a
t
h
n
o
t
r
e
-
l
i
e
v
e
d
b
y
m
e
d
i
c
a
t
i
o
n
o
r
o
n
l
y
b
r
i
e
f
r
e
l
i
e
f
M
e
d
i
c
a
t
i
o
n
i
n
s
t
r
u
c
t
i
o
n
s
:
G
i
v
e
o
r
a
l
s
t
e
r
o
i
d
:
C
a
l
l
c
l
i
n
i
c
#
C
a
l
l
9
1
1
i
f
y
o
u
o
b
s
e
r
v
e
t
h
e
s
e
s
y
m
p
t
o
m
s
:
G
a
s
p
i
n
g
f
o
r
a
i
r
w
i
t
h
s
w
e
a
t
i
n
g
E
x
t
r
e
m
e
a
n
x
i
e
t
y
d
u
e
t
o
d
i
f
f
i
c
u
l
t
y
b
r
e
a
t
h
i
n
g
C
o
n
d
i
t
i
o
n
r
a
p
i
d
l
y
g
e
t
t
i
n
g
w
o
r
s
e
A
s
t
h
m
a
i
n
s
c
h
o
o
l
o
r
d
a
y
c
a
r
e
N
e
x
t
a
s
t
h
m
a
a
p
p
o
i
n
t
m
e
n
t
a
n
d
h
o
w
m
u
c
h
t
i
m
e
w
i
l
l
b
e
n
e
e
d
e
d
P
a
t
i
e
n
t
N
a
m
e
D
a
t
e
o
f
B
i
r
t
h
P
r
o
v
i
d
e
r
S
i
g
n
a
t
u
r
e
D
a
t
e
Availability of references
References cited are available to ICSI participating member groups
on request from the ICSI ofce. Please ll out the reference request
sheet included with your guideline and send it to ICSI.
27 Copyright 2005 by Institute for Clinical Systems Improvement
Released in March 2005 for Seventh Edition.
The next scheduled revision will occur within 24 months.
Contact ICSI at:
8009 34th Avenue South, Suite 1200; Bloomington, MN 55425; (952) 814-7060; (952) 858-9675 (fax)
Online at http://www.ICSI.org
I I
CS
INSTITUTE FOR CLINICAL
SYSTEMS IMPROVEMENT
Document Drafted
Adults: Mar Jun 1994
Peds: May Aug 1993
First Edition
Jun 1998
Second Edition
Jul 1999
Third Edition
Jul 2000
Fourth Edition
Jul 2001
Fifth Edition
Jul 2002
Sixth Edition
Jun 2003
Seventh Edition
Begins April 2005
Supporting Evidence:
Diagnosis and Outpatient Management of Asthma
Original Work Group Members
Shirley Nordahl, PNP
Nursing
Allina North
Jane Norstrom
Health Education
Institute for Research &
Education HealthSystem
Minnesota
Michael Rethwill, MD
Family Practice
HealthPartners
Hyacinth Roberts
Buyers Health Care Action
Group Representative
Honeywell
Kent duRivage, MD
Pediatrics
HealthPartners
Jane Gendron
Measurement Advisor
ICSI
Keith Harmon, MD
Pulmonary Medicine
HealthSystem Minnesota
James Li, MD
Allergy, Work Group Leader
Mayo Clinic
William Schoenwetter, MD
Allergy
HealthSystem Minnesota
Richard Sveum, MD
Allergy
HealthSystem Minnesota
Eunice Weslander, PA-C
Family Practice
Central MN Group Health
Margaret White, RN, MS
Facilitator
ICSI
Institute for Clinical Systems Improvement
www.icsi.org
28
I. CLASSES OF RESEARCH REPORTS
A. Primary Reports of New Data Collection:
Class A: Randomized, controlled trial
Class B: Cohort study
Class C: Non-randomized trial with concurrent or historical controls
Case-control study
Study of sensitivity and specicity of a diagnostic test
Population-based descriptive study
Class D: Cross-sectional study
Case series
Case report
B. Reports that Synthesize or Reect upon Collections of Primary Reports:
Class M: Meta-analysis
Systematic review
Decision analysis
Cost-effectiveness analysis
Class R: Consensus statement
Consensus report
Narrative review
Class X: Medical opinion
II. CONCLUSION GRADES
Key conclusions (as determined by the work group) are supported by a conclusion grading worksheet that
summarizes the important studies pertaining to the conclusion. Individual studies are classed according
to the system dened in Section I, above, and are assigned a designator of +, -, or to reect the study
quality. Conclusion grades are determined by the work group based on the following denitions:
Grade I: The evidence consists of results from studies of strong design for answering the question
addressed. The results are both clinically important and consistent with minor exceptions at most. The
results are free of any signicant doubts about generalizability, bias, and aws in research design. Studies
with negative results have sufciently large samples to have adequate statistical power.
Grade II: The evidence consists of results from studies of strong design for answering the question
addressed, but there is some uncertainty attached to the conclusion because of inconsistencies among the
results from the studies or because of minor doubts about generalizability, bias, research design aws,
or adequacy of sample size. Alternatively, the evidence consists solely of results from weaker designs
for the question addressed, but the results have been conrmed in separate studies and are consistent
with minor exceptions at most.
Grade III: The evidence consists of results from studies of strong design for answering the question
addressed, but there is substantial uncertainty attached to the conclusion because of inconsistencies
among the results from different studies or because of serious doubts about generalizability, bias, research
design aws, or adequacy of sample size. Alternatively, the evidence consists solely of results from a
limited number of studies of weak design for answering the question addressed.
Evidence Grading System
Diagnosis and Outpatient Management of Asthma
Seventh Edition/March 2005
Institute for Clinical Systems Improvement
www.icsi.org
29
Grade Not Assignable: There is no evidence available that directly supports or refutes the
conclusion.
The symbols +, , , and N/A found on the conclusion grading worksheets are used to designate the quality
of the primary research reports and systematic reviews:
+ indicates that the report or review has clearly addressed issues of inclusion/exclusion, bias, generaliz-
ability, and data collection and analysis;
indicates that these issues have not been adequately addressed;
indicates that the report or review is neither exceptionally strong or exceptionally weak;
N/A indicates that the report is not a primary reference or a systematic review and therefore the quality has
not been assessed.
Diagnosis and Outpatient Management of Asthma
Evidence Grading System Seventh Edition/March 2005
Institute for Clinical Systems Improvement
www.icsi.org
30
References
American Thoracic Society. Lung function testing: selection of reference values and interpretive strate-
gies. Am Rev Respir Dis 1991;144:1202-18. (Class R)
Blanc P. Occupational asthma in a national disability survey. Chest 1987;92:613-17. (Class C)
Bleecker ER, Welch MJ, Weinstein SF, et al. Low-dose inhaled uticasone propionate versus oral zar-
lukast in the treatment of persistent asthma. J Allergy Clin Immunol 2000;105:1123-29. (Class A)
Chapman KR, Verbeek PR, White JG, et al. Effect of a short course of prednisone in the prevention of
early relapse after the emergency room treatment of acute asthma. N Eng J Med 1991;324:788-94.
(Class A)
Childhood Asthma Management Program Research Group, The. Long-term effects of budesonide or
nedocromil in children with asthma. N Engl J Med 2000;343:1054-63. (Class A)
Connolly MJ, Crowley JJ, Charan NB, et al. Reduced subjective awareness of bronchoconstriction
provoked by methacholine in elderly asthmatic and normal subjects as measured on a simple aware-
ness scale. Thorax 1992;47:410-13. (Class C)
Corren J, Adinoff AD, Irvin CG. Changes in bronchial responsiveness following nasal provocation with
allergen. J Allergy Clin Immunol 1992;89:611-18. (Class A)
Ducharme FM, Hicks GC. Anti-leukotriene agents compared to inhaled corticosteroids in the manage-
ment of recurrent and/or chronic asthma in adults and children. Cochrane Database Syst Rev. 2002.
(Class M)
Enright PL, Lebowitz MD, Cockroft DW. Physiologic measures: pulmonary function tests. Am J Respir
Crit Care Med 1994;149:S9-S18. (Class R)
Fanta CH, Rossing TH, McFadden ER. Glucocorticoids in acute asthma: a critical controlled trial. Am
J Med 1983;74:845-51. (Class A)
Gibson PG, Coughlan J, Wilson AJ, et al. Self-management education and regular practitioner review
for adults with asthma. The Cochrane Library, 2:2000. (Class M)
Harper PC, Bergner A, Kaye MD. Antireux treatment for asthma: improvement in patients with associ-
ated gastroesophageal reux. Arch Intern Med 1987;147:56-60. (Class D)
Harris JB, Weinberger MM, Nassif E, et al. Early intervention with short course prednisone to prevent
progression of asthma in ambulatory patients incompletely responsive to bronchodilators. J Pediatr
1987;110:627-33. (Class A)
Ignatio-Garcia J, Gonzalez-Santos P. Asthma self-management education program by home monitoring
of peak ow expiratory ow. Am J Respir Care Med 1995;151:353-59. (Class A)
Juniper EF, Guyatt GH, Epstein RS, et al. Evaluation of impairment of health related quality of life in
asthma: development of a questionnaire for use in clinical trials. Thorax 1992;47:76-83. (Class D)
Juniper EF, Guyatt GH, Ferrie PJ, Grifth LE. Measuring quality of life in asthma. Am Rev Respir Dis
1993;147:832-38. (Class D)
Kikuchi Y, Okabe S, Tamura G, et al. Chemosensitivity and perception of dyspnea in patients with a
history of near-fatal asthma. N Engl J Med 1994;330:1329-34. (Class C)
Lahdensuo A, Haahtela T, Herrala J, et al. Randomised comparison of guided self-management and
traditional treatment of asthma over one year. BMJ 1996;312:748-52. (Class A)
Diagnosis and Outpatient Management of Asthma
Seventh Edition/March 2005
Institute for Clinical Systems Improvement
www.icsi.org
31
Lung Health Study Research Group, The. Effect of inhaled triamcinolone on the decline in pulmonary
function in chronic obstructive pulmonary disease. N Engl J Med 2000;343:1902-09. (Class A)
Malo JL, Ghezzo H, D'Aquino C, et al. Natural history of occupational asthma: relevance of type of
agent and other factors in the rate of development of symptoms in affected subjects. J Allergy Clin
Immunol 1992;90:937-44. (Class C)
Miles JF, Bright P, Ayres JG, et al. The performance of mini Wright peak ow meters after prolonged
use. Resp Med 1995;89:603-05. (Class C)
NAEPP Expert Panel Report. Managing asthma during pregnancy: recommendations for pharmacologic
treatment 2004 update. J Allergy Clin Immunol 2005;115:34-46. (Class R)
National Asthma Education and Prevention Program Expert Panel Report 2. Guidelines for the Diag-
nosis and Outpatient Management of Asthma. Publication # 97-4051. National Institutes of Health/
National Heart, Lung, and Blood Institute, April 1997. (Class R)
National Asthma Education and Prevention Program Expert Panel Report: Guidelines for the Diagnosis
and Outpatient Management of Asthma. Update on Selected Topics 2002. J Allergy Clin Immunol
2002;110:S141-S219. (Class M)
O'Hollaren MT, Yunginger JW, Offord KP, et al. Exposure to an aeroallergen as a possible precipitating
factor in respiratory arrest in young patients with asthma. N Engl J Med 1991;324:359-63. (Class D)
Pollart SM, Reid MJ, Fling JA, et al. Epidemiology of emergency room asthma in northern California:
association with IgE antibody to ryegrass pollen. J Allergy Clin Immunol 1988;82:224-30. (Class C)
Rachelefsky GS, Katz RM, Siegel SC. Chronic sinus disease with associated reactive airway disease
in children. Pediatrics 1984;73:526-29. (Class D)
Scarfone RJ, Fuchs SM, Nager AL, et al. Controlled trial of oral prednisone in the emergency depart-
ment treatment of children with acute asthma. Pediatrics 1993;2:513-18. (Class A)
Spitzer WO, Suissa S, Ernst P, et al. The use of beta-agonists and the risk of death and near death
from asthma. N Engl J Med 1992;326:501-06. (Class C)
Szeer SJ, Phillips BR, Martinez FD, et al. Characterization of within-subject responses to uticasone
and montelukast in childhood asthma. J Allergy Clin Immunol 2005;115:233-42. (Class A)
Zieger RS, Heller S, Mellon MH, et al. Facilitated referral to asthma specialist reduces relapses in
asthma emergency room visits. J Allergy Clin Immunol 1991;87:1160-68. (Class C)
Diagnosis and Outpatient Management of Asthma
References Seventh Edition/March 2005
Institute for Clinical Systems Improvement
www.icsi.org
32
Conclusion Grading Worksheet Appendix A
Annotation #8 (Leukotriene Receptor Antagonists [LTRAs])
Diagnosis and Outpatient Management of Asthma
Seventh Edition/March 2005
W
o
r
k
G
r
o
u
p
'
s
C
o
n
c
l
u
s
i
o
n
:
B
a
s
e
d
o
n
d
a
t
a
c
o
m
p
a
r
i
n
g
L
T
R
A
s
t
o
i
n
h
a
l
e
d
c
o
r
t
i
c
o
s
t
e
r
o
i
d
s
,
i
n
h
a
l
e
d
c
o
r
t
i
c
o
s
t
e
r
o
i
d
s
a
r
e
t
h
e
p
r
e
-
f
e
r
r
e
d
t
r
e
a
t
m
e
n
t
o
p
t
i
o
n
f
o
r
m
i
l
d
p
e
r
s
i
s
t
e
n
t
a
s
t
h
m
a
i
n
a
d
u
l
t
s
,
a
n
d
b
y
e
x
t
r
a
p
o
l
a
t
i
o
n
u
n
t
i
l
p
u
b
l
i
s
h
e
d
d
a
t
a
b
e
c
o
m
e
a
v
a
i
l
a
b
l
e
,
f
o
r
c
h
i
l
d
r
e
n
.
L
T
R
A
s
a
r
e
a
n
a
l
t
e
r
n
a
t
i
v
e
a
l
t
h
o
u
g
h
n
o
t
p
r
e
f
e
r
r
e
d
t
r
e
a
t
m
e
n
t
.
C
o
n
c
l
u
s
i
o
n
G
r
a
d
e
:
I
A
u
t
h
o
r
/
Y
e
a
r
D
e
s
i
g
n
T
y
p
e
C
l
a
s
s
Q
u
a
l
-
i
t
y
+
,
P
o
p
u
l
a
t
i
o
n
S
t
u
d
i
e
d
/
S
a
m
p
l
e
S
i
z
e
P
r
i
m
a
r
y
O
u
t
c
o
m
e
M
e
a
s
u
r
e
(
s
)
/
R
e
s
u
l
t
s
(
e
.
g
.
,
p
-
v
a
l
u
e
,
c
o
n
f
i
d
e
n
c
e
i
n
t
e
r
v
a
l
,
r
e
l
a
t
i
v
e
r
i
s
k
,
o
d
d
s
r
a
t
i
o
,
l
i
k
e
l
i
-
h
o
o
d
r
a
t
i
o
,
n
u
m
b
e
r
n
e
e
d
e
d
t
o
t
r
e
a
t
)
A
u
t
h
o
r
s
'
C
o
n
c
l
u
s
i
o
n
s
/
W
o
r
k
G
r
o
u
p
'
s
C
o
m
m
e
n
t
s
(
i
t
a
l
i
c
i
z
e
d
)
M
a
l
m
s
t
r
o
m
e
t
a
l
.
,
1
9
9
9
R
C
T
A
-
A
g
e
s
1
5
y
r
s
a
n
d
o
l
d
e
r
;
m
a
l
e
s
a
n
d
f
e
m
a
l
e
s
;
h
e
a
l
t
h
y
,
n
o
n
s
m
o
k
-
i
n
g
;
a
s
t
h
m
a
f
o
r
1
y
r
;
F
E
V
1
5
0
-
8
5
%
o
f
p
r
e
d
i
c
t
e
d
;
i
n
c
r
e
a
s
e
o
f
1
5
%
i
n
a
b
s
o
l
u
t
e
F
E
V
1
a
f
t
e
r
u
s
e
o
f
i
n
h
a
l
e
d
-
a
g
o
n
i
s
t
(
a
t
l
e
a
s
t
2
o
f
3
v
i
s
i
t
s
)
;
d
a
y
t
i
m
e
a
s
t
h
m
a
s
y
m
p
t
o
m
s
c
o
r
e
6
4
(
o
f
3
3
6
p
o
s
s
i
b
l
e
)
;
a
v
e
r
a
g
e
d
a
i
l
y
u
s
e
o
f
1
p
u
f
f
o
f
s
h
o
r
t
-
a
c
t
i
n
g
-
a
g
o
n
i
s
t
-
E
x
c
l
u
d
e
d
:
u
s
e
o
f
i
n
h
a
l
e
d
a
n
d
o
r
a
l
c
o
r
t
i
c
o
s
t
e
r
o
i
d
s
,
c
r
o
m
o
l
y
n
,
o
r
n
e
d
o
c
r
o
m
i
l
w
i
t
h
i
n
4
w
k
s
b
e
-
f
o
r
e
i
n
i
t
i
a
l
e
v
a
l
;
u
s
e
o
f
l
o
n
g
-
a
c
t
i
n
g
-
a
g
o
n
i
s
t
s
,
a
n
t
i
m
u
s
c
a
r
i
n
-
i
c
s
,
o
r
t
h
e
o
p
h
y
l
l
i
n
e
w
i
t
h
i
n
2
w
k
s
b
e
f
o
r
e
i
n
i
t
i
a
l
e
v
a
l
;
h
a
d
u
s
e
d
l
o
n
g
-
a
c
t
i
n
g
a
n
t
i
h
i
s
t
a
m
i
n
e
s
-
2
w
k
p
l
a
c
e
b
o
r
u
n
-
i
n
,
1
2
w
k
t
r
e
a
t
m
e
n
t
p
e
r
i
o
d
,
3
w
k
w
a
s
h
o
u
t
-
R
a
n
d
o
m
i
z
e
d
t
o
m
o
n
t
e
l
u
k
a
s
t
(
1
0
m
g
1
X
/
d
a
y
[
e
v
e
n
i
n
g
]
)
,
i
n
-
h
a
l
e
d
b
e
c
l
o
m
e
t
h
a
s
o
n
e
(
2
0
0
g
2
X
/
d
a
y
)
,
o
r
p
l
a
c
e
b
o
(
3
:
2
:
2
r
a
t
i
o
)
-
C
l
i
n
i
c
:
F
E
V
1
-
H
o
m
e
:
d
a
i
l
y
d
i
a
r
y
c
a
r
d
f
o
r
s
y
m
p
t
o
m
s
,
P
E
F
R
,
a
n
d
n
e
e
d
f
o
r
s
a
l
b
u
t
a
m
o
l
-
8
9
5
p
a
t
i
e
n
t
s
r
a
n
d
o
m
i
z
e
d
(
3
8
7
m
o
n
t
e
l
u
k
a
s
t
,
2
5
1
b
e
-
c
l
o
m
e
t
h
a
s
o
n
e
,
2
5
7
p
l
a
c
e
b
o
)
;
t
r
e
a
t
m
e
n
t
c
o
m
p
l
e
t
e
d
b
y
9
1
.
5
%
,
9
2
.
8
%
,
a
n
d
8
3
.
7
%
,
r
e
s
p
e
c
t
i
v
e
l
y
;
t
o
t
a
l
s
t
u
d
y
c
o
m
p
l
e
t
e
d
b
y
8
9
.
4
%
,
9
0
.
4
%
,
a
n
d
8
1
.
7
%
-
G
r
o
u
p
s
s
i
m
i
l
a
r
a
t
b
a
s
e
l
i
n
e
;
m
e
a
n
c
o
m
p
l
i
a
n
c
e
w
i
t
h
i
n
h
a
l
e
d
m
e
d
i
c
a
t
i
o
n
(
t
r
e
a
t
m
e
n
t
p
h
a
s
e
)
8
8
%
-
9
0
%
f
o
r
a
l
l
g
r
o
u
p
s
;
m
e
a
n
c
o
m
p
l
i
a
n
c
e
w
i
t
h
o
r
a
l
m
e
d
i
c
a
t
i
o
n
>
9
9
%
f
o
r
a
l
l
g
r
o
u
p
s
-
O
u
t
c
o
m
e
s
:P
l
a
c
e
b
o
M
o
n
t
e
l
u
k
a
s
t
B
e
c
l
o
m
e
t
h
a
s
o
n
e
F
E
V
1
*
0
.
7
%
7
.
4
%
a
1
3
.
1
%
a
S
y
m
p
t
o
m
-
0
.
1
7
-
0
.
4
1
a
-
0
.
6
2
a
S
c
o
r
e
#
P
E
F
R
-
a
m
0
.
8
l
/
m
i
n
2
3
.
8
l
/
m
i
n
a
3
9
.
2
l
/
m
i
n
a
P
E
F
R
-
p
m
0
.
3
l
/
m
i
n
2
0
.
8
l
/
m
i
n
a
3
2
.
1
l
/
m
i
n
a
A
t
t
a
c
k
s
^
2
7
.
3
%
1
5
.
6
%
a
1
0
.
1
%
a
a
p
<
0
.
0
0
1
c
o
m
p
a
r
e
d
w
i
t
h
p
l
a
c
e
b
o
;
*
m
o
r
n
i
n
g
v
a
l
u
e
,
%
c
h
a
n
g
e
f
r
o
m
b
a
s
e
l
i
n
e
;
#
d
a
y
t
i
m
e
s
c
o
r
e
,
c
h
a
n
g
e
f
r
o
m
b
a
s
e
l
i
n
e
;
^
p
e
r
c
e
n
t
a
g
e
o
f
p
a
t
i
e
n
t
s
-
D
u
r
i
n
g
3
w
k
w
a
s
h
o
u
t
,
p
a
t
i
e
n
t
s
s
w
i
t
c
h
e
d
t
o
p
l
a
c
e
b
o
r
e
t
u
r
n
e
d
t
o
b
a
s
e
l
i
n
e
l
e
v
e
l
s
-
I
n
i
t
i
a
l
r
e
s
p
o
n
s
e
g
r
e
a
t
e
r
f
o
r
m
o
n
t
e
l
u
k
a
s
t
g
r
o
u
p
;
e
f
f
e
c
t
o
f
b
e
c
l
o
m
e
t
h
a
s
o
n
e
s
u
r
p
a
s
s
e
d
m
o
n
t
e
l
u
k
a
s
t
7
-
1
0
d
a
y
s
a
f
t
e
r
s
t
a
r
t
o
f
t
h
e
r
a
p
y
-
N
o
i
n
t
e
r
a
c
t
i
o
n
s
b
a
s
e
d
o
n
b
a
s
e
l
i
n
e
F
E
V
1
,
s
y
m
p
t
o
m
s
c
o
r
e
,
n
e
e
d
f
o
r
-
a
g
o
n
i
s
t
,
o
r
P
E
F
R
-
I
m
p
r
o
v
e
m
e
n
t
s
i
n
q
u
a
l
i
t
y
o
f
l
i
f
e
g
r
e
a
t
e
r
w
i
t
h
m
o
n
t
e
-
l
u
k
a
s
t
a
n
d
b
e
c
l
o
m
e
t
h
a
s
o
n
e
(
p
<
0
.
0
0
1
)
-
M
o
s
t
c
o
m
m
o
n
c
l
i
n
i
c
a
l
a
d
v
e
r
s
e
e
f
f
e
c
t
s
:
w
o
r
s
e
n
i
n
g
a
s
t
h
m
a
(
p
<
0
.
0
5
f
o
r
a
c
t
i
v
e
t
r
e
a
t
m
e
n
t
v
s
.
p
l
a
c
e
b
o
)
,
h
e
a
d
a
c
h
e
,
u
p
p
e
r
r
e
s
p
i
r
a
t
o
r
y
i
n
f
e
c
t
i
o
n
(
b
o
t
h
N
S
)
-
O
r
a
l
m
o
n
t
e
l
u
k
a
s
t
t
h
e
r
a
p
y
h
a
s
b
e
e
n
s
h
o
w
n
t
o
b
e
e
f
f
e
c
t
i
v
e
i
n
c
h
r
o
n
i
c
a
s
t
h
m
a
,
p
r
o
d
u
c
i
n
g
s
i
g
n
i
f
i
c
a
n
t
i
m
p
r
o
v
e
m
e
n
t
s
i
n
F
E
V
1
a
n
d
s
i
g
-
n
i
f
i
c
a
n
t
a
l
l
e
v
i
a
t
i
o
n
o
f
d
a
y
t
i
m
e
a
s
t
h
m
a
s
y
m
p
-
t
o
m
s
.
A
l
t
h
o
u
g
h
i
n
h
a
l
e
d
b
e
c
l
o
m
e
t
h
a
s
o
n
e
h
a
d
a
l
a
r
g
e
r
a
v
e
r
a
g
e
e
f
f
e
c
t
t
h
a
n
m
o
n
t
e
l
u
k
a
s
t
,
m
o
n
t
e
l
u
k
a
s
t
h
a
d
a
m
o
r
e
r
a
p
i
d
i
n
i
t
i
a
l
r
e
-
s
p
o
n
s
e
.
T
h
e
t
w
o
a
g
e
n
t
s
e
a
c
h
p
r
o
t
e
c
t
e
d
a
g
a
i
n
s
t
w
o
r
s
e
n
i
n
g
e
p
i
s
o
d
e
s
o
f
a
s
t
h
m
a
.
N
O
T
E
S
:
u
s
e
o
f
i
m
m
u
n
o
t
h
e
r
a
p
y
w
a
s
p
e
r
m
i
t
-
t
e
d
i
f
i
t
h
a
d
b
e
e
n
s
t
a
r
t
e
d
6
m
o
s
b
e
f
o
r
e
i
n
i
-
t
i
a
l
e
v
a
l
u
a
t
i
o
n
;
r
u
n
-
i
n
w
a
s
s
i
n
g
l
e
-
b
l
i
n
d
,
t
r
e
a
t
m
e
n
t
a
n
d
w
a
s
h
o
u
t
w
a
s
d
o
u
b
l
e
-
b
l
i
n
d
;
d
u
r
i
n
g
w
a
s
h
o
u
t
s
o
m
e
p
a
t
i
e
n
t
s
c
o
n
t
i
n
u
e
d
a
c
-
t
i
v
e
t
r
e
a
t
m
e
n
t
a
n
d
o
t
h
e
r
s
s
w
i
t
c
h
e
d
t
o
p
l
a
-
c
e
b
o
;
s
t
u
d
y
d
o
n
e
a
t
3
6
c
e
n
t
e
r
s
i
n
1
9
c
o
u
n
-
t
r
i
e
s
;
p
a
t
i
e
n
t
s
c
o
u
l
d
u
s
e
s
h
o
r
t
-
a
c
t
i
n
g
i
n
h
a
l
e
d
-
a
g
o
n
i
s
t
(
s
a
l
b
u
t
a
m
o
l
)
a
s
n
e
e
d
e
d
;
i
f
a
d
d
i
-
t
i
o
n
a
l
t
h
e
r
a
p
y
w
a
s
n
e
e
d
e
d
o
r
a
l
c
o
r
t
i
c
o
s
t
e
r
-
o
i
d
s
w
e
r
e
g
i
v
e
n
(
i
f
2
s
u
c
h
e
p
i
s
o
d
e
p
a
t
i
e
n
t
w
a
s
d
r
o
p
p
e
d
f
r
o
m
s
t
u
d
y
)
;
c
o
m
p
l
i
a
n
c
e
m
o
n
i
-
t
o
r
e
d
b
y
w
e
i
g
h
i
n
g
i
n
h
a
l
e
r
s
a
n
d
c
o
u
n
t
i
n
g
t
a
b
-
l
e
t
s
;
a
n
a
l
y
s
i
s
i
n
c
l
u
d
e
d
a
l
l
p
a
t
i
e
n
t
s
w
i
t
h
b
a
s
e
-
l
i
n
e
a
n
d
a
t
l
e
a
s
t
o
n
e
m
e
a
s
u
r
e
m
e
n
t
a
f
t
e
r
r
a
n
-
d
o
m
i
z
a
t
i
o
n
;
d
i
d
s
a
m
p
l
e
s
i
z
e
e
s
t
i
m
a
t
i
o
n
f
o
r
9
5
%
p
o
w
e
r
t
o
d
e
t
e
c
t
d
i
f
f
e
r
e
n
c
e
o
f
6
%
i
n
c
h
a
n
g
e
f
r
o
m
b
a
s
e
l
i
n
e
a
n
d
1
0
%
i
n
d
a
y
t
i
m
e
s
y
m
p
t
o
m
s
c
o
r
e
s
(
m
o
n
t
e
l
u
k
a
s
t
v
s
.
p
l
a
c
e
b
o
)
Institute for Clinical Systems Improvement
www.icsi.org
33
Conclusion Grading Worksheet Appendix A Diagnosis and Outpatient Management of Asthma
Annotation #8 (Leukotriene Receptor Antagonists [LTRAs]) Seventh Edition/March 2005
B
l
e
e
k
e
r
e
t
a
l
.
,
2
0
0
0
R
C
T
A
-
A
g
e
s
1
2
+
;
p
e
r
s
i
s
t
e
n
t
a
s
t
h
m
a
(
6
m
o
s
)
;
p
r
e
d
o
s
e
F
E
V
1
o
f
5
0
-
8
0
%
o
f
p
r
e
d
i
c
t
e
d
n
o
r
m
a
l
a
n
d
i
n
-
c
r
e
a
s
e
F
E
V
1
1
2
%
f
r
o
m
b
a
s
e
l
i
n
e
a
f
t
e
r
1
8
0
g
i
n
h
a
l
e
d
a
l
b
u
t
e
r
o
l
;
h
a
d
u
s
e
d
a
l
b
u
t
e
r
o
l
o
n
s
c
h
e
d
u
l
e
o
r
a
s
-
n
e
e
d
e
d
b
a
s
e
s
d
u
r
i
n
g
4
w
k
s
b
e
f
o
r
e
s
c
r
e
e
n
i
n
g
;
n
o
m
o
n
t
e
l
u
-
k
a
s
t
,
z
a
f
i
r
l
u
k
a
s
t
,
o
r
z
i
l
e
u
t
o
n
w
i
t
h
i
n
2
w
k
s
o
f
s
c
r
e
e
n
i
n
g
-
E
x
c
l
u
d
e
d
:
h
i
s
t
o
r
y
o
f
l
i
f
e
-
t
h
r
e
a
t
e
n
i
n
g
a
s
t
h
m
a
;
>
3
b
u
r
s
t
s
o
f
o
r
a
l
o
r
p
a
r
e
n
t
e
r
a
l
c
o
r
t
i
c
o
s
t
e
r
o
i
d
s
w
i
t
h
i
n
1
y
r
;
u
s
e
o
f
t
o
b
a
c
c
o
p
r
o
d
u
c
t
s
i
n
p
a
s
t
y
r
o
r
s
m
o
k
i
n
g
h
i
s
t
o
r
y
o
f
>
1
0
p
a
c
k
-
y
r
s
;
r
e
s
p
i
r
a
-
t
o
r
y
i
n
f
e
c
t
i
o
n
w
i
t
h
i
n
2
w
k
s
o
f
s
c
r
e
e
n
i
n
g
,
c
u
r
r
e
n
t
e
v
i
d
e
n
c
e
o
f
s
i
g
n
i
f
i
c
a
n
t
d
i
s
o
r
d
e
r
s
-
8
-
1
4
d
a
y
r
u
n
-
i
n
w
i
t
h
r
e
s
c
u
e
a
l
-
b
u
t
e
r
o
l
(
b
a
s
e
l
i
n
e
d
a
t
a
,
c
o
m
p
l
i
-
a
n
c
e
a
s
s
e
s
s
m
e
n
t
)
-
E
l
i
g
i
b
l
e
p
a
t
i
e
n
t
s
r
a
n
d
o
m
i
z
e
d
t
o
i
n
h
a
l
e
d
f
l
u
t
i
c
a
s
o
n
e
p
r
o
p
i
o
n
a
t
e
(
F
P
)
a
e
r
o
s
o
l
(
8
8
g
)
o
r
o
r
a
l
z
a
f
i
r
-
l
u
k
a
s
t
(
2
0
m
g
)
;
b
o
t
h
2
X
/
d
a
y
f
o
r
1
2
w
k
s
w
i
t
h
a
l
b
u
t
e
r
o
l
a
s
n
e
e
d
e
d
-
H
o
m
e
:
s
y
m
p
t
o
m
s
,
P
E
F
R
,
a
l
-
b
u
t
e
r
o
l
u
s
e
-
C
l
i
n
i
c
:
F
E
V
1
-
2
2
0
r
a
n
d
o
m
i
z
e
d
t
o
z
a
f
i
r
l
u
k
a
s
t
,
2
3
1
t
o
F
P
;
g
r
o
u
p
s
s
i
m
i
l
a
r
a
t
b
a
s
e
l
i
n
e
;
7
7
%
o
f
z
a
f
i
r
l
u
k
a
s
t
a
n
d
8
7
%
o
f
p
l
a
c
e
b
o
g
r
o
u
p
s
f
i
n
i
s
h
e
d
p
r
o
t
o
c
o
l
-
O
u
t
c
o
m
e
s
(
c
h
a
n
g
e
a
f
t
e
r
1
2
w
k
s
o
f
t
r
e
a
t
m
e
n
t
)
:
F
P
Z
a
f
i
r
l
u
k
a
s
t
F
E
V
1
-
a
m
(
L
)
+
0
.
4
2
+
0
.
2
0
*
P
E
F
R
-
a
m
(
L
/
m
i
n
)
+
4
9
.
9
4
+
1
1
.
6
8
*
P
E
F
R
-
p
m
(
L
/
m
i
n
)
+
3
8
.
9
1
+
1
0
.
5
0
*
S
y
m
p
t
o
m
s
c
o
r
e
-
0
.
4
6
-
0
.
1
9
*
S
y
m
p
t
o
m
-
f
r
e
e
d
a
y
s
(
%
)
+
2
8
.
5
+
1
5
.
6
*
A
l
b
u
t
e
r
o
l
(
p
u
f
f
s
/
d
a
y
)
-
2
.
3
9
-
1
.
4
5
*
R
e
s
c
u
e
-
f
r
e
e
d
a
y
s
+
4
0
.
4
+
2
4
.
2
*
#
N
i
g
h
t
a
w
a
k
e
n
i
n
g
s
-
0
.
2
8
-
0
.
1
5
*
*
p
<
0
.
0
0
1
-
5
6
%
o
f
p
h
y
s
i
c
i
a
n
s
r
a
t
e
d
t
r
e
a
t
m
e
n
t
w
i
t
h
F
P
a
s
"
e
f
-
f
e
c
t
i
v
e
"
o
r
"
v
e
r
y
e
f
f
e
c
t
i
v
e
"
c
o
m
p
a
r
e
d
w
i
t
h
4
1
%
f
o
r
z
a
f
i
r
l
u
k
a
s
t
(
p
<
0
.
0
0
1
)
-
4
%
o
f
F
P
g
r
o
u
p
a
n
d
6
%
o
f
z
a
f
i
r
l
u
k
a
s
t
g
r
o
u
p
h
a
d
a
n
e
x
a
c
e
r
b
a
t
i
o
n
(
N
S
)
-
1
0
%
i
n
e
a
c
h
g
r
o
u
p
h
a
d
1
a
d
v
e
r
s
e
e
v
e
n
t
c
o
n
s
i
d
e
r
e
d
p
o
t
e
n
t
i
a
l
l
y
r
e
l
a
t
e
d
t
o
t
r
e
a
t
m
e
n
t
;
h
e
a
d
a
c
h
e
,
d
r
y
m
o
u
t
h
,
&
h
o
a
r
s
e
n
e
s
s
w
e
r
e
m
o
s
t
c
o
m
m
o
n
-
T
h
e
c
l
i
n
i
c
a
l
e
f
f
e
c
t
i
v
e
n
e
s
s
o
f
a
l
o
w
d
o
s
e
o
f
F
P
a
s
f
i
r
s
t
-
l
i
n
e
t
h
e
r
a
p
y
i
n
p
a
t
i
e
n
t
s
w
i
t
h
p
e
r
-
s
i
s
t
e
n
t
a
s
t
h
m
a
w
h
o
a
r
e
s
y
m
p
t
o
m
a
t
i
c
o
n
2
-
a
g
o
n
i
s
t
s
a
l
o
n
e
i
s
s
u
p
e
r
i
o
r
t
o
t
h
a
t
o
f
z
a
f
i
r
l
u
-
k
a
s
t
.
N
O
T
E
S
:
c
o
n
c
u
r
r
e
n
t
u
s
e
o
f
m
e
d
i
c
a
t
i
o
n
s
t
h
a
t
m
i
g
h
t
a
f
f
e
c
t
t
h
e
c
o
u
r
s
e
o
f
a
s
t
h
m
a
o
r
i
n
t
e
r
a
c
t
w
i
t
h
z
a
f
i
r
l
u
k
a
s
t
w
e
r
e
p
r
o
h
i
b
i
t
e
d
;
a
n
t
i
h
i
s
t
a
-
m
i
n
e
s
,
d
e
c
o
n
g
e
s
t
a
n
t
s
,
a
n
d
i
n
t
r
a
n
a
s
a
l
m
e
d
i
c
a
-
t
i
o
n
s
f
o
r
a
l
l
e
r
g
i
c
r
h
i
n
i
t
i
s
w
e
r
e
a
l
l
o
w
e
d
;
d
o
u
-
b
l
e
-
b
l
i
n
d
t
r
e
a
t
m
e
n
t
p
h
a
s
e
;
p
a
t
i
e
n
t
s
w
i
t
h
a
s
t
h
m
a
e
x
a
c
e
r
b
a
t
i
o
n
(
r
e
q
u
i
r
i
n
g
c
o
r
t
i
c
o
s
t
e
r
-
o
i
d
s
)
d
u
r
i
n
g
s
t
u
d
y
p
h
a
s
e
w
e
r
e
w
i
t
h
d
r
a
w
n
;
s
t
u
d
y
d
e
s
i
g
n
e
d
w
i
t
h
8
0
%
p
o
w
e
r
t
o
d
e
t
e
c
t
d
i
f
f
e
r
e
n
c
e
o
f
0
.
1
7
8
L
/
m
i
n
i
n
F
E
V
1
b
e
t
w
e
e
n
g
r
o
u
p
s
Institute for Clinical Systems Improvement
www.icsi.org
34
B
u
s
s
e
e
t
a
l
.
f
o
r
t
h
e
F
l
u
t
i
c
a
s
o
n
e
P
r
o
p
i
o
n
a
t
e
C
l
i
n
i
c
a
l
R
e
-
s
e
a
r
c
h
S
t
u
d
y
,
2
0
0
1
R
C
T
A
-
A
g
e
s
1
5
+
;
a
s
t
h
m
a
d
i
a
g
n
o
s
e
d
f
o
r
6
m
o
s
;
p
r
e
d
o
s
e
F
E
V
1
5
0
-
8
0
%
o
f
p
r
e
d
i
c
t
e
d
n
o
r
m
a
l
a
n
d
i
n
-
c
r
e
a
s
e
i
n
F
E
V
1
o
f
1
5
%
a
f
t
e
r
1
8
0
g
a
l
b
u
t
e
r
o
l
;
u
s
e
d
i
n
h
a
l
e
d
o
r
o
r
a
l
s
h
o
r
t
-
a
c
t
i
n
g
2
-
a
g
o
n
i
s
t
o
n
a
r
e
g
u
l
a
r
o
r
a
s
-
n
e
e
d
e
d
b
a
s
i
s
f
o
r
3
m
o
s
b
e
f
o
r
e
s
c
r
e
e
n
i
n
g
-
E
x
c
l
u
d
e
d
:
u
s
e
o
f
I
C
S
s
i
n
p
a
s
t
2
m
o
s
;
u
s
e
o
f
t
o
b
a
c
c
o
p
r
o
d
u
c
t
s
i
n
p
a
s
t
y
e
a
r
;
s
m
o
k
i
n
g
h
i
s
t
o
r
y
o
f
1
0
p
a
c
k
-
y
r
s
;
h
o
s
p
i
t
a
l
i
z
e
d
f
o
r
a
s
t
h
m
a
i
n
p
a
s
t
3
m
o
s
;
r
e
s
p
i
r
a
-
t
o
r
y
t
r
a
c
t
i
n
f
e
c
t
i
o
n
i
n
p
a
s
t
4
w
k
s
;
h
y
p
e
r
s
e
n
s
i
t
i
v
i
t
y
t
o
a
s
t
h
m
a
d
r
u
g
s
-
8
-
1
4
d
a
y
r
u
n
-
i
n
p
e
r
i
o
d
(
c
o
n
f
i
r
m
e
l
i
g
i
b
i
l
i
t
y
,
b
a
s
e
l
i
n
e
d
a
t
a
)
;
u
s
e
o
f
a
l
b
u
t
e
r
o
l
a
s
n
e
e
d
e
d
-
R
a
n
d
o
m
i
z
e
d
(
s
e
e
N
O
T
E
S
)
t
o
8
8
g
2
X
/
d
a
y
F
P
+
p
l
a
c
e
b
o
c
a
p
-
s
u
l
e
i
n
e
v
e
n
i
n
g
o
r
1
0
m
g
o
r
a
l
m
o
n
t
e
l
u
k
a
s
t
i
n
e
v
e
n
i
n
g
+
2
p
u
f
f
s
p
l
a
c
e
b
o
2
X
/
d
a
y
f
o
r
2
4
w
k
s
;
i
n
h
a
l
e
d
a
l
b
u
t
e
r
o
l
a
s
n
e
e
d
e
d
-
C
l
i
n
i
c
v
i
s
i
t
s
:
F
E
V
1
,
a
d
v
e
r
s
e
e
v
e
n
t
s
;
p
h
y
s
i
c
i
a
n
r
a
t
i
n
g
o
f
e
f
f
e
c
-
t
i
v
e
n
e
s
s
,
q
u
a
l
i
t
y
o
f
l
i
f
e
,
p
a
t
i
e
n
t
s
a
t
i
s
f
a
c
t
i
o
n
w
i
t
h
m
e
d
i
c
a
t
i
o
n
-
H
o
m
e
(
a
m
/
p
m
)
:
s
y
m
p
t
o
m
s
,
P
E
F
R
,
p
u
f
f
s
o
f
a
l
b
u
t
e
r
o
l
,
n
i
g
h
t
-
t
i
m
e
a
w
a
k
e
n
i
n
g
s
,
c
o
m
p
l
i
a
n
c
e
-
2
7
1
i
n
F
P
g
r
o
u
p
,
2
6
2
i
n
m
o
n
t
e
l
u
k
a
s
t
g
r
o
u
p
;
g
r
o
u
p
s
c
o
m
p
a
r
a
b
l
e
a
t
b
a
s
e
l
i
n
e
;
s
t
u
d
y
c
o
m
p
l
e
t
e
d
b
y
7
2
%
o
f
F
P
g
r
o
u
p
a
n
d
7
1
%
o
f
m
o
n
t
e
l
u
k
a
s
t
g
r
o
u
p
;
r
e
p
o
r
t
e
d
c
o
m
p
l
i
a
n
c
e
(
i
n
h
a
l
e
r
a
n
d
c
a
p
s
u
l
e
s
)
9
1
%
-
O
u
t
c
o
m
e
s
(
c
h
a
n
g
e
f
r
o
m
b
a
s
e
l
i
n
e
)
:
F
P
M
o
n
t
e
l
u
k
a
s
t
F
E
V
1
(
L
)
0
.
5
1
0
.
3
3
*
P
E
F
R
-
a
m
(
L
/
m
i
n
)
6
8
.
5
3
4
.
1
*
P
E
F
R
-
p
m
(
L
/
m
i
n
)
5
3
.
9
2
8
.
7
*
S
y
m
p
t
o
m
s
c
o
r
e
-
0
.
8
5
-
0
.
6
0
*
A
l
b
u
t
e
r
o
l
(
p
u
f
f
s
/
d
a
y
)
-
3
.
1
0
-
2
.
3
1
*
*
p
<
0
.
0
0
1
-
P
h
y
s
i
c
i
a
n
s
g
l
o
b
a
l
a
s
s
e
s
s
m
e
n
t
f
a
v
o
r
e
d
F
P
o
v
e
r
m
o
n
-
t
e
l
u
k
a
s
t
(
7
1
%
r
a
t
e
d
F
P
e
f
f
e
c
t
i
v
e
o
r
v
e
r
y
e
f
f
e
c
t
i
v
e
v
s
.
5
3
%
f
o
r
m
o
n
t
e
l
u
k
a
s
t
,
p
<
0
.
0
0
1
)
-
P
a
t
i
e
n
t
s
a
t
i
s
f
a
c
t
i
o
n
f
a
v
o
r
e
d
F
P
o
v
e
r
m
o
n
t
e
l
u
k
a
s
t
(
8
5
%
o
f
p
a
t
i
e
n
t
s
s
a
t
i
s
f
i
e
d
w
i
t
h
F
P
v
s
.
6
5
%
f
o
r
m
o
n
-
t
e
l
u
k
a
s
t
,
p
<
0
.
0
0
1
)
;
q
u
a
l
i
t
y
-
o
f
-
l
i
f
e
s
c
o
r
e
s
s
i
g
n
i
f
i
-
c
a
n
t
l
y
g
r
e
a
t
e
r
i
n
F
P
p
a
t
i
e
n
t
s
(
p
<
0
.
0
0
1
)
e
s
p
e
c
i
a
l
l
y
a
s
t
h
m
a
s
y
m
p
t
o
m
s
a
n
d
e
m
o
t
i
o
n
a
l
f
u
n
c
t
i
o
n
d
o
m
a
i
n
s
-
A
d
v
e
r
s
e
e
v
e
n
t
s
:
7
1
%
o
f
F
P
p
a
t
i
e
n
t
s
,
6
8
%
o
f
m
o
n
-
t
e
l
u
k
a
s
t
p
a
t
i
e
n
t
s
;
f
e
w
w
e
r
e
c
o
n
s
i
d
e
r
e
d
d
r
u
g
r
e
l
a
t
e
d
;
m
o
s
t
c
o
m
m
o
n
(
p
o
s
s
i
b
l
y
d
r
u
g
r
e
l
a
t
e
d
)
w
e
r
e
h
e
a
d
-
a
c
h
e
,
s
o
r
e
t
h
r
o
a
t
,
h
o
a
r
s
e
n
e
s
s
,
o
r
a
l
p
h
a
r
y
n
g
e
a
l
c
a
n
-
d
i
d
i
a
s
i
s
-
A
s
t
h
m
a
e
x
a
c
e
r
b
a
t
i
o
n
s
:
4
%
o
f
F
P
g
r
o
u
p
,
8
%
o
f
m
o
n
t
e
l
u
k
a
s
t
g
r
o
u
p
-
L
o
w
-
d
o
s
e
F
P
i
s
m
o
r
e
e
f
f
e
c
t
i
v
e
t
h
a
n
m
o
n
t
e
-
l
u
k
a
s
t
a
s
f
i
r
s
t
-
l
i
n
e
m
a
i
n
t
e
n
a
n
c
e
t
h
e
r
a
p
y
f
o
r
p
a
t
i
e
n
t
s
w
i
t
h
p
e
r
s
i
s
t
e
n
t
a
s
t
h
m
a
w
h
o
a
r
e
u
n
-
d
e
r
r
a
t
e
d
a
n
d
r
e
m
a
i
n
s
y
m
p
t
o
m
a
t
i
c
w
h
i
l
e
t
a
k
-
i
n
g
s
h
o
r
t
-
a
c
t
i
n
g
2
-
a
g
o
n
i
s
t
s
a
l
o
n
e
.
N
O
T
E
S
:
a
t
r
a
n
d
o
m
i
z
a
t
i
o
n
p
a
t
i
e
n
t
s
h
a
d
t
o
d
e
m
o
n
s
t
r
a
t
e
t
h
a
t
a
d
d
i
t
i
o
n
a
l
t
h
e
r
a
p
y
w
a
s
w
a
r
-
r
a
n
t
e
d
(
u
n
m
e
d
i
c
a
t
e
d
F
E
V
1
o
f
5
0
-
8
0
%
o
f
p
r
e
-
d
i
c
t
e
d
n
o
r
m
a
l
a
n
d
w
i
t
h
i
n
1
5
%
o
f
s
c
r
e
e
n
i
n
g
F
E
V
1
,
u
s
e
o
f
a
l
b
u
t
e
r
o
l
o
n
6
o
f
7
d
a
y
s
b
e
-
f
o
r
e
r
a
n
d
o
m
i
z
a
t
i
o
n
,
a
n
d
a
s
t
h
m
a
s
y
m
p
t
o
m
s
c
o
r
e
2
[
0
-
5
s
c
a
l
e
]
o
n
4
o
f
7
d
a
y
s
b
e
f
o
r
e
r
a
n
d
o
m
i
z
a
t
i
o
n
)
;
u
s
e
o
f
m
e
d
i
a
t
i
o
n
s
f
o
r
r
h
i
n
i
-
t
i
s
w
a
s
a
l
l
o
w
e
d
;
d
i
d
s
a
m
p
l
e
s
i
z
e
e
s
t
i
m
a
t
i
o
n
f
o
r
8
0
%
p
o
w
e
r
t
o
d
e
t
e
c
t
d
i
f
f
e
r
e
n
c
e
o
f
6
p
e
r
-
c
e
n
t
a
g
e
p
o
i
n
t
s
i
n
F
E
V
1
c
h
a
n
g
e
b
e
t
w
e
e
n
2
t
r
e
a
t
m
e
n
t
g
r
o
u
p
s
;
s
t
u
d
y
c
o
n
d
u
c
t
e
d
a
t
5
2
s
i
t
e
s
Conclusion Grading Worksheet Appendix A Diagnosis and Outpatient Management of Asthma
Annotation #8 (Leukotriene Receptor Antagonists [LTRAs]) Seventh Edition/March 2005
Institute for Clinical Systems Improvement
www.icsi.org
35
D
u
c
h
a
r
m
e
&
H
i
c
k
s
,
2
0
0
2
S
y
s
-
t
e
m
a
t
i
c
R
e
v
i
e
w
M
+
-
S
e
a
r
c
h
o
f
c
l
i
n
i
c
a
l
t
r
i
a
l
s
d
a
t
a
-
b
a
s
e
s
;
c
o
n
t
a
c
t
w
i
t
h
p
h
a
r
m
a
c
e
u
t
i
-
c
a
l
c
o
m
p
a
n
i
e
s
-
Q
u
a
l
i
t
y
o
f
s
t
u
d
i
e
s
a
s
s
e
s
s
e
d
b
y
2
m
a
s
k
e
d
r
e
v
i
e
w
e
r
s
-
1
4
t
r
i
a
l
s
m
e
t
i
n
c
l
u
s
i
o
n
c
r
i
t
e
r
i
a
(
i
n
c
l
u
d
i
n
g
B
l
e
e
k
e
r
,
2
0
0
0
,
B
u
s
s
e
2
0
0
1
,
a
n
d
M
a
l
m
s
t
r
o
m
,
1
9
9
9
,
[
a
b
o
v
e
]
)
;
a
l
l
R
C
T
s
e
x
c
e
p
t
o
n
e
;
1
2
f
o
c
u
s
e
d
o
n
a
d
u
l
t
s
;
i
n
t
e
r
v
e
n
-
t
i
o
n
d
u
r
a
t
i
o
n
o
f
4
t
o
3
7
w
k
s
;
i
n
c
l
u
d
e
d
m
o
n
t
e
l
u
k
a
s
t
,
p
r
a
n
l
u
-
k
a
s
t
,
z
a
f
i
r
l
u
k
a
s
t
,
b
e
c
l
o
m
e
t
h
a
-
s
o
n
e
,
a
n
d
f
l
u
t
i
c
a
s
o
n
e
-
1
0
t
r
i
a
l
s
h
a
d
h
i
g
h
q
u
a
l
i
t
y
(
4
o
f
5
p
o
i
n
t
s
)
;
1
1
w
i
t
h
a
p
p
r
o
p
r
i
a
t
e
r
a
n
d
o
m
i
z
a
t
i
o
n
m
e
t
h
o
d
s
;
1
1
d
o
u
b
l
e
-
b
l
i
n
d
;
w
i
t
h
d
r
a
w
a
l
r
a
t
e
s
o
f
0
%
-
2
9
%
-
P
r
i
m
a
r
y
o
u
t
c
o
m
e
(
r
e
s
u
l
t
s
f
r
o
m
1
1
t
r
i
a
l
s
)
:
r
a
t
e
o
f
e
x
a
c
e
r
b
a
t
i
o
n
s
r
e
q
u
i
r
i
n
g
s
y
s
t
e
m
i
c
c
o
r
t
i
c
o
s
t
e
r
o
i
d
s
;
p
a
-
t
i
e
n
t
s
t
r
e
a
t
e
d
w
i
t
h
a
n
t
i
-
l
e
u
k
o
t
r
i
e
n
e
s
h
a
d
6
1
%
i
n
-
c
r
e
a
s
e
d
r
i
s
k
o
f
e
x
a
c
e
r
b
a
t
i
o
n
c
o
m
p
a
r
e
d
t
o
p
a
t
i
e
n
t
s
t
r
e
a
t
e
d
w
i
t
h
I
C
S
s
(
R
R
=
1
.
6
1
;
9
5
%
C
I
1
.
1
5
-
2
.
2
5
)
;
n
o
a
p
p
a
r
e
n
t
d
i
f
f
e
r
e
n
c
e
d
u
e
t
o
m
o
n
t
e
l
u
k
a
s
t
v
s
.
z
a
f
i
r
l
u
-
k
a
s
t
,
b
e
c
l
o
m
e
t
h
a
s
o
n
e
v
s
.
f
l
u
t
i
c
a
s
o
n
e
,
q
u
a
l
i
t
y
o
f
s
t
u
d
i
e
s
,
p
u
b
l
i
s
h
e
d
v
s
.
u
n
p
u
b
l
i
s
h
e
d
d
a
t
a
,
s
o
u
r
c
e
o
f
f
u
n
d
i
n
g
;
g
r
e
a
t
e
r
e
f
f
e
c
t
i
n
t
r
i
a
l
s
o
f
1
2
-
1
6
w
k
s
v
s
4
-
6
w
k
s
,
p
a
t
i
e
n
t
s
w
i
t
h
m
o
d
e
r
a
t
e
v
s
.
m
i
l
d
a
s
t
h
m
a
-
O
t
h
e
r
o
u
t
c
o
m
e
s
:
i
m
p
r
o
v
e
m
e
n
t
s
i
n
F
E
V
1
,
P
E
F
R
-
a
m
,
c
h
a
n
g
e
i
n
s
y
m
p
t
o
m
s
c
o
r
e
,
n
i
g
h
t
t
i
m
e
a
w
a
k
e
n
-
i
n
g
s
,
s
y
m
p
t
o
m
-
f
r
e
e
d
a
y
s
,
a
n
d
q
u
a
l
i
t
y
o
f
l
i
f
e
a
l
l
f
a
-
v
o
r
e
d
I
C
S
s
;
a
n
t
i
-
l
e
u
k
o
t
r
i
e
n
e
t
h
e
r
a
p
y
a
s
s
o
c
i
a
t
e
d
w
i
t
h
g
r
e
a
t
e
r
r
i
s
k
o
f
o
v
e
r
a
l
l
w
i
t
h
d
r
a
w
a
l
s
(
R
R
=
1
.
3
;
9
5
%
C
I
1
.
1
-
1
.
6
)
a
p
p
a
r
e
n
t
l
y
d
u
e
t
o
p
o
o
r
a
s
t
h
m
a
c
o
n
t
r
o
l
;
n
o
d
i
f
f
e
r
e
n
c
e
i
n
p
a
t
i
e
n
t
s
e
x
p
e
r
i
e
n
c
i
n
g
"
a
n
y
a
d
v
e
r
s
e
e
f
-
f
e
c
t
s
"
-
F
o
r
m
o
s
t
a
s
t
h
m
a
o
u
t
c
o
m
e
s
,
I
C
S
s
a
t
4
0
0
m
c
g
/
d
a
y
o
f
b
e
c
l
o
m
e
t
h
a
s
o
n
e
-
e
q
u
i
v
a
l
e
n
t
a
r
e
m
o
r
e
e
f
f
e
c
t
i
v
e
t
h
a
n
a
n
t
i
-
l
e
u
k
o
t
r
i
e
n
e
a
g
e
n
t
s
g
i
v
e
n
i
n
t
h
e
u
s
u
a
l
l
i
c
e
n
s
e
d
d
o
s
e
s
.
T
h
e
e
x
a
c
t
d
o
s
e
-
e
q
u
i
v
a
l
e
n
c
e
o
f
a
n
t
i
-
l
e
u
k
o
t
r
i
e
n
e
a
g
e
n
t
s
i
n
m
c
g
o
f
I
C
S
s
r
e
m
a
i
n
s
t
o
b
e
d
e
t
e
r
m
i
n
e
d
.
Conclusion Grading Worksheet Appendix A Diagnosis and Outpatient Management of Asthma
Annotation #8 (Leukotriene Receptor Antagonists [LTRAs]) Seventh Edition/March 2005
Institute for Clinical Systems Improvement
www.icsi.org
36
Conclusion Grading Worksheet Appendix B
Annotation #9 (Asthma Education)
Diagnosis and Outpatient Management of Asthma
Seventh Edition/March 2005
W
o
r
k
G
r
o
u
p
'
s
C
o
n
c
l
u
s
i
o
n
:
S
u
p
e
r
v
i
s
e
d
s
e
l
f
-
m
a
n
a
g
e
m
e
n
t
(
u
s
i
n
g
p
a
t
i
e
n
t
e
d
u
c
a
t
i
o
n
a
n
d
a
d
j
u
s
t
m
e
n
t
s
o
f
a
n
t
i
-
i
n
f
l
a
m
m
a
t
o
r
y
m
e
d
i
c
a
t
i
o
n
b
a
s
e
d
o
n
P
E
F
o
r
s
y
m
p
t
o
m
s
c
o
u
p
l
e
d
w
i
t
h
r
e
g
u
l
a
r
m
e
d
i
c
a
l
r
e
v
i
e
w
,
u
t
i
l
i
z
a
t
i
o
n
a
n
d
a
d
h
e
r
e
n
c
e
t
o
m
e
d
i
c
a
t
i
o
n
)
r
e
d
u
c
e
s
a
s
t
h
m
a
m
o
r
b
i
d
i
t
y
.
T
h
i
s
r
e
d
u
c
t
i
o
n
i
n
c
l
u
d
e
s
l
o
s
t
w
o
r
k
d
a
y
s
,
u
n
s
c
h
e
d
u
l
e
d
o
f
f
i
c
e
v
i
s
i
t
s
,
a
n
d
E
R
a
n
d
h
o
s
p
i
t
a
l
a
d
m
i
s
s
i
o
n
s
.
C
o
n
c
l
u
s
i
o
n
G
r
a
d
e
:
I
A
u
t
h
o
r
/
Y
e
a
r
D
e
s
i
g
n
T
y
p
e
C
l
a
s
s
Q
u
a
l
-
i
t
y
+
,
P
o
p
u
l
a
t
i
o
n
S
t
u
d
i
e
d
/
S
a
m
p
l
e
S
i
z
e
P
r
i
m
a
r
y
O
u
t
c
o
m
e
M
e
a
s
u
r
e
(
s
)
/
R
e
s
u
l
t
s
(
e
.
g
.
,
p
-
v
a
l
u
e
,
c
o
n
f
i
d
e
n
c
e
i
n
t
e
r
v
a
l
,
r
e
l
a
t
i
v
e
r
i
s
k
,
o
d
d
s
r
a
t
i
o
,
l
i
k
e
l
i
-
h
o
o
d
r
a
t
i
o
,
n
u
m
b
e
r
n
e
e
d
e
d
t
o
t
r
e
a
t
)
A
u
t
h
o
r
s
'
C
o
n
c
l
u
s
i
o
n
s
/
W
o
r
k
G
r
o
u
p
'
s
C
o
m
m
e
n
t
s
(
i
t
a
l
i
c
i
z
e
d
)
M
a
y
o
,
R
i
c
h
-
m
a
n
,
&
H
a
r
r
i
s
,
1
9
9
0
R
C
T
A
-
P
a
t
i
e
n
t
s
h
o
s
p
i
t
a
l
i
z
e
d
w
i
t
h
a
c
u
t
e
a
s
t
h
m
a
e
x
a
c
e
r
b
a
t
i
o
n
;
1
8
+
y
r
s
o
l
d
;
>
4
E
R
v
i
s
i
t
s
i
n
p
a
s
t
1
2
m
o
s
o
r
>
1
h
o
s
p
i
t
a
l
i
z
a
t
i
o
n
i
n
p
a
s
t
2
4
m
o
s
-
R
a
n
d
o
m
i
z
e
d
t
o
s
p
e
c
i
a
l
c
l
i
n
i
c
g
r
o
u
p
o
r
r
o
u
t
i
n
e
c
l
i
n
i
c
g
r
o
u
p
;
a
f
t
e
r
8
m
o
n
t
h
s
,
1
9
p
a
t
i
e
n
t
s
f
r
o
m
r
o
u
t
i
n
e
g
r
o
u
p
s
e
l
e
c
t
e
d
(
b
a
s
e
d
o
n
m
u
l
t
i
p
l
e
h
o
s
p
i
t
a
l
i
z
a
t
i
o
n
s
)
t
o
c
r
o
s
s
t
o
s
p
e
c
i
a
l
c
l
i
n
i
c
g
r
o
u
p
-
1
0
4
r
a
n
d
o
m
i
z
e
d
(
4
7
t
o
s
p
e
c
i
a
l
c
l
i
n
i
c
,
5
7
t
o
r
o
u
t
i
n
e
c
l
i
n
i
c
)
;
1
0
o
f
4
7
n
e
v
e
r
a
t
t
e
n
d
e
d
s
p
e
c
i
a
l
c
l
i
n
i
c
;
a
f
t
e
r
8
m
o
n
t
h
s
1
9
f
r
o
m
r
o
u
t
i
n
e
c
l
i
n
i
c
g
r
o
u
p
j
o
i
n
e
d
s
p
e
c
i
a
l
c
l
i
n
i
c
g
r
o
u
p
(
n
=
5
6
w
i
t
h
1
l
o
s
t
t
o
f
o
l
l
o
w
-
u
p
)
-
S
p
e
c
i
a
l
c
l
i
n
i
c
,
r
o
u
t
i
n
e
c
l
i
n
i
c
,
a
n
d
c
r
o
s
s
-
o
v
e
r
g
r
o
u
p
s
s
i
m
i
l
a
r
a
t
b
a
s
e
l
i
n
e
e
x
c
e
p
t
f
e
w
e
r
i
n
c
r
o
s
s
-
o
v
e
r
g
r
o
u
p
e
v
e
r
r
e
q
u
i
r
e
d
i
n
t
u
b
a
t
i
o
n
-
A
f
t
e
r
e
n
r
o
l
l
m
e
n
t
i
n
s
p
e
c
i
a
l
c
l
i
n
i
c
(
n
=
5
6
)
:
l
e
s
s
u
s
e
o
f
o
r
a
l
b
e
t
a
a
g
o
n
i
s
t
s
a
n
d
d
a
i
l
y
p
r
e
d
n
i
s
o
n
e
,
g
r
e
a
t
e
r
u
s
e
o
f
c
h
r
o
n
i
c
i
n
h
a
l
e
d
c
o
r
t
i
c
o
s
t
e
r
o
i
d
s
,
b
r
i
e
f
p
r
e
d
n
i
-
s
o
n
e
p
u
l
s
e
s
,
r
e
s
e
r
v
o
i
r
s
p
a
c
e
r
d
e
v
i
c
e
s
,
a
n
d
h
o
m
e
p
e
a
k
f
l
o
w
m
o
n
i
t
o
r
s
-
S
p
e
c
i
a
l
c
l
i
n
i
c
g
r
o
u
p
(
n
=
4
7
)
h
a
d
l
o
w
e
r
h
o
s
p
i
t
a
l
u
s
e
t
h
a
n
r
o
u
t
i
n
e
c
l
i
n
i
c
(
n
=
5
7
)
(
0
.
4
v
s
.
1
.
2
a
d
m
i
s
s
i
o
n
s
p
e
r
p
a
t
i
e
n
t
[
p
<
0
.
0
0
4
]
a
n
d
3
.
1
v
s
.
6
.
7
r
e
-
h
o
s
p
i
t
a
l
i
z
a
t
i
o
n
d
a
y
s
p
e
r
p
a
t
i
e
n
t
[
p
<
0
.
0
2
]
)
-
F
o
r
3
4
o
f
3
7
w
h
o
a
t
t
e
n
d
s
p
e
c
i
a
l
c
l
i
n
i
c
r
e
-
a
d
m
i
s
s
i
o
n
r
a
t
e
p
e
r
p
a
t
i
e
n
t
p
e
r
m
o
n
t
h
d
e
c
r
e
a
s
e
d
f
r
o
m
0
.
1
3
b
e
-
f
o
r
e
e
n
r
o
l
l
m
e
n
t
t
o
0
.
0
4
a
f
t
e
r
(
p
=
0
.
0
0
3
)
a
n
d
r
e
-
h
o
s
p
i
t
a
l
i
z
a
t
i
o
n
d
a
y
s
p
e
r
p
a
t
i
e
n
t
p
e
r
m
o
n
t
h
d
e
c
r
e
a
s
e
d
f
r
o
m
0
.
7
3
t
o
0
.
2
6
(
p
=
0
.
0
0
3
)
;
s
i
m
i
l
a
r
f
i
n
d
i
n
g
s
f
o
r
c
r
o
s
s
-
o
v
e
r
g
r
o
u
p
-
N
o
d
e
a
t
h
s
f
r
o
m
a
s
t
h
m
a
i
n
s
p
e
c
i
a
l
c
l
i
n
i
c
g
r
o
u
p
;
o
n
e
d
e
a
t
h
i
n
r
o
u
t
i
n
e
g
r
o
u
p
;
4
s
p
e
c
i
a
l
c
l
i
n
i
c
p
a
t
i
e
n
t
s
r
e
-
q
u
i
r
e
d
i
n
t
u
b
a
t
i
o
n
i
n
3
2
m
o
n
t
h
s
f
o
l
l
o
w
-
u
p
-
A
v
i
g
o
r
o
u
s
m
e
d
i
c
a
l
r
e
g
i
m
e
n
a
n
d
i
n
t
e
n
s
i
v
e
e
d
u
c
a
t
i
o
n
p
r
o
g
r
a
m
w
a
s
a
b
l
e
t
o
d
e
c
r
e
a
s
e
h
o
s
-
p
i
t
a
l
u
s
e
a
m
o
n
g
a
g
r
o
u
p
o
f
a
d
u
l
t
a
s
t
h
m
a
t
i
c
s
w
h
o
h
a
d
p
r
e
v
i
o
u
s
l
y
r
e
q
u
i
r
e
d
r
e
p
e
a
t
e
d
r
e
a
d
-
m
i
s
s
i
o
n
s
f
o
r
a
c
u
t
e
a
s
t
h
m
a
e
x
a
c
e
r
b
a
t
i
o
n
s
.
N
O
T
E
S
:
a
s
p
e
c
i
a
l
o
u
t
p
a
t
i
e
n
t
a
s
t
h
m
a
c
l
i
n
i
c
w
a
s
d
e
v
e
l
o
p
e
d
t
o
r
e
d
u
c
e
r
e
-
a
d
m
i
s
s
i
o
n
s
f
o
r
a
s
t
h
m
a
e
x
a
c
e
r
b
a
t
i
o
n
;
a
l
l
p
a
t
i
e
n
t
s
t
r
e
a
t
e
d
b
y
s
a
m
e
p
h
y
s
i
c
i
a
n
;
c
l
i
n
i
c
p
r
o
g
r
a
m
i
n
c
l
u
d
e
d
p
a
-
t
i
e
n
t
e
d
u
c
a
t
i
o
n
a
n
d
i
n
d
i
v
i
d
u
a
l
m
e
d
i
c
a
t
i
o
n
r
e
g
i
m
e
n
s
w
i
t
h
e
m
p
h
a
s
i
s
o
n
s
e
l
f
-
m
a
n
a
g
e
-
m
e
n
t
;
h
o
s
p
i
t
a
l
u
s
a
g
e
b
e
f
o
r
e
s
p
e
c
i
a
l
c
l
i
n
i
c
e
n
-
r
o
l
l
m
e
n
t
w
a
s
l
i
m
i
t
e
d
t
o
1
h
o
s
p
i
t
a
l
w
h
i
l
e
u
s
-
a
g
e
a
f
t
e
r
e
n
r
o
l
l
m
e
n
t
i
n
c
l
u
d
e
d
o
t
h
e
r
h
o
s
p
i
t
a
l
s
i
n
t
h
e
a
r
e
a
;
n
o
a
t
t
e
m
p
t
w
a
s
m
a
d
e
t
o
d
e
t
e
r
-
m
i
n
e
w
h
a
t
e
l
e
m
e
n
t
o
f
t
h
e
p
r
o
g
r
a
m
,
i
f
a
n
y
,
w
a
s
e
s
s
e
n
t
i
a
l
W
o
r
k
G
r
o
u
p
'
s
C
o
m
m
e
n
t
s
:
d
i
f
f
e
r
e
n
t
o
b
s
e
r
v
a
-
t
i
o
n
s
c
h
e
d
u
l
e
s
;
n
o
s
t
a
t
i
s
t
i
c
s
f
o
r
d
r
u
g
u
s
e
d
a
t
a
;
p
o
p
u
l
a
t
i
o
n
w
a
s
l
a
r
g
e
l
y
H
i
s
p
a
n
i
c
;
n
o
d
a
t
a
o
n
c
o
m
p
l
i
a
n
c
e
w
i
t
h
p
r
o
g
r
a
m
s
Institute for Clinical Systems Improvement
www.icsi.org
37
Conclusion Grading Worksheet Appendix B Diagnosis and Outpatient Management of Asthma
Annotation #9 (Asthma Education) Seventh Edition/March 2005
A
u
t
h
o
r
/
Y
e
a
r
D
e
s
i
g
n
T
y
p
e
C
l
a
s
s
Q
u
a
l
-
i
t
y
+
,
P
o
p
u
l
a
t
i
o
n
S
t
u
d
i
e
d
/
S
a
m
p
l
e
S
i
z
e
P
r
i
m
a
r
y
O
u
t
c
o
m
e
M
e
a
s
u
r
e
(
s
)
/
R
e
s
u
l
t
s
(
e
.
g
.
,
p
-
v
a
l
u
e
,
c
o
n
f
i
d
e
n
c
e
i
n
t
e
r
v
a
l
,
r
e
l
a
t
i
v
e
r
i
s
k
,
o
d
d
s
r
a
t
i
o
,
l
i
k
e
l
i
-
h
o
o
d
r
a
t
i
o
,
n
u
m
b
e
r
n
e
e
d
e
d
t
o
t
r
e
a
t
)
A
u
t
h
o
r
s
'
C
o
n
c
l
u
s
i
o
n
s
/
W
o
r
k
G
r
o
u
p
'
s
C
o
m
m
e
n
t
s
(
i
t
a
l
i
c
i
z
e
d
)
I
g
n
a
c
i
o
-
G
a
r
c
i
a
&
G
o
n
z
a
l
e
z
-
S
a
n
t
o
s
,
1
9
9
5
R
C
T
A
-
P
a
t
i
e
n
t
s
f
r
o
m
o
n
e
o
u
t
p
a
t
i
e
n
t
a
s
t
h
m
a
c
l
i
n
i
c
;
1
4
t
o
6
5
y
e
a
r
s
w
i
t
h
a
s
t
h
m
a
d
i
a
g
n
o
s
e
d
2
y
r
s
p
r
i
o
r
-
R
a
n
d
o
m
i
z
e
d
t
o
e
x
p
e
r
i
m
e
n
t
a
l
(
s
e
l
f
m
a
n
a
g
e
m
e
n
t
w
i
t
h
p
e
a
k
-
f
l
o
w
r
e
a
d
i
n
g
s
a
s
b
a
s
i
s
f
o
r
t
r
e
a
t
-
m
e
n
t
p
l
a
n
p
l
u
s
e
d
u
c
a
t
i
o
n
p
r
o
-
g
r
a
m
)
o
r
c
o
n
t
r
o
l
(
s
y
m
p
t
o
m
s
a
n
d
s
p
i
r
o
m
e
t
r
i
c
d
a
t
a
f
o
r
f
o
l
l
o
w
i
n
g
p
h
y
s
i
c
i
a
n
'
s
t
r
e
a
t
m
e
n
t
p
l
a
n
)
-
M
e
d
i
c
a
l
r
e
g
i
m
e
n
s
t
a
i
l
o
r
e
d
t
o
i
n
d
i
v
i
d
u
a
l
p
a
t
i
e
n
t
-
F
o
l
l
o
w
-
u
p
:
1
,
3
,
5
,
a
n
d
6
m
o
s
-
D
e
g
r
e
e
o
f
i
l
l
n
e
s
s
:
m
o
r
b
i
d
i
t
y
p
a
-
r
a
m
e
t
e
r
s
,
s
p
i
r
o
m
e
t
r
i
c
d
a
t
a
,
c
o
n
-
s
u
m
p
t
i
o
n
o
f
d
r
u
g
s
,
r
a
t
e
s
a
t
-
t
a
i
n
e
d
b
y
p
e
a
k
f
l
o
w
m
e
t
e
r
i
n
g
-
C
o
m
p
a
r
e
d
6
m
o
s
b
e
f
o
r
e
i
n
t
e
r
-
v
e
n
t
i
o
n
w
i
t
h
6
m
o
s
a
f
t
e
r
-
9
4
e
n
r
o
l
l
e
d
;
2
4
c
o
m
p
l
e
t
e
d
i
n
i
t
i
a
l
a
s
s
e
s
s
m
e
n
t
b
u
t
l
a
t
e
r
d
r
o
p
p
e
d
o
u
t
o
r
w
e
r
e
e
x
c
l
u
d
e
d
f
o
r
p
r
o
t
o
c
o
l
v
i
o
-
l
a
t
i
o
n
s
(
9
c
o
n
t
r
o
l
,
1
5
e
x
p
e
r
i
m
e
n
t
a
l
)
-
A
n
a
l
y
s
i
s
b
a
s
e
d
o
n
7
0
p
a
t
i
e
n
t
s
(
3
2
M
,
3
8
F
)
,
m
e
a
n
a
g
e
4
2
(
r
a
n
g
e
1
6
-
6
4
)
;
3
5
e
x
p
e
r
i
m
e
n
t
a
l
,
3
5
c
o
n
t
r
o
l
;
g
r
o
u
p
s
c
o
m
p
a
r
a
b
l
e
a
t
b
a
s
e
l
i
n
e
i
n
a
g
e
,
g
e
n
d
e
r
,
s
o
c
i
a
l
c
l
a
s
s
,
s
m
o
k
i
n
g
,
y
e
a
r
s
o
f
a
s
t
h
m
a
,
c
h
r
o
n
i
c
b
r
o
n
c
h
i
t
i
s
-
A
f
t
e
r
i
n
t
e
r
v
e
n
t
i
o
n
g
r
o
u
p
s
d
i
f
f
e
r
e
d
(
p
<
0
.
0
5
)
i
n
d
a
y
s
l
o
s
t
f
r
o
m
w
o
r
k
,
e
x
a
c
e
r
b
a
t
i
o
n
s
,
d
a
y
s
o
n
a
n
t
i
b
i
o
t
i
c
s
,
p
h
y
s
i
c
i
a
n
c
o
n
s
u
l
t
a
t
i
o
n
s
,
E
R
a
d
m
i
s
s
i
o
n
s
,
n
o
c
t
u
r
n
a
l
w
a
k
e
n
i
n
g
-
C
o
n
t
r
o
l
g
r
o
u
p
:
f
e
w
e
r
e
x
a
c
e
r
b
a
t
i
o
n
s
a
n
d
p
h
y
s
i
c
i
a
n
c
o
n
s
u
l
t
a
t
i
o
n
s
a
f
t
e
r
s
t
u
d
y
p
e
r
i
o
d
(
b
o
t
h
p
<
0
.
0
1
)
-
E
x
p
e
r
i
m
e
n
t
a
l
g
r
o
u
p
:
f
e
w
e
r
d
a
y
s
l
o
s
t
f
r
o
m
w
o
r
k
,
e
x
a
c
e
r
b
a
t
i
o
n
s
,
d
a
y
s
o
n
a
n
t
i
b
i
o
t
i
c
s
,
p
h
y
s
i
c
i
a
n
c
o
n
s
u
l
-
t
a
t
i
o
n
s
,
E
R
a
d
m
i
s
s
i
o
n
s
a
f
t
e
r
s
t
u
d
y
p
e
r
i
o
d
(
a
l
l
p
<
0
.
0
1
)
-
F
E
V
1
,
F
V
C
,
a
n
d
F
E
V
1
/
F
V
C
i
m
p
r
o
v
e
d
o
v
e
r
s
t
u
d
y
p
e
r
i
o
d
i
n
e
x
p
e
r
i
m
e
n
t
a
l
g
r
o
u
p
(
a
l
l
p
<
0
.
0
0
3
f
r
o
m
b
a
s
e
l
i
n
e
)
;
c
o
n
t
r
o
l
g
r
o
u
p
i
m
p
r
o
v
e
d
F
E
V
1
a
n
d
F
E
V
1
/
F
V
C
a
t
f
i
r
s
t
f
o
l
l
o
w
-
u
p
b
u
t
r
e
t
u
r
n
e
d
t
o
w
a
r
d
b
a
s
e
l
i
n
e
t
h
e
r
e
a
f
t
e
r
-
M
e
a
n
p
e
a
k
e
x
p
i
r
a
t
o
r
y
f
l
o
w
r
a
t
e
(
P
E
F
R
)
h
i
g
h
e
r
i
n
e
x
p
e
r
i
m
e
n
t
a
l
g
r
o
u
p
a
t
a
l
l
f
o
l
l
o
w
-
u
p
v
i
s
i
t
s
(
a
l
l
p
<
0
.
0
5
)
;
m
e
a
n
P
E
F
R
a
n
d
m
o
r
n
i
n
g
P
E
F
R
i
n
c
r
e
a
s
e
d
s
i
g
n
i
f
i
c
a
n
t
l
y
f
r
o
m
b
a
s
e
l
i
n
e
i
n
e
x
p
e
r
i
m
e
n
t
a
l
g
r
o
u
p
(
p
<
0
.
0
0
1
)
;
P
E
F
R
m
o
r
e
v
a
r
i
a
b
l
e
i
n
c
o
n
t
r
o
l
g
r
o
u
p
-
E
x
p
e
r
i
m
e
n
t
a
l
g
r
o
u
p
u
s
e
d
l
e
s
s
f
e
n
o
t
e
r
o
l
a
n
d
p
r
e
d
n
i
-
s
o
n
e
(
b
o
t
h
p
<
0
.
0
5
)
t
h
a
n
c
o
n
t
r
o
l
a
n
d
d
e
c
r
e
a
s
e
d
u
s
e
o
f
a
l
b
u
t
e
r
o
l
,
t
e
r
b
u
t
a
l
i
n
e
,
f
e
n
o
t
e
r
o
l
,
t
h
e
o
p
h
y
l
l
i
n
e
,
a
n
d
b
u
d
e
s
o
n
i
d
e
d
u
r
i
n
g
s
t
u
d
y
p
e
r
i
o
d
(
a
l
l
p
<
0
.
0
5
)
;
-
P
e
a
k
f
l
o
w
m
o
n
i
t
o
r
i
n
g
a
s
s
o
c
i
a
t
e
d
w
i
t
h
a
n
e
d
u
c
a
t
i
o
n
p
r
o
g
r
a
m
r
e
d
u
c
e
d
m
o
r
b
i
d
i
t
y
,
i
m
-
p
r
o
v
e
d
l
u
n
g
f
u
n
c
t
i
o
n
,
a
n
d
o
p
t
i
m
i
z
e
d
t
h
e
u
s
e
o
f
m
e
d
i
c
a
t
i
o
n
i
n
a
d
u
l
t
a
s
t
h
m
a
p
a
t
i
e
n
t
s
.
N
O
T
E
S
:
o
n
e
p
h
y
s
i
c
i
a
n
(
u
n
b
l
i
n
d
e
d
)
a
s
s
e
s
s
e
d
p
a
t
i
e
n
t
s
'
c
o
n
d
i
t
i
o
n
a
n
d
m
o
d
i
f
i
e
d
t
r
e
a
t
m
e
n
t
a
t
f
o
l
l
o
w
-
u
p
v
i
s
i
t
s
;
b
e
f
o
r
e
i
n
t
e
r
v
e
n
t
i
o
n
g
r
o
u
p
s
c
o
m
p
a
r
a
b
l
e
i
n
d
a
y
s
l
o
s
t
f
r
o
m
w
o
r
k
,
a
c
u
t
e
e
x
a
c
e
r
b
a
t
i
o
n
s
,
d
a
y
s
o
n
a
n
t
i
b
i
o
t
i
c
s
,
p
h
y
s
i
c
i
a
n
c
o
n
s
u
l
t
a
t
i
o
n
s
,
E
R
a
d
m
i
s
s
i
o
n
s
,
h
o
s
p
i
t
a
l
a
d
-
m
i
s
s
i
o
n
s
W
o
r
k
G
r
o
u
p
'
s
C
o
m
m
e
n
t
s
:
L
i
t
t
l
e
i
n
f
o
r
m
a
-
t
i
o
n
a
b
o
u
t
i
n
c
l
u
s
i
o
n
/
e
x
c
l
u
s
i
o
n
c
r
i
t
e
r
i
a
o
r
c
o
m
o
r
b
i
d
i
t
i
e
s
;
a
n
a
l
y
s
i
s
w
a
s
n
o
t
i
n
t
e
n
t
i
o
n
-
t
o
-
t
r
e
a
t
Institute for Clinical Systems Improvement
www.icsi.org
38
A
u
t
h
o
r
/
Y
e
a
r
D
e
s
i
g
n
T
y
p
e
C
l
a
s
s
Q
u
a
l
-
i
t
y
+
,
P
o
p
u
l
a
t
i
o
n
S
t
u
d
i
e
d
/
S
a
m
p
l
e
S
i
z
e
P
r
i
m
a
r
y
O
u
t
c
o
m
e
M
e
a
s
u
r
e
(
s
)
/
R
e
s
u
l
t
s
(
e
.
g
.
,
p
-
v
a
l
u
e
,
c
o
n
f
i
d
e
n
c
e
i
n
t
e
r
v
a
l
,
r
e
l
a
t
i
v
e
r
i
s
k
,
o
d
d
s
r
a
t
i
o
,
l
i
k
e
l
i
-
h
o
o
d
r
a
t
i
o
,
n
u
m
b
e
r
n
e
e
d
e
d
t
o
t
r
e
a
t
)
A
u
t
h
o
r
s
'
C
o
n
c
l
u
s
i
o
n
s
/
W
o
r
k
G
r
o
u
p
'
s
C
o
m
m
e
n
t
s
(
i
t
a
l
i
c
i
z
e
d
)
L
a
h
d
e
n
s
u
o
e
t
a
l
.
,
1
9
9
6
R
C
T
A
-
A
d
u
l
t
s
(
1
8
+
)
f
r
o
m
3
o
u
t
p
a
t
i
e
n
t
c
e
n
t
e
r
s
;
m
i
l
d
t
o
m
o
d
e
r
a
t
e
l
y
s
e
-
v
e
r
e
a
s
t
h
m
a
;
i
n
c
l
u
s
i
o
n
/
e
x
c
l
u
s
i
o
n
c
r
i
t
e
r
i
a
b
a
s
e
d
o
n
p
e
a
k
f
l
o
w
r
a
t
e
a
n
d
m
e
d
i
c
a
t
i
o
n
s
(
s
e
e
N
O
T
E
S
)
-
R
a
n
d
o
m
i
z
e
d
t
o
s
e
l
f
-
m
a
n
a
g
e
-
m
e
n
t
(
p
e
r
s
o
n
a
l
e
d
u
c
a
t
i
o
n
s
e
s
-
s
i
o
n
s
,
d
a
i
l
y
m
o
r
n
i
n
g
p
e
a
k
f
l
o
w
m
e
a
s
u
r
e
m
e
n
t
s
w
i
t
h
m
e
d
i
c
a
t
i
o
n
p
l
a
n
b
a
s
e
d
o
n
r
e
s
u
l
t
s
)
o
r
t
r
a
d
i
-
t
i
o
n
a
l
t
r
e
a
t
m
e
n
t
(
i
n
f
o
.
o
n
i
n
h
a
l
e
r
u
s
e
,
n
o
c
h
a
n
g
e
s
i
n
m
e
d
i
c
a
t
i
o
n
s
o
n
t
h
e
i
r
o
w
n
)
-
B
a
s
e
l
i
n
e
a
n
d
3
f
o
l
l
o
w
-
u
p
v
i
s
i
t
s
o
v
e
r
1
2
m
o
n
t
h
s
-
1
2
2
i
n
i
t
i
a
l
l
y
e
n
r
o
l
l
e
d
,
a
n
a
l
y
s
i
s
b
a
s
e
d
o
n
1
1
5
w
i
t
h
a
t
l
e
a
s
t
4
m
o
s
f
o
l
l
o
w
-
u
p
(
5
6
s
e
l
f
-
m
a
n
a
g
e
m
e
n
t
,
5
9
t
r
a
d
i
t
i
o
n
a
l
)
;
m
o
r
e
w
o
m
e
n
a
n
d
l
o
w
e
r
m
e
a
n
w
e
i
g
h
t
i
n
s
e
l
f
-
m
a
n
a
g
e
m
e
n
t
g
r
o
u
p
(
p
=
0
.
0
2
)
o
t
h
e
r
w
i
s
e
c
o
m
p
a
-
r
a
b
l
e
a
t
b
a
s
e
l
i
n
e
-
O
u
t
c
o
m
e
S
e
l
f
-
m
g
m
t
T
r
a
d
i
t
i
o
n
a
l
p
A
d
m
i
s
s
i
o
n
s
f
o
r
2
p
a
t
i
e
n
t
s
3
p
a
t
i
e
n
t
s
a
s
t
h
m
a
U
n
s
c
h
e
d
u
l
e
d
0
.
5
1
.
0
*
0
.
0
4
o
u
t
p
a
t
i
e
n
t
v
i
s
i
t
s
*
D
a
y
s
o
f
f
w
o
r
k
*
2
.
8
4
.
8
0
.
0
2
C
o
u
r
s
e
s
o
f
0
.
4
0
.
9
0
.
0
0
9
a
n
t
i
b
i
o
t
i
c
s
*
C
o
u
r
s
e
s
o
f
0
.
4
1
.
0
0
.
0
0
6
p
r
e
d
n
i
s
o
n
e
*
T
o
t
a
l
(
a
n
y
0
.
6
2
.
1
<
0
.
0
0
1
i
n
c
i
d
e
n
t
c
a
u
s
e
d
b
y
a
s
t
h
m
a
)
*
*
m
e
a
n
n
u
m
b
e
r
s
p
e
r
p
a
t
i
e
n
t
-
I
n
c
i
d
e
n
c
e
f
r
e
e
s
u
r
v
i
v
a
l
(
p
<
0
.
0
0
0
1
)
a
n
d
q
u
a
l
i
t
y
o
f
l
i
f
e
(
p
=
0
.
0
0
9
)
f
a
v
o
r
e
d
s
e
l
f
-
m
a
n
a
g
e
m
e
n
t
g
r
o
u
p
(
p
<
0
.
0
0
0
1
)
t
h
r
o
u
g
h
o
u
t
s
t
u
d
y
p
e
r
i
o
d
-
E
x
p
l
o
r
a
t
o
r
y
a
n
a
l
y
s
e
s
:
6
2
%
a
d
h
e
r
e
d
t
o
s
e
l
f
-
m
a
n
a
g
e
m
e
n
t
i
n
s
t
r
u
c
t
i
o
n
s
f
o
r
b
u
d
e
s
o
n
i
d
e
d
o
s
e
;
7
7
%
t
o
i
n
s
t
r
u
c
t
i
o
n
s
t
o
s
t
a
r
t
o
r
a
l
p
r
e
d
n
i
s
o
l
o
n
e
;
a
d
h
e
r
e
n
c
e
w
a
s
r
e
l
a
t
e
d
t
o
s
e
v
e
r
i
t
y
o
f
s
y
m
p
t
o
m
s
-
G
u
i
d
e
d
s
e
l
f
-
m
a
n
a
g
e
m
e
n
t
,
u
s
i
n
g
p
a
t
i
e
n
t
e
d
u
-
c
a
t
i
o
n
a
n
d
a
d
j
u
s
t
m
e
n
t
o
f
a
n
t
i
-
i
n
f
l
a
m
m
a
t
o
r
y
t
r
e
a
t
m
e
n
t
b
a
s
e
d
o
n
p
e
a
k
e
x
p
i
r
a
t
o
r
y
m
e
a
s
-
u
r
e
m
e
n
t
s
,
r
e
d
u
c
e
d
b
y
h
a
l
f
o
r
m
o
r
e
t
h
e
n
u
m
-
b
e
r
o
f
i
n
c
i
d
e
n
t
s
c
a
u
s
e
d
b
y
a
s
t
h
m
a
w
h
e
n
c
o
m
p
a
r
e
d
w
i
t
h
t
r
a
d
i
t
i
o
n
a
l
t
r
e
a
t
m
e
n
t
a
n
d
i
m
-
p
r
o
v
e
d
q
u
a
l
i
t
y
o
f
l
i
f
e
.
I
t
i
s
n
o
t
p
o
s
s
i
b
l
e
t
o
d
e
t
e
r
m
i
n
e
w
h
e
t
h
e
r
e
a
r
l
y
t
r
e
a
t
m
e
n
t
o
f
i
n
-
f
l
a
m
m
a
t
i
o
n
,
p
e
a
k
f
l
o
w
m
e
a
s
u
r
e
m
e
n
t
p
e
r
s
e
,
p
a
t
i
e
n
t
e
d
u
c
a
t
i
o
n
,
o
r
i
m
p
r
o
v
e
d
c
o
m
p
l
i
a
n
c
e
i
s
m
o
s
t
i
m
p
o
r
t
a
n
t
.
N
O
T
E
S
:
s
t
u
d
y
w
a
s
s
i
n
g
l
e
-
b
l
i
n
d
;
e
l
i
g
i
b
l
e
p
a
t
i
e
n
t
s
h
a
d
a
)
m
o
r
n
i
n
g
-
e
v
e
n
i
n
g
p
e
a
k
f
l
o
w
v
a
l
u
e
t
h
a
t
v
a
r
i
e
d
b
y
>
1
5
%
i
n
2
d
a
y
s
w
i
t
h
i
n
1
w
k
d
u
r
i
n
g
p
a
s
t
6
m
o
s
,
b
)
o
p
t
i
m
a
l
p
e
a
k
f
l
o
w
2
5
0
l
/
m
i
n
,
c
)
a
n
t
i
-
i
n
f
l
a
m
m
a
t
o
r
y
t
r
e
a
t
m
e
n
t
w
i
t
h
b
u
d
e
s
o
n
i
d
e
(
4
0
0
-
1
6
0
0
g
/
d
a
y
)
o
r
b
e
c
l
o
m
e
t
h
a
s
o
n
e
d
i
p
r
o
p
i
o
n
a
t
e
(
5
0
0
-
2
0
0
0
g
/
d
a
y
)
i
n
p
a
s
t
6
m
o
s
,
d
)
4
w
k
s
s
i
n
c
e
l
a
s
t
c
o
u
r
s
e
o
f
o
r
a
l
c
o
r
t
i
c
o
s
t
e
r
o
i
d
s
;
s
a
m
p
l
e
s
i
z
e
e
s
-
t
i
m
a
t
i
o
n
o
f
6
0
p
e
r
g
r
o
u
p
b
a
s
e
d
o
n
e
s
t
i
m
a
t
e
d
n
u
m
b
e
r
o
f
i
n
c
i
d
e
n
t
s
p
e
r
y
e
a
r
c
a
u
s
e
d
b
y
a
s
t
h
m
a
(
1
w
i
t
h
t
r
a
d
i
t
i
o
n
a
l
t
x
,
0
.
4
7
w
i
t
h
s
e
l
f
-
m
a
n
a
g
e
m
e
n
t
)
;
p
a
t
i
e
n
t
s
w
i
t
h
s
e
v
e
r
e
a
s
t
h
m
a
w
e
r
e
e
x
c
l
u
d
e
d
a
s
m
o
s
t
a
l
r
e
a
d
y
h
a
v
e
p
e
a
k
f
l
o
w
m
e
t
e
r
s
W
o
r
k
G
r
o
u
p
'
s
C
o
m
m
e
n
t
s
:
L
i
t
t
l
e
i
n
f
o
r
m
a
-
t
i
o
n
a
b
o
u
t
c
o
m
o
r
b
i
d
i
t
i
e
s
;
a
n
a
l
y
s
i
s
w
a
s
n
o
t
i
n
t
e
n
t
i
o
n
-
t
o
-
t
r
e
a
t
Conclusion Grading Worksheet Appendix B Diagnosis and Outpatient Management of Asthma
Annotation #9 (Asthma Education) Seventh Edition/March 2005
39
This section provides resources, strategies and measurement specications
for use in closing the gap between current clinical practice and the
recommendations set forth in the guideline.
The subdivisions of this section are:
Priority Aims and Suggested Measures
- Measurement Specications
Key Implementation Recommendations
Knowledge Products
Recommended Resources
I I
CS
INSTITUTE FOR CLINICAL
SYSTEMS IMPROVEMENT
Support for Implementation:
Diagnosis and Outpatient Management of Asthma
Copyright 2005 by Institute for Clinical Systems Improvement
Institute for Clinical Systems Improvement
www.icsi.org
40
Priority Aims and Suggested Measures
1. Promote the accurate assessment of asthma severity through the use of objective measures of lung func-
tion.
Possible measures of accomplishing this aim:
a. Percentage of patients with asthma with spirometry or peak ow documented at the last visit.
b. Percentage of patients with asthma, for whom a peak ow meter is appropriate, who report using
a home peak ow meter.
c. Percentage of patients with asthma with any assessment of asthma severity documented at the last
visit.
2. Promote long-term control of persistent asthma through the use of inhaled corticosteroid drug
therapy.
Possible measure of accomplishing this aim:
a. Percentage of patients with persistent asthma who are on inhaled corticosteroid medication.
3. Promote the partnership of patients with asthma and/or their parents with health care professionals
through education and the use of written action plans.
Possible measures of accomplishing this aim:
a. Percentage of patients with asthma with an asthma action plan in the medical record.
b. Percentage of patients with asthma with education about asthma documented in the medical
record.
Diagnosis and Outpatient Management of Asthma
Seventh Edition/March 2005
Institute for Clinical Systems Improvement
www.icsi.org
41
Measurement Specications
Possible Success Measure #1a
Percentage of patients with asthma with spirometry or peak ow meter reading documented in the medical
record at the last visit.
Population Denition
Patients age 5 through 55 years diagnosed with asthma, continuously enrolled for 6 months.
Data of Interest
# of patients with asthma with spirometry or peak ow meter reading documented at the last visit
total # of patients ages 5-55 with asthma
Numerator/Denominator Denitions
Numerator: Documented is dened as any evidence in the medical record that spirometry or peak ow
reading was done at the last visit as recommended in the guideline.
Denominator: Patients with a diagnosis code of 493.00, 493.01, 493.10, 493.11, 493.90, 493.91, continuously
enrolled for 6 months.
Method/Source of Data Collection
Data may be collected electronically using the claims/encounter database or the enrollment database. Medical
groups should identify patients with asthma seen at the clinic. Each medical group can then generate a list
of all eligible patients with asthma seen during the target month/quarter. A random sample of 20 charts can
be chosen from this list. The eligible patients are those who are 5-55 years old and have been diagnosed
with asthma. The patient medical records are reviewed for any evidence that spirometry or peak ow meter
reading was done at the last visit as recommended in the guideline.
Time Frame Pertaining to Data Collection
A minimum of 20 charts per month can be reviewed.
Notes
It is important to periodically assess pulmonary function. The main methods are spirometry or PEFR.
Spirometry is more precise and yields more information than PEFR. It is helpful to verify the accuracy of
the peak ow meter. It is useful when certain physical limitations affect accuracy of PEFR (e.g., very young
or elderly, neuromuscular or orthopedic problems). PEFR provides a simple, quantitative and reproductive
measure of severity of airow obstruction. The results are more reliable if the same type and preferably
the patient's own meter are used.
Diagnosis and Outpatient Management of Asthma
Priority Aims and Suggested Measures Seventh Edition/March 2005
Institute for Clinical Systems Improvement
www.icsi.org
42
Diagnosis and Outpatient Management of Asthma
Priority Aims and Suggested Measures Seventh Edition/March 2005
Possible Success Measure #2a (children)
Percentage of children with persistent asthma who are on inhaled corticosteroids medication.
Population Denition
Children aged 17 and under with persistent asthma, continuously enrolled for 6 months.
Data of Interest
# children in denominator who have one or more prescriptions for inhaled corticosteroids medications
# of children with persistent asthma
Numerator/ Denominator Denitions
Numerator
Among the children in the denominator, the number who have one or more prescriptions for inhaled corti-
costeroids medications:
- beclomethasone HFA (Vanceril, Beclovent, QVAR) - unisolide (Aerobid)
- triamcinolone (Azmacort) - budesonide (Pulmicort)
- uticasone (Flovent, Advair)
Denominator
Children with persistent asthma with a diagnosis code of 493.00, 493.01, 493.10, 493.11, 493.90, 493.91,
continuously enrolled for 6 months.
Method/Source of Data Collection
This measure may be collected electronically using the pharmacy data base, the claims/encounter data base,
or the enrollment data base.
Time Frame of Data Collection
It is suggested that data are collected quarterly.
Notes
Since asthma is a chronic inammatory disorder of the airways with recurrent exacerbations, therapy for
persistent asthma emphasizes efforts to suppress inammation over the long-term and prevent exacerba-
tions.
Institute for Clinical Systems Improvement
www.icsi.org
43
Diagnosis and Outpatient Management of Asthma
Priority Aims and Suggested Measures Seventh Edition/March 2005
Possible Success Measure #2a (adults)
Percentage of adults with persistent asthma who are on inhaled corticosteroids medication.
Population Denition
Adults age 18 through 39 with persistent asthma, continuously enrolled for 6 months.
Data of Interest
# of adults in the denominator who have 1 or more prescriptions
for inhaled corticosteroids medications
# of adults with persistent asthma
Numerator/Denominator Denitions
Numerator: Persons in the denominator who have 1 or more prescriptions lled for inhaled anti-inam-
matory medications
Inhaled anti-inammatory medications are:
- beclomethasone HFA - triamcinolone - uticasone
- unisolide - budesonide - uticasone
propionatel
salmeterol DPI
Denominator: Adults age 18 through 39 with persistent asthma with a diagnosis code of 493.00,
493.01, 493.10, 493.11, 493.90, 493.91, continuously enrolled for 6 months,
identied by having received one or more rells of the following medications during
the 6 month period:
- beclomethasone HFA - triamcinolone - uticasone
- unisolide - budesonide - uticasone
propionatel
salmeterol DPI
Method/Source of Data Collection
Data may be collected electronically using the pharmacy database, the claims/encounter database or the
enrollment database.
Time Frame Pertaining to Data Collection
It is suggested that data are collected quarterly.
Institute for Clinical Systems Improvement
www.icsi.org
44
Diagnosis and Outpatient Management of Asthma
Priority Aims and Suggested Measures Seventh Edition/March 2005
Possible Success Measure #3b
Percentage of patients with asthma with education about asthma documented in the medical record.
Population Denition
Patients age 5 through 55 years diagnosed with asthma continuously enrolled for 6 months.
Data of Interest
# of patients in the denominator with documentation in the record of education about asthma
total # of patients with asthma whose medical records are reviewed
Numerator/Denominator Denitions
Numerator: Documented is dened as any evidence in the medical record that a clinician provided patient
(or parent) education related to:
- basic facts about asthma
- role of medications
- skills (in managing asthma)
- environmental control measures
- when and how to take actions
- need for follow-up visits
Denominator: Patients with a diagnosis code of 493.00, 493.01, 493.10, 493.11, 493.90, 493.91, continuously
enrolled for 6 months.
Method/Source of Data Collection
Data may be collected electronically using the claims/encounter database or the enrollment database. Medical
groups should identify patients with asthma seen at the clinic. Each medical group can then generate a list
of all eligible patients with asthma seen during the target month/quarter. The eligible patients are those
who are 5-55 years old and have been diagnosed with asthma. A random sample of 20 charts can be chosen
from this list. The patients' medical records will be reviewed for any evidence that a clinician provided
patient education.
Time Frame Pertaining to Data Collection
A minimum of 20 charts per month can be reviewed.
Notes
Patient education is essential for successful management of asthma. It should begin at the time of diagnosis
and be ongoing.
Institute for Clinical Systems Improvement
www.icsi.org
45
Key Implementation Recommendations
The following system changes were identied by the guideline work group as key strategies for health care
systems to incorporate in support of the implementation of this guideline.
1. Facilitate timely and accurate diagnosis of asthma and asthma severity.
2. Educate providers in the use of spirometry as a diagnostic tool.
3. Educate providers and patients in the importance of developing and maintaining an asthma action plan
and assessing adherence.
Knowledge Products
Resources and knowledge products are developed by the guideline work group, member and non-member
organizations, or identied by ICSI staff as useful implementation tools.
1. Scientic Documents
Related guidelines
- Emergency and Inpatient Management of Asthma
- Chronic Obstructive Pulmonary Disease
- Rhinitis
3. Educational Resources
Improvement Case Report on Asthma: Family HealthServices Minnesota PA, Process Improvement
Report #19
HealthEast Case Improvement Report on Asthma, Process Improvement Report #4
Asthma Toolkit Action Plans; Assessment Surveys; Education (ideas for elementary classrooms);
Flow Sheets, Information/Patient Education Modules, Manual for Families of Children with Special
Needs; NAEPP Export Panel Report, Shingle; other tools.
ICSI has a wide varity of other knowledge products including tool kits on CQI processes and Rapid
Cycling that can be helpful. To obtain copies of these or other Knowledge Products, go to
http://www.icsi.org/knowledge.
Many of the materials listed in the Knowledge Products resource are only available to ICSI
members.
Diagnosis and Outpatient Management of Asthma
Seventh Edition/March 2005
Institute for Clinical Systems Improvement
www.icsi.org
46
Recommended Resources
Title/Description Audience Author/Organization Websites/Order Information
A national nonprot network
of families whose desire is to
overcome allergies and asthma
through knowledge. This web-
site provides accurate, timely,
practical, and livable
alternatives to suffering.
Patients
Professionals
Allergy and Asthma
Network/Mothers of
Asthmatics
http://www.aanma.org
Offers comprehensive
information for patients of all
ages. In-depth information on
medications, exacerbations,
peak ow meters and control
over environmental allergens.
Espaol material as well.
Patients
Professionals
ALA (American Lung
Association)
http://www.lungusa.org/
Resources from the American
Lung Association (ALA) are
available from: American Lung
Association of Minnesota, 490
Concordia Avenue, St. Paul,
MN 55103. (651)227-8014.
For clinics in Hennepin County
contact the American Lung
Association of Hennepin County,
4220 West Old Shakopee Road,
Suite 101, Bloomington, MN
55437. (952)885-0338.
http://www.alamn.org
The website offers asthma
education resources for patients
and providers. The site includes
special sections for children and
seniors, seasonal educational
materials. Health Headlines are
posted daily.
Patients
Professionals
American Academy of
Allergy, Asthma and
Immunology (AAAAI)
http://www.aaaai.org/
611 East Wells Street
Milwaukee, WI 53202
(800) 822-2762
Focus is on improving the
quality of life for people with
asthma and allergies and their
caregivers, through education,
advocacy and research. Provides
practical information,
community-based services,
support and referrals through a
national network of chapters and
educational groups.
Patients
Professionals
Asthma and Allergy
Foundation of America
http://www.aafa.org
Diagnosis and Outpatient Management of Asthma
Seventh Edition/March 2005
Institute for Clinical Systems Improvement
www.icsi.org
47
Criteria for Selecting Websites
The preceding websites were selected by the Diagnosis and Outpatient Management of Asthma guideline work group as
additional resources for practitioners and the public. The following criteria were considered in selecting these sites.
The site contains information specic to the particular disease or condition addressed in the guideline.
The site contains information that does not conict with the guideline's recommendations.
The information is accurate and/or factual. The author of the material or the sponsor of the site can be contacted
by means other than e-mail. For example, a nurse line or other support is provided.
The material includes the source/author, date and whether the information has been edited in any way. The
site clearly states revision dates or the date the information was placed on the internet.
The site sponsor is an objective group without an obvious or possible bias. For example, the site does not
promote a product, service or other provider.
The coverage of the topic is appropriate for the guideline's target audience. It is clearly written, well-organized
and easy to read. The site is easy to navigate.
Title/Description Audience Author/Organization Websites/Order Information
Offers asthma education that
incorporates an awareness of
indoor environmental asthma
triggers (e.g., secondhand
smoke, dust mites, mold, pet
dander, and cockroaches) and
actions that can be taken to
reduce children's exposure to
them in homes, schools and
child care settings.
Patients
Professionals
EPA (U.S. Environmental
Protection Agency)
http://www.epa.gov/iaq
Offers information for
healthcare professionals,
schools and patients about
asthma. An asthma action
plan is also included in
English and Spanish.
Patients and
Professionals
Minnesota Department of
Health
http://www.health.state.mn.us
Provides asthma health
education resources for
patients, school/day care
providers and health
professionals. Materials
written in Spanish are
available.
Patients
Professionals
National Heart, Lung, and
Blood Institute (NHLBI)
http://www.nhlbi.nih.gov
Brochure. Signs, symptoms,
management, MDI use
Patients Mayo Clinic,
Asthma
Mayo members call Mary Ann
Djonne at (507) 284-8780
Your Child's Asthma
Book, 26 pages
Patients Mayo Clinic Mayo members call Mary Ann
Djonne at (507) 284-8780
Diagnosis and Outpatient Management of Asthma
Recommended Website Resources Seventh Edition/March 2005
Summary of Changes March 2005
Diagnosis and Management of Asthma
Algorithm, Clinical Highlights, Annotations
Title: Revised the title of this guideline to: Diagnosis and Outpatient Management of Asthma.
This clearly differentiates it from the ER and Inpatient Management of Asthma
Guideline.
Added a bullet to Box #9 Asthma Educationhow medications work. This was also
added to the Clinical Highlight #5 (provide asthma education) and revised as an
independent item in Annotation #9 Asthma Education.
*1: Added Objective measures of lung function (FEV
1
PEF, PEF variability) to CSeverity
of symptom classification.
Throughout the guideline, added administered by nebulizer or metered dose inhaler
(MDI), either is acceptable.
*8: Added a statement and reference regarding Pregnancy in Asthma. Managing Asthma
during pregnancy is the same treatment used for non-pregnant asthma patients. NAEPP
Update, 2005. And, in table 8C, added a comment that Budesonide is the preferred
inhaled corticosteroid for use in pregnancy.
Also added reference Characterization of within-subject responses to flucticasone and
montelukast in childhood asthma. Szefler, 2005. This recent article also supports the
statement, Inhaled corticosteroids are the preferred treatment option for mild persistent
asthma in adults, and LTRAs are an alternative.
Added a statement recommending annual influenza vaccinations for patients with
persistent asthma
ICSI has developed a new format for all guidelines. Key additions and changes are:
The annotation and discussion section have been combined. Any duplicated
statements have been removed.
Most of the annotations will have Key Points at the beginning. This informs the
reader of key recommendations, highlights, or information pertinent to the steps of
the algorithm.
References in support of recommendations or conclusions are listed in the body of the
annotation. A complete list of references is included in the Supporting Evidence
section.
Priority Aims only will be listed in the front of the guideline section. Both aims and
measures are contained in the Support for Implementation section as usual.
Support for Implementation
Added new website from Minnesota Department of Health for asthma action plans
*An asterisk indicates any changes in clinical practice recommendation.
You might also like
- A Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryFrom EverandA Heartbreaking Work Of Staggering Genius: A Memoir Based on a True StoryRating: 3.5 out of 5 stars3.5/5 (231)
- The Sympathizer: A Novel (Pulitzer Prize for Fiction)From EverandThe Sympathizer: A Novel (Pulitzer Prize for Fiction)Rating: 4.5 out of 5 stars4.5/5 (119)
- Never Split the Difference: Negotiating As If Your Life Depended On ItFrom EverandNever Split the Difference: Negotiating As If Your Life Depended On ItRating: 4.5 out of 5 stars4.5/5 (838)
- Devil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaFrom EverandDevil in the Grove: Thurgood Marshall, the Groveland Boys, and the Dawn of a New AmericaRating: 4.5 out of 5 stars4.5/5 (265)
- The Little Book of Hygge: Danish Secrets to Happy LivingFrom EverandThe Little Book of Hygge: Danish Secrets to Happy LivingRating: 3.5 out of 5 stars3.5/5 (399)
- Grit: The Power of Passion and PerseveranceFrom EverandGrit: The Power of Passion and PerseveranceRating: 4 out of 5 stars4/5 (587)
- The World Is Flat 3.0: A Brief History of the Twenty-first CenturyFrom EverandThe World Is Flat 3.0: A Brief History of the Twenty-first CenturyRating: 3.5 out of 5 stars3.5/5 (2219)
- The Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeFrom EverandThe Subtle Art of Not Giving a F*ck: A Counterintuitive Approach to Living a Good LifeRating: 4 out of 5 stars4/5 (5794)
- Team of Rivals: The Political Genius of Abraham LincolnFrom EverandTeam of Rivals: The Political Genius of Abraham LincolnRating: 4.5 out of 5 stars4.5/5 (234)
- Shoe Dog: A Memoir by the Creator of NikeFrom EverandShoe Dog: A Memoir by the Creator of NikeRating: 4.5 out of 5 stars4.5/5 (537)
- The Emperor of All Maladies: A Biography of CancerFrom EverandThe Emperor of All Maladies: A Biography of CancerRating: 4.5 out of 5 stars4.5/5 (271)
- The Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreFrom EverandThe Gifts of Imperfection: Let Go of Who You Think You're Supposed to Be and Embrace Who You AreRating: 4 out of 5 stars4/5 (1090)
- Her Body and Other Parties: StoriesFrom EverandHer Body and Other Parties: StoriesRating: 4 out of 5 stars4/5 (821)
- The Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersFrom EverandThe Hard Thing About Hard Things: Building a Business When There Are No Easy AnswersRating: 4.5 out of 5 stars4.5/5 (344)
- Hidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceFrom EverandHidden Figures: The American Dream and the Untold Story of the Black Women Mathematicians Who Helped Win the Space RaceRating: 4 out of 5 stars4/5 (890)
- Elon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureFrom EverandElon Musk: Tesla, SpaceX, and the Quest for a Fantastic FutureRating: 4.5 out of 5 stars4.5/5 (474)
- The Unwinding: An Inner History of the New AmericaFrom EverandThe Unwinding: An Inner History of the New AmericaRating: 4 out of 5 stars4/5 (45)
- The Yellow House: A Memoir (2019 National Book Award Winner)From EverandThe Yellow House: A Memoir (2019 National Book Award Winner)Rating: 4 out of 5 stars4/5 (98)
- Legal Medicine ReviewerDocument13 pagesLegal Medicine ReviewerJernel Janz100% (1)
- On Fire: The (Burning) Case for a Green New DealFrom EverandOn Fire: The (Burning) Case for a Green New DealRating: 4 out of 5 stars4/5 (73)
- Graphology by June.E.Downey (Book Written in 1919)Document160 pagesGraphology by June.E.Downey (Book Written in 1919)Nav D100% (6)
- Pharmacy DC Pharmacy Laws and RegulationsDocument430 pagesPharmacy DC Pharmacy Laws and RegulationsTanganGondrongNo ratings yet
- Umbra Cuvintelor Octavian PalerDocument51 pagesUmbra Cuvintelor Octavian PalerCismaru Elena100% (1)
- Janssen 2008Document8 pagesJanssen 2008Alina GheNo ratings yet
- 81 Full PDFDocument13 pages81 Full PDFAlina GheNo ratings yet
- Risk Perception: Nicolai Bodemer and Wolfgang GaissmaierDocument14 pagesRisk Perception: Nicolai Bodemer and Wolfgang GaissmaierAlina GheNo ratings yet
- Anxiety and Panic in Chronic Obstructive Pulmonary Disease: The Role of Catastrophic ThoughtsDocument13 pagesAnxiety and Panic in Chronic Obstructive Pulmonary Disease: The Role of Catastrophic ThoughtsAlina Ghe100% (1)
- Integrative Cancer Therapies: The Impact of Healing Touch On Pediatric Oncology PatientsDocument7 pagesIntegrative Cancer Therapies: The Impact of Healing Touch On Pediatric Oncology PatientsAlina GheNo ratings yet
- 217 FullDocument10 pages217 FullAlina GheNo ratings yet
- Freest On 1994Document12 pagesFreest On 1994Alina GheNo ratings yet
- Craske 2001Document20 pagesCraske 2001Alina GheNo ratings yet
- 43 Full PDFDocument10 pages43 Full PDFAlina GheNo ratings yet
- Integrative Cancer Therapies: An Oncology Mind-Body Medicine Day Care Clinic: Concept and Case PresentationDocument6 pagesIntegrative Cancer Therapies: An Oncology Mind-Body Medicine Day Care Clinic: Concept and Case PresentationAlina GheNo ratings yet
- 346 FullDocument16 pages346 FullAlina GheNo ratings yet
- 455 FullDocument10 pages455 FullAlina GheNo ratings yet
- 496 FullDocument8 pages496 FullAlina GheNo ratings yet
- 158 FullDocument18 pages158 FullAlina GheNo ratings yet
- 201 FullDocument11 pages201 FullAlina GheNo ratings yet
- Managementul Emboliei Pulmonare PDFDocument23 pagesManagementul Emboliei Pulmonare PDFAlina GheNo ratings yet
- 167 FullDocument10 pages167 FullAlina GheNo ratings yet
- Balter GuidelinesDocument30 pagesBalter GuidelinesAlina GheNo ratings yet
- Evaluare Pentru Terapia Cu OxigenDocument3 pagesEvaluare Pentru Terapia Cu OxigenAlina GheNo ratings yet
- 283 FullDocument22 pages283 FullAlina GheNo ratings yet
- FingerprintpatternDocument21 pagesFingerprintpatternAlina GheNo ratings yet
- Boala Parenchimatoasa Pulmonara DifuzaDocument30 pagesBoala Parenchimatoasa Pulmonara DifuzaAlina GheNo ratings yet
- Psychological Science: Business Not As UsualDocument5 pagesPsychological Science: Business Not As UsualAlina GheNo ratings yet
- Psychological Science: ''Top-Down'' Effects Where None Should Be Found: The El Greco Fallacy in Perception ResearchDocument10 pagesPsychological Science: ''Top-Down'' Effects Where None Should Be Found: The El Greco Fallacy in Perception ResearchAlina GheNo ratings yet
- Tratamentul Inhalator Al Astmului Bronsic La CopilDocument14 pagesTratamentul Inhalator Al Astmului Bronsic La CopilAlina GheNo ratings yet
- Astm Bronsic CANDocument3 pagesAstm Bronsic CANAlina GheNo ratings yet
- Hematopoiesis - Curs (Engl)Document9 pagesHematopoiesis - Curs (Engl)Alina GheNo ratings yet
- Assignment Marks: 30: InstructionsDocument3 pagesAssignment Marks: 30: InstructionsAYUSH PRADHANNo ratings yet
- News Letter Feb - Mar2022Document17 pagesNews Letter Feb - Mar2022Pushpanjali HospitalNo ratings yet
- Nacho LibreDocument6 pagesNacho Libreapi-257172337100% (1)
- 2ndgfmd Report PDFDocument236 pages2ndgfmd Report PDFSAURABH KUMARNo ratings yet
- Dengue Clinical Presentation - History, Physical ExaminationDocument6 pagesDengue Clinical Presentation - History, Physical Examinationm.m.m.mNo ratings yet
- Sensors BMS PDFDocument45 pagesSensors BMS PDFPearl BaskarNo ratings yet
- 1950 Third - Inter - American - Congress - On - BrucellDocument327 pages1950 Third - Inter - American - Congress - On - BrucellcostanicolevNo ratings yet
- Checklist For Persons Under Monitoring (PUM) : Eastern VisayasDocument1 pageChecklist For Persons Under Monitoring (PUM) : Eastern VisayasSophie Rose V R-zNo ratings yet
- Trey Walden ResumeDocument2 pagesTrey Walden Resumeapi-402141887No ratings yet
- PHD Thesis by Publication - MD IRTEJA ISLAM - 0061107404 - 200521Document228 pagesPHD Thesis by Publication - MD IRTEJA ISLAM - 0061107404 - 200521Tanvir Ahmed NayeemNo ratings yet
- CV Drg. Jeffry KurniawanDocument1 pageCV Drg. Jeffry KurniawanJeffry KurniawanNo ratings yet
- National Programme For Prevenation and Control of Cancer, Diabetes, CardiovascularDocument10 pagesNational Programme For Prevenation and Control of Cancer, Diabetes, Cardiovascularnandini singhNo ratings yet
- Influence of Preoperative Patient Factors On Tka OutcomesDocument5 pagesInfluence of Preoperative Patient Factors On Tka OutcomesHerald Scholarly Open AccessNo ratings yet
- Cornwall & Isles of Scilly LMC Newsletter Dec 2013Document8 pagesCornwall & Isles of Scilly LMC Newsletter Dec 2013Cornwall and Isles of Scilly LMCNo ratings yet
- Nursing Care PlanDocument26 pagesNursing Care PlanNeil Anthony78% (18)
- Mentor Assessment 1Document2 pagesMentor Assessment 1api-539190120No ratings yet
- DUPIXENT Doctor Discussion GuideDocument4 pagesDUPIXENT Doctor Discussion GuideTAP THANH CHAUNo ratings yet
- Cir 0000000000000628Document101 pagesCir 0000000000000628Diana AngelesNo ratings yet
- Screenshot 2019-11-26 at 19.19.16Document2 pagesScreenshot 2019-11-26 at 19.19.16mesho twoNo ratings yet
- Updated Resume DKDocument5 pagesUpdated Resume DKDK Aquino GomezNo ratings yet
- Antimicrobial-Awareness-Week OtsuzolDocument46 pagesAntimicrobial-Awareness-Week Otsuzolhassan shahidNo ratings yet
- Dr. Marvin T. Reyes MD infectious disease specialistDocument1 pageDr. Marvin T. Reyes MD infectious disease specialistMicah TidwellNo ratings yet
- Hospital Accreditation: Improving Quality CareDocument19 pagesHospital Accreditation: Improving Quality Caredr_vikasNo ratings yet
- Health Quiz No. 2 TitleDocument2 pagesHealth Quiz No. 2 TitleLove LeiNo ratings yet
- Nursing Care Plan PreoperativeDocument5 pagesNursing Care Plan Preoperativekuro hanabusaNo ratings yet
- Campbell Julie Resume 2023Document2 pagesCampbell Julie Resume 2023api-588270833No ratings yet
- Object Localization TechniqueDocument9 pagesObject Localization TechniqueShabana Serju50% (2)
- Ra-105320 Professional Teacher - Elementary Bacolod 10-2022Document70 pagesRa-105320 Professional Teacher - Elementary Bacolod 10-2022Arman D. VillarascoNo ratings yet